Post-Delivery Milking Delay Influence on the Effect of Oral Supplementation with Bovine Colostrum as Measured with Intestinal Permeability Test

 ,
,  , , and
, , and
Abstract
:1. Introduction
- The hygiene standards of harvesting—the cleaner the collection, the fewer and the less aggressive manipulations are required to obtain a microbiologically clean final product;
- The time of milking the colostrum—the sooner after delivery, the higher the content of biologically active products in colostrum;
- The method used to obtain dehydrated product—the less aggressive thermic treatment used, the better the chance of preserving the bioactivity of the proteins and peptides in the product.
2. Materials and Methods
2.1. Recruitment
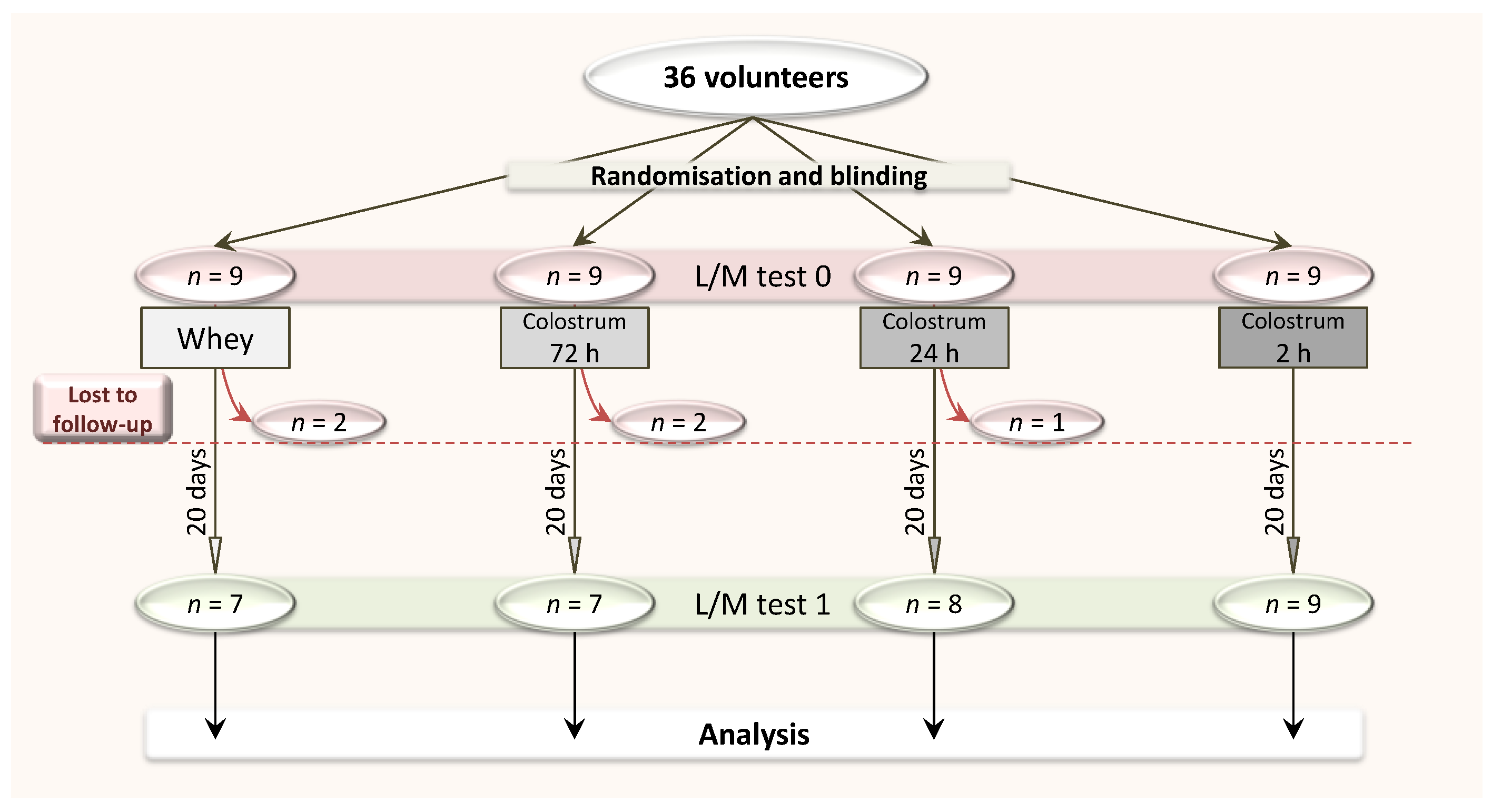
2.2. Study Design
2.2.1. Allocation of Participants to Tested Groups and Initial Assessment: Day 0
2.2.2. Supplementation: Days 1–20
2.2.3. Final Assessment: Day 21
2.3. The Lactulose/Mannitol (L/M) Differential Sugar Absorption Test
2.3.1. Sugar Ingestion and Urine Collection
2.3.2. L/M Test Procedure
2.4. Reference Limits
2.5. Statistical Analysis
2.6. Bioethical Approval
3. Results
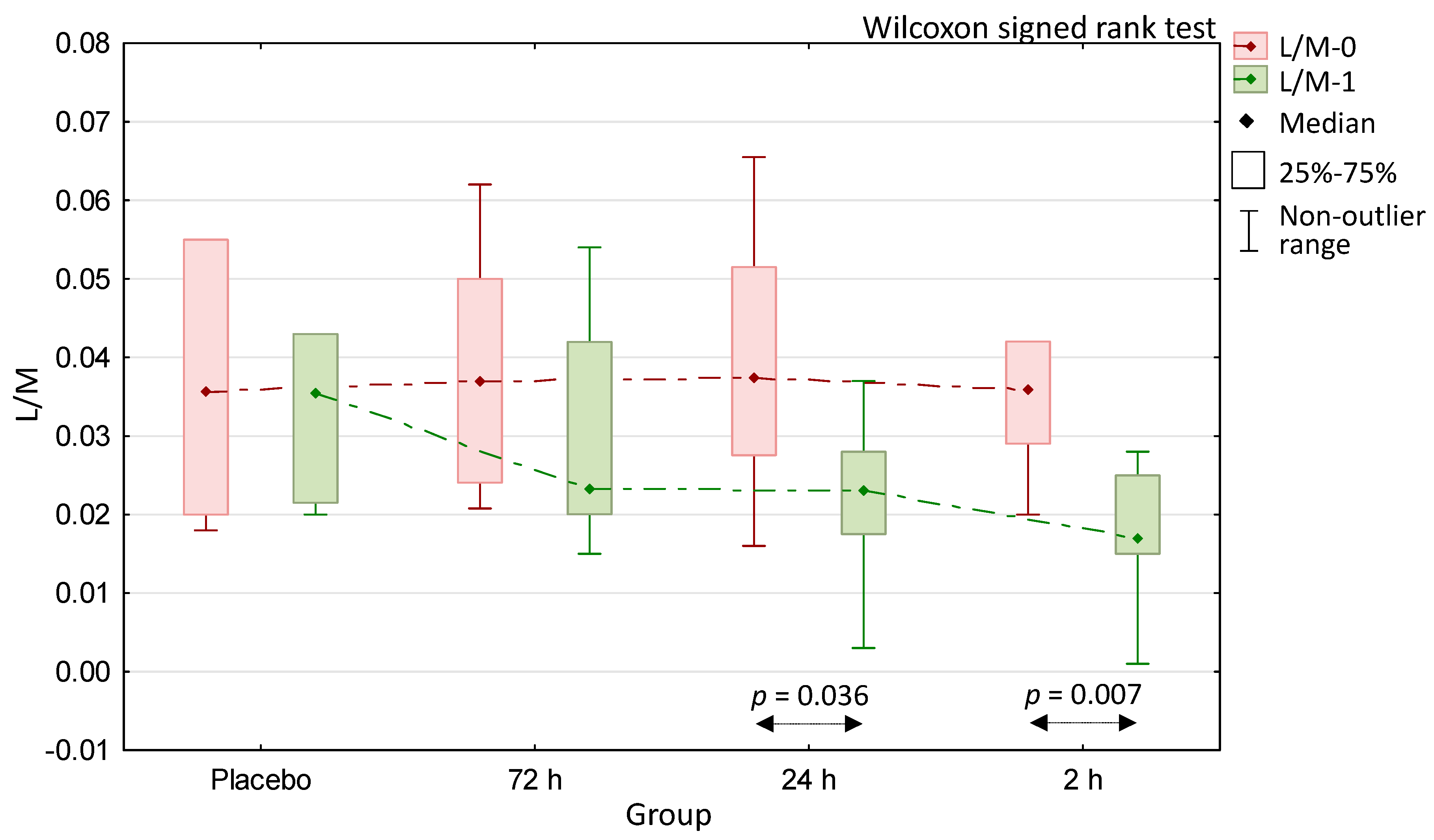
3.1. Change of Intestinal Permeability upon Supplementation across the Groups
3.2. Comparison of Intestinal Permeability Change (Δ) Due to Supplementation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dwyer, J.T.; Coates, P.M.; Smith, M.J. Dietary Supplements: Regulatory Challenges and Research Resources. Nutrients 2018, 10, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shenkar, J.; Griffiths, J.C. Industry Actions to Address Quality Issues for Dietary Supplements, Botanicals, and Other Natural Products. Clin. Pharmacol. Ther. 2018, 104, 423–425. [Google Scholar] [CrossRef] [PubMed]
- Kelly, G.S. Bovine colostrums: A review of clinical uses. Altern. Med. Rev. 2003, 8, 378–394. [Google Scholar] [PubMed]
- Struff, W.G.; Sprotte, G. Bovine colostrum as a biologic in clinical medicine: A review—Part II: Clinical studies. Int. J. Clin. Pharmacol. Ther. 2008, 46, 211–225. [Google Scholar] [CrossRef] [Green Version]
- Rathe, M.; Müller, K.; Sangild, P.T.; Husby, S. Clinical applications of bovine colostrum therapy: A systematic review. Nutr. Rev. 2014, 72, 237–254. [Google Scholar] [CrossRef]
- Struff, W.G.; Sprotte, G. Bovine colostrum as a biologic in clinical medicine: A review. Part I: Biotechnological standards, pharmacodynamic and pharmacokinetic characteristics and principles of treatment. Int. J. Clin. Pharmacol. Ther. 2007, 45, 193–202. [Google Scholar] [CrossRef]
- Sacerdote, P.; Mussano, F.; Franchi, S.; Panerai, A.E.; Bussolati, G.; Carossa, S.; Bartorelli, A.; Bussolati, B. Biological components in a standardized derivative of bovine colostrum. J. Dairy Sci. 2013, 96, 1745–1754. [Google Scholar] [CrossRef] [Green Version]
- Morrill, K.M.; Conrad, E.; Lago, A.; Campbell, J.; Quigley, J.; Tyler, H. Nationwide evaluation of quality and composition of colostrum on dairy farms in the United States. J. Dairy Sci. 2012, 95, 3997–4005. [Google Scholar] [CrossRef] [Green Version]
- Kehoe, S.I.; Jayarao, B.M.; Heinrichs, A.J. A survey of bovine colostrum composition and colostrum management practices on Pennsylvania dairy farms. J. Dairy Sci. 2007, 90, 4108–4116. [Google Scholar] [CrossRef] [Green Version]
- Purup, S.; Vestergaard, M.; Pedersen, L.O.; Sejrsen, K. Biological activity of bovine milk on proliferation of human intestinal cells. J. Dairy Res. 2007, 74, 58–65. [Google Scholar] [CrossRef]
- Playford, R.J.; MacDonald, C.E.; Calnan, D.P.; Floyd, D.N.; Podas, T.; Johnson, W.; Wicks, A.C.; Bashir, O.; Marchbank, T. Co-administration of the health food supplement, bovine colostrum, reduces the acute non-steroidal anti-inflammatory drug-induced increase in intestinal permeability. Clin. Sci. 2001, 100, 627–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davison, G.; Marchbank, T.; March, D.S.; Thatcher, R.; Playford, R.J. Zinc carnosine works with bovine colostrum in truncating heavy exercise-induced increase in gut permeability in healthy volunteers. Am. J. Clin. Nutr. 2016, 104, 526–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrillo, A.E.; Koutedakis, Y.; Flouris, A.D. Exercise and exposure to heat following bovine colostrum supplementation: A review of gastrointestinal and immune function. Cell. Mol. Biol. 2013, 59, 84–88. [Google Scholar] [PubMed]
- Marchbank, T.; Davison, G.; Oakes, J.R.; Ghatei, M.A.; Patterson, M.; Moyer, M.P.; Playford, R.J. The nutriceutical bovine colostrum truncates the increase in gut permeability caused by heavy exercise in athletes. Am. J. Physiol. Gastrointest. Liver Physiol. 2011, 300, G477–G484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hałasa, M.; Maciejewska, D.; Baśkiewicz-Hałasa, M.; Machaliński, B.; Safranow, K.; Stachowska, E. Oral Supplementation with Bovine Colostrum Decreases Intestinal Permeability and Stool Concentrations of Zonulin in Athletes. Nutrients 2017, 9, 370. [Google Scholar] [CrossRef] [PubMed]
- Georgiev, I.P. Alterations in chemical composition of colostrum in relationship to post-partum time. Bulg. J. Vet. Med. 2005, 8, 35–39. [Google Scholar]
- Ballard, O.; Morrow, A.L. Human Milk Composition: Nutrients and Bioactive Factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [Green Version]
- Puppel, K.; Gołębiewski, M.; Grodkowski, G.; Slósarz, J.; Kunowska-Slósarz, M.; Solarczyk, P.; Łukasiewicz, M.; Balcerak, M.; Przysucha, T. Composition and Factors Affecting Quality of Bovine Colostrum: A Review. Animals 2019, 9, 1070. [Google Scholar] [CrossRef] [Green Version]
- Lamprecht, M.; Bogner, S.; Schippinger, G.; Steinbauer, K.; Fankhauser, F.; Hallstroem, S.; Schuetz, B.; Greilberger, J.F. Probiotic supplementation affects markers of intestinal barrier, oxidation, and inflammation in trained men; a randomized, double-blinded, placebo-controlled trial. J. Int. Soc. Sports Nutr. 2012, 9, 45. [Google Scholar] [CrossRef] [Green Version]
- Hałasa, M.; Maciejewska, D.; Ryterska, K.; Baśkiewicz-Hałasa, M.; Safranow, K.; Stachowska, E. Assessing the Association of Elevated Zonulin Concentration in Stool with Increased Intestinal Permeability in Active Professional Athletes. Medicina 2019, 55, E710. [Google Scholar] [CrossRef] [Green Version]
- Boudry, C.; Dehoux, J.-P.; Portetelle, D.; Buldgen, A. Bovine colostrum as a natural growth promoter for newly weaned piglets: A review. Biotechnol. Agron. Soc. Environ. 2008, 12, 157–170. [Google Scholar]
- Korhonen, H. Antimicrobial factors in bovine colostrum. Agric. Food Sci. 1977, 49, 434–447. [Google Scholar] [CrossRef]
- Pakkanen, R.; Aalto, J. Growth factors and antimicrobial factors of bovine colostrum. Int. Dairy J. 1997, 7, 285–297. [Google Scholar] [CrossRef]
- Abd El-Fattah, A.M.; Abd Rabo, F.H.; El-Dieb, S.M.; El-Kashef, H.A. Changes in composition of colostrum of Egyptian buffaloes and Holstein cows. BMC Vet. Res. 2012, 5, 8–19. [Google Scholar] [CrossRef] [Green Version]
- Elfstrand, L.; Lindmark-Månsson, H.; Paulsson, M.; Akesson, B. Immunoglobulins, growth factors and growth hormone in bovine colostrum and the effects of processing. Int. Dairy J. 2002, 12, 879–887. [Google Scholar] [CrossRef]
- Cairangzhuoma; Yamamoto, M.; Muranishi, H.; Inagaki, M.; Uchida, K.; Yamashita, K.; Saito, S.; Yabe, T.; Kanamaru, Y. Skimmed, sterilized, and concentrated bovine late colostrum promotes both prevention and recovery from intestinal tissue damage in mice. J. Dairy Sci. 2013, 96, 1347–1355. [Google Scholar] [CrossRef] [Green Version]
- Godden, S.M.; Lombard, J.E.; Woolums, A.R. Colostrum Management for Dairy Calves. Vet. Clin. N. Am. Food Anim. Pract. 2019, 35, 535–556. [Google Scholar] [CrossRef]
- Morin, D.E.; Nelson, S.V.; Reid, E.D.; Nagy, D.W.; Dahl, G.E.; Constable, P.D. Effect of colostral volume, interval between calving and first milking, and photoperiod on colostral IgG concentrations in dairy cows. J. Am. Vet. Med. Assoc. 2010, 237, 420–428. [Google Scholar] [CrossRef]
- Jones, A.W.; March, D.S.; Curtis, F.; Bridle, C. Bovine colostrum supplementation and upper respiratory symptoms during exercise training: A systematic review and meta-analysis of randomised controlled trials. BMC Sports Sci. Med. Rehabil. 2016, 8, 21. [Google Scholar] [CrossRef] [Green Version]
- Bhavani Ramya, S.; Ramasamy, D.; Dhineshkumar, V. Effects of Refrigeration, Deep Freezing-Spray Drying and Pasteurization on IgG Bovine Colostrum Preservation. Int. J. Dairy Process Res. 2016, 3, 35–37. [Google Scholar]
- Mishra, A.; Makharia, G.K. Techniques of Functional and Motility Test: How to Perform and Interpret Intestinal Permeability. J. Neurogastroenterol. Motil. 2012, 18, 443–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graziani, C.; Talocco, C.; De Sire, R.; Petito, V.; Lopetuso, L.R.; Gervasoni, J.; Persichilli, S.; Franceschi, F.; Ojetti, V.; Gasbarrini, A.; et al. Intestinal permeability in physiological and pathological conditions: Major determinants and assessment modalities. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 795–810. [Google Scholar] [CrossRef] [PubMed]
- Karhu, E.; Forsgård, R.A.; Alanko, l.; Alfthan, H.; Pussinen, P.; Hämäläinen, E.; Korpela, R. Exercise and gastrointestinal symptoms: Running-induced changes in intestinal permeability and markers of gastrointestinal function in asymptomatic and symptomatic runners. Eur. J. Appl. Physiol. 2017, 117, 2519–2526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, R.; Sorrell, M.; Batra, S.; Dhawan, P.; Singh, A.B. Gut permeability and mucosal inflammation: Bad, good or context dependent. Mucosal Immunol. 2017, 10, 307–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cesarone, M.R.; Belcaro, G.; Di Renzo, A.; Dugall, M.; Cacchio, M.; Ruffini, I.; Pellegrini, L.; Del Boccio, G.; Fano, F.; Ledda, A.; et al. Prevention of influenza episodes with colostrum compared with vaccination in healthy and high-risk cardiovascular subjects: The epidemiologic study in San Valentino. Clin. Appl. Thromb. Hemost. 2007, 13, 130–136. [Google Scholar] [CrossRef]
- Lynn, D.J.; Pulendran, B. The potential of the microbiota to influence vaccine responses. J. Leukoc. Biol. 2018, 103, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Fasano, A. Physiological, Pathological, and Therapeutic Implications of Zonulin-Mediated Intestinal Barrier Modulation: Living Life on the Edge of the Wall. Am. J. Pathol. 2008, 173, 1243–1252. [Google Scholar] [CrossRef] [Green Version]
- Fasano, A. Zonulin and its regulation of intestinal barrier function: The biological door to inflammation, autoimmunity, and cancer. Physiol. Rev. 2011, 91, 151–175. [Google Scholar] [CrossRef] [Green Version]
- Chelakkot, C.; Ghim, J.; Ryu, S.H. Mechanisms regulating intestinal barrier integrity and its pathological implications. Exp. Mol. Med. 2018, 50, 103. [Google Scholar] [CrossRef] [Green Version]
- Arrieta, M.C.; Bistritz, L.; Meddings, J.B. Alterations in intestinal permeability. Gut 2006, 55, 1512–1520. [Google Scholar] [CrossRef] [Green Version]
- Bodammer, P.; Kerkhoff, C.; Maletzki, C.; Lamprecht, G. Bovine Colostrum Increases Pore-Forming claudin-2 Protein Expression but Paradoxically Not Ion Permeability Possibly by a Change of the Intestinal Cytokine Milieu. PLoS ONE 2013, 8, e64210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Playford, R.J.; Cattell, M.; Marchbank, T. Marked variability in bioactivity between commercially available bovine colostrum for human use; implications for clinical trials. PLoS ONE 2020, 15, e0234719. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| L/M-0 Equal or Above Reference Limit | L/M-1 Equal or Above Reference Limit | L/M Δ <0 | |
|---|---|---|---|
| Placebo | 4 | 4 | 3 |
| n = 7 | 57% | 57% | 43% |
| Colostrum 72 h | 5 | 3 | 4 |
| n = 7 | 71% | 43% | 57% |
| Colostrum 24 h | 6 | 1 | 6 |
| n = 8 | 75% | 13% | 75% |
| Colostrum 2 h | 6 | 1 | 9 |
| n = 9 | 67% | 11% | 100% * |
| p-value (exact test for 4 × 2 table) | 0.95 | 0.15 | 0.049 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hałasa, M.; Maciejewska-Markiewicz, D.; Baśkiewicz-Hałasa, M.; Safranow, K.; Stachowska, E. Post-Delivery Milking Delay Influence on the Effect of Oral Supplementation with Bovine Colostrum as Measured with Intestinal Permeability Test. Medicina 2020, 56, 495. https://doi.org/10.3390/medicina56100495
Hałasa M, Maciejewska-Markiewicz D, Baśkiewicz-Hałasa M, Safranow K, Stachowska E. Post-Delivery Milking Delay Influence on the Effect of Oral Supplementation with Bovine Colostrum as Measured with Intestinal Permeability Test. Medicina. 2020; 56(10):495. https://doi.org/10.3390/medicina56100495
Chicago/Turabian StyleHałasa, Maciej, Dominika Maciejewska-Markiewicz, Magdalena Baśkiewicz-Hałasa, Krzysztof Safranow, and Ewa Stachowska. 2020. "Post-Delivery Milking Delay Influence on the Effect of Oral Supplementation with Bovine Colostrum as Measured with Intestinal Permeability Test" Medicina 56, no. 10: 495. https://doi.org/10.3390/medicina56100495