Cervical Lymph Nodes Detected by F-18 FDG PET/CT in Oncology Patients: Added Value of Subsequent Ultrasonography for Determining Nodal Metastasis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Populations
2.2. Imaging Techniques of PET/CT and US
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
3.1. Study Population
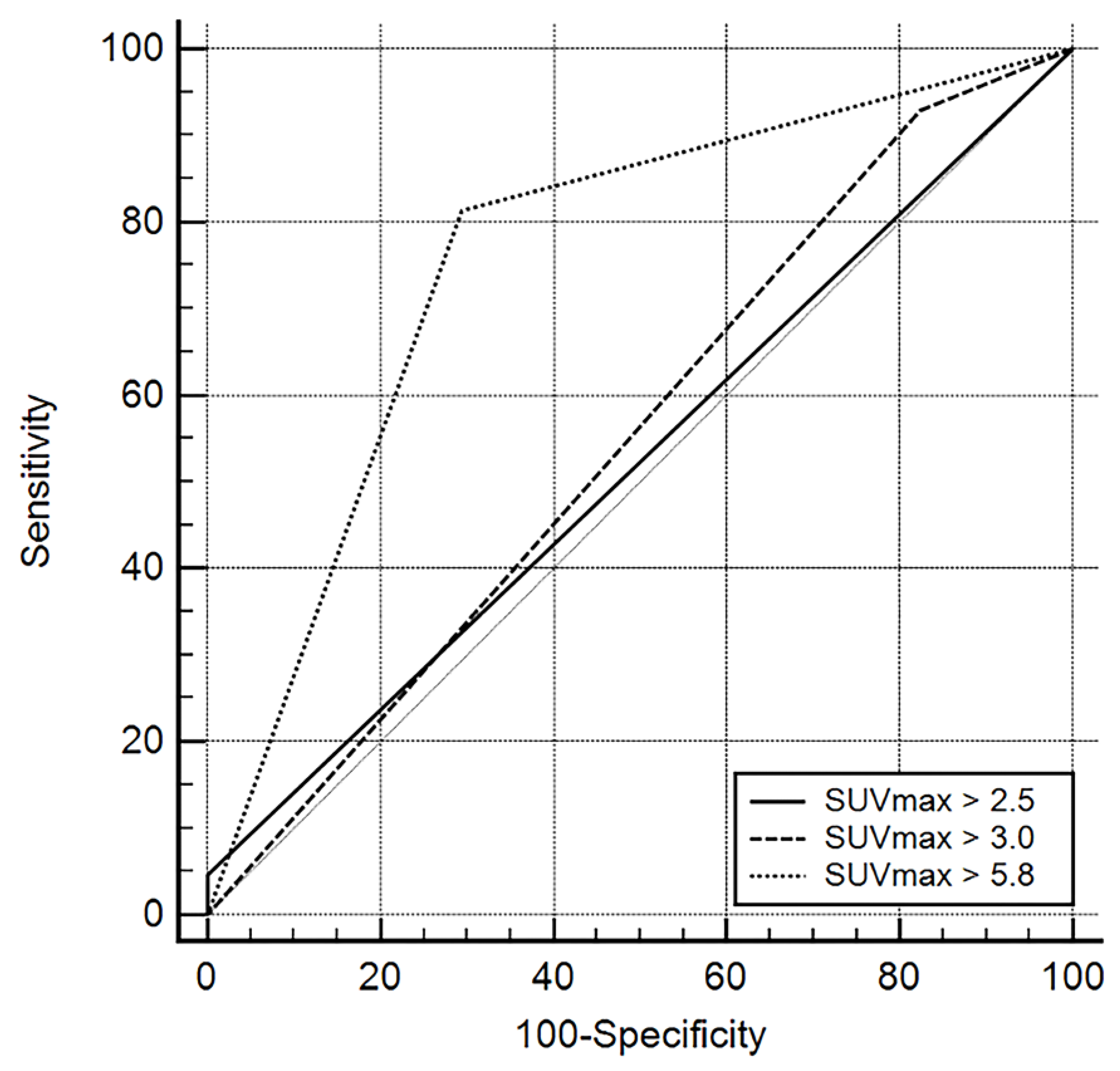
3.2. PET/CT Findings
3.3. Subsequent US Findings
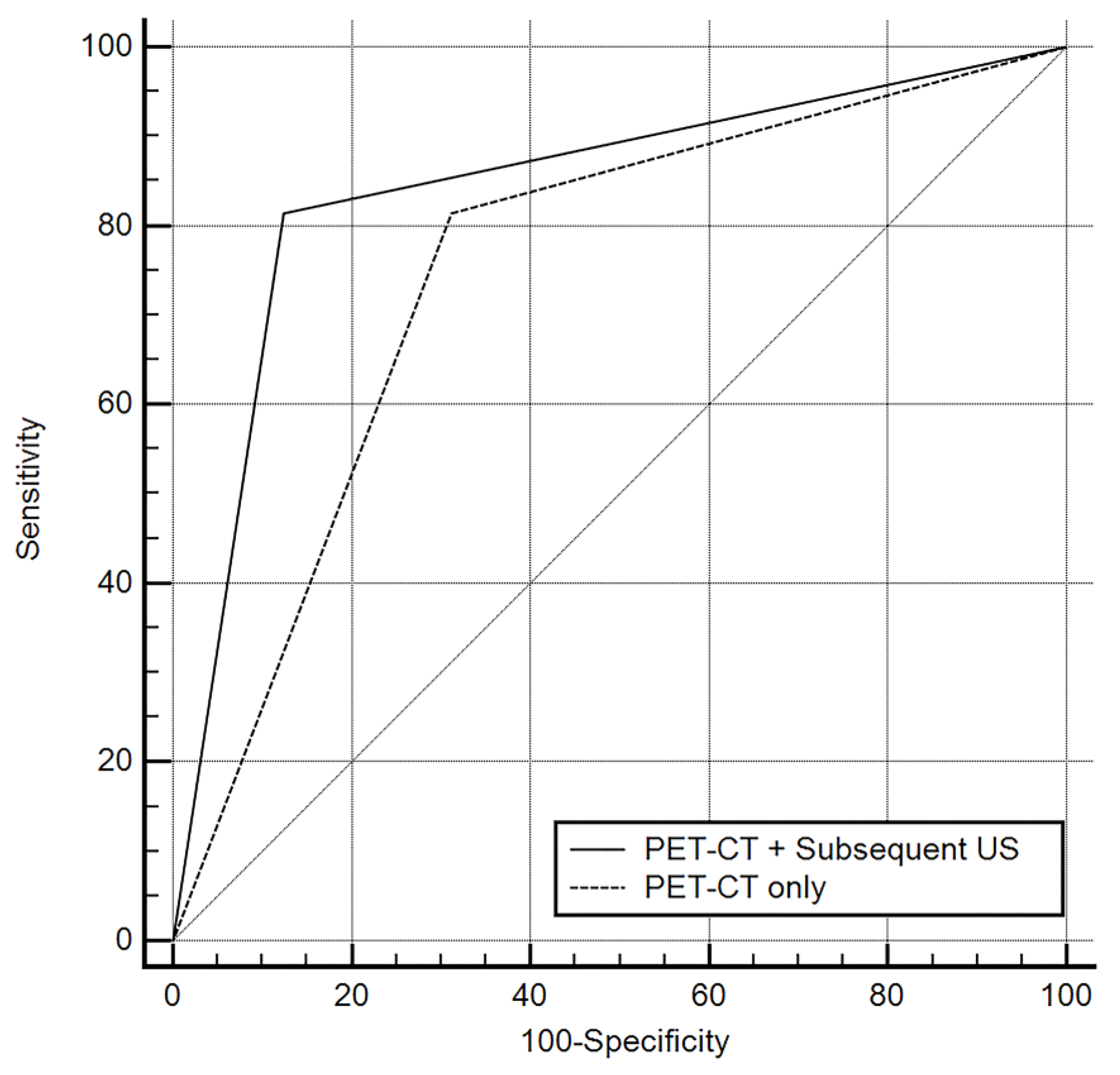
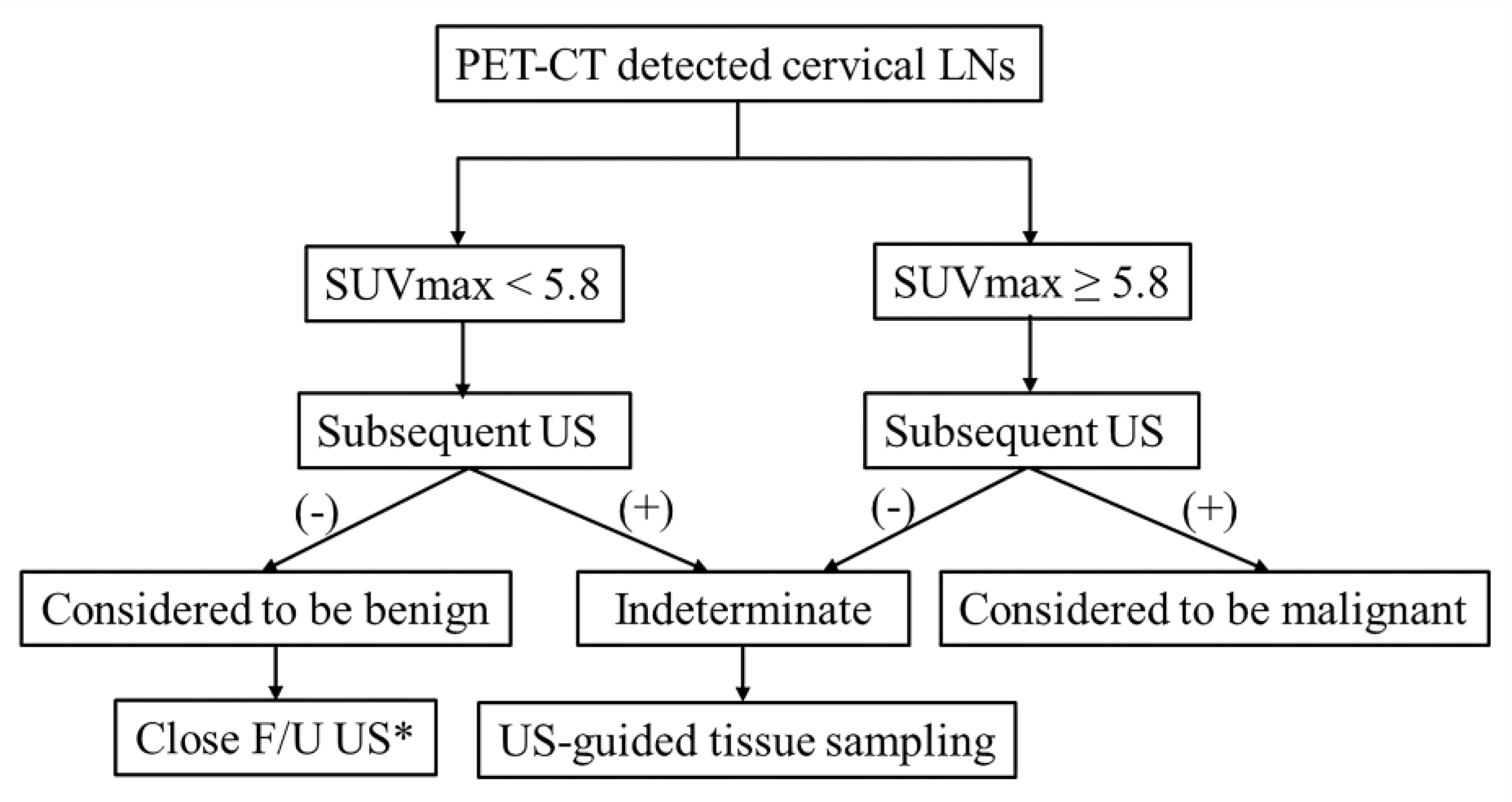
3.4. Combined Diagnosis Using Subsequent US Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual; Springer: New York, NY, USA, 2017. [Google Scholar]
- Murakami, R.; Uozumi, H.; Hirai, T.; Nishimura, R.; Shiraishi, S.; Ota, K.; Murakami, D.; Tomiguchi, S.; Oya, N.; Katsuragawa, S.; et al. Impact of FDGPET/CT imaging on nodal staging for head-and-neck squamous cell carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 377–382. [Google Scholar] [CrossRef]
- Sung, Y.M.; Lee, K.S.; Kim, B.T.; Kim, S.; Kwon, O.J.; Choi, J.Y.; Yang, S.O. Nonpalpable supraclavicular lymph nodes in lung cancer patients: Preoperative characterization with 18F-FDG PET/CT. AJR. Am. J. Roentgenol. 2008, 190, 246–252. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, J.; Moon, H.J.; Cho, A.; Yun, M.; Lee, J.D.; Kang, W.J. Supraclavicular lymph nodes detected by 18F-FDG PET/CT in cancer patients: Assessment with 18F-FDG PET/CT and sonography. AJR. Am. J. Roentgenol. 2012, 198, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Sohn, B.; Koh, Y.W.; Kang, W.J.; Lee, J.H.; Shin, N.Y.; Kim, J. Is there an additive value of 18 F-FDG PET-CT to CT/MRI for detecting nodal metastasis in oropharyngeal squamous cell carcinoma patients with palpably negative neck? Acta. Radiol. 2016, 57, 1352–1359. [Google Scholar] [CrossRef] [PubMed]
- Yoon, D.Y.; Hwang, H.S.; Chang, S.K.; Rho, Y.S.; Ahn, H.Y.; Kim, J.H.; Lee, I.J. CT, MR, US, 18F-FDG PET/CT, and their combined use for the assessment of cervical lymph node metastases in squamous cell carcinoma of the head and neck. Eur. Radiol. 2009, 19, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Shin, N.Y.; Lee, J.H.; Kang, W.J.; Koh, Y.W.; Sohn, B.; Kim, J. Clinical usefulness of [18F]FDG PET-CT and CT/MRI for detecting nodal metastasis in patients with hypopharyngeal squamous cell carcinoma. Ann. Surg. Oncol. 2015, 22, 994–999. [Google Scholar] [CrossRef]
- Roh, J.L.; Park, J.P.; Kim, J.S.; Lee, J.H.; Cho, K.J.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. 18F Fluorodeoxyglucose PET/CT in Head and Neck Squamous Cell Carcinoma with Negative Neck Palpation Findings: A Prospective Study. Radiology 2014, 271, 153–161. [Google Scholar] [CrossRef] [Green Version]
- Liao, L.J.; Lo, W.C.; Hsu, W.L.; Wang, C.T.; Lai, M.S. Detection of cervical lymph node metastasis in head and neck cancer patients with clinically N0 neck-a meta-analysis comparing different imaging modalities. BMC Cancer 2012, 12, 236. [Google Scholar] [CrossRef]
- Bae, M.R.; Roh, J.L.; Kim, J.S.; Lee, J.H.; Cho, K.J.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. 18F-FDG PET/CT versus CT/MR imaging for detection of neck lymph node metastasis in palpably node-negative oral cavity cancer. J. Cancer Res. Clin. Oncol. 2019. [Google Scholar] [CrossRef]
- Peltenburg, B.; de Keizer, B.; Dankbaar, J.W.; de Boer, M.; Willems, S.M.; Philippens, M.E.P.; Terhaard, C.H.J.; de Bree, R. Prediction of ultrasound guided fine needle aspiration cytology results by FDG PET-CT for lymph node metastases in head and neck squamous cell carcinoma patients. Acta Oncol. 2018, 57, 1687–1692. [Google Scholar] [CrossRef]
- Liao, L.J.; Wang, C.T.; Young, Y.H.; Cheng, P.W. Real-time and computerized sonographic scoring system for predicting malignant cervical lymphadenopathy. Head. Neck. 2010, 32, 594–598. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Rahman, K.; Shahid, M.; Kumar, A.; Qaseem, S.M.; Hassan, S.A. Sonographic assessment of cervical lymphadenopathy: Role of high-resolution and color Doppler imaging. Head. Neck. 2011, 33, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Chikui, T.; Yonetsu, K.; Nakamura, T. Multivariate feature analysis of sonographic findings of metastatic cervical lymph nodes: Contribution of blood flow features revealed by power Doppler sonography for predicting metastasis. AJNR. Am. J. Neuroradiol. 2000, 21, 561–567. [Google Scholar] [PubMed]
- Wu, M.; Chen, H.; Zheng, X.; Burstein, D.E. Evaluation of a scoring system for predicting lymph node malignancy in ultrasound guided fine needle aspiration practice. Diagn. Cytopathol. 2013, 41, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Rege, S.; Maass, A.; Chaiken, L.; Hoh, C.K.; Choi, Y.; Lufkin, R.; Anzai, Y.; Juillard, G.; Maddahi, J.; Phelps, M.E. Use of positron emission tomography with fluorodeoxyglucose in patients with extracranial head and neck cancers. Cancer 1994, 73, 3047–3058. [Google Scholar] [CrossRef]
- Haberkorn, U.; Strauss, L.G.; Reisser, C.; Haag, D.; Dimitrakopoulou, A.; Ziegler, S.; Oberdorfer, F.; Rudat, V.; van Kaick, G. Glucose uptake, perfusion, and cell proliferation in head and neck tumors: Relation of positron emission tomography to flow cytometry. J. Nucl. Med. 1991, 32, 1548–1555. [Google Scholar]
- Braams, J.W.; Pruim, J.; Freling, N.J.; Nikkels, P.G.; Roodenburg, J.L.; Boering, G.; Vaalburg, W.; Vermey, A. Detection of lymph node metastases of squamous-cell cancer of the head and neck with FDG-PET and MRI. J. Nucl. Med. 1995, 36, 211–216. [Google Scholar]
- Kau, R.J.; Alexiou, C.; Laubenbacher, C.; Werner, M.; Schwaiger, M.; Arnold, W. Lymph node detection of head and neck squamous cell carcinomas by positron emission tomography with fluorodeoxyglucose F 18 in a routine clinical setting. Arch. Otolaryngol. Head. Neck. Surg. 1999, 125, 1322–1328. [Google Scholar] [CrossRef] [Green Version]
- Purohit, B.S.; Ailianou, A.; Dulguerov, N.; Becker, C.D.; Ratib, O.; Becker, M. FDG-PET/CT pitfalls in oncological head and neck imaging. Insights Imaging 2014, 5, 585–602. [Google Scholar] [CrossRef]
- Laubenbacher, C.; Saumweber, D.; Wagner-Manslau, C.; Kau, R.J.; Herz, M.; Avril, N.; Ziegler, S.; Kruschke, C.; Arnold, W.; Schwaiger, M. Comparison of fluorine-18-fluorodeoxyglucose PET, MRI and endoscopy for staging head and neck squamous-cell carcinomas. J. Nucl. Med. 1995, 36, 1747–1757. [Google Scholar] [PubMed]
- Kitajima, K.; Suenaga, Y.; Minamikawa, T.; Komori, T.; Otsuki, N.; Nibu, K.; Sasaki, R.; Itoh, T.; Sugimura, K. Clinical significance of SUVmax in (18)F-FDG PET/CT scan for detecting nodal metastases in patients with oral squamous cell carcinoma. Springerplus 2015, 4, 718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Çaylaklı, F.; Yılmaz, S.; Özer, C.; Reyhan, M. The Role of PET-CT in Evaluation of Cervical Lymph Node Metastases in Oral Cavity Squamous Cell Carcinomas. Turk. Arch. Otorhinolaryngol. 2015, 53, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Xia, X.; Qin, C.; Sun, X.; Zhang, Y.; Lan, X. Is SUVmax Helpful in the Differential Diagnosis of Enlarged Mediastinal Lymph Nodes? A Pilot Study. Contrast Media Mol. Imaging 2018, 28. [Google Scholar] [CrossRef] [Green Version]
- Goense, L.; Meziani, J.; van Rossum, P.S.N.; Wessels, F.J.; Lam, M.G.E.H.; van Hillegersberg, R.; Ruurda, J.P. Cervical ultrasonography has no additional value over negative 18F-FDG PET/CT scans for diagnosing cervical lymph node metastases in patients with esophageal cancer. Eur. Radiol. 2018, 28, 2031–2037. [Google Scholar] [CrossRef] [Green Version]
- Tachibana, M.; Dhar, D.K.; Kinugasa, S.; Kotoh, T.; Shibakita, M.; Ohno, S.; Masunaga, R.; Kubota, H.; Nagasue, N. Esophageal cancer with distant lymph node metastasis: Prognostic significance of metastatic lymph node ratio. J. Clin. Gastroenterol. 2000, 31, 318–322. [Google Scholar] [CrossRef]
- Allin, D.; David, S.; Jacob, A.; Mir, N.; Giles, A.; Gibbins, N. Use of core biopsy in diagnosing cervical lymphadenopathy: A viable alternative to surgical excisional biopsy of lymph nodes? Ann. R. Coll. Surg. Engl. 2017, 99, 242–244. [Google Scholar] [CrossRef] [Green Version]
- Oh, K.H.; Woo, J.S.; Cho, J.G.; Baek, S.K.; Jung, K.Y.; Kwon, S.Y. Efficacy of ultrasound-guided core needle gun biopsy in diagnosing cervical lymphadenopathy. Eur. Ann. Otorhinolaryngol. Head. Neck. Dis. 2016, 133, 401–404. [Google Scholar] [CrossRef]
- Groneck, L.; Quaas, A.; Hallek, M.; Zander, T.; Weihrauch, M.R. Ultrasound-guided core needle biopsies for workup of lymphadenopathy and lymphoma. Eur. J. Haematol. 2016, 97, 379–386. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Character | Value |
|---|---|
| Sex | |
| Male | 35 (62.5 %) |
| Female | 21 (37.5 %) |
| Age | |
| Mean ± SD | 63 ± 21.1 |
| Range | 32–90 |
| Size (Dmin) | |
| Mean ± SD | 1.1 ± 0.7 |
| Primary tumor sites | |
| Lung cancer | 20 (35.7 %) |
| Laryngeal cancer | 4 (7.1 %) |
| Tongue cancer | 4 (7.1 %) |
| Tonsil cancer | 4 (7.1 %) |
| Gastric cancer | 4 (7.1 %) |
| Salivary gland cancer | 3 (5.4 %) |
| Hypopharyngeal cancer | 3 (5.4 %) |
| Nasopharyngeal cancer | 2 (3.6 %) |
| Thyroid cancer | 2 (3.6 %) |
| Pancreas cancer | 1 (1.8%) |
| Prostate cancer | 1 (1.8%) |
| Skin cancer | 1 (1.8%) |
| Ureter cancer | 1 (1.8%) |
| Breast cancer | 1 (1.8%) |
| Cholangiocarcinoma | 1 (1.8%) |
| Colon cancer | 1 (1.8%) |
| Esophageal cancer | 1 (1.8%) |
| Myxoinflammatory fibroblastic sarcoma | 1 (1.8%) |
| Malignancy of unknown origin | 1 (1.8%) |
| Imaging Characteristics | % (No. with Positive Findings/Total No.) | |||
|---|---|---|---|---|
| Malignant | Benign | Total | p Value | |
| Increased size (short-axis diameter >0.8 cm) | 65.1 (28/43) | 18.8 (3/16) | 52.5 (31/59) | 0.005 |
| Loss of fatty hilum | 76.7 (33/43) | 18.9 (3/16) | 61.0 (36/59) | <0.001 |
| Hypo-or heterogeneous echogenicity | 95.3 (41/43) | 43.6 (7/16) | 81.4 (48/59) | <0.001 |
| Round shape | 93.0 (40/43) | 56.3 (9/16) | 83.1 (49/59) | 0.008 |
| No. of Suspicious US Finding | % (No. with Positive Findings/Total No.) | ||
|---|---|---|---|
| Malignant | Benign | Total | |
| 0 | 2.3 (1/43) | 37.5 (6/16) | 11.9 (7/59) |
| 1 | 0 (0/43) | 25.0 (4/16) | 6.8 (4/59) |
| 2 | 14.0 (6/43) | 12.5 (2/16) | 13.6 (8/59) |
| 3 | 30.2 (13/43) | 18.6 (3/16) | 27.1 (16/59) |
| 4 | 53.5 (23/43) | 6.3 (1/16) | 40.7 (24/59) |
| Type of Imaging | Imaging Diagnosis | Pathologic Diagnosis | Total (No.) | Sen. (%) | Spe. (%) | PPV (%) | NPV (%) | Accuracy (%) | |
|---|---|---|---|---|---|---|---|---|---|
| Metastasis (No.) | Benign (No.) | ||||||||
| PET-CT (SUVmax≥ 5.8) | Positive (No.) | 35 | 5 | 40 | 81.4 | 68.8 | 87.5 | 57.9 | 78.0 |
| Negative (No.) | 8 | 11 | 19 | ||||||
| Total (No.) | 43 | 16 | |||||||
| PET-CT + subsequent US | Positive (No.) | 35 | 2 | 37 | 81.4 | 87.5 | 94.6 | 63.6 | 83.1 |
| Negative (No.) | 8 | 14 | 22 | ||||||
| Total (No.) | 43 | 16 | |||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, S.; Ryu, K.H.; Baek, H.J.; Kim, T.H.; Moon, J.I.; Choi, B.H.; Park, S.E.; Ha, J.Y.; Song, D.H.; An, H.J.; et al. Cervical Lymph Nodes Detected by F-18 FDG PET/CT in Oncology Patients: Added Value of Subsequent Ultrasonography for Determining Nodal Metastasis. Medicina 2020, 56, 16. https://doi.org/10.3390/medicina56010016
Yoon S, Ryu KH, Baek HJ, Kim TH, Moon JI, Choi BH, Park SE, Ha JY, Song DH, An HJ, et al. Cervical Lymph Nodes Detected by F-18 FDG PET/CT in Oncology Patients: Added Value of Subsequent Ultrasonography for Determining Nodal Metastasis. Medicina. 2020; 56(1):16. https://doi.org/10.3390/medicina56010016
Chicago/Turabian StyleYoon, Seokho, Kyeong Hwa Ryu, Hye Jin Baek, Tae Hoon Kim, Jin Il Moon, Bo Hwa Choi, Sung Eun Park, Ji Young Ha, Dae Hyun Song, Hyo Jung An, and et al. 2020. "Cervical Lymph Nodes Detected by F-18 FDG PET/CT in Oncology Patients: Added Value of Subsequent Ultrasonography for Determining Nodal Metastasis" Medicina 56, no. 1: 16. https://doi.org/10.3390/medicina56010016