1. Introduction
Parkinson’s disease (PD) is a progressive neurological disorder affecting more than 10 million people worldwide [
1] and is the second most common neurodegenerative disease. PD symptoms appear gradually and worsen as disease progresses. Different motor and non-motor symptoms constitute the clinical hallmarks of PD, including bradykinesia, rigidity, tremor, or postural instability as cardinal motor symptoms, and cognitive/behavioral disorders, sleep disturbances, or autonomic alterations as frequent non-motor manifestations. Autonomous nervous system dysfunction symptoms are highly prevalent in PD, being present in up to 80% of cases [
2], and might affect multiple physiological spheres (e.g., gastrointestinal, cardiovascular, urogenital, or thermoregulatory). Autonomic dysfunction imposes a significant burden on people with PD, deeply limiting their health-related quality-of-life [
3].
Autonomous nervous system (dys)function can be assessed by capturing different physiological signals. Skin conductance measures have been traditionally used to evaluate the level of activation of the sympathetic division. To that end, the most used biosignal is electrodermal activity (EDA), which measures the electrical properties of the individual’s skin. Typically, it is recorded as a conductance or a potential signal through placing electrodes in contact with the skin [
4], although recent developments now allow it to be acquired through different sensors. The amplitude of this measurement is strongly related to the autonomous nervous system activity. In the literature, the most expanded uses of this signal are studies linking EDA measurements to anxiety [
5] or stress [
6]. While there are not many studies that make use of these signals in the context of Parkinson’s disease, our recent literature review found that when they are utilized in this disease, they frequently employ a variety of methods without established normative values specific to Parkinson’s disease.
Dopaminergic replacement therapy represents the standard symptomatic treatment for PD. The ON state is the denomination used to designate when the medication is working and symptoms are controlled, while the OFF state defines the time when the medication effect is over or is not working. Fluctuations among ON/OFF states are common as the disease progresses; these fluctuations significantly affect quality-of-life of people with PD [
7]. Its assessment, often in terms of onset, frequency, and severity, is crucial to perform treatment adjustments and, up to now, is usually conducted by relying on self-reported diaries filled in by patients.
The instrumental detection of fluctuations has been proved effective using accelerometers but it is limited to detecting changes in motor symptoms exclusively [
8,
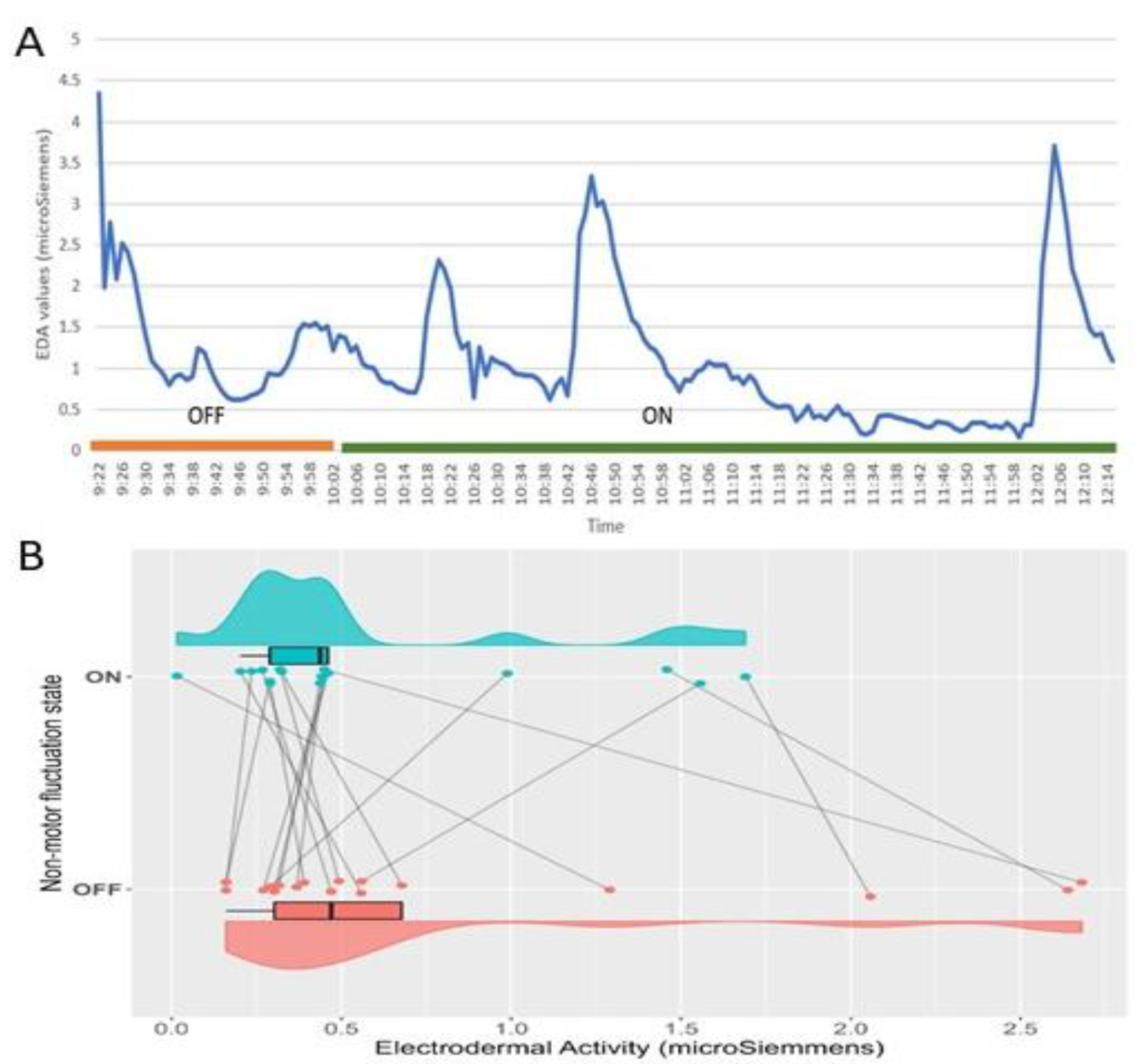
9]; the study of non-motor fluctuations remains notably unexplored. Previous evidence identified differences between the level of sweating (measured as the amplitude of the EDA) in PD patients in ON and OFF states, showing higher levels of EDA in the OFF state [
10]. Moreover, previous studies suggest there might be a relationship between EDA measures and motor fluctuations in PD [
11], but its usefulness to accurately detect their non-motor counterparts remains largely unexamined.
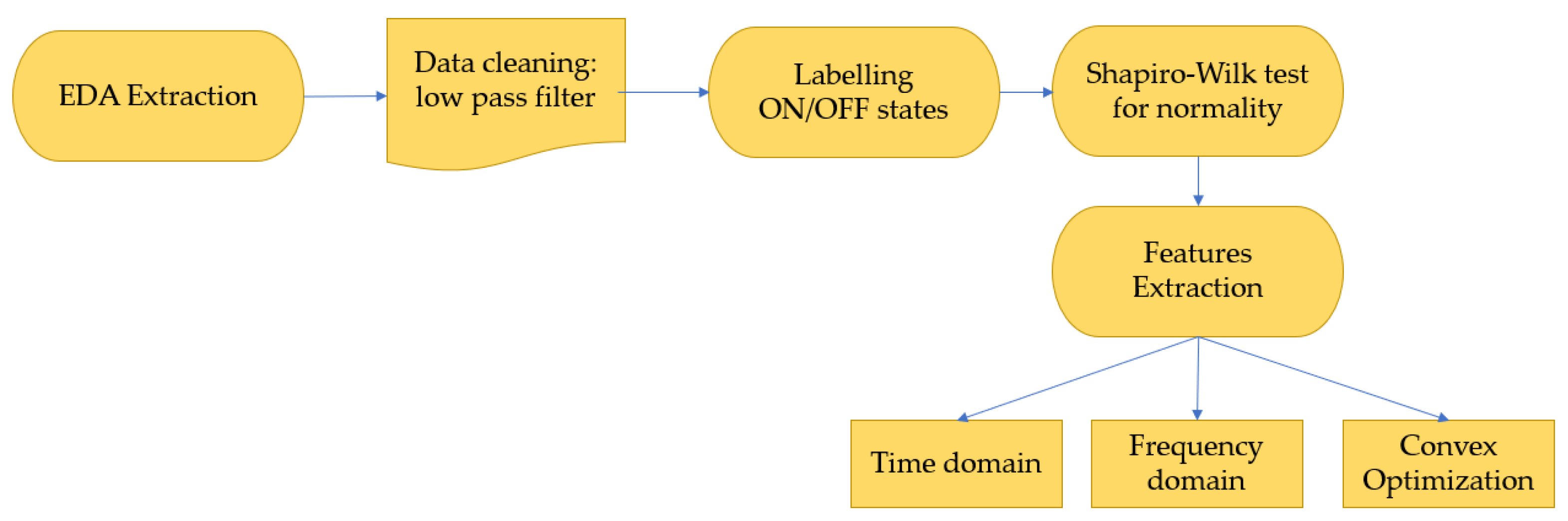
Different methods have been employed to analyze the EDA signal, with the most common approaches occurring in the time and frequency domains. Time domain analyses offer a wealth of information; however, pinpointing specific points, such as the onset of ON/OFF states or peaks, can be challenging due to the presence of noise and other events. [
4,
12]. On the other hand, frequency domain analysis offers fewer details but is generally more robust, sensitive, and simpler to implement [
6]. However, there remains a scarcity of studies utilizing this domain to evaluate the EDA signal in PD. Some studies have employed the tonic and phasic decomposition of the signal to obtain results [
13], and a recent study introduced a new index for evaluating the EDA signal from a stress perspective [
14].
To date, signals from wearable sensors recording autonomic nervous system (ANS) activity, electrodermal activity (EDA), heart rate (HR), blood volume pulse (BVP), and skin temperature (TEMP), have been used in combination to look for markers to detect wearing-off in people on L-dopa [
15].
Machine learning applications, a subset of artificial intelligence, have shown promise in addressing various challenges in medical diagnosis and treatment. In PD, these techniques have been used to analyze spatiotemporal features from different sensors related to motor features detection (e.g., accelerometers or gyroscopes) to identify the patient’s status [
15] by employing methods like Support Vector Machines (SVM), artificial neural networks (ANN), or convolutional neural networks (CNN). There is remarkably scarce evidence regarding the use of these techniques to perform advanced analysis of nervous system (ANS) activity biosignals like EDA.
The objective of this study was to assess the capability of simple and advanced EDA analyses, along with a machine learning algorithm, to detect non-motor fluctuations in individuals with PD.
4. Discussion
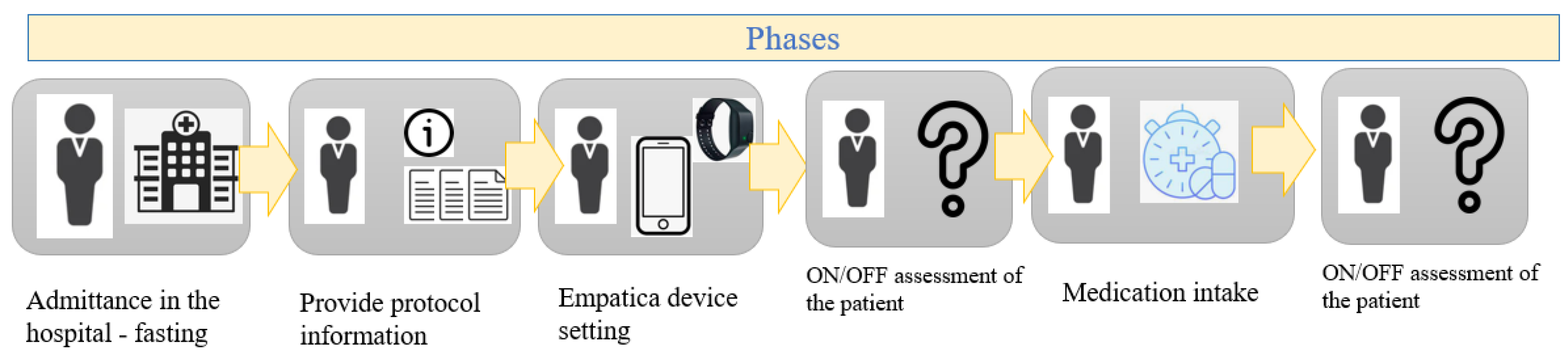
This study evaluated the characteristics of the electrodermal activity in the PD patients in response to dopaminergic medication administration and thus corresponding to the different states known as OFF (without medication) and ON (with medication).
Although there are no normative values for EDA in PD, we have determined that the mean value of the overall EDA signal decreases with dopaminergic activation (1.62 ± 2.56 µS for the OFF period and 1.18 ± 1.7 µS for the ON period). The windowing procedure appears to increase those values but keeps a similar trend (2.16 ± 3.34 µS and 1.36 µS ± 2.4 µS for the OFF and ON states, respectively). We identified differences in the time domain (amplitude mean, amplitude median, SCR number of peaks, and the area under peaks), in the frequency (average power), and in the complex optimization approach (under the peaks for the tonic component) concluding a small effect size between those states. The average mean values for the overall signal and for the windowed signal comparing the ON and OFF states showed a higher arousal activity in the OFF state, as patients without levodopa drugs are more nervous, more excited, more affected by pain, and, therefore, they tend to sweat more because of a higher sympathetic tone [
10]. Moreover, windowing the signal was useful to extract characteristics about the signal that later allowed us to train different ML models to predict the OFF and ON states.
Using logistic regression as a straightforward analytical approach to detect signal changes resulting from LEDD administration, our model showed a moderate accuracy of 67.01%. This model incorporated the EDA features mentioned earlier, as well as socio-demographic and clinical characteristics. When assessing the socio-demographic and clinical variables, we found that age, Hoehn and Yahr (H&Y) stage, disease duration, LEDD dosage, and UPDRS score were all significant factors in the evaluated model. In our study, we found that the average amplitude of the EDA signal did not show statistical significance. Interestingly, this parameter is considered a crucial measure in various models within the literature for predicting patient status [
25]. This discrepancy might be attributed to the limitations of the logistic regression model, which may fail to capture non-linear relationships between variables or handle complex decision boundaries, especially in cases of multicollinearity. Furthermore, the AuC-ROC score of the model is only 0.603, indicating that for a reliable and accurate discrimination between ON and OFF states, more sophisticated analytical approaches should be employed to enhance predictive capabilities. In the context of discriminating between ON and OFF states, the current model’s performance might be hindered by the intricate and multifaceted nature of Parkinson’s disease dynamics. Employing advanced analytical techniques and machine learning algorithms could potentially unlock hidden patterns and yield higher predictive accuracy.
The application of machine learning techniques is widespread in the medicine and biomedicine fields and its usage in Parkinson patients may allow to identify the complex relationships between the characteristics of the patient’s data. The usage of the SVM algorithm to evaluate the EDA signal has been previously reported [
25] to detect stress conditions in individuals or to identify boredom, pain, or surprised emotions [
26] providing very good results. Moreover, the utilization of neural network to evaluate the EDA in patients was studied previously in order to identify the arousal status with very promising results [
27].
The first ML model proposed, a SVM model was tested with different kernel configuration to extend the potential relationship between the data. The results provided promising metrics to identify the fluctuations in Parkinson patients, achieving an accuracy of 72% using a radial based function in the kernel of the SVM. The radial based function of the SVM model provides the best results of the different configurations tested. This function is powerful and more complex than the linear and polynomial ones as its main property is the capacity of combining different polynomial kernels several times looking for non-linear separable data [
28]. This type of kernel is likely more suitable for these signals, given the presence of non-linear relationships among the utilized features that can be effectively captured by this type of kernel function [
29]. In the literature, this function is among the most commonly employed when working with SVM methods for arousal classification [
30]. Consequently, our study demonstrates that SVM methods can effectively identify autonomic changes in response to levodopa intake in PD patients, producing promising results. Both techniques employed a cross-validation mechanism to assess the model’s generalization performance on an independent dataset [
31]. This process involves creating various subsets from the training data to detect any potential overfitting in the model.
The results presented above demonstrate the robustness of the Support Vector Machine (SVM) in accurately identifying the state of the patient (ON or OFF). The literature has already established that SVM-based models exhibit strong robustness and precision compared to other classifiers [
32]. This study not only validates the effectiveness of SVM using the EDA signal to identify stress levels [
25] and emotional arousal [
26], but also to determine the fluctuation state of PD patients.
However, there is room for improvement in terms of enhancing the performance of the designed models. Various configurations of neural networks were explored to assess their capacity to detect the fluctuation states in PD patients.
The results obtained from the artificial and spiking configurations of the neuronal networks demonstrated a very solid performance. This indicates that these neural network models effectively captured the complex relationships among input features, thereby improving upon models like logistic regression that fail to capture the non-linear patterns in the data. The primary distinction between the two models is that, despite our dataset’s limitations, spiking neural networks offer an efficient approach to conserving energy and reducing computational costs, as opposed to traditional neural networks [
33].
Both neural network approaches presented here are viable options for deploying an application with embedded machine learning algorithms aimed at identifying the status of the patient. This would allow for medication adjustments based on the patient’s state, ultimately leading to an enhanced quality of life.
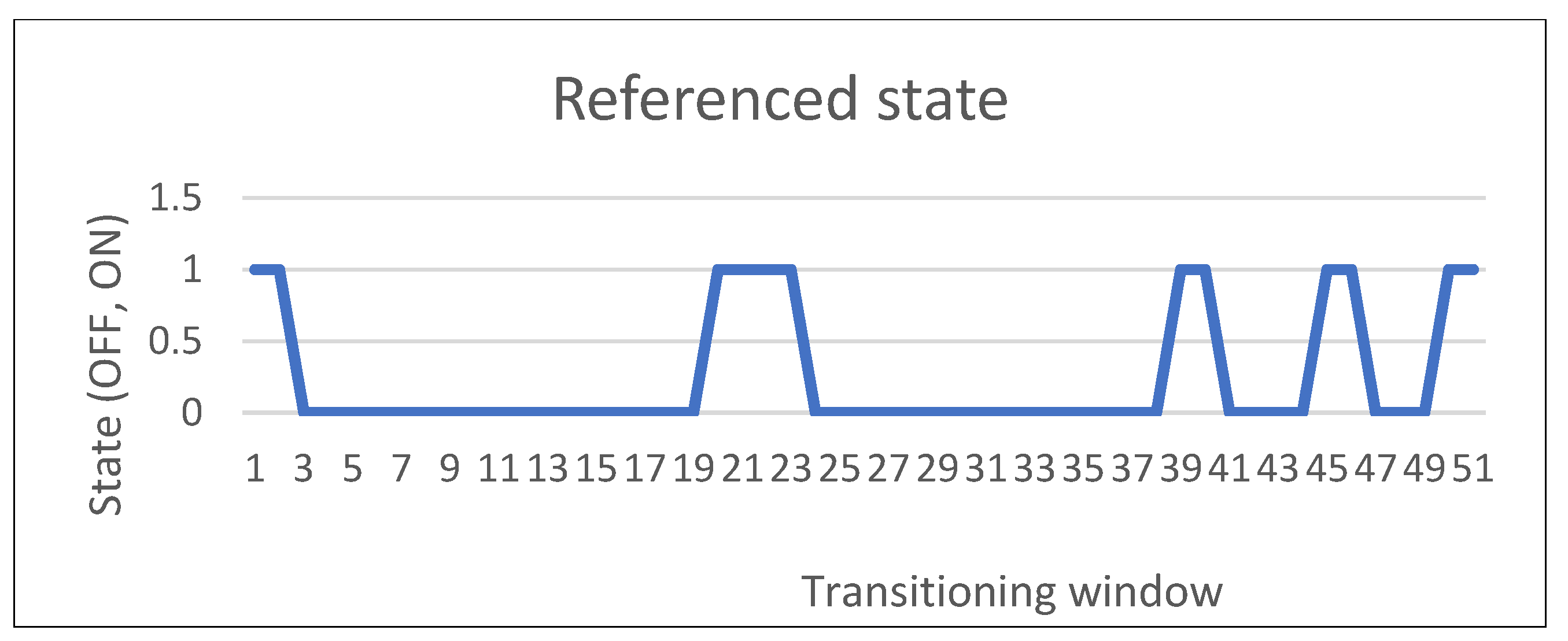
The transition between the OFF and ON state, called in our study the intermediate state, was also evaluated using the information gathered from the PD patients and the ANN with the best performance obtained in the model construction. The results showed that the transition between both states is not a sudden change but a smooth transition from one to another, clearly conditioned to the levodopa pharmacokinetics and absorption [
34].
EDA serves as a potential biomarker for Parkinson’s disease (PD), facilitating the detection of changes in dopaminergic stimulation. Depending on the choice of features and the design of the model, the patient’s condition can be assessed with greater precision. To explore this potential, we constructed a neural network-based model utilizing these features to enhance its performance.
Our proposed approach harnesses the power of a single non-invasive device, such as Empatica, to capture EDA data. This approach distinguishes itself from other contemporary analysis techniques, described in the literature [
35], which rely on canonical correlation analysis and utilize four biosignals (EDA, temperature, heart rate, and blood pressure volume).
However, it’s important to note that our model’s performance could not be personalized for each individual due to the limited number of patients in our database. Also. the sample of patients recruited for the database created had heterogeneous clinical characteristics (H&Y state, age, LEDD) that could also have conditioned the results obtained in the models. In the future, as the database expands, we envision the potential for individualized models to further optimize performance outcomes.
5. Conclusions
In this study, we examined the analysis of electrodermal activity in Parkinson’s disease (PD) patients and its association with non-motor fluctuations. We investigated the characteristics of electrodermal activity in PD patients during different medication stages, referred to as ‘OFF’ (without medication) and ‘ON’ (with medication), identifying some differences between both conditions.
We employed a logistic model to assess the significance of considered variables, including electrodermal activity features, as well as social, demographic, and clinical factors, in classifying the states of PD patients. Additionally, we constructed SVM and various NN models to identify its power and suitability to discriminate between the OFF and ON states with a good level of accuracy.
While our study utilized a dataset from 19 patients to identify these ‘ON/OFF’ states, future work could benefit from adopting an intra-patient approach, using patient-specific characteristics to train the model, thus enhancing accuracy. Longer recording sessions during ‘OFF’ and ‘ON’ periods could provide valuable data for individualized algorithm training. Additionally, exploring other machine learning techniques such as convolutional neural networks or generative adversarial networks could be considered to assess their performance compared to the classifiers built in this study.
Furthermore, our analysis focused solely on electrodermal activity to discriminate between states, but there is potential to incorporate data from other biosignals, such as heart rate, temperature, or blood volume pulse, as features in the algorithms introduced here, enriching the potential relationships identified between the data.
The potential of combining biosignals with machine learning algorithms for the characterization and treatment of PD fluctuations remains a promising avenue for further development.

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}



