In Vivo Study for Clinical Application of Dental Stem Cell Therapy Incorporated with Dental Titanium Implants

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Titanium Surface Preparation
2.2. Cell Preparation
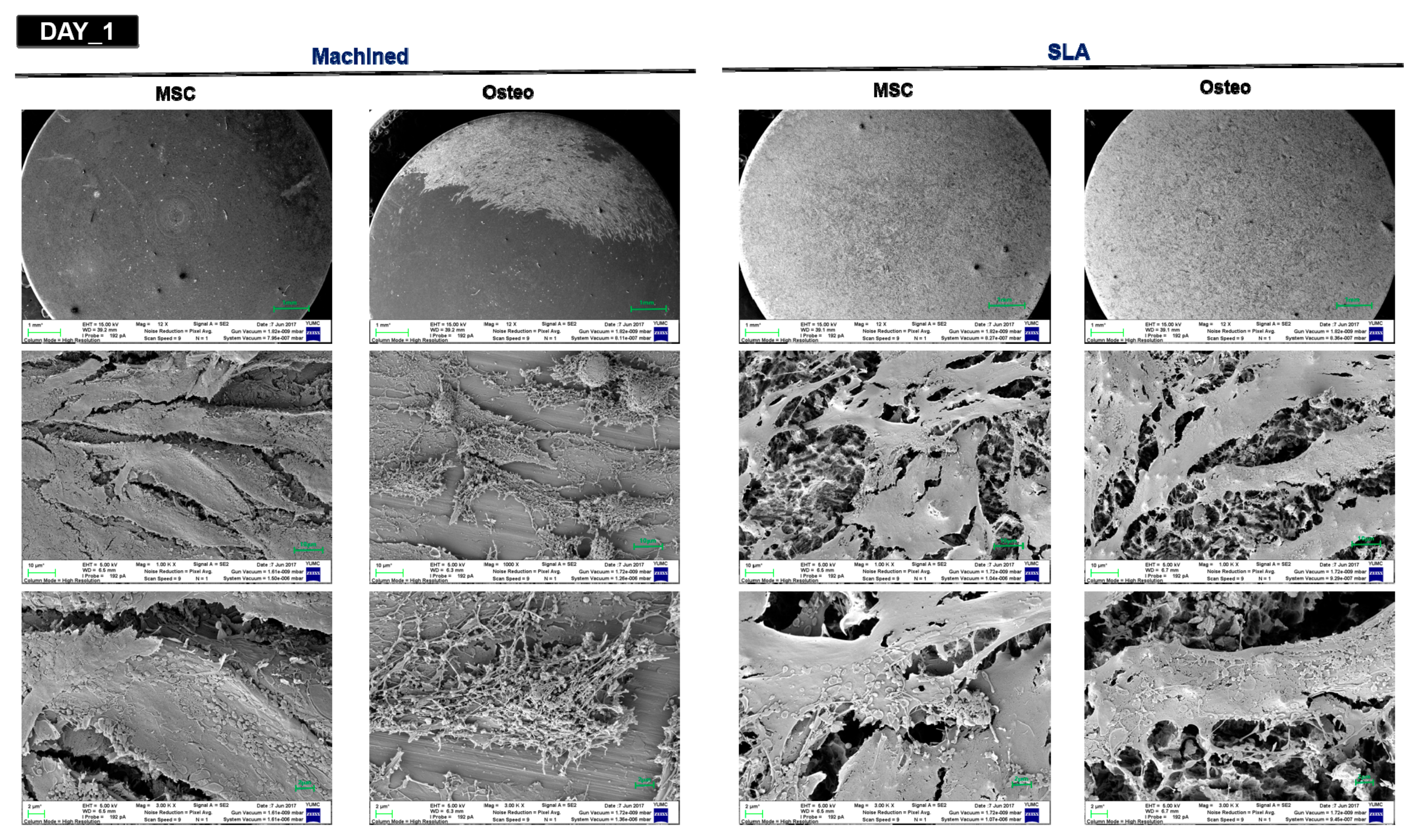
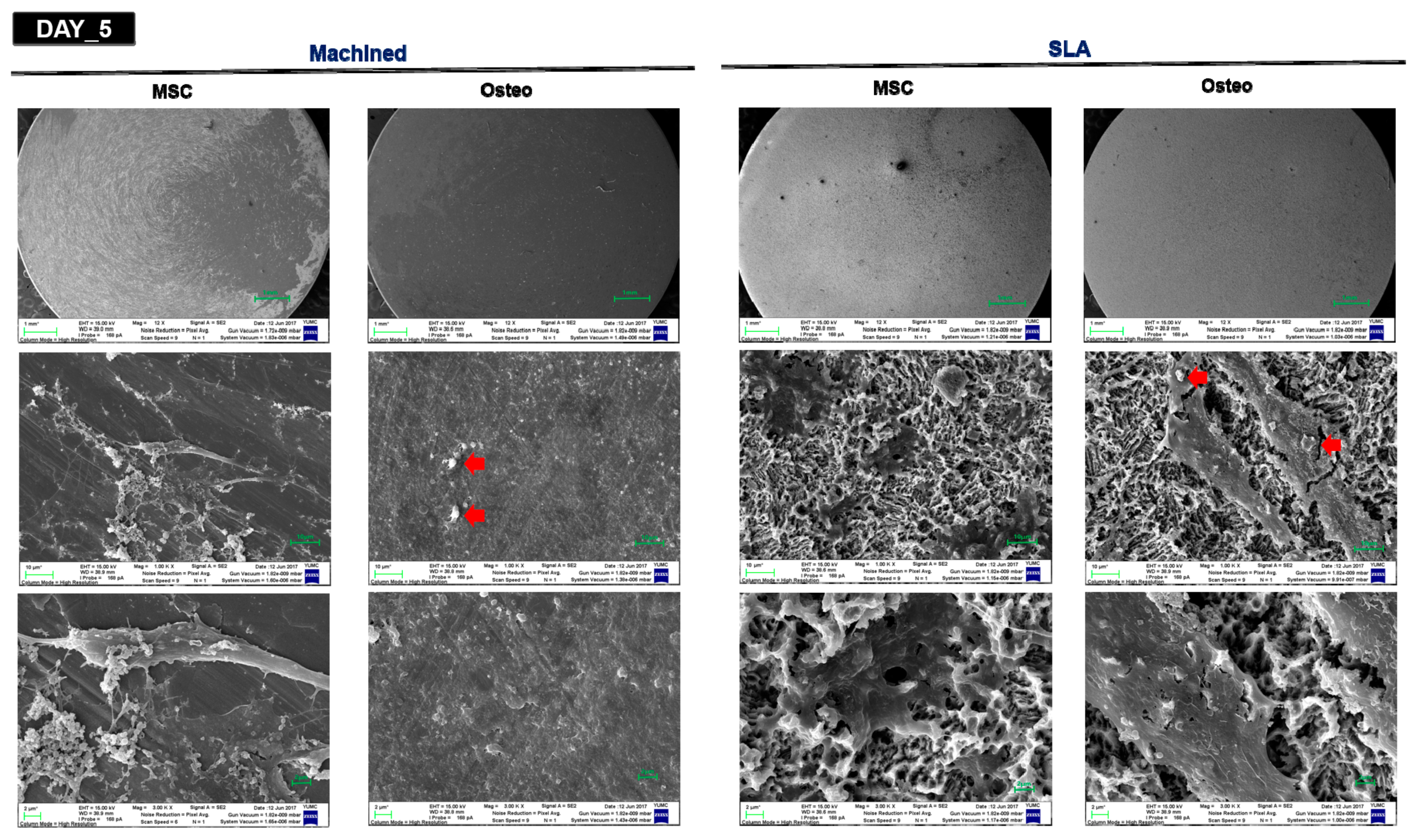
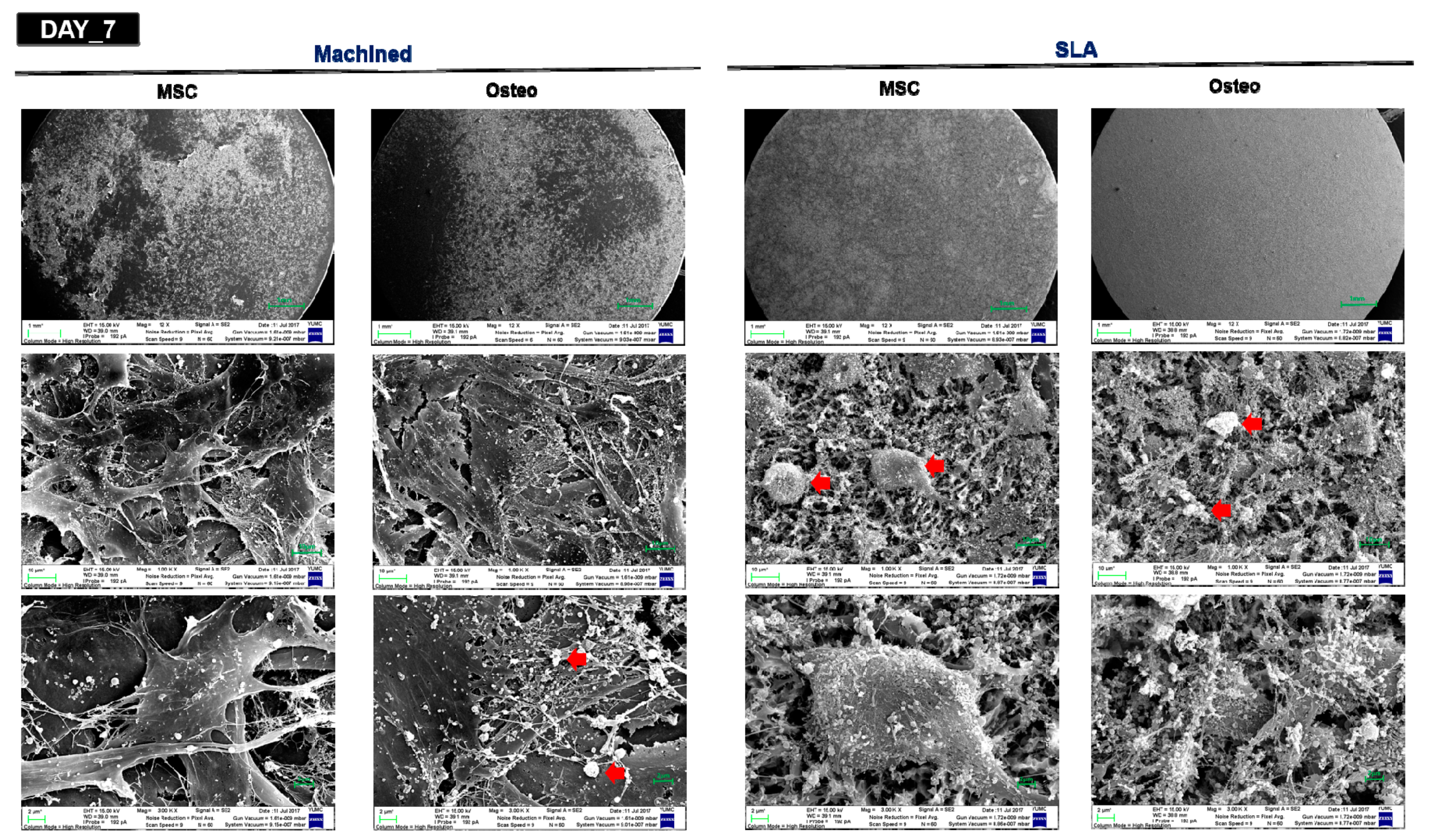
2.3. Surface Analysis by SEM
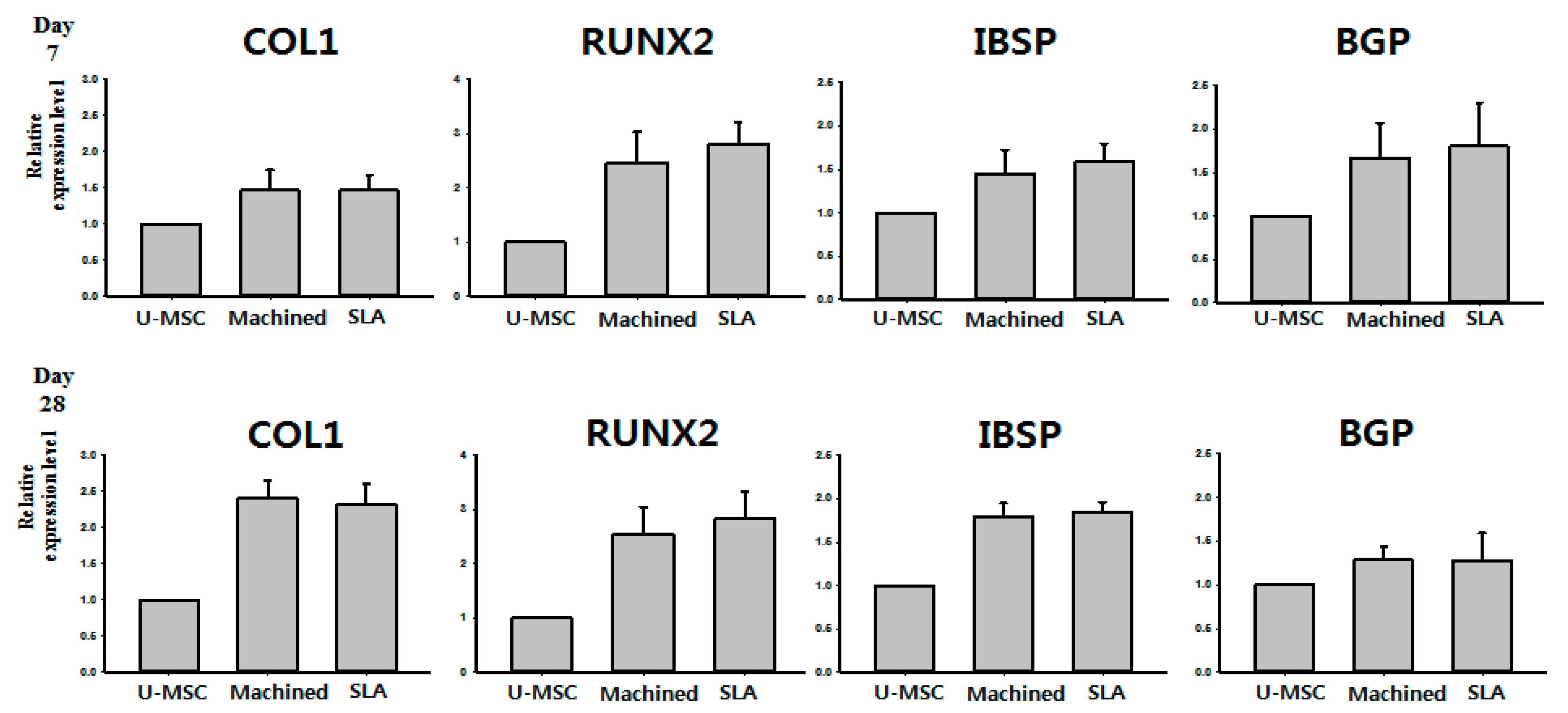
2.4. Quantitative RT-PCR
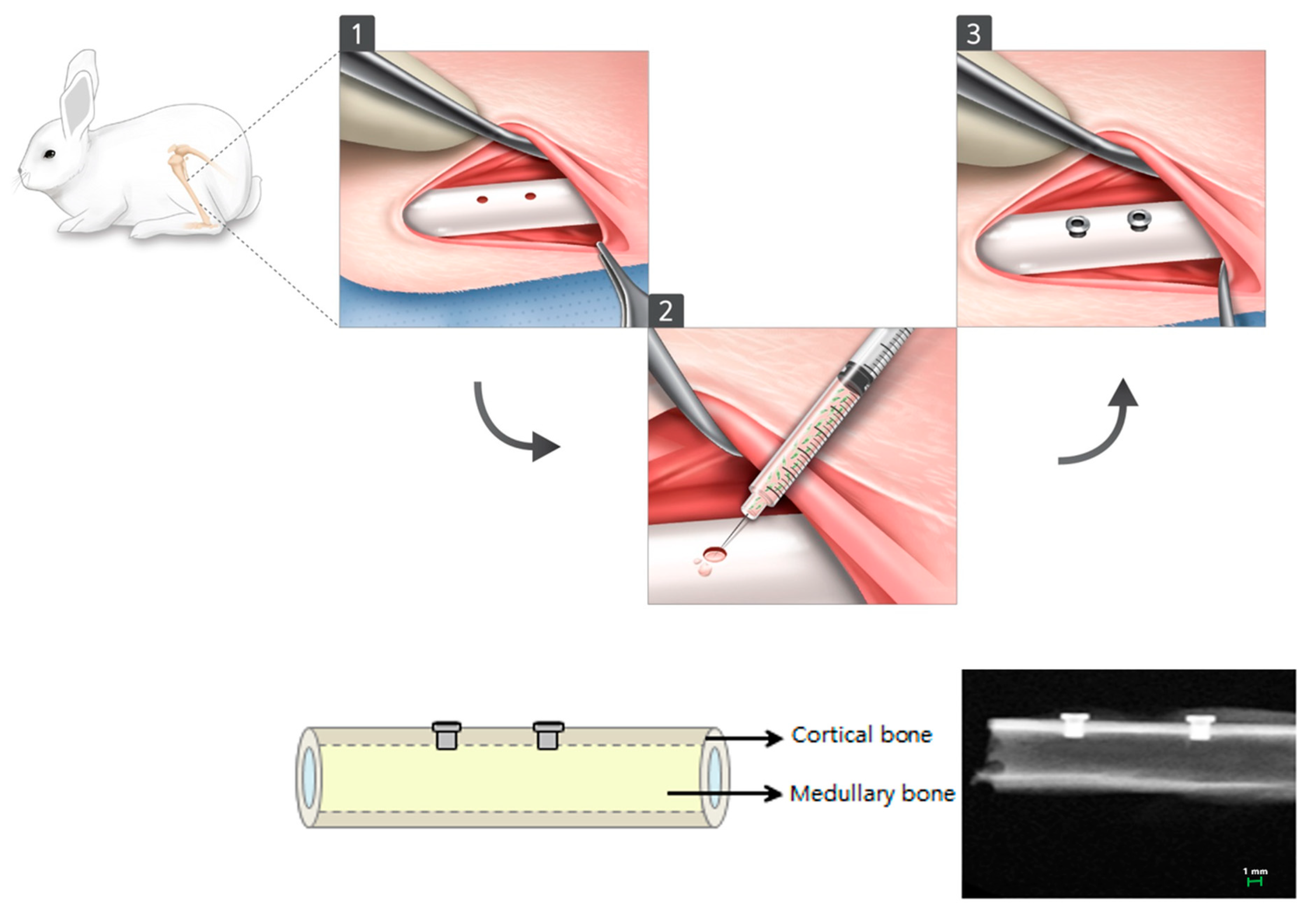
2.5. Preparation of Customized Implant and Animal Preparation and In Vivo d-hMSC Transplant
2.6. Radiological Analysis
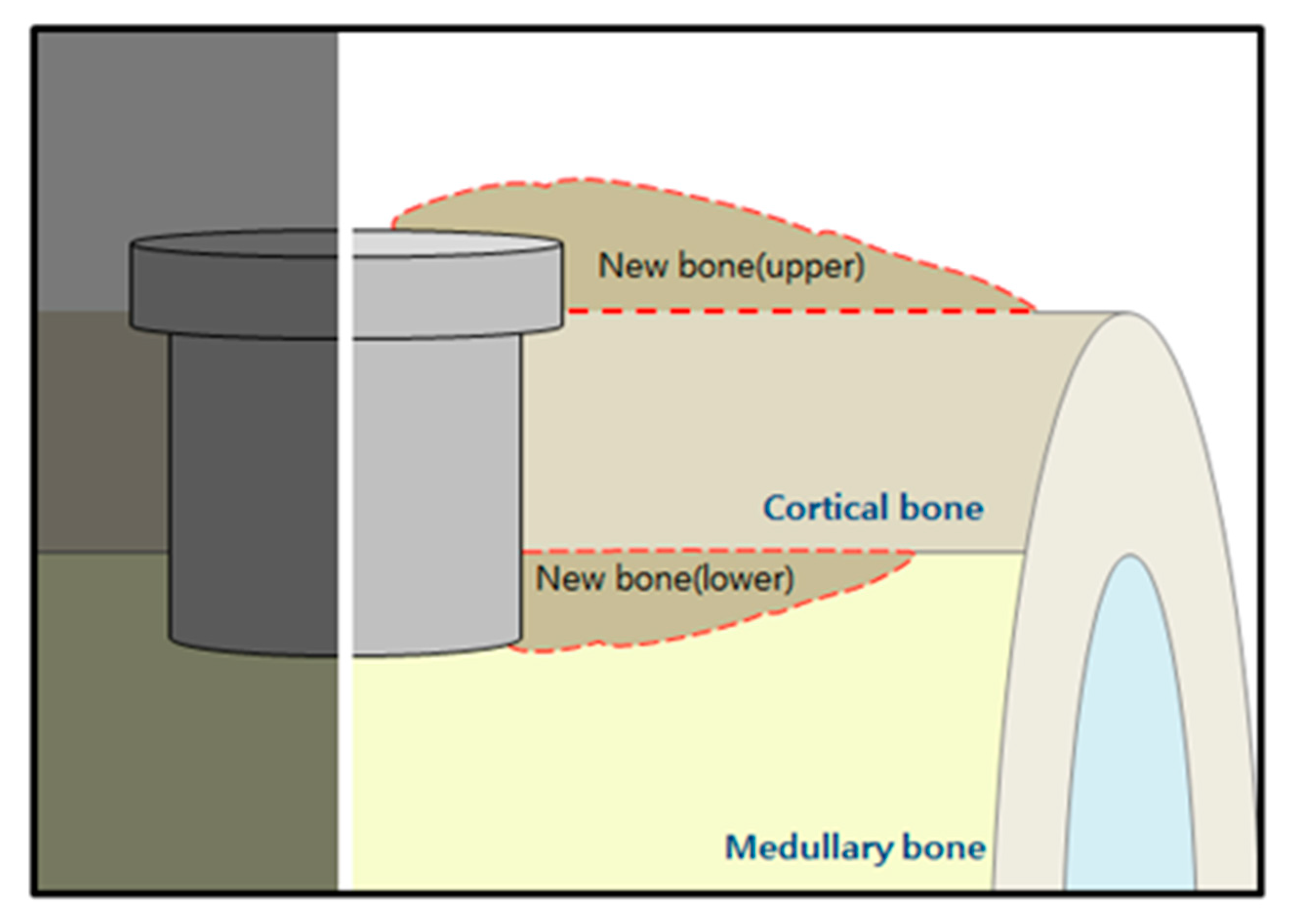
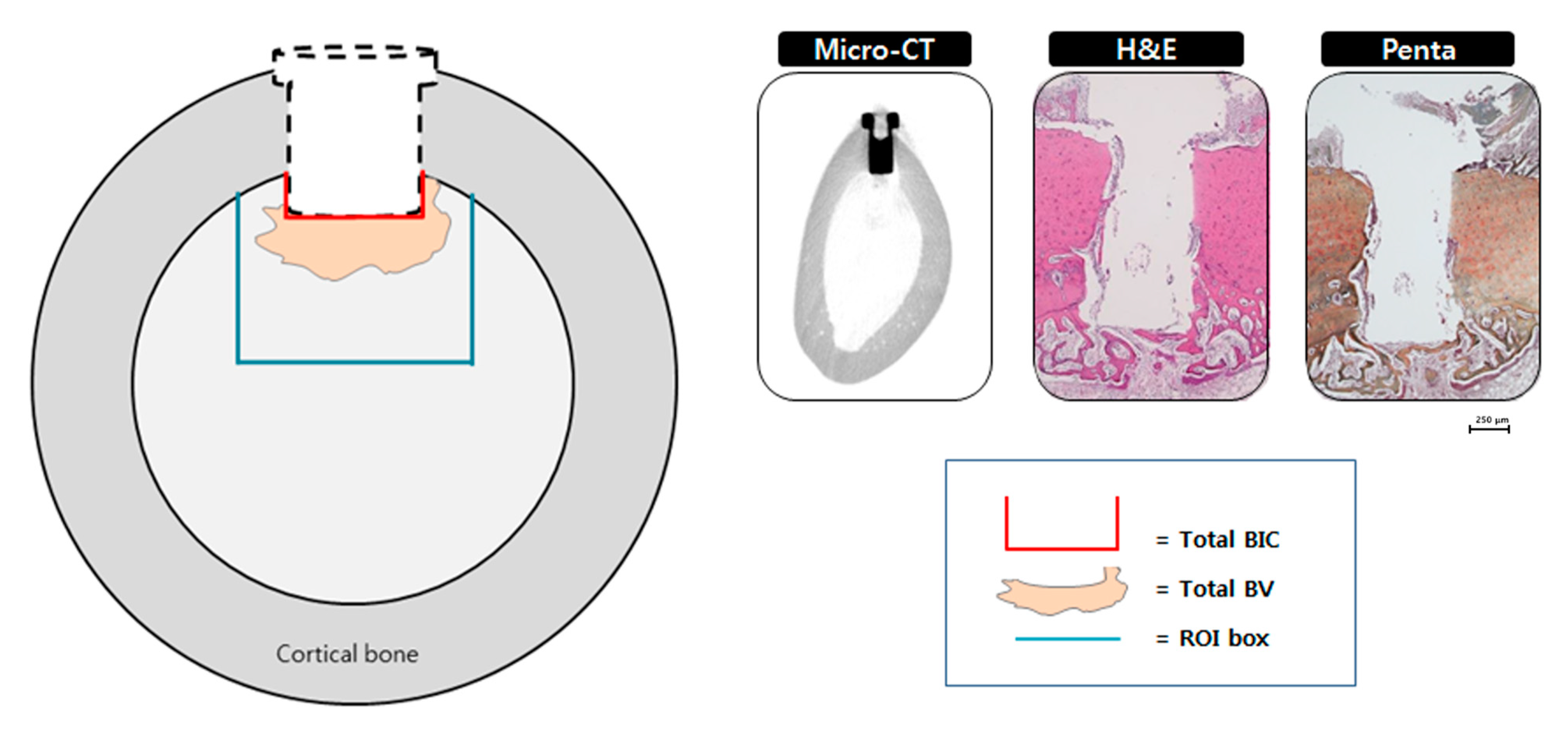
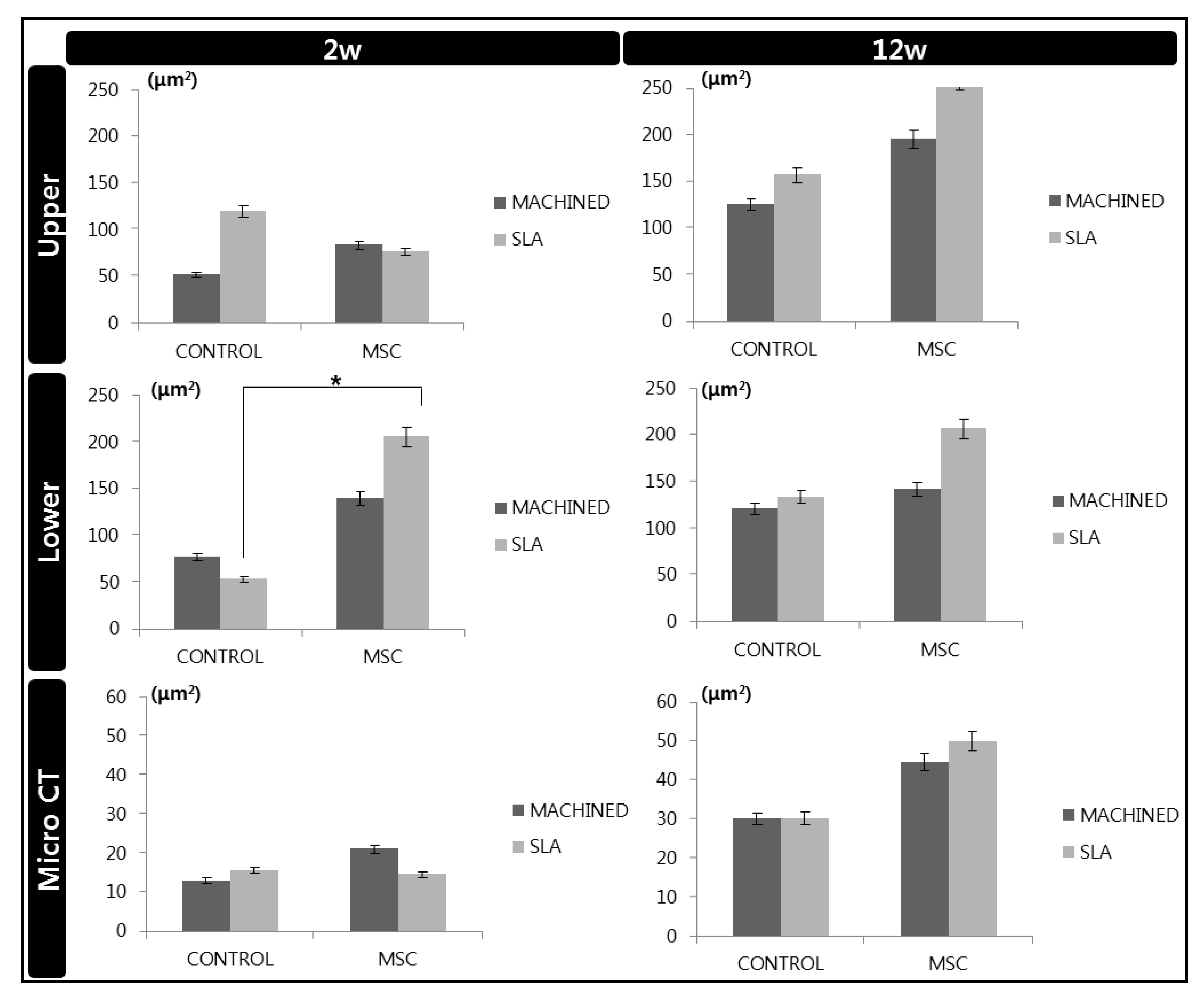
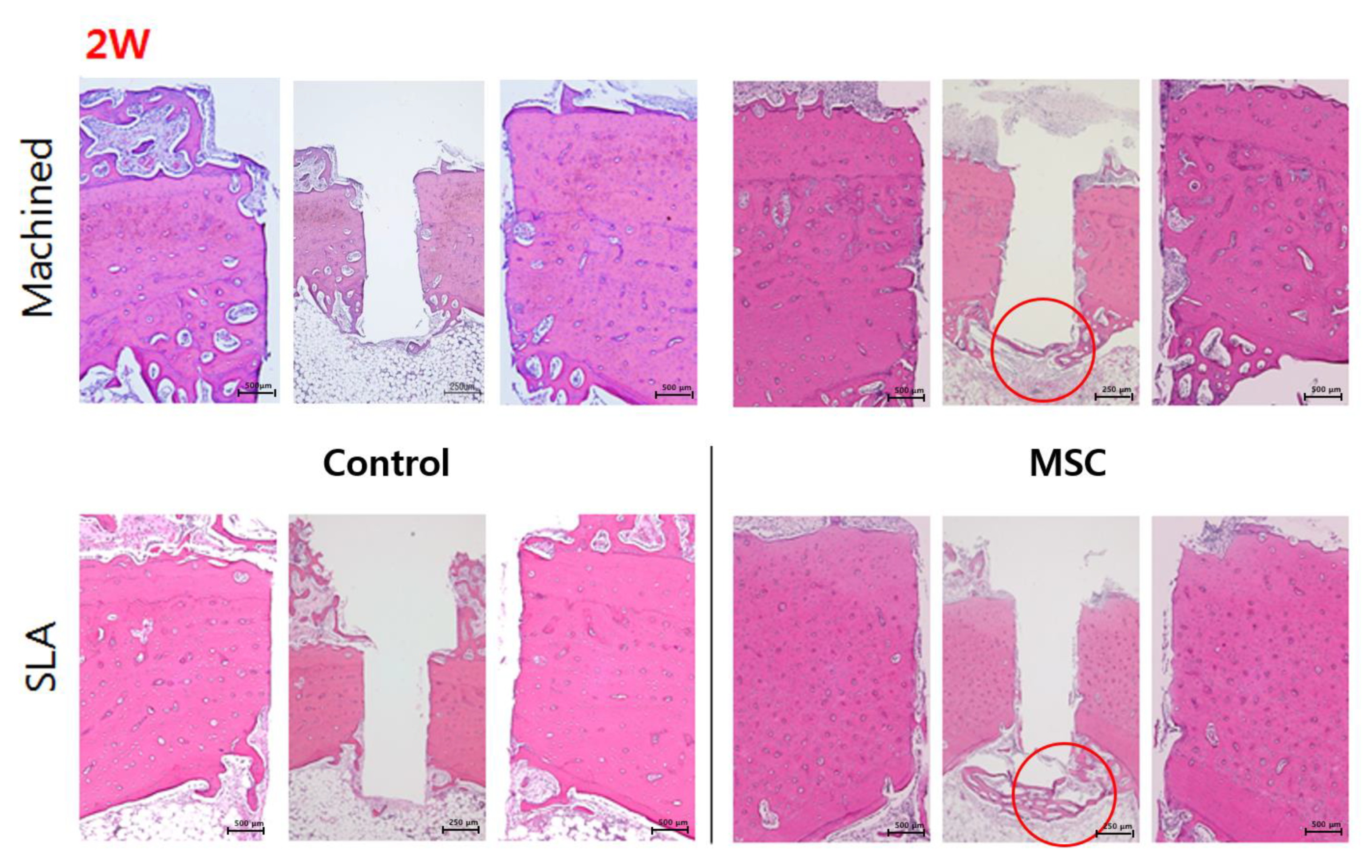
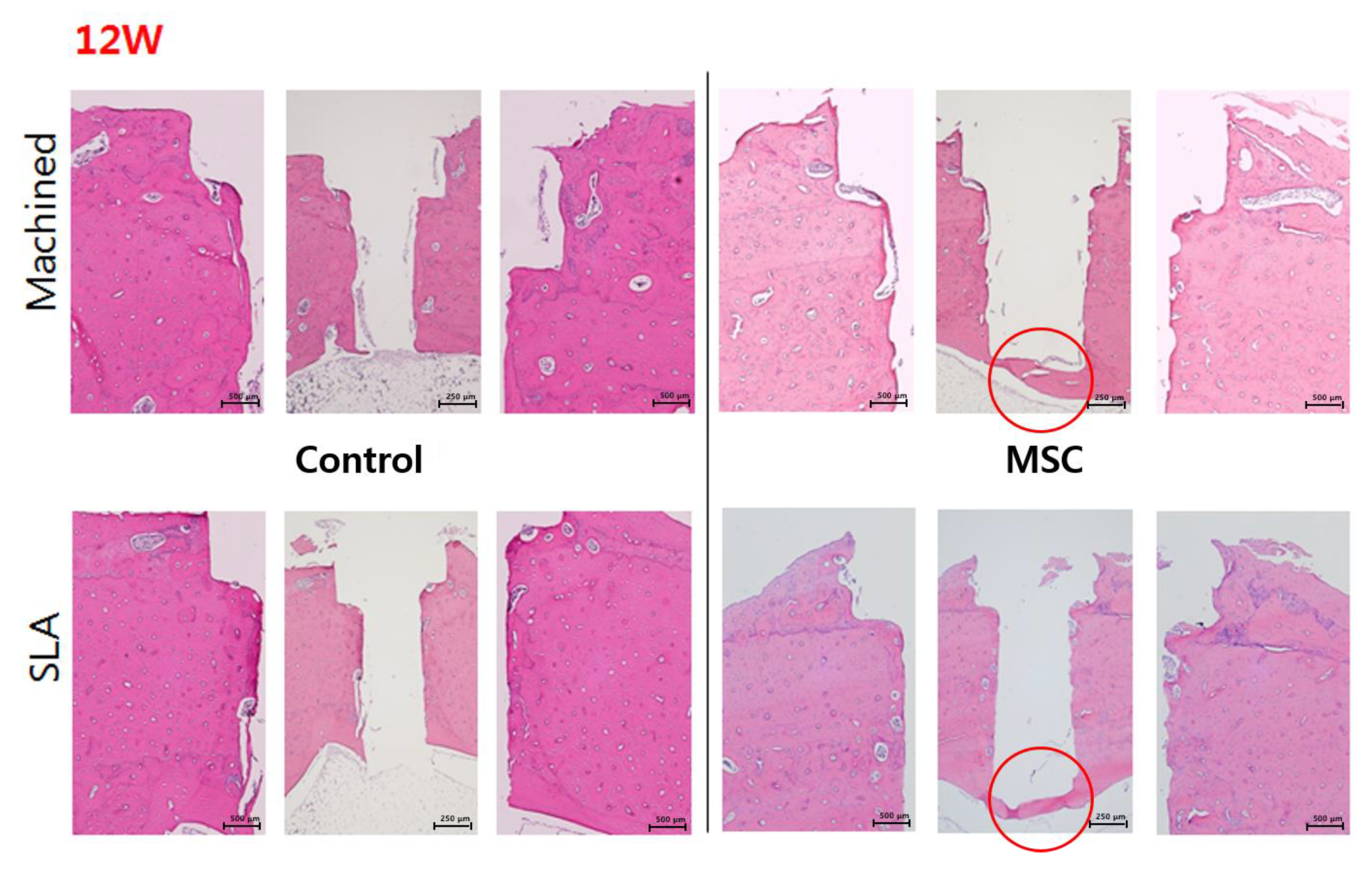
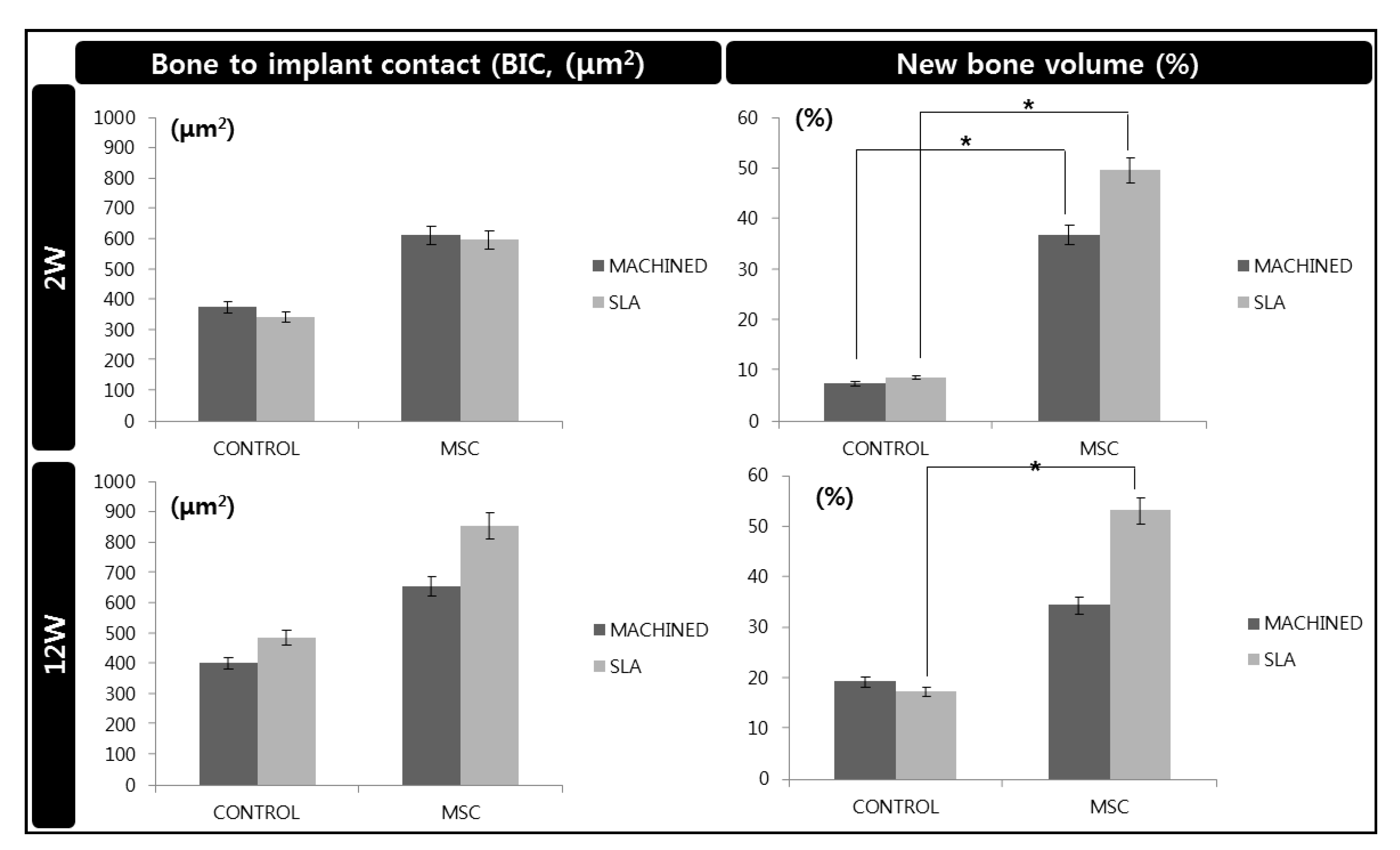
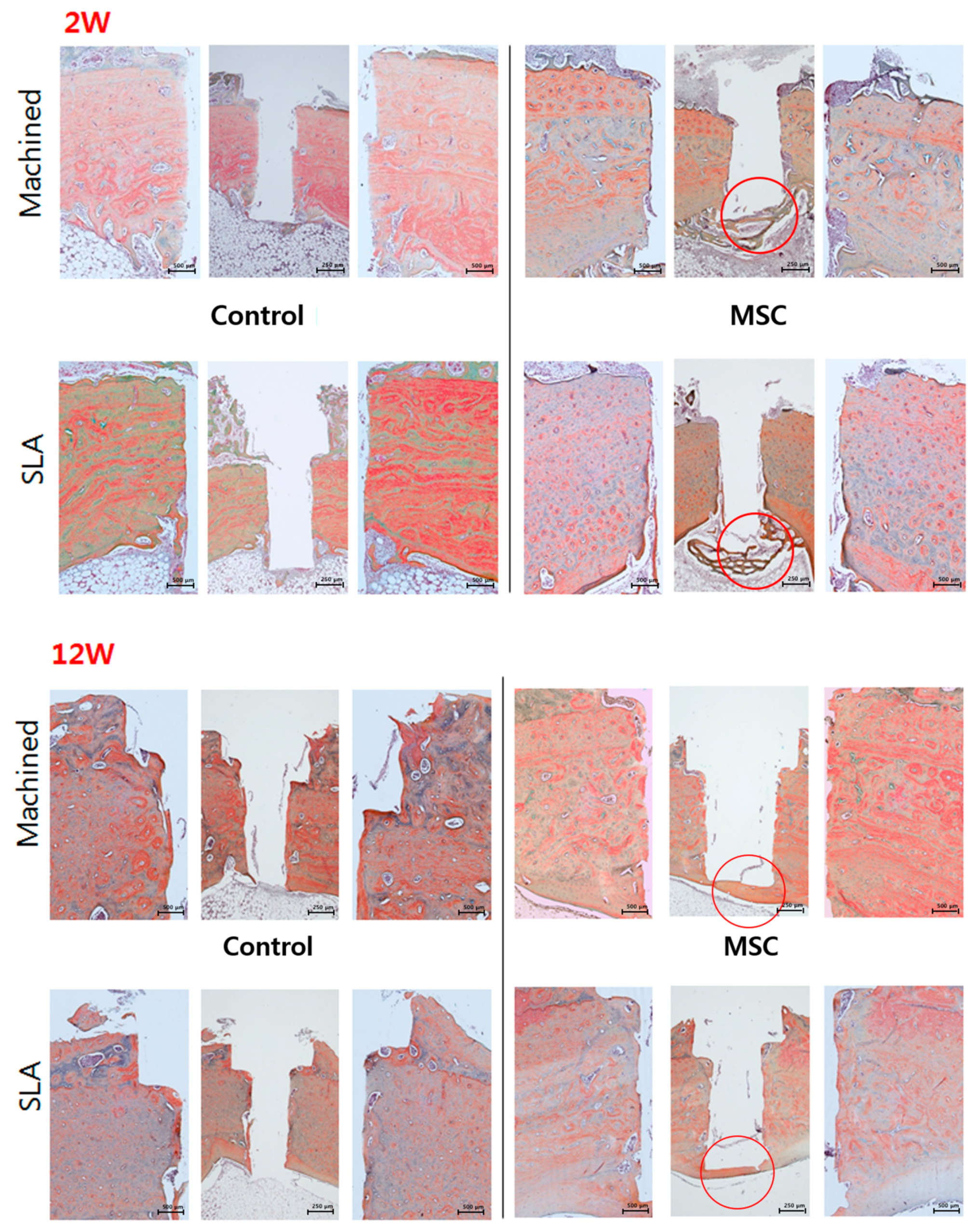
2.7. Histological and Histomorphometric Analysis (H&E, Russell-Movat Pentachrome: Bone Volume, Bone-Implant Contact) and Immunohistochemistry (Human nuclei A, BrdU)
2.8. Statistical Analysis
3. Results
3.1. Surface Analysis by SEM
3.2. Expression of Osteogenic Genes of d-hMSCs (RT-PCR)
3.3. Radiological Analysis
3.4. Histological and Histomorphometric Analysis (H&E, Russell-Movat Pentachrome: BIC, BV)
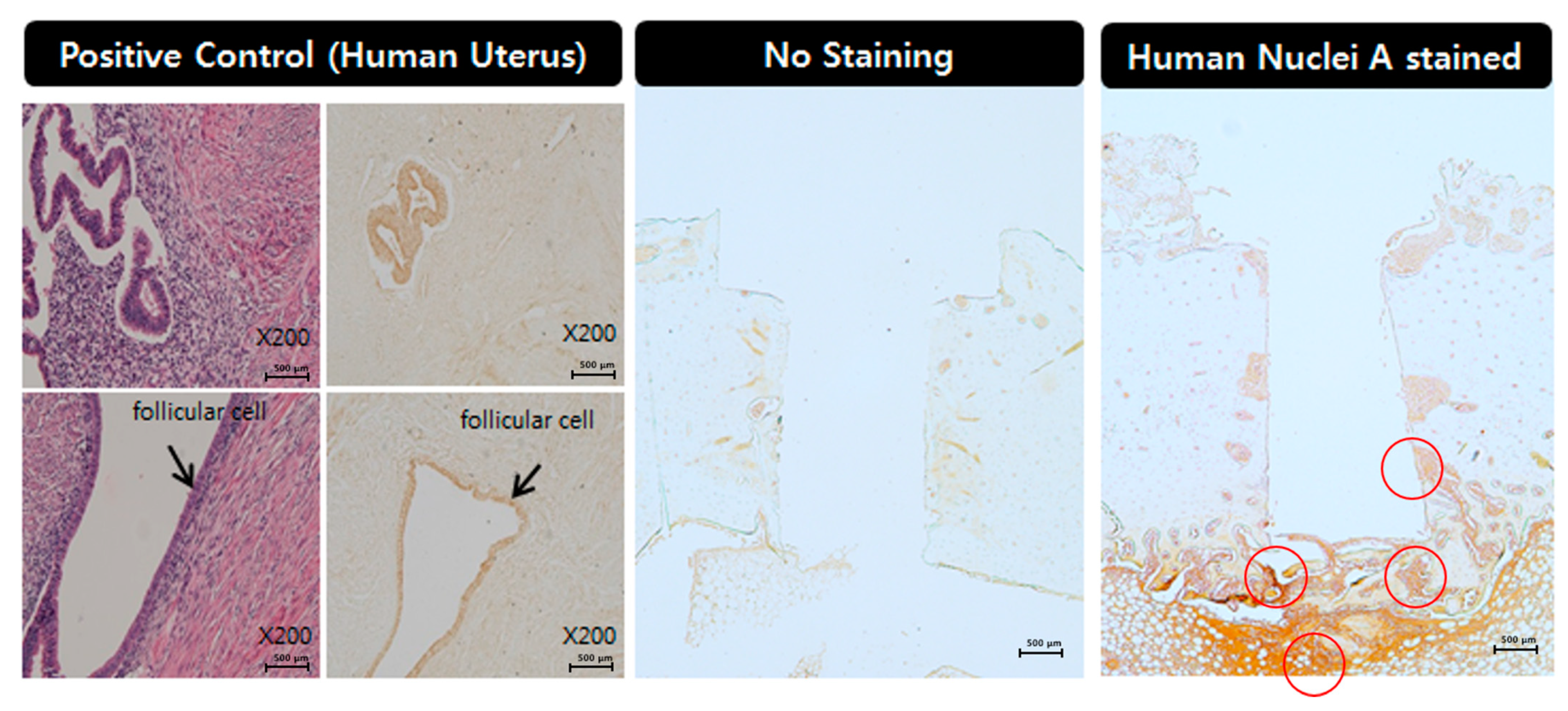
3.5. Immunohistochemistry
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, C.Y.; Zhao, B.H.; Ai, H.J.; Wang, Y.W. Comparison of biological characteristics of mesenchymal stem cells grown on two different titanium implant surfaces. Biomed. Mater. 2008, 3, 015004. [Google Scholar] [CrossRef]
- Mante, M.; Daniels, B.; Golden, E.; Diefenderfer, D.; Reilly, G.; Leboy, P.S. Attachment of human marrow stromal cells to titanium surfaces. J. Oral Implantol. 2003, 29, 66–72. [Google Scholar] [CrossRef] [Green Version]
- Logan, N.; Brett, P. The Control of Mesenchymal Stromal Cell Osteogenic Differentiation through Modified Surfaces. Stem Cells Int. 2013, 2013, 361637. [Google Scholar] [CrossRef] [Green Version]
- Cochran, D.L.; Nummikoski, P.V.; Higginbottom, F.L.; Hermann, J.S.; Makins, S.R.; Buser, D. Evaluation of an endosseous titanium implant with a sandblasted and acid-etched surface in the canine mandible: Radiographic results. Clin. Oral Implant. Res. 1996, 7, 240–252. [Google Scholar] [CrossRef]
- Eom, T.G.; Jeon, G.R.; Jeong, C.M.; Kim, Y.K.; Kim, S.G.; Cho, I.H.; Cho, Y.S.; Oh, J.S. Experimental study of bone response to hydroxyapatite coating implants: Bone-implant contact and removal torque test. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 411–418. [Google Scholar] [CrossRef]
- Duske, K.; Koban, I.; Kindel, E.; Schroder, K.; Nebe, B.; Holtfreter, B.; Jablonowski, L.; Weltmann, K.D.; Kocher, T. Atmospheric plasma enhances wettability and cell spreading on dental implant metals. J. Clin. Periodontol. 2012, 39, 400–407. [Google Scholar] [CrossRef]
- Ogawa, T. Ultraviolet photofunctionalization of titanium implants. Int. J. Oral Maxillofac. Implant. 2014, 29, e95–e102. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.Y.; Choi, H.; Lee, J.H.; Kim, J.H.; Jung, H.S.; Kim, J.H.; Park, Y.B.; Moon, H.S. UV Photofunctionalization Effect on Bone Graft in Critical One-Wall Defect around Implant: A Pilot Study in Beagle Dogs. BioMed Res. Int. 2016, 2016, 4385279. [Google Scholar] [CrossRef]
- Klinker, M.W.; Wei, C.H. Mesenchymal stem cells in the treatment of inflammatory and autoimmune diseases in experimental animal models. World J. Stem Cells 2015, 7, 556–567. [Google Scholar] [CrossRef]
- Pileggi, A. Mesenchymal stem cells for the treatment of diabetes. Diabetes 2012, 61, 1355–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin-Rendon, E.; Brunskill, S.J.; Hyde, C.J.; Stanworth, S.J.; Mathur, A.; Watt, S.M. Autologous bone marrow stem cells to treat acute myocardial infarction: A systematic review. Eur. Heart J. 2008, 29, 1807–1818. [Google Scholar] [CrossRef] [Green Version]
- Vainshtein, J.M.; Kabarriti, R.; Mehta, K.J.; Roy-Chowdhury, J.; Guha, C. Bone marrow-derived stromal cell therapy in cirrhosis: Clinical evidence, cellular mechanisms, and implications for the treatment of hepatocellular carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 786–803. [Google Scholar] [CrossRef] [Green Version]
- Davies, J.E. Mechanisms of endosseous integration. Int. J. Prosthodont. 1998, 11, 391–401. [Google Scholar]
- Davies, J.E. Understanding peri-implant endosseous healing. J. Dent. Educ. 2003, 67, 932–949. [Google Scholar] [CrossRef]
- Bigerelle, M.; Anselme, K.; Noel, B.; Ruderman, I.; Hardouin, P.; Iost, A. Improvement in the morphology of Ti-based surfaces: A new process to increase in vitro human osteoblast response. Biomaterials 2002, 23, 1563–1577. [Google Scholar] [CrossRef]
- Yang, Y.; Tian, J.; Deng, L.; Ong, J.L. Morphological behavior of osteoblast-like cells on surface-modified titanium in vitro. Biomaterials 2002, 23, 1383–1389. [Google Scholar] [CrossRef]
- Ku, C.H.; Pioletti, D.P.; Browne, M.; Gregson, P.J. Effect of different Ti-6Al-4V surface treatments on osteoblasts behaviour. Biomaterials 2002, 23, 1447–1454. [Google Scholar] [CrossRef] [Green Version]
- Mayr-Wohlfart, U.; Fiedler, J.; Gunther, K.P.; Puhl, W.; Kessler, S. Proliferation and differentiation rates of a human osteoblast-like cell line (SaOS-2) in contact with different bone substitute materials. J. Biomed. Mater. Res. 2001, 57, 132–139. [Google Scholar] [CrossRef]
- Shi, S.R.; Shi, Y.; Taylor, C.R. Antigen retrieval immunohistochemistry: Review and future prospects in research and diagnosis over two decades. J. Histochem. Cytochem. 2011, 59, 13–32. [Google Scholar] [CrossRef]
- McAllister, B.S. Stem cell-containing allograft matrix enhances periodontal regeneration: Case presentations. Int. J. Periodontics Restor. Dent. 2011, 31, 149–155. [Google Scholar]
- McAllister, B.S.; Haghighat, K.; Gonshor, A. Histologic evaluation of a stem cell-based sinus-augmentation procedure. J. Periodontol. 2009, 80, 679–686. [Google Scholar] [CrossRef]
- Park, J.B. Use of cell-based approaches in maxillary sinus augmentation procedures. J. Craniofacial Surg. 2010, 21, 557–560. [Google Scholar] [CrossRef]
- Razzouk, S.; Schoor, R. Mesenchymal stem cells and their challenges for bone regeneration and osseointegration. J. Periodontol. 2012, 83, 547–550. [Google Scholar] [CrossRef]
- Fischer, U.M.; Harting, M.T.; Jimenez, F.; Monzon-Posadas, W.O.; Xue, H.; Savitz, S.I.; Laine, G.A.; Cox, C.S. Pulmonary passage is a major obstacle for intravenous stem cell delivery: The pulmonary first-pass effect. Stem Cells Dev. 2009, 18, 683–692. [Google Scholar] [CrossRef]
- Morad, G.; Kheiri, L.; Khojasteh, A. Dental pulp stem cells for in vivo bone regeneration: A systematic review of literature. Arch. Oral Biol. 2013, 58, 1818–1827. [Google Scholar] [CrossRef]
- Bright, R.; Hynes, K.; Gronthos, S.; Bartold, P.M. Periodontal ligament-derived cells for periodontal regeneration in animal models: A systematic review. J. Periodontal Res. 2015, 50, 160–172. [Google Scholar] [CrossRef]
- Choi, H.; Park, K.H.; Lee, A.R.; Mun, C.H.; Shin, Y.D.; Park, Y.B.; Park, Y.B. Control of dental-derived induced pluripotent stem cells through modified surfaces for dental application. Acta Odontol. Scand. 2017, 75, 309–318. [Google Scholar] [CrossRef]
- Barone, A.; Toti, P.; Bertossi, D.; Marconcini, S.; De Santis, D.; Nocini, P.F.; Abdel, M.P.; Kakar, S.; Dietz, A.B.; Cohen, R.C.; et al. Gene Expression of Human Mesenchymal Stem Cells Cultured on Titanium Dental Implant Surfaces. J. Craniofacial Surg. 2016, 27, 712–717. [Google Scholar] [CrossRef]
- Inzunza, D.; Covarrubias, C.; Von Marttens, A.; Leighton, Y.; Carvajal, J.C.; Valenzuela, F.; Díaz-Dosque, M.; Méndez, N.; Martínez, C.; Pino, A.M.; et al. Synthesis of nanostructured porous silica coatings on titanium and their cell adhesive and osteogenic differentiation properties. J. Biomed. Mater. Res. Part A 2014, 102, 37–48. [Google Scholar] [CrossRef]
- Olivares-Navarrete, R.; Hyzy, S.L.; Park, J.H.; Dunn, G.R.; Haithcock, D.A.; Wasilewski, C.E.; Boyan, B.D.; Schwartz, Z. Mediation of osteogenic differentiation of human mesenchymal stem cells on titanium surfaces by a Wnt-integrin feedback loop. Biomaterials 2011, 32, 6399–6411. [Google Scholar] [CrossRef] [Green Version]
- Yao, X.; Peng, R.; Ding, J. Effects of aspect ratios of stem cells on lineage commitments with and without induction media. Biomaterials 2013, 34, 930–939. [Google Scholar] [CrossRef]
- Janson, I.A.; Putnam, A.J. Extracellular matrix elasticity and topography: Material-based cues that affect cell function via conserved mechanisms. J. Biomed. Mater. Res. Part A 2015, 103, 1246–1258. [Google Scholar] [CrossRef] [Green Version]
- Ko, J.Y.; Park, S.; Im, G.I. Osteogenesis from human induced pluripotent stem cells: An in vitro and in vivo comparison with mesenchymal stem cells. Stem Cells Dev. 2014, 23, 1788–1797. [Google Scholar] [CrossRef]
- Tortelli, F.; Tasso, R.; Loiacono, F.; Cancedda, R. The development of tissue-engineered bone of different origin through endochondral and intramembranous ossification following the implantation of mesenchymal stem cells and osteoblasts in a murine model. Biomaterials 2010, 31, 242–249. [Google Scholar] [CrossRef]
- Le Blanc, K.; Pittenger, M. Mesenchymal stem cells: Progress toward promise. Cytotherapy 2005, 7, 36–45. [Google Scholar] [CrossRef]
- Le Blanc, K.; Rasmusson, I.; Sundberg, B.; Gotherstrom, C.; Hassan, M.; Uzunel, M.; Ringdén, O. Treatment of severe acute graft-versus-host disease with third party haploidentical mesenchymal stem cells. Lancet 2004, 363, 1439–1441. [Google Scholar] [CrossRef]
- Piattelli, A.; Scarano, A.; Piattelli, M. Detection of alkaline and acid phosphatases around titanium implants: A light microscopical and histochemical study in rabbits. Biomaterials 1995, 16, 1333–1338. [Google Scholar] [CrossRef]
- Sotiropoulou, P.A.; Perez, S.A.; Salagianni, M.; Baxevanis, C.N.; Papamichail, M. Characterization of the optimal culture conditions for clinical scale production of human mesenchymal stem cells. Stem Cells 2006, 24, 462–471. [Google Scholar] [CrossRef] [Green Version]
- Paschos, N.K.; Brown, W.E.; Eswaramoorthy, R.; Hu, J.C.; Athanasiou, K.A. Advances in tissue engineering through stem cell-based co-culture. J. Tissue Eng. Regen. Med. 2015, 9, 488–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrancio, S.; Lopez-Holgado, N.; Sanchez-Guijo, F.M.; Villaron, E.; Barbado, V.; Tabera, S.; Díez-Campelo, M.; Blanco, J.; San Miguel, J.F.; del Cañizo, M.C.; et al. Optimization of mesenchymal stem cell expansion procedures by cell separation and culture conditions modification. Exp. Hematol. 2008, 36, 1014–1021. [Google Scholar] [CrossRef] [PubMed]
- Bieback, K.; Hecker, A.; Kocaomer, A.; Lannert, H.; Schallmoser, K.; Strunk, D.; Klüter, H. Human alternatives to fetal bovine serum for the expansion of mesenchymal stromal cells from bone marrow. Stem Cells 2009, 27, 2331–2341. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene Name | Gene ID | Sequences | Am Pliconlength (bp) |
|---|---|---|---|
| Hum: an GAPDH F | M33197.1 | cgaccactttgteaagetea | 203 |
| Human GAPDH R | aggggagatteagtgtggtg | ||
| Human IBSP F | NM_004967.3 | egecaatgaatacgacaatg | 196 |
| Human IBSP R | gatgcaaagccagaatggat | ||
| Human COL1A1 F | NM_000088.3 | ggeccagaagaactggtaca | 200 |
| Human COLIA1 R | cgetgttettgcagtggtag | ||
| Human BGLAP F | NM_199173.4 | ggcagegaggtagtgaagag | 194 |
| Human BGLAP R | agcagagegacacectagac | ||
| Human RUNX2 F | NM_001015051.3 | agtgccagetgcatectatt | 201 |
| Hum an RUNX2 R | tgettgaattteccaagg |
| No. of Samples | No. of Animals | 2 Week Group | 12 Week Group | ||
|---|---|---|---|---|---|
| Control machined | 10 | 5 | 10 | 5 | |
| Control SLA | 10 | 10 | |||
| d-MSC machined | 10 | 5 | 10 | 5 | |
| d-MSC SLA | 10 | 10 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.; Park, K.-H.; Jung, N.; Shim, J.-S.; Moon, H.-S.; Kim, H.-J.; Oh, S.-H.; Kim, Y.Y.; Ku, S.-Y.; Park, Y.-B. In Vivo Study for Clinical Application of Dental Stem Cell Therapy Incorporated with Dental Titanium Implants. Materials 2021, 14, 381. https://doi.org/10.3390/ma14020381
Choi H, Park K-H, Jung N, Shim J-S, Moon H-S, Kim H-J, Oh S-H, Kim YY, Ku S-Y, Park Y-B. In Vivo Study for Clinical Application of Dental Stem Cell Therapy Incorporated with Dental Titanium Implants. Materials. 2021; 14(2):381. https://doi.org/10.3390/ma14020381
Chicago/Turabian StyleChoi, Hyunmin, Kyu-Hyung Park, Narae Jung, June-Sung Shim, Hong-Seok Moon, Hyung-Jun Kim, Seung-Han Oh, Yoon Young Kim, Seung-Yup Ku, and Young-Bum Park. 2021. "In Vivo Study for Clinical Application of Dental Stem Cell Therapy Incorporated with Dental Titanium Implants" Materials 14, no. 2: 381. https://doi.org/10.3390/ma14020381