
3D-Printed Barrier Membrane Using Mixture of Polycaprolactone and Beta-Tricalcium Phosphate for Regeneration of Rabbit Calvarial Defects

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Preparation of the PCL and β-TCP Mixture
2.3. Fabrication of the PCL/β-TCP Membrane Using a 3D Printer
2.4. Synthetic Bone Graft Material
2.5. Study Design
- Sham control group;
- PCL/β-TCP membrane group (PCL group): the defect was covered using the PCL/β-TCP membrane (10 mm × 10 mm) without bone graft; and
- PCL/β-TCP membrane with synthetic bone graft group (PCL-BG group): the defect was filled with synthetic bone graft material and covered using the PCL/β-TCP membrane.
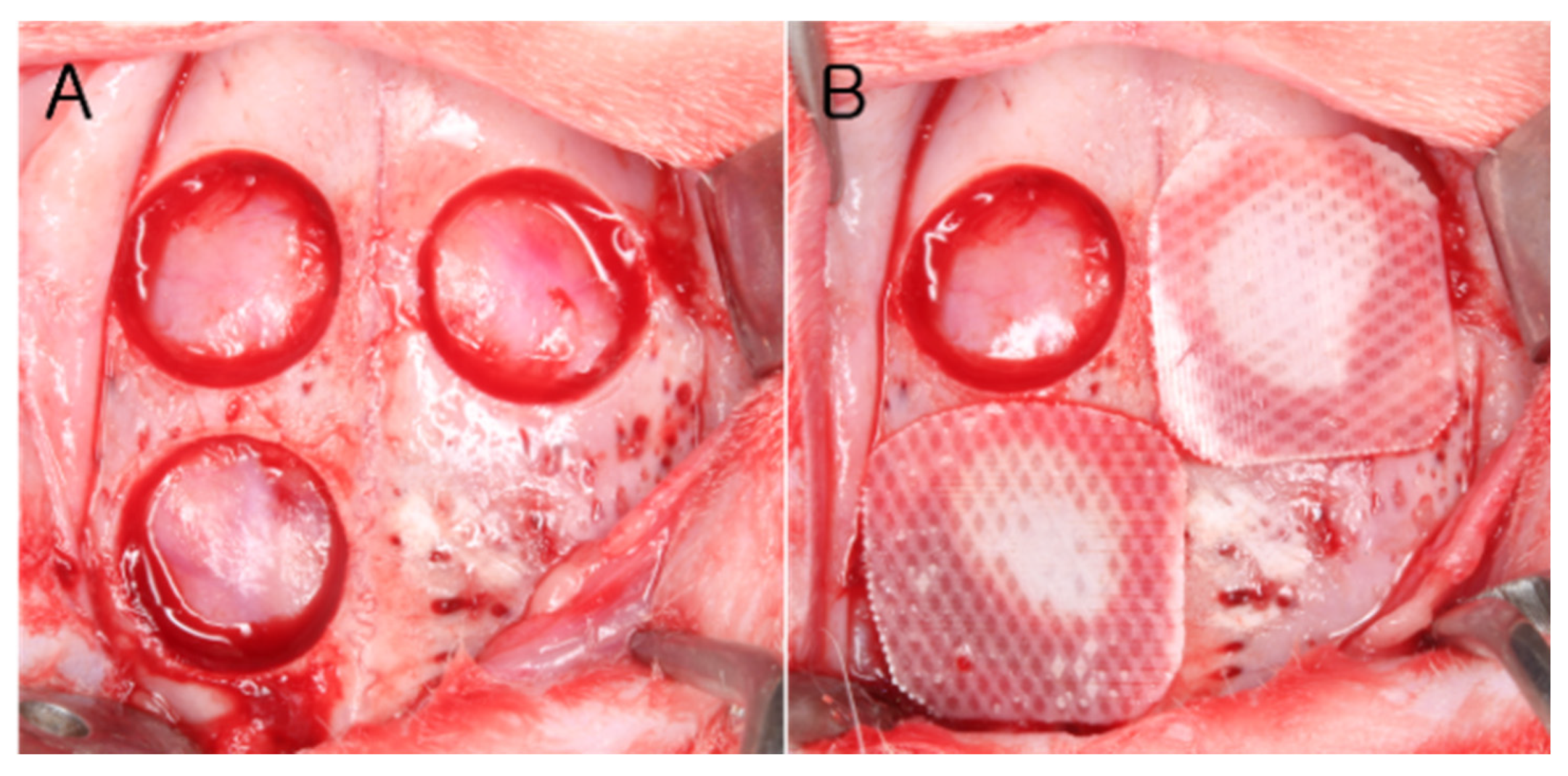
2.6. Surgical Procedure
2.7. Data Analysis
2.7.1. Clinical Observations
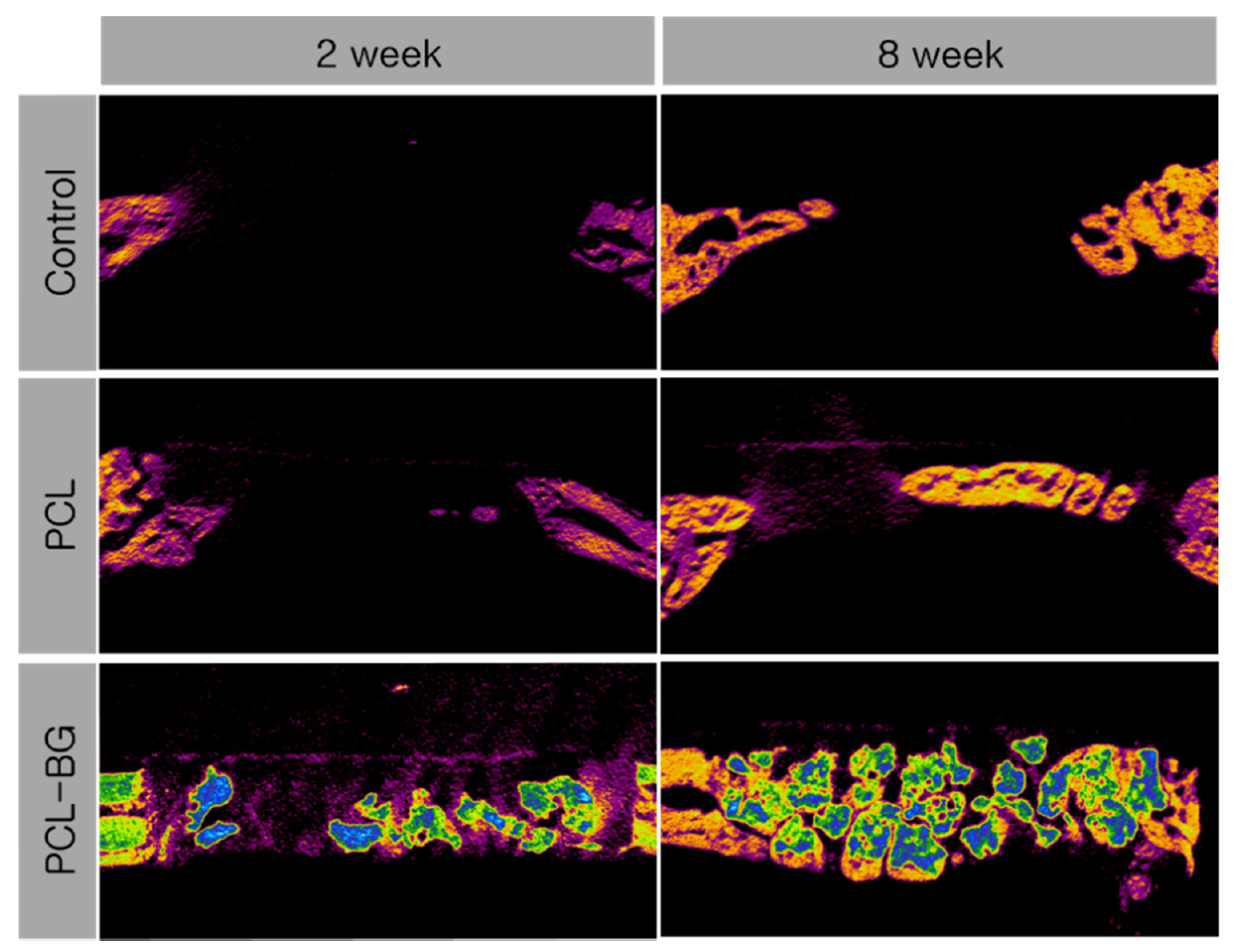
2.7.2. Micro-Computed Tomography (Micro-CT) Analysis
- Total augmented volume (TAV): the volume of the entire grafted materials and regenerated tissue.
- New bone volume (NBV): the volume of newly formed bone.
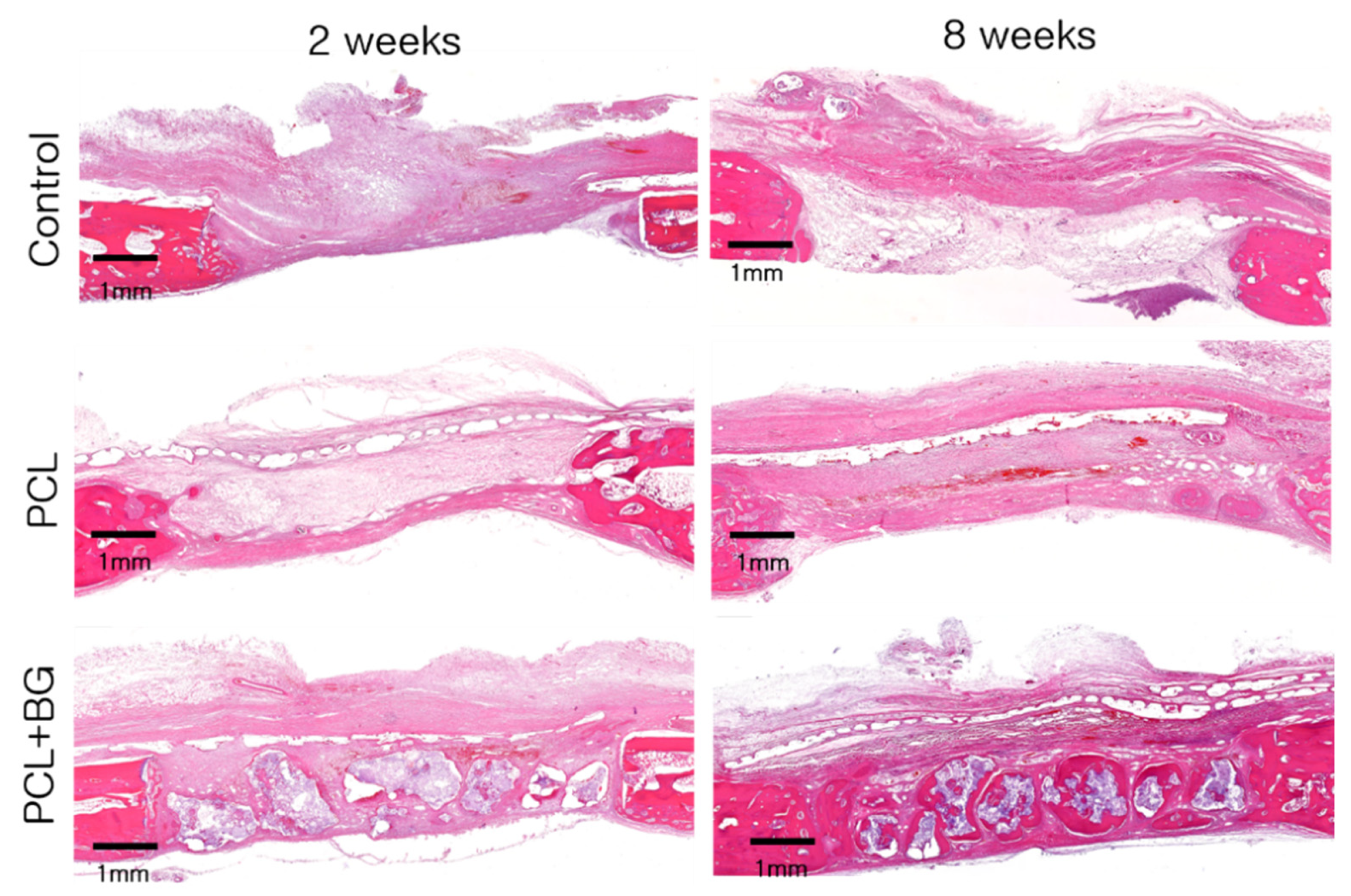
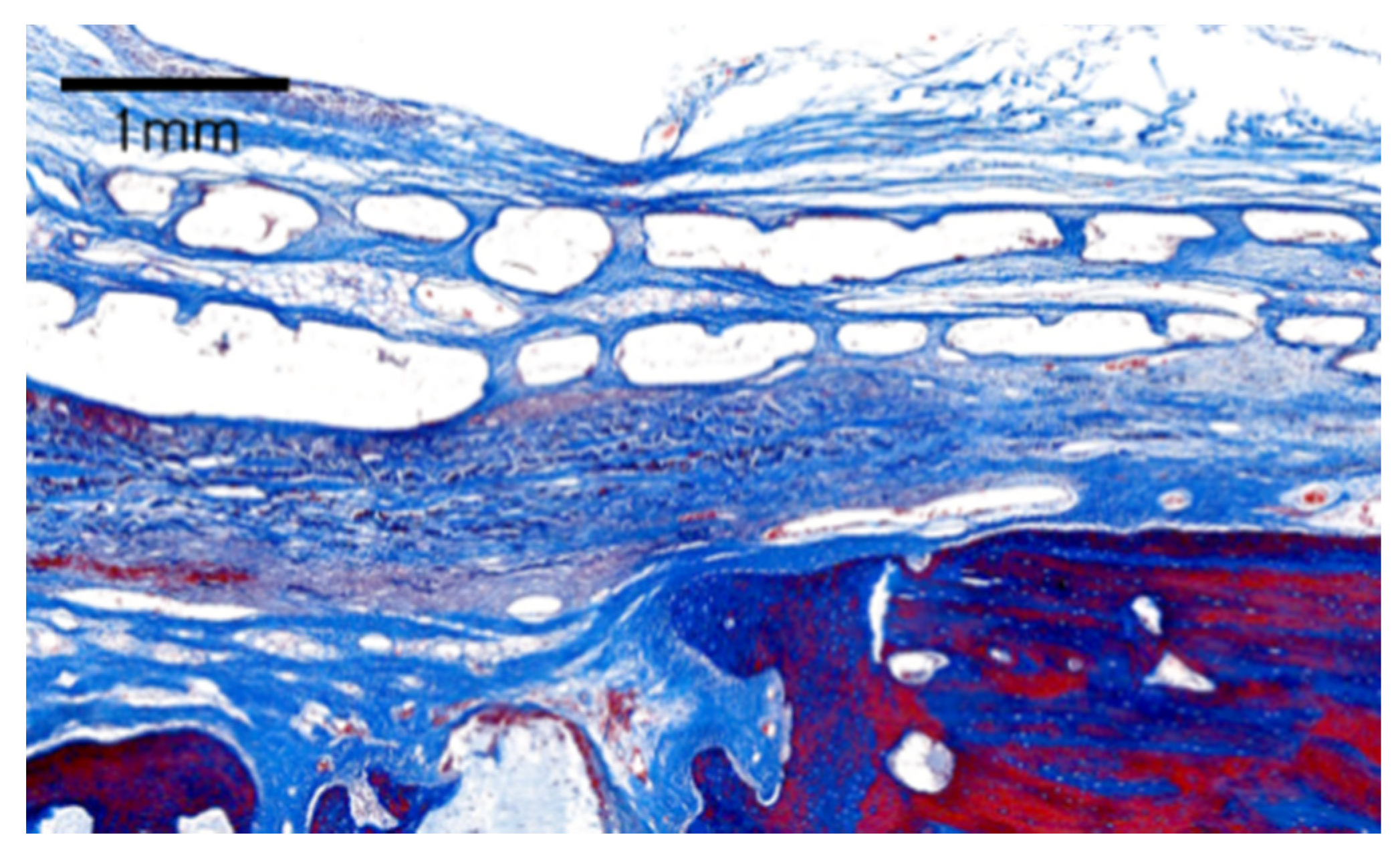
2.7.3. Histologic Analysis
- Total augmented area (TAA): the area of entire augmented tissues consisting of bone substitute, newly formed bone, loose fibrous connective tissue, and adipose tissue.
- New bone area (NBA): the area of newly formed bone, which can be immature woven bone or mature lamellar bone.
2.8. Statistical Analysis
3. Results
3.1. Clinical Observation
3.2. Micro-CT Analysis
3.3. Observational Histology
3.3.1. Control Group
3.3.2. PCL Group
3.3.3. PCL-BG Group
3.4. Histomorphometric Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schenk, R.K.; Buser, D.; Hardwick, W.R.; Dahlin, C. Healing pattern of bone regeneration in membrane-protected defects: A histologic study in the canine mandible. Int. J. Oral Maxillofac. Implants 1994, 9, 13–29. [Google Scholar]
- Park, J.Y.; Jung, I.H.; Kim, Y.K.; Lim, H.C.; Lee, J.S.; Jung, U.W.; Choi, S.H. Guided bone regeneration using 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide (EDC)-cross-linked type-I collagen membrane with biphasic calcium phosphate at rabbit calvarial defects. Biomater. Res. 2015, 19, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz-Sanchez, I.; Ortiz-Vigon, A.; Sanz-Martin, I.; Figuero, E.; Sanz, M. Effectiveness of Lateral Bone Augmentation on the Alveolar Crest Dimension: A Systematic Review and Meta-analysis. J. Dent. Res. 2015, 94, 128S–142S. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Fenner, N.; Hammerle, C.H.; Zitzmann, N.U. Long-term outcome of implants placed with guided bone regeneration (GBR) using resorbable and non-resorbable membranes after 12–14 years. Clin. Oral Implants Res. 2013, 24, 1065–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urban, I.A.; Nagursky, H.; Lozada, J.L.; Nagy, K. Horizontal ridge augmentation with a collagen membrane and a combination of particulated autogenous bone and anorganic bovine bone-derived mineral: A prospective case series in 25 patients. Int. J. Periodontics Restorative Dent. 2013, 33, 299–307. [Google Scholar] [CrossRef] [Green Version]
- Moest, T.; Frabschka, J.; Kesting, M.R.; Schmitt, C.M.; Frohwitter, G.; Lutz, R.; Schlegel, K.A. Osseous ingrowth in allogeneic bone blocks applied for vertical bone augmentation: A preclinical randomised controlled study. Clin. Oral Investig. 2020, 24, 2867–2879. [Google Scholar] [CrossRef]
- Sanchez-Labrador, L.; Molinero-Mourelle, P.; Perez-Gonzalez, F.; Saez-Alcaide, L.M.; Brinkmann, J.C.; Martinez, J.L.; Martinez-Gonzalez, J.M. Clinical performance of alveolar ridge augmentation with xenogeneic bone block grafts versus autogenous bone block grafts. A systematic review. J. Stomatol. Oral Maxillofac. Surg. 2021, 122, 293–302. [Google Scholar] [CrossRef]
- Ye, G.; Bao, F.; Zhang, X.; Song, Z.; Liao, Y.; Fei, Y.; Bunpetch, V.; Heng, B.C.; Shen, W.; Liu, H.; et al. Nanomaterial-based scaffolds for bone tissue engineering and regeneration. Nanomedicine (Lond.) 2020, 15, 1995–2017. [Google Scholar] [CrossRef]
- Park, J.Y.; Yang, C.; Jung, I.H.; Lim, H.C.; Lee, J.S.; Jung, U.W.; Seo, Y.K.; Park, J.K.; Choi, S.H. Regeneration of rabbit calvarial defects using cells-implanted nano-hydroxyapatite coated silk scaffolds. Biomater. Res. 2015, 19, 7. [Google Scholar] [CrossRef] [Green Version]
- Xie, Y.; Li, S.; Zhang, T.; Wang, C.; Cai, X. Titanium mesh for bone augmentation in oral implantology: Current application and progress. Int. J. Oral Sci. 2020, 12, 37. [Google Scholar] [CrossRef]
- Barber, H.D.; Lignelli, J.; Smith, B.M.; Bartee, B.K. Using a dense PTFE membrane without primary closure to achieve bone and tissue regeneration. J. Oral Maxillofac. Surg. 2007, 65, 748–752. [Google Scholar] [CrossRef]
- Soldatos, N.K.; Stylianou, P.; Koidou, V.P.; Angelov, N.; Yukna, R.; Romanos, G.E. Limitations and options using resorbable versus nonresorbable membranes for successful guided bone regeneration. Quintessence Int. 2017, 48, 131–147. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.H.; Jeong, J.H.; Won, J.Y.; Bae, J.H.; Ahn, G.; Jeon, H.; Yun, W.S.; Bae, E.B.; Choi, J.W.; Lee, S.H.; et al. Porosity effect of 3D-printed polycaprolactone membranes on calvarial defect model for guided bone regeneration. Biomed. Mater. 2017, 13, 015014. [Google Scholar] [CrossRef]
- Won, J.Y.; Park, C.Y.; Bae, J.H.; Ahn, G.; Kim, C.; Lim, D.H.; Cho, D.W.; Yun, W.S.; Shim, J.H.; Huh, J.B. Evaluation of 3D printed PCL/PLGA/beta-TCP versus collagen membranes for guided bone regeneration in a beagle implant model. Biomed. Mater. 2016, 11, 055013. [Google Scholar] [CrossRef]
- Bruyas, A.; Lou, F.; Stahl, A.M.; Gardner, M.; Maloney, W.; Goodman, S.; Yang, Y.P. Systematic characterization of 3D-printed PCL/beta-TCP scaffolds for biomedical devices and bone tissue engineering: Influence of composition and porosity. J. Mater. Res. 2018, 33, 1948–1959. [Google Scholar] [CrossRef]
- Low, Z.-X.; Chua, Y.T.; Ray, B.M.; Mattia, D.; Metcalfe, I.S.; Patterson, D.A. Perspective on 3D printing of separation membranes and comparison to related unconventional fabrication techniques. J. Membr. Sci. 2017, 523, 596–613. [Google Scholar] [CrossRef] [Green Version]
- Shim, J.H.; Won, J.Y.; Park, J.H.; Bae, J.H.; Ahn, G.; Kim, C.H.; Lim, D.H.; Cho, D.W.; Yun, W.S.; Bae, E.B.; et al. Effects of 3D-Printed Polycaprolactone/beta-Tricalcium Phosphate Membranes on Guided Bone Regeneration. Int. J. Mol. Sci. 2017, 18, 899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bae, J.C.; Lee, J.J.; Shim, J.H.; Park, K.H.; Lee, J.S.; Bae, E.B.; Choi, J.W.; Huh, J.B. Development and Assessment of a 3D-Printed Scaffold with rhBMP-2 for an Implant Surgical Guide Stent and Bone Graft Material: A Pilot Animal Study. Materials (Basel) 2017, 10, 1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, I.; Khalid, A.W.; Pae, H.C.; Song, Y.W.; Cha, J.K.; Lee, J.S.; Paik, J.W.; Choi, S.H. Diverse patterns of bone regeneration in rabbit calvarial defects depending on the type of collagen membrane. J. Periodontal. Implant Sci. 2021, 51, 40–52. [Google Scholar] [CrossRef]
- Sohn, J.Y.; Park, J.C.; Um, Y.J.; Jung, U.W.; Kim, C.S.; Cho, K.S.; Choi, S.H. Spontaneous healing capacity of rabbit cranial defects of various sizes. J. Periodontal Implant Sci. 2010, 40, 180–187. [Google Scholar] [CrossRef] [Green Version]
- Elgali, I.; Omar, O.; Dahlin, C.; Thomsen, P. Guided bone regeneration: Materials and biological mechanisms revisited. Eur. J. Oral Sci. 2017, 125, 315–337. [Google Scholar] [CrossRef]
- Urban, I.A.; Monje, A.; Lozada, J.L.; Wang, H.L. Long-term Evaluation of Peri-implant Bone Level after Reconstruction of Severely Atrophic Edentulous Maxilla via Vertical and Horizontal Guided Bone Regeneration in Combination with Sinus Augmentation: A Case Series with 1 to 15 Years of Loading. Clin. Implant Dent. Relat. Res. 2017, 19, 46–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maiorana, C.; Beretta, M.; Salina, S.; Santoro, F. Reduction of autogenous bone graft resorption by means of bio-oss coverage: A prospective study. Int. J. Periodontics Restorative Dent. 2005, 25, 19–25. [Google Scholar]
- Lee, J.S.; Cha, J.K.; Thoma, D.S.; Jung, U.W. Report of a human autopsy case in maxillary sinuses augmented using a synthetic bone substitute: Micro-computed tomographic and histologic observations. Clin. Oral Implants Res. 2018, 29, 339–345. [Google Scholar] [CrossRef]
- Lee, S.; Choi, D.; Shim, J.H.; Nam, W. Efficacy of three-dimensionally printed polycaprolactone/beta tricalcium phosphate scaffold on mandibular reconstruction. Sci. Rep. 2020, 10, 4979. [Google Scholar] [CrossRef]
- Bohner, M.; Santoni, B.L.G.; Dobelin, N. beta-tricalcium phosphate for bone substitution: Synthesis and properties. Acta Biomater. 2020, 113, 23–41. [Google Scholar] [CrossRef]
- Turri, A.; Cirgic, E.; Shah, F.A.; Hoffman, M.; Omar, O.; Dahlin, C.; Trobos, M. Early plaque formation on PTFE membranes with expanded or dense surface structures applied in the oral cavity of human volunteers. Clin. Exp. Dent. Res. 2021, 7, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Atef, M.; Tarek, A.; Shaheen, M.; Alarawi, R.M.; Askar, N. Horizontal ridge augmentation using native collagen membrane vs titanium mesh in atrophic maxillary ridges: Randomized clinical trial. Clin. Implant. Dent. Relat. Res. 2020, 22, 156–166. [Google Scholar] [CrossRef]
- Sun, H.; Mei, L.; Song, C.; Cui, X.; Wang, P. The in vivo degradation, absorption and excretion of PCL-based implant. Biomaterials 2006, 27, 1735–1740. [Google Scholar] [CrossRef] [PubMed]
- Hong, I.; Khalid, A.W.; Pae, H.C.; Cha, J.K.; Lee, J.S.; Paik, J.W.; Jung, U.W.; Choi, S.H. Distinctive bone regeneration of calvarial defects using biphasic calcium phosphate supplemented ultraviolet-crosslinked collagen membrane. J. Periodontal Implant Sci. 2020, 50, 14–27. [Google Scholar] [CrossRef] [PubMed]
- Sbricoli, L.; Guazzo, R.; Annunziata, M.; Gobbato, L.; Bressan, E.; Nastri, L. Selection of Collagen Membranes for Bone Regeneration: A Literature Review. Materials (Basel) 2020, 13, 786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunyaratavej, P.; Wang, H.L. Collagen membranes: A review. J. Periodontol. 2001, 72, 215–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.A.; Lee, H.J.; Kim, S.Y.; Kim, K.S.; Jo, D.W.; Park, S.Y. Three-dimensionally printed polycaprolactone/beta-tricalcium phosphate scaffold was more effective as an rhBMP-2 carrier for new bone formation than polycaprolactone alone. J. Biomed. Mater. Res. A 2021, 109, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Pae, H.C.; Kang, J.H.; Cha, J.K.; Lee, J.S.; Paik, J.W.; Jung, U.W.; Kim, B.H.; Choi, S.H. 3D-printed polycaprolactone scaffold mixed with beta-tricalcium phosphate as a bone regenerative material in rabbit calvarial defects. J. Biomed. Mater. Res. B Appl. Biomater. 2019, 107, 1254–1263. [Google Scholar] [CrossRef]
- Huang, S.H.; Hsu, T.T.; Huang, T.H.; Lin, C.Y.; Shie, M.Y. Fabrication and characterization of polycaprolactone and tricalcium phosphate composites for tissue engineering applications. J. Dent. Sci. 2017, 12, 33–43. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healing Period | Study Group | Total Augmented Volume (TAV) | New Bone Volume (NBV) |
|---|---|---|---|
| 2 weeks | CONTROL | 3.13 ± 2.13 | 2.94 ± 2.04 |
| PCL | 3.34 ± 1.88 | 3.22 ± 1.94 | |
| PCL-BG | 28.94 ± 8.15 *,# | 16.14 ± 8.38 *,# | |
| 8 weeks | CONTROL | 10.89 ± 11.77 | 10.42 ± 11.59 |
| PCL | 20.41 ± 5.75 † | 19.45 ± 5.17 † | |
| PCL-BG | 62.20 ± 21.58 *,# | 33.55 ± 12.08 *,# |
| Healing Period | Study Group | Total Augmented Area (TAA) | New Bone Area (NBA) |
|---|---|---|---|
| 2 weeks | CONTROL | 4.89 ± 2.51 | 0.69 ± 0.27 |
| PCL | 8.12 ± 4.26 | 1.01 ± 0.67 | |
| PCL-BG | 13.09 ± 3.89 * | 0.90 ± 0.22 | |
| 8 weeks | CONTROL | 5.02 ± 2.69 | 0.99 ± 0.64 |
| PCL | 8.13 ± 1.15 | 2.20 ± 1.03 † | |
| PCL-BG | 14.19 ± 3.92 *,# | 2.80 ± 1.55 † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-Y.; Park, J.-Y.; Hong, I.-P.; Jeon, S.-H.; Cha, J.-K.; Paik, J.-W.; Choi, S.-H. 3D-Printed Barrier Membrane Using Mixture of Polycaprolactone and Beta-Tricalcium Phosphate for Regeneration of Rabbit Calvarial Defects. Materials 2021, 14, 3280. https://doi.org/10.3390/ma14123280
Lee J-Y, Park J-Y, Hong I-P, Jeon S-H, Cha J-K, Paik J-W, Choi S-H. 3D-Printed Barrier Membrane Using Mixture of Polycaprolactone and Beta-Tricalcium Phosphate for Regeneration of Rabbit Calvarial Defects. Materials. 2021; 14(12):3280. https://doi.org/10.3390/ma14123280
Chicago/Turabian StyleLee, Jun-Young, Jin-Young Park, In-Pyo Hong, Su-Hee Jeon, Jae-Kook Cha, Jeong-Won Paik, and Seong-Ho Choi. 2021. "3D-Printed Barrier Membrane Using Mixture of Polycaprolactone and Beta-Tricalcium Phosphate for Regeneration of Rabbit Calvarial Defects" Materials 14, no. 12: 3280. https://doi.org/10.3390/ma14123280