The Impact of Prostate Cancer Upgrading and Upstaging on Biochemical Recurrence and Cancer-Specific Survival

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Study Population
3.2. Upgrading, Upstaging and Surgical Margin
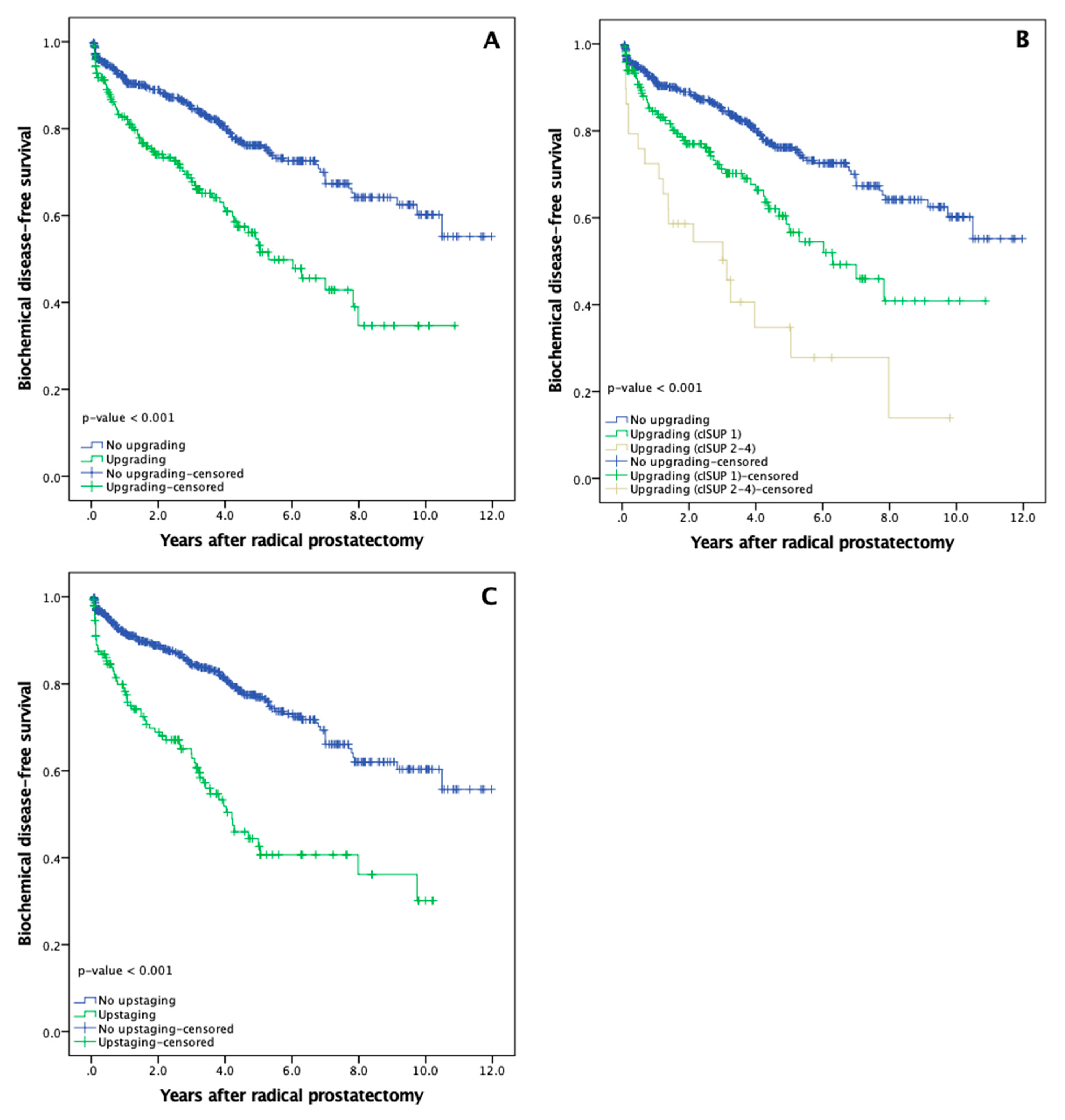
3.3. Biochemical Recurrence
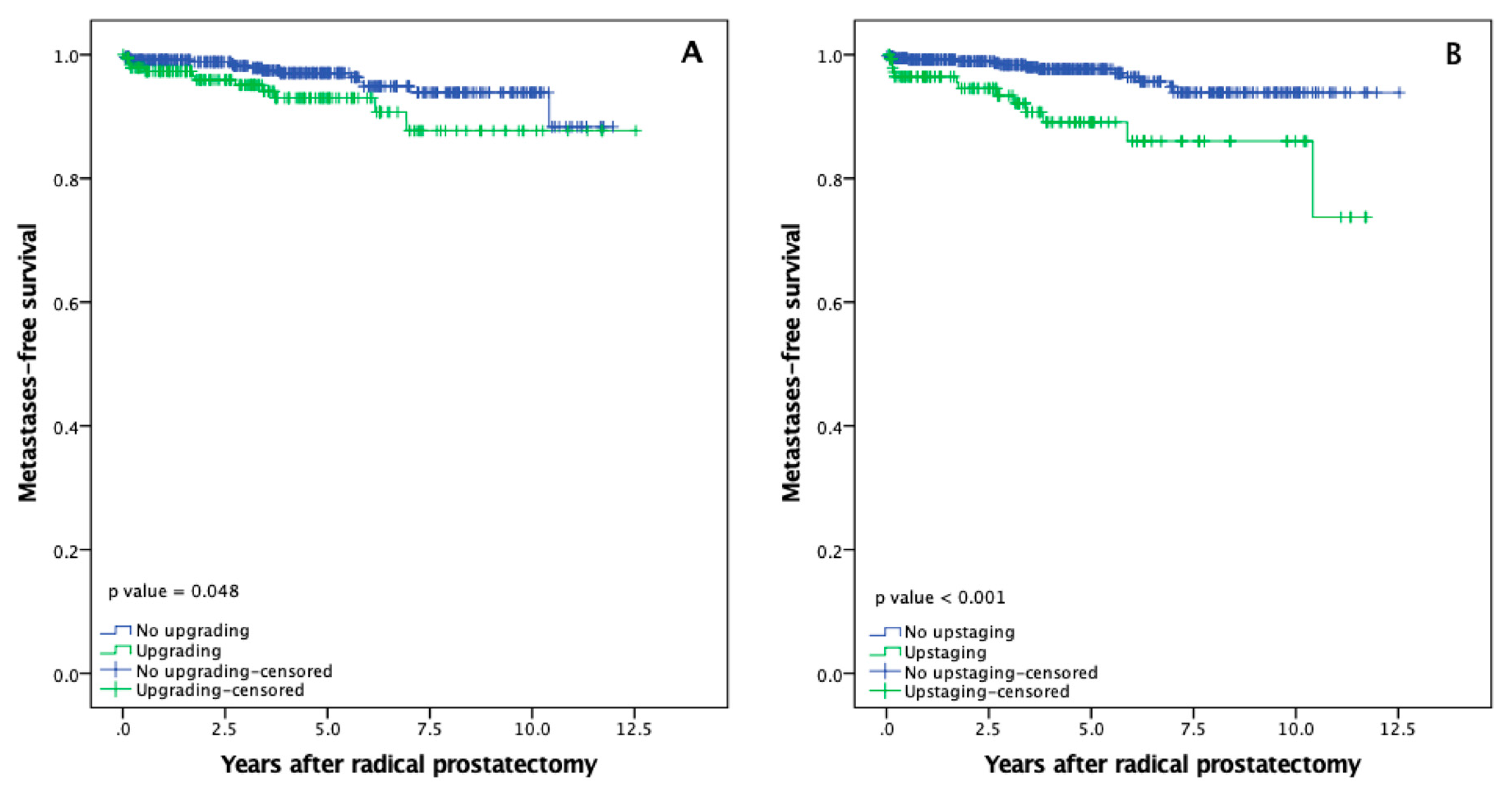
3.4. Metastasis-Free Survival
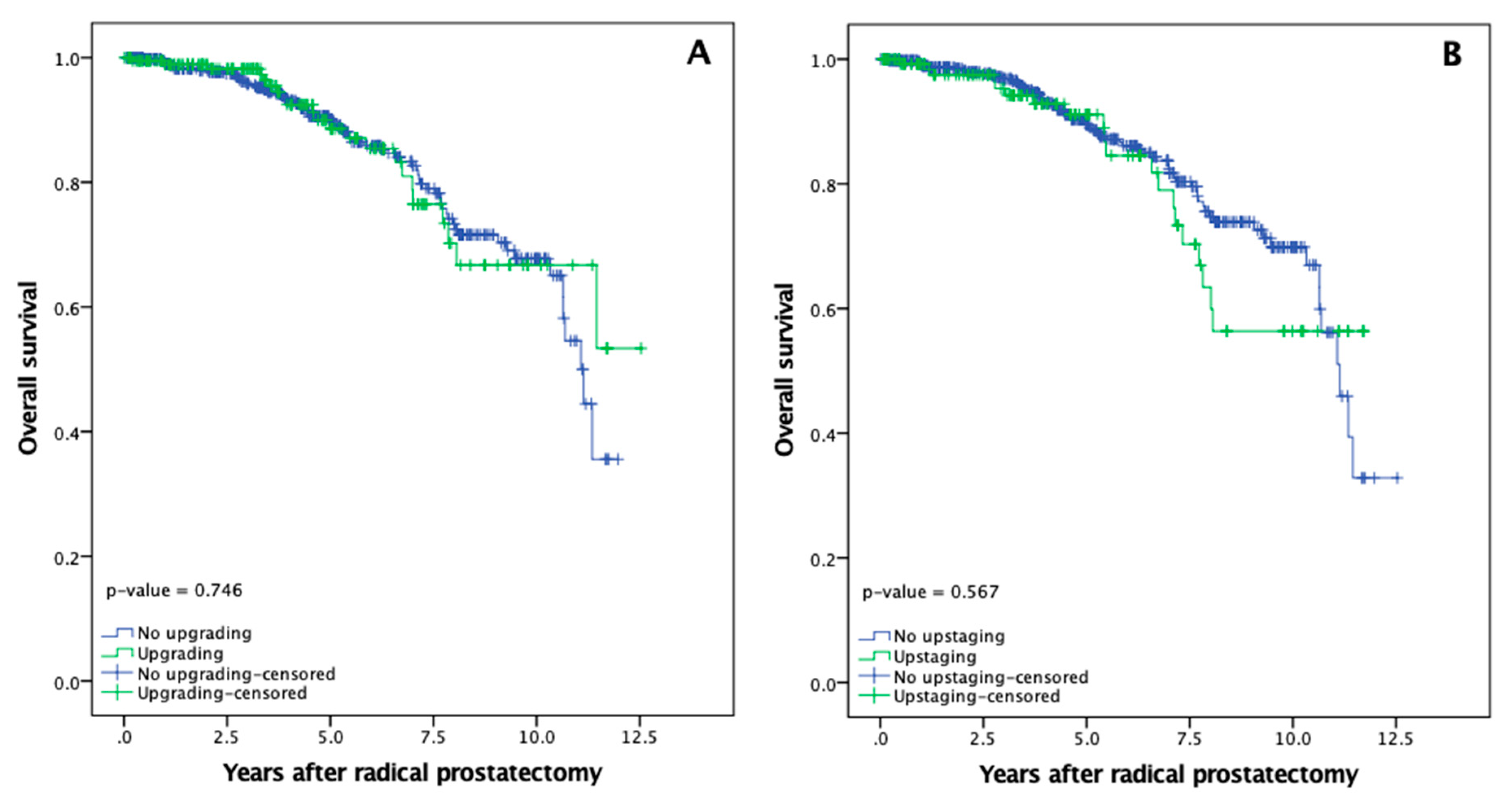
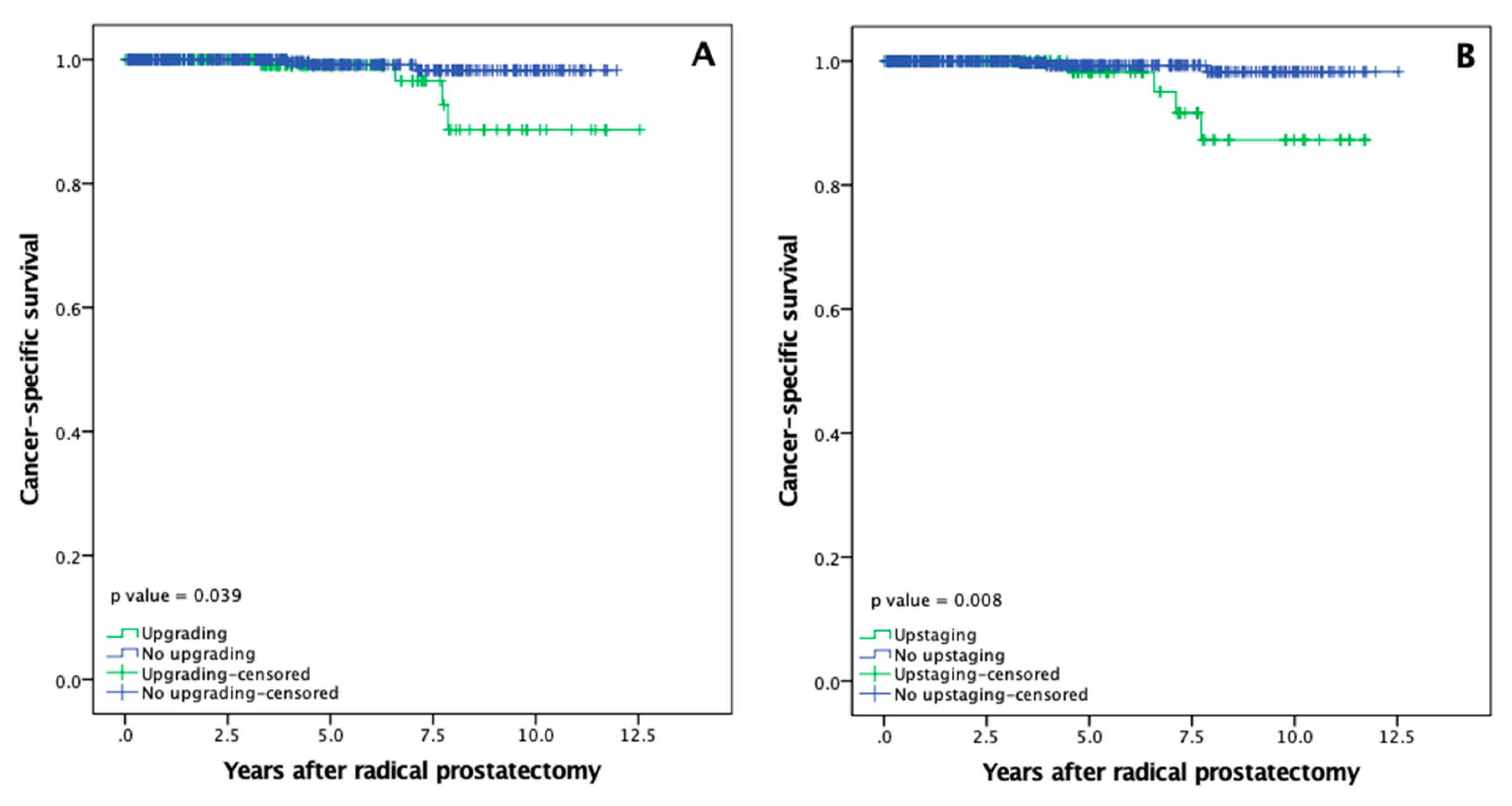
3.5. Overall and Cancer Specific Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; Abdulle, A.S.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar]
- Tolkach, Y.; Kristiansen, G. The Heterogeneity of Prostate Cancer: A Practical Approach. Pathobiology 2018, 85, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Ruijter, E.T.; Van De Kaa, C.A.; Schalken, J.A.; Debruyne, F.M.; Ruiter, D.J. Histological Grade Heterogeneity in Multifocal Prostate Cancer. Biological and Clinical Implications. J. Pathol. 1996, 180, 295–299. [Google Scholar] [CrossRef]
- Cintra, M.L.; Billis, A. Histologic grading of prostatic adenocarcinoma: Intraobserver reproducibility of the Mostofi, Gleason and Böcking grading systems. Int. Urol. Nephrol. 1991, 23, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y. Promoter Hypermethylation as a Biomarker in Prostate Adenocarcinoma. In Cancer Epigenetics; Verma, M., Ed.; Humana Press: New York, NY, USA, 2015; Volume 1238, pp. 607–625. [Google Scholar]
- Brassetti, A.; Lombardo, R.; Emiliozzi, P.; Cardi, A.; Antonio, I.; Aldo, S.; Tommaso, R.; Alberto, P. Prostate-specific Antigen Density Is a Good Predictor of Upstaging and Upgrading, According to the New Grading System: The Keys We Are Seeking May Be Already in Our Pocket. Urology 2018, 111, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Bakavicius, A.; Daniunaite, K.; Zukauskaite, K.; Barisiene, M.; Jarmalaite, S.; Jankevicius, F. Urinary DNA Methylation Biomarkers for Prediction of Prostate Cancer Upgrading and Upstaging. Clin. Epigenet. 2019, 11, 115. [Google Scholar] [CrossRef] [Green Version]
- Epstein, J.I.; Allsbrook, W.C., Jr.; Amin, M.B.; Egevad, L.L.; ISUP Grading Committee. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2005, 29, 1228–1242. [Google Scholar] [CrossRef] [Green Version]
- Epstein, J.I.; Amin, M.; Boccon-Gibod, L.; Egevad, L.; Humphrey, P.A.; Mikuz, G.; Newling, D.; Nilsson, S.; Sakr, W.; Srigley, J.R.; et al. Prognostic Factors and Reporting of Prostate Carcinoma in Radical Prostatectomy and Pelvic Lymphadenectomy Specimens. Scand. J. Urol. Neophrol. Suppl. 2005, 216, 34–63. [Google Scholar] [CrossRef]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Moul, J.W. Prostate Specific Antigen Only Progression of Prostate Cancer. J. Urol. 2000, 163, 1632–1642. [Google Scholar] [CrossRef]
- Assel, M.; Sjoberg, D.; Elders, A.; Wang, X.; Huo, D.; Botchway, A.; Delfino, K.; Fan, Y.; Zhao, Z.; Koyama, T.; et al. Guidelines for Reporting Statistics for Clinical Research in Urology. Eur. Urol. 2019, 75, 358–367. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.A.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical Outcome after Radical Prostatectomy, External Beam Radiation Therapy, or Interstitial Radiation Therapy for Clinically Localized Prostate Cancer. JAMA 1998, 280, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Imnadze, M.; Sjoberg, D.D.; Vickers, A.J. Adverse Pathologic Features at Radical Prostatectomy: Effect of Preoperative Risk on Oncologic Outcomes. Eur. Urol. 2016, 69, 143–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeldres, C.; Suardi, N.; Walz, J.; Hutterer, G.C.; Ahyai, S.; Lattouf, J.B.; Haese, A.; Graefen, M.; Erbersdobler, A.; Heinzer, H.; et al. Validation of the Contemporary Epstein Criteria for Insignificant Prostate Cancer in European Men. Eur. Urol. 2008, 54, 1306–1313. [Google Scholar] [CrossRef]
- Beauval, J.B.; Ploussard, G.; Soulié, M.; Pfister, C.; Van Agt, S.; Vincendeau, S.; Larue, S.; Rigaud, J.; Gaschignard, N.; Rouprêt, M.; et al. Pathologic Findings in Radical Prostatectomy Specimens from Patients Eligible for Active Surveillance with Highly Selective Criteria: A Multicenter Study. Urology 2012, 80, 656–660. [Google Scholar] [CrossRef]
- Epstein, J.I.; Feng, Z.; Trock, B.J.; Pierorazio, P.M. Upgrading and Downgrading of Prostate Cancer from Biopsy to Radical Prostatectomy: Incidence and Predictive Factors Using the Modified Gleason Grading System and Factoring in Tertiary Grades. Eur. Urol. 2012, 61, 1019–1024. [Google Scholar] [CrossRef] [Green Version]
- Orosco, R.K.; Tapia, V.J.; Califano, J.A.; Clary, B.; Cohen, E.E.; Kane, C.; Lippman, S.M.; Messer, K.; Molinolo, A.; Murphy, J.D.; et al. Positive Surgical Margins in the 10 Most Common Solid Cancers. Sci. Rep. 2018, 8, 5686. [Google Scholar] [CrossRef] [Green Version]
- Tan, W.S.; Krimphove, M.J.; Cole, A.P.; Marchese, M.; Berg, S.; Lipsitz, S.R.; Löppenberg, B.; Nabi, J.; Abdollah, F.; Choueiri, T.K.; et al. Variation in Positive Surgical Margin Status After Radical Prostatectomy for pT2 Prostate Cancer. Clin. Genitourin. Cancer 2019, 17, e1060–e1068. [Google Scholar] [CrossRef]
- Freedland, S.J.; Kane, C.J.; Amling, C.L.; Aronson, W.J.; Terris, M.K.; Presti, J.C., Jr.; SEARCH Database Study Group. Upgrading and Downgrading of Prostate Needle Biopsy Specimens: Risk Factors and Clinical Implications. Urology 2007, 69, 495–499. [Google Scholar] [CrossRef] [Green Version]
- Ham, W.S.; Chalfin, H.J.; Feng, Z.; Trock, B.J.; Epstein, J.I.; Cheung, C.; Humphreys, E.; Partin, A.W.; Han, M. The Impact of Downgrading from Biopsy Gleason 7 to Prostatectomy Gleason 6 on Biochemical Recurrence and Prostate Cancer Specific Mortality. J. Urol. 2017, 197, 1060–1067. [Google Scholar] [CrossRef]
- Freedland, S.J.; Humphreys, E.B.; Mangold, L.A.; Eisenberger, M.; Dorey, F.J.; Walsh, P.C.; Partin, A.W. Risk of Prostate Cancer-specific Mortality Following Biochemical Recurrence after Radical Prostatectomy. JAMA 2005, 294, 433–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muralidhar, V.; Dinh, K.T.; Mahal, B.A.; Ziehr, D.R.; Chen, Y.W.; Viswanathan, V.B.; Nezolosky, M.D.; Choueiri, T.K.; Hoffman, K.E.; Hu, J.C.; et al. Differential Post-prostatectomy Cancer-specific Survival of Occult T3 vs. Clinical T3 Prostate Cancer: Implications for Managing Patients Upstaged on Prostate Magnetic Resonance Imaging. Urol. Oncol. 2015, 33, 330.e19–330.e25. [Google Scholar] [CrossRef] [PubMed]
- Kovac, E.; Vertosick, E.A.; Sjoberg, D.D.; Vickers, A.J.; Stephenson, A.J. Effects of Pathological Upstaging or Upgrading on Metastasis and Cancer-Specific Mortality in Men with Clinical Low-risk Prostate Cancer. BJU Int. 2018, 122, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Moussa, A.S.; Kattan, M.W.; Berglund, R.; Yu, C.; Fareed, K.; Jones, J.S. A Nomogram for Predicting Upgrading in Patients with Low- and Intermediate-grade Prostate Cancer in the Era of Extended Prostate Sampling. BJU Int. 2010, 105, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Truong, M.; Slezak, J.A.; Lin, C.P.; Iremashvili, V.; Sado, M.; Razmaria, A.A.; Leverson, G.; Soloway, M.S.; Eggener, S.E.; Abel, E.J.; et al. Development and multi-institutional validation of an upgrading risk tool for Gleason 6 prostate cancer. Cancer 2013, 119, 3992–4002. [Google Scholar] [CrossRef] [Green Version]
- Qi, F.; Zhu, K.; Cheng, Y.; Hua, L.; Cheng, G. How to Pick Out the “Unreal” Gleason 3 + 3 Patients: A Nomogram for More Precise Active Surveillance Protocol in Low-Risk Prostate Cancer in a Chinese Population. J. Investig. Surg. 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Stuopelyte, K.; Daniunaite, K.; Bakavicius, A.; Lazutka, J.R.; Jankevicius, F.; Jarmalaite, S. The utility of urine-circulating miRNAs for detection of prostate cancer. Br. J. Cancer 2016, 115, 707–715. [Google Scholar] [CrossRef] [Green Version]
- Daniunaite, K.; Jarmalaite, S.; Kalinauskaite, N.; Petroska, D.; Laurinavicius, A.; Lazutka, J.R.; Jankevicius, F. Prognostic Value of RASSF1 Promoter Methylation in Prostate Cancer. J. Urol. 2014, 192, 1849–1855. [Google Scholar] [CrossRef]
- Moreira-Barbosa, C.; Barros-Silva, D.; Costa-Pinheiro, P.; Torres-Ferreira, J.; Constâncio, V.; Freitas, R.; Oliveira, J.; Antunes, L.; Henrique, R.; Jeronimo, C. Comparing Diagnostic and Prognostic Performance of Two-gene Promoter Methylation Panels in Tissue Biopsies and Urines of Prostate Cancer Patients. Clin. Epigenet. 2018, 10, 132. [Google Scholar] [CrossRef]
- Goel, S.; Shoag, J.E.; Gross, M.D.; Al Awamlh, B.A.; Robinson, B.; Khani, F.; Baltich, R.; Margolis, D.J.; Hu, J.C. Concordance Between Biopsy and Radical Prostatectomy Pathology in the Era of Targeted Biopsy: A Systematic Review and Meta-analysis. Eur. Urol. Oncol. 2019. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | PCa Patients (N = 676) |
|---|---|
| Age at surgery, years | |
| Mean (±SD) | 62.1 (7.8) |
| Preoperative PSA, ng/mLa | |
| Mean (±SD) | 8.2 (7.2) |
| Prostate size, gb | |
| Mean (±SD) | 52.5 (23.3) |
| cISUP grade group, n (%) | |
| 1 | 459 (67.9) |
| 2 | 152 (22.5) |
| 3 | 40 (5.9) |
| 4 | 23 (3.4) |
| 5 | 2 (0.3) |
| pISUP grade group, n (%) | |
| 1 | 312 (46.1) |
| 2 | 284 (42.0) |
| 3 | 58 (8.6) |
| 4 | 8 (1.2) |
| 5 | 14 (2.1) |
| cT stage, n (%) | |
| ≤cT1c | 406 (60.1) |
| cT2a | 7 (1.0) |
| cT2b | 84 (12.4) |
| cT2c | 120 (17.8) |
| cT3a | 50 (7.4) |
| cT3b | 9 (1.3) |
| cT4 | 0 (0.0) |
| pT stage, n (%) | |
| pT2a | 41 (6.1) |
| pT2b | 6 (0.9) |
| pT2c | 448 (66.3) |
| pT3a | 105 (15.5) |
| pT3b | 74 (10.9) |
| pT4 | 2 (0.3) |
| pN stage, n (%) | |
| pN0 | 653 (96.6) |
| pN+ | 23 (3.4) |
| Time from biopsy to RP, daysc | |
| Mean (±SD) | 114.7 (186.5) |
| Variable | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| Odds ratio | 95% CI | P-Value | Odds ratio | 95% CI | P-Value | |
| PSA, ng/mL | 1.10 | (1.07–1.13) | <0.001 | 1.09 | (1.05–1.13) | <0.001 |
| Prostate size, g | 0.99 | (0.99–1.00) | 0.182 | 0.99 | (0.98–1.00) | 0.057 |
| PSM | 3.27 | (2.28–4.69) | <0.001 | 2.29 | (1.55–3.40) | <0.001 |
| Upgrading* | 2.28 | (1.59–3.28) | <0.001 | 1.92 | (1.29–2.86) | 0.001 |
| Upstaging | 2.97 | (2.02–4.37) | <0.001 | 2.14 | (1.39–3.27) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakavičius, A.; Drevinskaitė, M.; Daniūnaitė, K.; Barisienė, M.; Jarmalaitė, S.; Jankevičius, F. The Impact of Prostate Cancer Upgrading and Upstaging on Biochemical Recurrence and Cancer-Specific Survival. Medicina 2020, 56, 61. https://doi.org/10.3390/medicina56020061
Bakavičius A, Drevinskaitė M, Daniūnaitė K, Barisienė M, Jarmalaitė S, Jankevičius F. The Impact of Prostate Cancer Upgrading and Upstaging on Biochemical Recurrence and Cancer-Specific Survival. Medicina. 2020; 56(2):61. https://doi.org/10.3390/medicina56020061
Chicago/Turabian StyleBakavičius, Arnas, Mingailė Drevinskaitė, Kristina Daniūnaitė, Marija Barisienė, Sonata Jarmalaitė, and Feliksas Jankevičius. 2020. "The Impact of Prostate Cancer Upgrading and Upstaging on Biochemical Recurrence and Cancer-Specific Survival" Medicina 56, no. 2: 61. https://doi.org/10.3390/medicina56020061