Risk Management Framework for Nano-Biomaterials Used in Medical Devices and Advanced Therapy Medicinal Products

 , , , , ,
, , , , ,  ,
,  , , , , , , ,
, , , , , , , 
Abstract
:1. Introduction
2. The BIORIMA Risk Management Framework
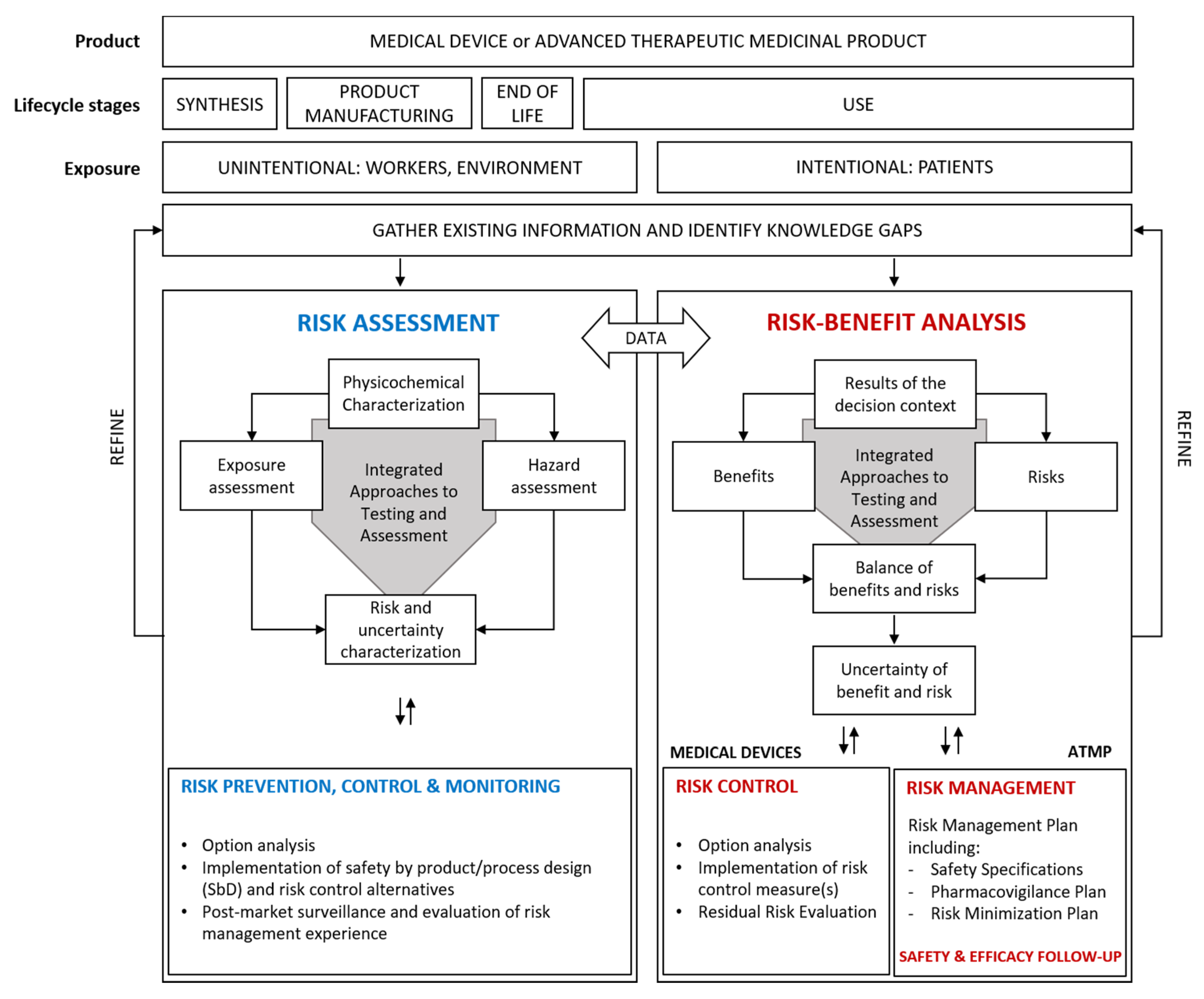
2.1. An Overview of the Risk Management Framework for NBMs
2.2. Risk Assessment Strategy
2.2.1. Occupational Risk Assessment
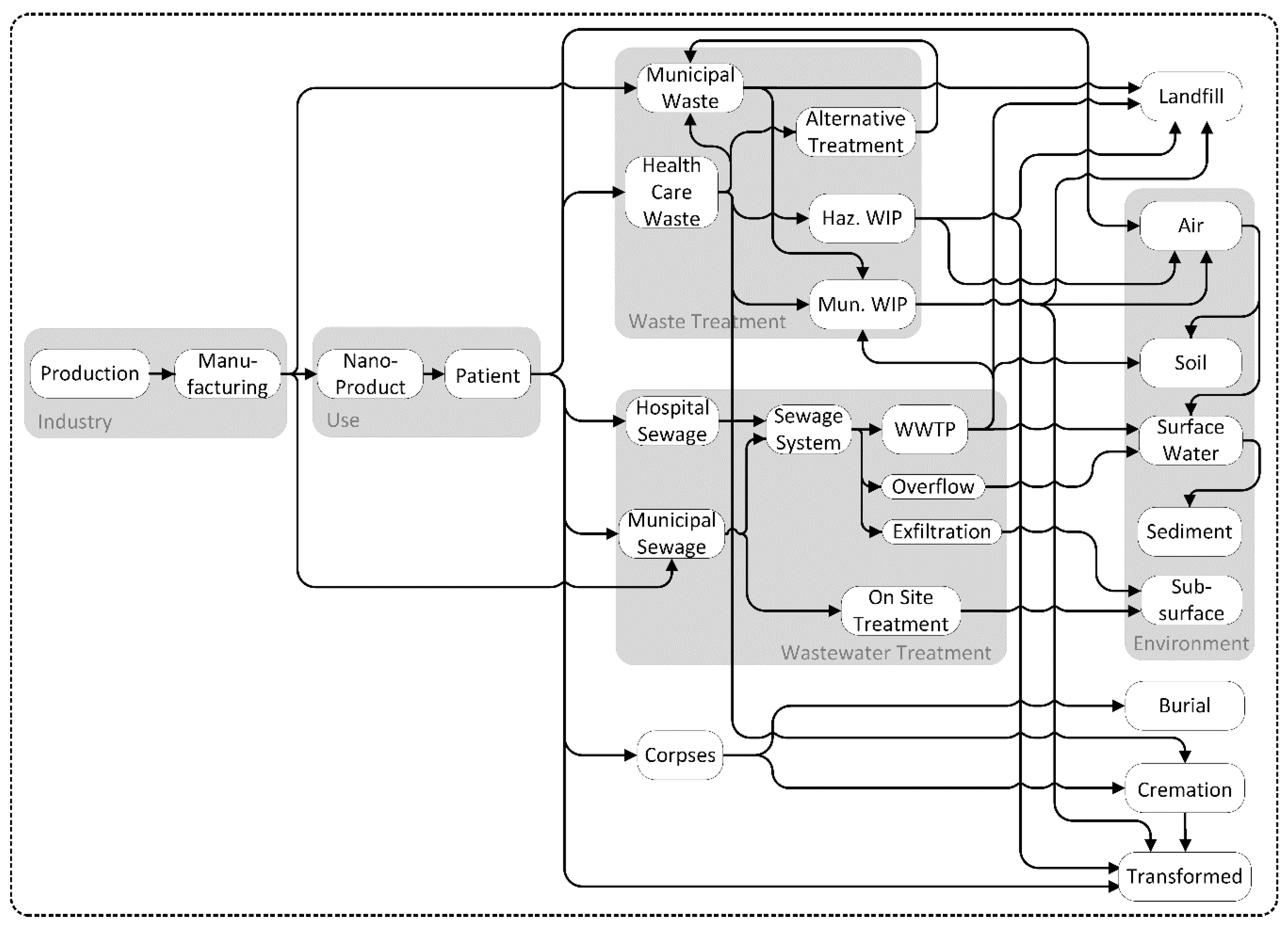
2.2.2. Environmental Risk Assessment
2.2.3. Accidental Risks
2.3. Strategy for Risk Prevention and Control
2.3.1. Safe by Material Design
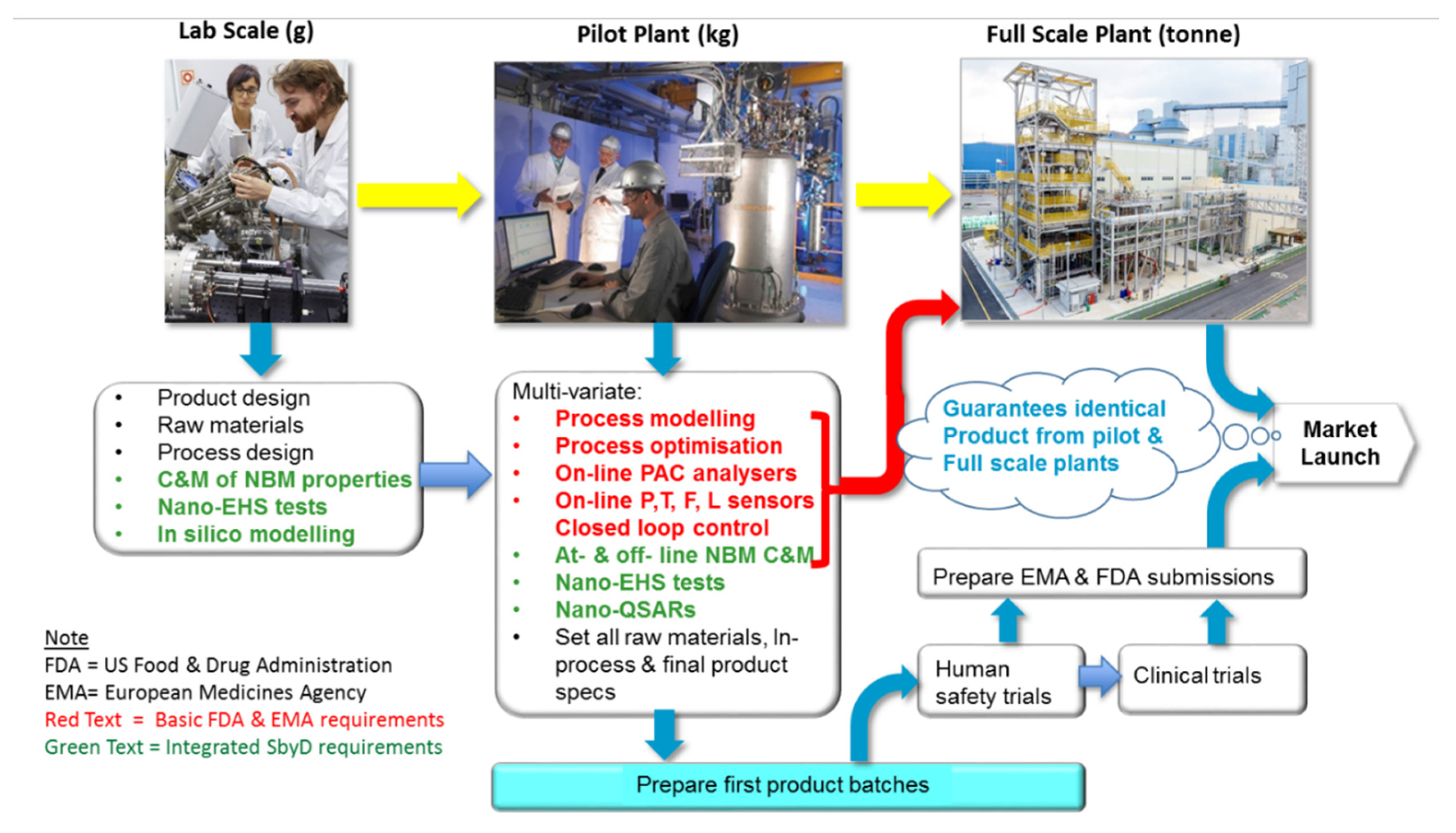
2.3.2. Safety by Process Design
2.3.3. Risk Reduction and Control
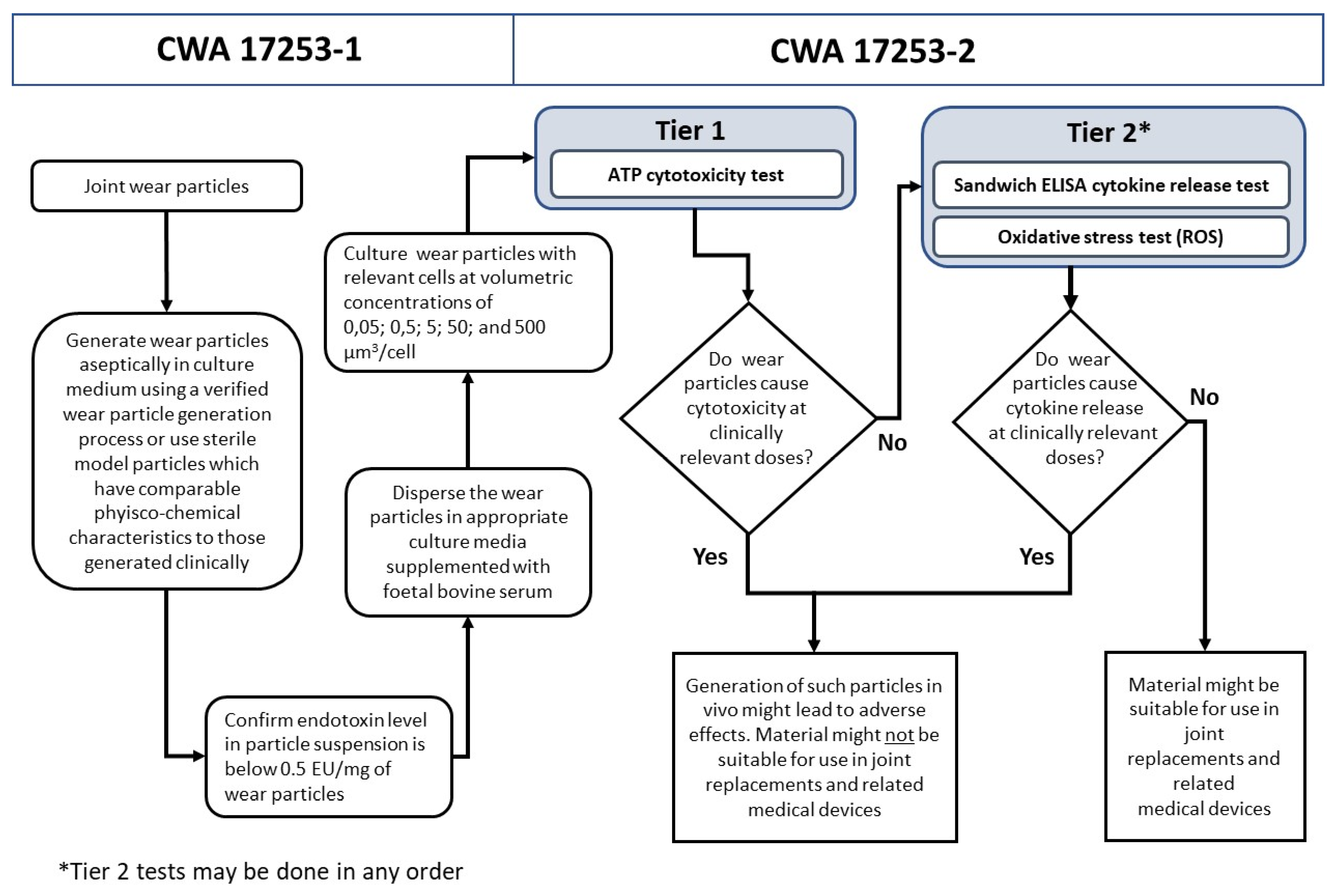
2.3.4. Benefit-Risk Analysis for Managing Risks for Patients
3. Perspectives on the Implementation of the Risk Management Framework
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AOP | Adverse Outcome Pathway |
| API | Active Pharmaceutical Ingredient |
| ATEX | Explosive Atmospheres |
| ATMP | Advanced Therapy Medicinal Products |
| CPC | Condensation Particle Counter |
| CWA | CEN Workshop Agreement |
| DDD | Drug Discovery and Development |
| ECHA | European Chemicals Agency |
| EFM | Environmental Fate Models |
| EFSA | European Food Safety Authority |
| EMA | European Medicines Agency |
| ENM | engineered nanomaterial |
| ERA | environmental risk assessment |
| FDA | Food and Drug Administration |
| FTIR | Fourier transform infrared spectroscopy |
| GMP | Good Manufacturing Practice |
| IATA | Integrated Approaches to Testing and Assessment |
| ICP-MS | Inductively Coupled Plasma-Mass Spectrometry |
| LAL | Limulus amebocyte lysate |
| MCDA | Multicriteria Decision Analysis |
| MD | Medical Device |
| MFA | Material Flow Analysis |
| MHLW | Ministry of Health, Labour and Welfare |
| NBM | nano-biomaterial |
| OECD | Organisation for Economic Co-operation and Development |
| PAC | Process Analytical Control |
| PBPK | Physiologically Based Pharmacokinetic |
| PEC | Predicted Environmental Concentrations |
| PhRMA BRAT | Pharmaceutical Research and Manufacturers of America, the Benefit-Risk Action Team |
| PNEC | Predicted No-Effect Concentrations |
| PrOACT-URL | Problem formulation, Objectives, Alternatives Consequences, Trade-offs, Uncertainties, Risk tolerance |
| QA | Quality Assurance |
| QSAR | Quantitative Structure Activity Relationship |
| REACH | Registration, Evaluation, Authorisation and restriction of Chemicals |
| RMF | Risk Management Framework |
| RMM | Risk Management Measures |
| RMP | Risk Management Plan |
| R&D | Research and Development |
| SbD | Safe-by-Design |
| SbMD | safe by material design |
| SbPD | safety by process design |
| S&E | Safety and Efficacy |
| SEM | Scanning Electron Microscopy |
| SMPS | Scanning Mobility Particle Sizer |
| TEM | Transmission Electron Microscopy |
| UMBRA | Universal Methodology for Benefit-Risk Assessment |
| UN/GHS | United Nations Globally Harmonized System of Classification and Labelling of Chemicals |
References
- Yang, L.; Zhang, L.; Webster, T.J. Nanobiomaterials: State of the Art and Future Trends. Adv. Eng. Mater. 2011, 13, 197–217. [Google Scholar] [CrossRef]
- Singh, T.G.; Dhiman, S.; Jindal, M.; Sandhu, I.S.; Chitkara, M. Nanobiomaterials: Applications in Biomedicine and Biotechnology. In Fabrication and Self-Assembly of Nanobiomaterials: Applications of Nanobiomaterials; William Andrew Publishing: Oxford, UK, 2016; pp. 401–429. [Google Scholar] [CrossRef]
- Genchi, G.G.; Marino, A.; Grillone, A.; Pezzini, I.; Ciofani, G. Smart Nanobiomaterials: Remote Control of Cellular Functions: The Role of Smart Nanomaterials in the Medicine of the Future. Adv. Healthc. Mater. 2017, 6. [Google Scholar] [CrossRef] [Green Version]
- Shivaramakrishnan, B.; Gurumurthy, B.; Balasubramanian, A. Potential Biomedical Applications of Metallic Nanobiomaterials: A Review. Int. J. Pharm. Sci. Res. 2017, 8, 985–1000. [Google Scholar] [CrossRef]
- Li, X.; Lee, S.C.; Zhang, S.; Akasaka, T. Biocompatibility and Toxicity of Nanobiomaterials 2014. J. Nanomater. 2015. [Google Scholar] [CrossRef]
- Falkner, R.; Jaspers, N. Regulating Nanotechnologies: Risk, Uncertainty and the Global Governance Gap. Glob. Environ. Polit. 2012, 12, 30–55. [Google Scholar] [CrossRef] [Green Version]
- Linkov, I.; Steevens, J. Nanomaterials: Risks and Benefits; Springer Science & Business Media: Berlin, Germany, 2008. [Google Scholar]
- Linkov, I.; Satterstrom, F.K.; Corey, L.M. Nanotoxicology and Nanomedicine: Making Hard Decisions. Nanomed. Nanotechnol. Biol. Med. 2008, 4, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Schummer, J.; Pariotti, E. Regulating Nanotechnologies: Risk Management Models and Nanomedicine. Nanoethics 2008, 2, 39–42. [Google Scholar] [CrossRef]
- Halamoda-Kenzaoui, B.; Box, H.; van Elk, M.; Gaitan, S.; Geertsma, R.E.; Gainza Lafuente, E.; Owen, A.; Del Pozo, A.; Roesslein, M.; Bremer-Hoffmann, S. Anticipation of Regulatory Needs for Nanotechnology—Enabled Health Products; The REFINE White Paper; Publications Office of the European Union: Luxembourg, 2019. [Google Scholar] [CrossRef]
- BIORIMA|Risk Management of Biomaterials. Available online: https://www.biorima.eu/ (accessed on 17 September 2020).
- European Commission (EC). Regulation (EC) No 1907/2006 of the European Parliament and of the Council of 18 December 2006 Concerning the Registration, Evaluation, Authorisation and Restriction of Chemicals (REACH), Establishing a European Chemicals Agency, Amending Directive 1999/45/EC and Repealing Council Regulation (EEC) No 793/93 and Commission Regulation (EC) No 1488/94 as well as Council Directive 76/769/EEC and Commission Directives 91/155/EEC, 93/67/EEC, 93/105/EC and 2000/21/EC; Official Journal of the European Union: Brussels, Belgium, 2006.
- European Commission (EC). Directive No. 1999/92/EC, of 16 December 1999, on Minimum Requirements for Improving the Safety and Health Protection of Workers Potentially at Risk from Explosive Atmospheres; Official Journal of the European Union: Brussels, Belgium, 2000.
- European Medicines Agency (EMA). Report of the CHMP Working Group on Benifit-Risk Assessment Models and Methods; European Medicines Agency (EMA): London, UK, 2007.
- European Commission (EC). Regulation (EC) No 1394/2007 of the European Parliament and of the Council of the 13 November 2007 on Advanced Therapy Medicinal Products and Amending Directive 2001/83/EC and Regulation (EC) No 726/2004; Official Journal of the European Union: Brussels, Belgium, 2007.
- European Commission (EC). Regulation (EU) 2017/745 of the European Parliament and of the Council of 5 April 2017 on Medical Devices, Amending Directive 2001/83/EC, Regulation (EC) No 178/2002 and Regulation (EC) No 1223/2009 and Repealing Council Directives 90/385/EEC and 93/42/EEC; Official Journal of the European Union: Brussels, Belgium, 2017.
- European Commission (EC). Commission Directive 2009/120/EC of 14 September 2009 Amending Directive 2001/83/EC of the European Parliament and of the Council on the Community code Relating to Medicinal Products for Human Use as Regards Advanced Therapy Medicinal Products; Official Journal of the European Union: Brussels, Belgium, 2009.
- International Organization for Standardization (ISO). ISO 14971:2019 Medical Devices—Application of Risk Management to Medical Devices; ISO: Geneva, Switzerland, 2019. [Google Scholar]
- Cavero, I. Exploratory Safety Pharmacology: A New Safety Paradigm to de-Risk Drug Candidates Prior to Selection for Regulatory Science Investigations. Expert Opin. Drug Saf. 2009, 8, 627–647. [Google Scholar] [CrossRef] [PubMed]
- Curtin, F.; Schulz, P. Assessing the Benefit: Risk Ratio of a Drug--Randomized and Naturalistic Evidence. Dialogues Clin. Neurosci. 2011, 13, 183–190. [Google Scholar] [PubMed]
- Jesus, S.; Schmutz, M.; Som, C.; Borchard, G.; Wick, P.; Borges, O. Hazard Assessment of Polymeric Nanobiomaterials for Drug Delivery: What Can We Learn From Literature So Far. Front. Bioeng. Biotechnol. 2019, 7, 261. [Google Scholar] [CrossRef] [Green Version]
- Amorim, M.J.B.; Fernández-Cruz, M.L.; Hund-Rinke, K.; Scott-Fordsmand, J.J. Environmental Hazard Testing of Nanobiomaterials. Environ. Sci. Eur. 2020, 32, 101. [Google Scholar] [CrossRef]
- Soddu, L.; Trinh, D.N.; Dunne, E.; Kenny, D.; Bernardini, G.; Kokalari, I.; Marucco, A.; Monopoli, M.P.; Fenoglio, I. Identification of Physicochemical Properties That Modulate Nanoparticle Aggregation in Blood. Beilstein J. Nanotechnol. 2020, 11, 550–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortelli, S.; Costa, A.L.; Blosi, M.; Brunelli, A.; Badetti, E.; Bonetto, A.; Hristozov, D.; Marcomini, A. Colloidal Characterization of CuO Nanoparticles in Biological and Environmental Media. Environ. Ment. Sci. Nano 2017, 4, 1201–1420. [Google Scholar] [CrossRef]
- Krpetić, Ž.; Anguissola, S.; Garry, D.; Kelly, P.M.; Dawson, K.A. Nanomaterials: Impact on Cells and Cell Organelles, Nanomateri; Capco, D., Chen, Y., Eds.; Springer: Dordrecht, The Netherlands, 2014. [Google Scholar] [CrossRef]
- Stone, V.; Pozzi-Mucelli, S.; Tran, L.; Aschberger, K.; Sabella, S.; Vogel, U.; Poland, C.; Balharry, D.; Fernandes, T.; Gottardo, S.; et al. ITS-NANO—Prioritising Nanosafety Research to Develop a Stakeholder Driven Intelligent Testing Strategy. Part. Fibre Toxicol. 2014, 11, 9. [Google Scholar] [CrossRef] [Green Version]
- Organisation for Economic Co-operation and Development (OECD). Guidance Document on the Reporting of Defined Approaches to Be Used within Integrated Approaches to Testing and Assessment; OECD: Paris, France, 2016.
- Integrated Approaches to Testing and Assessment (IATA)—OECD. Available online: http://www.oecd.org/chemicalsafety/risk-assessment/iata-integrated-approaches-to-testing-and-assessment.htm (accessed on 17 September 2020).
- Home|Gracious. Available online: https://www.h2020gracious.eu/ (accessed on 17 September 2020).
- Graham, M.L.; Prescott, M.J. The Multifactorial Role of the 3Rs in Shifting the Harm-Benefit Analysis in Animal Models of Disease. Eur. J. Pharmacol. 2015, 759, 19–29. [Google Scholar] [CrossRef] [Green Version]
- European Comission (EC). Commission Regulation (EU) 2018/1881 of 3 December 2018 Amending Regulation (EC) No 1907/2006 of the European Parliament and of the Council on the Registration, Evaluation, Authorisation and Restriction of Chemicals (REACH) as Regards Annexes I, III, VI, VII, VIII, IX, X, XI, and XII to Address Nanoforms of Substances; Official Journal of the European Union: Brussels, Belgium, 2018.
- van Leeuwen, C.J.; Vermeire, T.G. Risk Assessment of Chemicals: An Introduction, 2nd ed.; Springer Science & Business Media: Berlin, Germany, 2007. [Google Scholar]
- Meißner, T.; Potthoff, A.; Richter, V. Physico-Chemical Characterization in the Light of Toxicological Effects. Inhal. Toxicol. 2009, 21 (Suppl. 1), 35–39. [Google Scholar] [CrossRef]
- European Chemicals Agency (ECHA). Guidance on Information Requirements and Chemical Safety AssessmentPart D: Framework for Exposure Assessment; European Chemicals Agency: Helsinki, Finland, 2016. [CrossRef]
- Gao, X.; Lowry, G.V. Progress towards Standardized and Validated Characterizations for Measuring Physicochemical Properties of Manufactured Nanomaterials Relevant to Nano Health and Safety Risks. NanoImpact 2018, 9, 14–30. [Google Scholar] [CrossRef]
- Besinis, A.; De Peralta, T.; Tredwin, C.J.; Handy, R.D. Review of Nanomaterials in Dentistry: Interactions with the Oral. ACS Nano 2015, 9, 2255–2289. [Google Scholar] [CrossRef] [Green Version]
- Van Landuyt, K.L.; Hellack, B.; Van Meerbeek, B.; Peumans, M.; Hoet, P.; Wiemann, M.; Kuhlbusch, T.A.J.; Asbach, C. Nanoparticle Release from Dental Composites. Acta Biomater. 2014, 10, 365–374. [Google Scholar] [CrossRef]
- Wohlleben, W.; Kuhlbusch, T.A.J.; Schnekenburger, J.; Lehr, C.M. Safety of Nanomaterials along Their Lifecycle. Release, Exposure, and Human Hazards; Taylor & Francis Group: Boca Raton, FL, USA, 2015. [Google Scholar] [CrossRef]
- Eastlake, A.C.; Beaucham, C.; Martinez, K.F.; Dahm, M.M.; Sparks, C.; Hodson, L.L.; Geraci, C.L. Refinement of the Nanoparticle Emission Assessment Technique into the Nanomaterial Exposure Assessment Technique (NEAT 2.0). J. Occup. Environ. Hyg. 2016, 13, 708–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramachandran, G.; Park, J.Y.; Raynor, P.C. Assessing Exposures to Nanomaterials in the Occupational Environment; Elsevier: Amsterdam, The Netherlands, 2011. [Google Scholar] [CrossRef]
- Organisation for Economic Co-operation and Development (OECD). Harmonized Tiered Approach to Measure and Assess the Potential Exposure to Airborne Emissions of Engineered Nano-Objects and Their Agglomerates and Aggregates at Workplaces; ENV/JM/MONO1; OECD: Paris, France, 2015.
- Kuhlbusch, T.A.J.; Wijnhoven, S.W.P.; Haase, A. Nanomaterial Exposures for Worker, Consumer and the General Public. NanoImpact 2018, 10, 11–25. [Google Scholar] [CrossRef]
- McNally, K.; Gorce, J.P.; Goede, H.A.; Schinkel, J.; Warren, N. Calibration of the Dermal Advanced REACH Tool (DART) Mechanistic Model. Ann. Work Expo. Health 2019, 63, 637–650. [Google Scholar] [CrossRef] [PubMed]
- Riedmann, R.A.; Gasic, B.; Vernez, D. Sensitivity Analysis, Dominant Factors, and Robustness of the ECETOC TRA v3, Stoffenmanager 4.5, and ART 1.5 Occupational Exposure Models. Risk Anal. 2015, 35, 211–225. [Google Scholar] [CrossRef] [PubMed]
- Spinazzè, A.; Borghi, F.; Campagnolo, D.; Rovelli, S.; Keller, M.; Fanti, G.; Cattaneo, A.; Cavallo, D.M. How to Obtain a Reliable Estimate of Occupational Exposure? Review and Discussion of Models’ Reliability. Int. J. Environ. Res. Public Health 2019, 16, 2764. [Google Scholar] [CrossRef] [Green Version]
- Gorman Ng, M.; Semple, S.; Cherrie, J.; Christopher, Y.; Northage, C.; Tielemans, E.; Veroughstraete, V.; Van Tongeren, M. The relationship between inadvertent ingestion and dermal exposure pathways: A new integrated conceptual model and a database of dermal and oral transfer efficiencies. Ann Occup Hyg. 2012, 56, 1000–1012. [Google Scholar] [CrossRef] [Green Version]
- Miller, N.A.; Reddy, M.B.; Heikkinen, A.T.; Lukacova, V.; Parrott, N. Physiologically Based Pharmacokinetic Modelling for First-In-Human Predictions: An Updated Model Building Strategy Illustrated with Challenging Industry Case Studies. Clin. Pharmacokinet. 2019, 58, 727–746. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Zou, P.; Tyner, K.; Lee, S. Physiologically Based Pharmacokinetic (PBPK) Modeling of Pharmaceutical Nanoparticles. AAPS J. 2017, 19, 26–42. [Google Scholar] [CrossRef]
- Dusinska, M.; Boland, S.; Saunders, M.; Tran, L.; Pojana, G.; Marcomini, A.; Volkovova, K. Towards an Alternative Testing Strategy for Nanomaterials Used in Nanomedicine: Lessons from NanoTEST. Nanotoxicology 2015, 5390, 118–132. [Google Scholar] [CrossRef] [Green Version]
- Drasler, B.; Sayre, P.; Steinhäuser, K.G.; Petri-Fink, A.; Rothen-Rutishauser, B. In Vitro Approaches to Assess the Hazard of Nanomaterials. NanoImpact 2017, 8, 99–116. [Google Scholar] [CrossRef]
- Fadeel, B.; Farcal, L.; Hardy, B.; Vázquez-Campos, S.; Hristozov, D.; Marcomini, A.; Lynch, I.; Valsami-Jones, E.; Alenius, H.; Savolainen, K. Advanced Tools for the Safety Assessment of Nanomaterials. Nat. Nanotechnol. 2018, 13, 537–543. [Google Scholar] [CrossRef]
- Park, M.V.; Lankveld, D.P.; van Loveren, H.; de Jong, W.H. The Status of in Vitro Toxicity Studies in the Risk Assessment of Nanomaterials. Nanomedicine 2009, 4, 669–685. [Google Scholar] [CrossRef] [PubMed]
- Organisation for Economic Co-operation and Development (OECD). Oecd Series on Principles of Good Laboratory Practice and Compliance Monitoring Number 19; Advisory Document of the Working Group on Good Laboratory Practice on the Management, Characterisation and Use of Test Items. ENV/JM/MONO (2018)6; OECD: Paris, France, 2018.
- Halappanavar, S.; Brule, S.V.D.; Nymark, P.; Gaté, L.; Seidel, C.; Valentino, S.; Zhernovkov, V.; Danielsen, P.H.; De Vizcaya, A.; Wolff, H.; et al. Adverse Outcome Pathways as a Tool for the Design of Testing Strategies to Support the Safety Assessment of Emerging Advanced Materials at the Nanoscale. Part. Fibre Toxicol. 2020, 4, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Lynch, I.E. (Ed.) Compendium of Projects in the NanoSafetyCluster; NanoSafety Cluster: Graz, Austria, 2017; Available online: https://www.nanosafetycluster.eu/outputs/nsc-compendium/ (accessed on 12 October 2020).
- Guadagnini, R.; Kenzaoui, B.H.; Cartwright, L.; Pojana, G.; Magdolenova, Z.; Bilanicova, D.; Juillerat, L.; Marcomini, A.; Huk, A.; Fjellsbø, L.M.; et al. Toxicity Screenings of Nanomaterials: Challenges Due to Interference with Assay Processes and Components of Classic in Vitro Tests. Nanotoxicology 2013, 9, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Hansjosten, I.; Rapp, J.; Reiner, L.; Vatter, R.; Fritsch, S.; Ravindra, D.; Palosaari, T.; Joossens, E.; Gerloff, K.; Macko, P.; et al. Microscopy—Based High—Throughput Assays Enable Multi—Parametric Analysis to Assess Adverse Effects of Nanomaterials in Various Cell Lines. Arch. Toxicol. 2018, 92, 633–649. [Google Scholar] [CrossRef]
- Fadeel, B. (Ed.) Nanotoxicology. State-of-the-Art and Future Research Needs; IMM Report 1/2018; Institute of Environmental Medicine, Karolinska Institute: Stockholm, Sweden, 2018. [Google Scholar]
- Faria, M.; Björnmalm, M.; Thurecht, K.J.; Kent, S.J.; Parton, R.G.; Kavallaris, M.; Johnston, A.P.R.; Gooding, J.J.; Corrie, S.R.; Boyd, B.J.; et al. Minimum Information Reporting in Bio-Nano Experimental Literature. Nat. Nanotechnol. 2018, 13, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Hannon, G.; Lysaght, J.; Liptrott, N.J.; Prina-Mello, A. Immunotoxicity Considerations for Next Generation Cancer Nanomedicines. Adv. Sci. 2019, 6, 1900133. [Google Scholar] [CrossRef] [Green Version]
- Monopoli, M.P.; Walczyk, D.; Campbell, A.; Elia, G.; Lynch, I.; Baldelli Bombelli, F.; Dawson, K.A. Physical-Chemical Aspects of Protein Corona: Relevance to in Vitro and in Vivo Biological Impacts of Nanoparticles. J. Am. Chem. Soc. 2011, 133, 2525–2534. [Google Scholar] [CrossRef]
- Dai, Q.; Guo, J.; Yan, Y.; Ang, C.S.; Bertleff-Zieschang, N.; Caruso, F. Cell-Conditioned Protein Coronas on Engineered Particles Influence Immune Responses. Biomacromolecules 2017, 18, 431–439. [Google Scholar] [CrossRef] [Green Version]
- European Medicines Agency (EMA). Guideline on the Environmental Risk Assessment of Medicinal Products for Human Use; European Medicines Agency: London, UK, 2018.
- Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR). Guidance on the Determination of Potential Health Effects of Nanomaterials Used in Medical Devices; European Commission, DG Health and Food Safety: Luxembourg, 2015. [CrossRef]
- Sun, T.Y.; Bornhöft, N.A.; Hungerbühler, K.; Nowack, B. Dynamic Probabilistic Modeling of Environmental Emissions of Engineered Nanomaterials. Environ. Sci. Technol. 2016, 50, 4701–4711. [Google Scholar] [CrossRef]
- Kraas, M.; Schlich, K.; Knopf, B.; Wege, F.; Kägi, R.; Terytze, K.; Hund-Rinke, K. Long-Term Effects of Sulfidized Silver Nanoparticles in Sewage Sludge on Soil Microflora. Environ. Toxicol. Chem. 2017, 36, 3305–3313. [Google Scholar] [CrossRef] [Green Version]
- Irizar, A.; Amorim, M.J.B.; Fuller, K.P.; Zeugolis, D.I.; Scott-Fordsmand, J.J. Environmental Fate and Effect of Biodegradable Electro-Spun Scaffolds (Biomaterial)—A Case Study. J. Mater. Sci. Mater. Med. 2018, 29, 51. [Google Scholar] [CrossRef] [PubMed]
- Amorim, M.J.B.; Roca, C.P.; Scott-Fordsmand, J.J. Effect Assessment of Engineered Nanoparticles in Solid Media—Current Insight and the Way Forward. Environ. Pollut. 2016, 218, 1370–1375. [Google Scholar] [CrossRef] [PubMed]
- Bicho, R.C.; Santos, F.C.F.; Scott-Fordsmand, J.J.; Amorim, M.J.B. Multigenerational Effects of Copper Nanomaterials (CuONMs) Are Different of Those of CuCl2: Exposure in the Soil Invertebrate Enchytraeus Crypticus. Sci. Rep. 2017, 7, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bicho, R.C.; Ribeiro, T.; Rodrigues, N.P.; Scott-Fordsmand, J.J.; Amorim, M.J.B. Effects of Ag Nanomaterials (NM300K) and Ag Salt (AgNO3) Can Be Discriminated in a Full Life Cycle Long Term Test with Enchytraeus Crypticus. J. Hazard. Mater. 2016, 318, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, M.F.M.; Gomes, S.I.L.; Scott-Fordsmand, J.J.; Amorim, M.J.B. Shorter Lifetime of a Soil Invertebrate Species When Exposed to Copper Oxide Nanoparticles in a Full Lifespan Exposure Test. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendes, L.A.; Amorim, M.J.B.; Scott-Fordsmand, J.J. Interactions of Soil Species Exposed to CuO NMs Are Different from Cu Salt: A Multispecies Test. Environ. Sci. Technol. 2018, 52, 4413–4421. [Google Scholar] [CrossRef] [PubMed]
- Gomes, S.I.L.; Roca, C.P.; Pegoraro, N.; Trindade, T.; Scott-Fordsmand, J.J.; Amorim, M.J.B. High-Throughput Tool to Discriminate Effects of NMs (Cu-NPs, Cu-Nanowires, CuNO3, and Cu Salt Aged): Transcriptomics in Enchytraeus Crypticus. Nanotoxicology 2018, 12, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Maria, V.L.; Licha, D.; Ranninger, C.; Scott-Fordsmand, J.J.; Huber, C.G.; Amorim, M.J.B. The Enchytraeus Crypticus Stress Metabolome–CuO NM Case Study. Nanotoxicology 2018, 12, 766–780. [Google Scholar] [CrossRef]
- Europeand Food Safety Authority; Aguilera, J.; Aguilera-Gomez, M.; Barrucci, F.; Cocconcelli, P.S.; Davies, H.; Denslow, N.; Lou Dorne, J.; Grohmann, L.; Herman, L.; et al. EFSA Scientific Colloquium 24—omics in Risk Assessment: State of the Art and next Steps. EFSA Support. Publ. 2018, 15, 1512. [Google Scholar] [CrossRef] [Green Version]
- Hund-Rinke, K.; Baun, A.; Cupi, D.; Fernandes, T.F.; Handy, R.; Kinross, J.M.N.; Peijnenburg, W.; Schlich, K.; Shaw, B.J.; Scott-Fordsmand, J.J. Regulatory Ecotoxicity Testing of Nanomaterials—Proposed Modifications of OECD Test Guidelines Based on Laboratory Experience with Silver and Titanium Dioxide Nanoparticles. Nanotoxicology 2016, 10, 1442–1447. [Google Scholar] [CrossRef] [Green Version]
- Amorim, M.J.B.; Lin, S.; Schlich, K.; Navas, J.M.; Brunelli, A.; Neubauer, N.; Vilsmeier, K.; Costa, A.L.; Gondikas, A.; Xia, T.; et al. Environmental Impacts by Fragments Released from Nanoenabled Products: A Multiassay, Multimaterial Exploration by the SUN Approach. Environ. Sci. Technol. 2018, 52, 1514–1524. [Google Scholar] [CrossRef] [Green Version]
- Scott-Fordsmand, J.J.; Pozzi-Mucelli, S.; Tran, L.; Aschberger, K.; Sabella, S.; Vogel, U.; Poland, C.; Balharry, D.; Fernandes, T.; Gottardo, S.; et al. A Unified Framework for Nanosafety Is Needed. Nano Today 2014, 9, 546–549. [Google Scholar] [CrossRef]
- Scott-Fordsmand, J.J.; Peijnenburg, W.J.G.M.; Semenzin, E.; Nowack, B.; Hunt, N.; Hristozov, D.; Marcomini, A.; Irfan, M.A.; Jiménez, A.S.; Landsiedel, R.; et al. Environmental Risk Assessment Strategy for Nanomaterials. Int. J. Environ. Res. Public Health 2017, 14, 1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semenzin, E.; Lanzellotto, E.; Hristozov, D.; Critto, A.; Zabeo, A.; Giubilato, E.; Marcomini, A. Species Sensitivity Weighted Distribution for Ecological Risk Assessment of Engineered Nanomaterials: The n-TiO2 Case Study. Environ. Toxicol. Chem. 2015, 34, 2644–2659. [Google Scholar] [CrossRef] [PubMed]
- Oksel, C.; Ma, C.Y.; Wang, X.Z. Structure-Activity Relationship Models for Hazard Assessment and Risk Management of Engineered Nanomaterials. Procedia Eng. 2015, 102, 1500–1510. [Google Scholar] [CrossRef] [Green Version]
- Scott-Fordsmand, J.J.; Amorim, M.J.B.; Sørensen, P.B. Implementing the DF4 in a Robust Model, Allowing for Enhanced Comparison, Prioritisation and Grouping of Nanomaterials. Regul. Toxicol. Pharmacol. 2018, 92, 207–212. [Google Scholar] [CrossRef]
- Hayashi, Y.; Miclaus, T.; Engelmann, P.; Autrup, H.; Sutherland, D.S.; Scott-Fordsmand, J.J. Nanosilver Pathophysiology in Earthworms: Transcriptional Profiling of Secretory Proteins and the Implication for the Protein Corona. Nanotoxicology 2015, 5390, 1–9. [Google Scholar] [CrossRef]
- Petersen, E.J.; Mortimer, M.; Burgess, R.M.; Handy, R.; Hanna, S.; Ho, K.T.; Johnson, M.; Loureiro, S.; Selck, H.; Scott-Fordsmand, J.J.; et al. Strategies for Robust and Accurate Experimental Approaches to Quantify Nanomaterial Bioaccumulation across a Broad Range of Organisms. Environ. Sci. Nano 2019, 6, 1619–1656. [Google Scholar] [CrossRef]
- Navratilova, J.; Praetorius, A.; Gondikas, A.; Fabienke, W.; von der Kammer, F.; Hofmann, T. Detection of Engineered Copper Nanoparticles in Soil Using Single Particle ICP-MS. Int. J. Environ. Res. Public Health 2015, 12, 15756–15768. [Google Scholar] [CrossRef] [Green Version]
- Montaño, M.D.; Lowry, G.V.; Von Der Kammer, F.; Blue, J.; Ranville, J.F. Current Status and Future Direction for Examining Engineered Nanoparticles in Natural Systems. Environ. Chem. 2014, 11, 351–366. [Google Scholar] [CrossRef]
- Nowack, B. Evaluation of Environmental Exposure Models for Engineered Nanomaterials in a Regulatory Context. NanoImpact 2017, 8, 38–47. [Google Scholar] [CrossRef]
- Gottschalk, F.; Scholz, R.W.; Nowack, B. Probabilistic Material Flow Modeling for Assessing the Environmental Exposure to Compounds: Methodology and an Application to Engineered Nano-TiO2 Particles. Environ. Model. Softw. 2010, 25, 320–332. [Google Scholar] [CrossRef]
- Sun, T.Y.; Gottschalk, F.; Hungerbühler, K.; Nowack, B. Comprehensive Probabilistic Modelling of Environmental Emissions of Engineered Nanomaterials. Environ. Pollut. 2014, 185, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.Y.; Mitrano, D.M.; Bornhöft, N.A.; Scheringer, M.; Hungerbühler, K.; Nowack, B. Envisioning Nano Release Dynamics in a Changing World: Using Dynamic Probabilistic Modeling to Assess Future Environmental Emissions of Engineered Nanomaterials. Environ. Sci. Technol. 2017, 51, 2854–2863. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Nowack, B. Environmental Risk Assessment of Engineered Nano-SiO2, Nano Iron Oxides, Nano-CeO2, Nano-Al2O3, and Quantum Dots. Environ. Toxicol. Chem. 2018, 37, 1387–1395. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Kalinina, A.; Sun, T.; Nowack, B. Probabilistic Modeling of the Flows and Environmental Risks of Nano-Silica. Sci. Total Environ. 2016, 545–546, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Adam, V.; Caballero-Guzman, A.; Nowack, B. Considering the Forms of Released Engineered Nanomaterials in Probabilistic Material Flow Analysis. Environ. Pollut. 2018, 243, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Mahapatra, I.; Sun, T.Y.; Clark, J.R.A.; Dobson, P.J.; Hungerbuehler, K.; Owen, R.; Nowack, B.; Lead, J. Probabilistic Modelling of Prospective Environmental Concentrations of Gold Nanoparticles from Medical Applications as a Basis for Risk Assessment. J. Nanobiotechnol. 2015, 13, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Arvidsson, R.; Molander, S.; Sandén, B.A. Impacts of a Silver-Coated Future: Particle Flow Analysis of Silver Nanoparticles. J. Ind. Ecol. 2011, 15, 844–854. [Google Scholar] [CrossRef]
- Meesters, J.A.J.; Koelmans, A.A.; Quik, J.T.K.; Hendriks, A.J.; Van De Meent, D. Multimedia Modeling of Engineered Nanoparticles with SimpleBox4nano: Model Definition and Evaluation. Environ. Sci. Technol. 2014, 48, 5726–5736. [Google Scholar] [CrossRef]
- Liu, H.H.; Cohen, Y. Multimedia Environmental Distribution of Nanomaterials (MendNano). In Technical Proceedings of the 2012 NSTI Nanotechnology Conference and Expo; CRC Press: Boca Raton, FL, USA, 2012; pp. 304–306. [Google Scholar]
- Geitner, N.K.; Ogilvie Hendren, C.; Cornelis, G.; Kaegi, R.; Lead, J.R.; Lowry, G.V.; Lynch, I.; Nowack, B.; Petersen, E.; Bernhardt, E.; et al. Harmonizing across Environmental Nanomaterial Testing Media for Increased Comparability of Nanomaterial Datasets. Environ. Sci. Nano 2020, 7, 13–36. [Google Scholar] [CrossRef] [Green Version]
- Hendren, C.O.; Lowry, G.V.; Unrine, J.M.; Wiesner, M.R. A Functional Assay-Based Strategy for Nanomaterial Risk Forecasting. Sci. Total Environ. 2015, 536, 1029–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauser, M.; Li, G.; Nowack, B. Environmental Hazard Assessment for Polymeric and Inorganic Nanobiomaterials Used in Drug Delivery. J. Nanobiotechnol. 2019, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- European Committee for Standardization (CEN). CEN TS 17274:2018: Nanotechnologies—Guidelines for Determining Protocols for the Explosivity and Flammability of Powders Containing Nano-Objects (for Transport, Handling and Storage); CEN: Brussels, Belgium, 2018.
- National Institute for Occupational Safety and Health (NIOSH). Current Strategies for Engineering Controls in Nanomaterial Production and Downstream Handling Processes. Publication No. 2014–102; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health: Washington, DC, USA, 2013; pp. 1–95.
- Wang, X.Z.; Yang, Y.; Li, R.; Mcguinnes, C.; Adamson, J.; Megson, I.L.; Donaldson, K. Principal Component and Causal Analysis of Structural and Acute in Vitro Toxicity Data for Nanoparticles. Nanotoxicology 2014, 8, 465–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, A.L. Applying Safety by Molecular Design Concepts to Nanomaterials Risk Management. In Managing Risk in Nanotechnology: Topics in Governance, Assurance and Transfer; Murphy, F., McAlea, E.M., Mullins, M., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 171–195. [Google Scholar] [CrossRef]
- Brunelli, A.; Zabeo, A.; Semenzin, E.; Hristozov, D.; Marcomini, A. Extrapolated Long-Term Stability of Titanium Dioxide Nanoparticles and Multi-Walled Carbon Nanotubes in Artificial Freshwater. J. Nanopart. Res. 2016, 18, 113. [Google Scholar] [CrossRef]
- Le, T.C.; Yin, H.; Chen, R.; Chen, Y.; Zhao, L.; Casey, P.S.; Chen, C.; Winkler, D.A. An Experimental and Computational Approach to the Development of ZnO Nanoparticles That Are Safe by Design. Small 2016, 12, 3568–3577. [Google Scholar] [CrossRef]
- Hjorth, R.; van Hove, L.; Wickson, F. What Can Nanosafety Learn from Drug Development? The Feasibility of “Safety by Design”. Nanotoxicology 2017, 11, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Gottardo, S.; Crutzen, H.; Jantunen, P. (Eds.) NANoREG Framework for the Safety Assessment of Nanomaterials; JRC Science for Policy Report; European Commission—Joint Research Centre: Ispra, Italy, 2017.
- Joint EASAC-JRC Report. Impact of Engineered Nanomaterials on Health: Considerations for Benefit-Risk Assessment; Publications Office of the European Union: Luxembourg, 2011. [CrossRef]
- Besson, J.P.; King, P.W.B.; Wilkins, T.A.; McIvor, M.C.; Everall, N.J. European Patent Application EP 0 767 222 A2, Calcination of Titanium Dioxide; European Patent Office: Munich, Germany, 1996.
- U.S. Food and Drug Administration (FDA). Guidance for Industry, PAT-A Framework for Innovative Pharmaceutical Development, Manufacturing and Quality Assurance; U.S. Food and Drug Administration: Silver Spring, MD, USA, 2004.
- Brenderlberger, G. New PAT (Process Analytical Technology) Draft Guidance from FDA; U.S. Food and Drug Administration: Washinton, DC, USA, 2003.
- Strube, J.; Ditz, R.; Kornecki, M.; Huter, M.; Schmidt, A.; Thiess, H.; Zobel-Roos, S. Process Intensification in Biologics Manufacturing. Chem. Eng. Process. Process Intensif. 2018, 133, 278–293. [Google Scholar] [CrossRef]
- Babi, D.K.; Cruz, M.S.; Gni, R. Fundaments of Process Intensification: A Process Systems Engineering View. In Process Intensification in Chemical Engineering: Design Optimization and Control; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Tantra, R.; Oksel, C.; Puzyn, T.; Wang, J.; Robinson, K.N.; Wang, X.Z.; Ma, C.Y.; Wilkins, T. Nano(Q)SAR: Challenges, Pitfalls and Perspectives. Nanotoxicology 2015, 9, 636–642. [Google Scholar] [CrossRef] [Green Version]
- Oksel, C.; Winkler, D.A.; Ma, C.Y.; Wilkins, T.; Wang, X.Z. Accurate and interpretable nanoSAR models from genetic programming-based decision tree construction approaches. Nanotoxicology 2016, 10, 1001–1012. [Google Scholar] [CrossRef]
- Gajewicz, A.; Puzyn, T.; Odziomek, K.; Urbaszek, P.; Haase, A.; Riebeling, C.; Luch, A.; Irfan, M.A.; Landsiedel, R.; van der Zande, M.; et al. Decision Tree Models to Classify Nanomaterials According to the DF4nanoGrouping Scheme. Nanotoxicology 2018, 12, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Vazquez-Vazquez, F.C.; Chanes-Cuevas, O.A.; Masuoka, D.; Alatorre, J.A.; Chavarria-Bolaños, D.; Vega-Baudrit, J.R.; Serrano-Bello, J.; Alvarez-Perez, M.A. Biocompatibility of Developing 3D-Printed Tubular Scaffold Coated with Nanofibers for Bone Applications. J. Nanomater. 2019. [Google Scholar] [CrossRef] [Green Version]
- European Medicines Agency (EMA). Reflection Paper on the Data Requirements for Intravenous Iron-Based Nano-Colloidal Products Developed with Reference to an Innovator Medicinal Product; EMA: London, UK, 2015; Volume 44.
- Boisseau, P.; Loubaton, B. Nanomedicine, Nanotechnology in Medicine. Comptes Rendus Phys. 2011, 12, 620–636. [Google Scholar] [CrossRef] [Green Version]
- European Medicines Agency (EMA). European Medicines Agency Benefit-Risk Methodology Project- Description of the Current Practice of Benefit-Risk Assessment for Cetralised Procedure Products in the EU Regulatory Network—Summary of Original Report. Reproduction 2010, 44, 2–4. [Google Scholar]
- Hughes, D.; Mt-Isa, S.; Chan, E.; Downey, G.; Hallgreen, C.E.; Hockley, K.S.; Juhaeri, J.; Lieftucht, A.; Metcalfe, M.A.; Noel, R.A.; et al. IMI-PROTECT Benefit-Risk Group Recommendations Report. Recommendations for the Methodology and Visualisation Techniques to Be Used in the Assessment of Benefit and Risk of Medicines. 2013. Available online: http://www.imi-protect.eu/documents/HughesetalRecommendationsforthemethodologyandvisualisationtechniquestobeusedintheassessmento.pdf (accessed on 30 September 2020).
- European Medicines Agency (EMA). Benefit-Risk Methodology Project—Work Package 2 Report: Applicability of Current Tools and Processes for Regulatory Benefit-Risk Assessment; European Medicines Agency: London, UK, 2011.
- Coplan, P.M.; Noel, R.A.; Levitan, B.S.; Ferguson, J.; Mussen, F. Development of a Framework for Enhancing the Transparency, Reproducibility and Communication of the Benefit-Risk Balance of Medicines. Clin. Pharmacol. Ther. 2011, 89, 312–315. [Google Scholar] [CrossRef]
- European Medicines Agency (EMA). Reflection Paper on Benefit-Risk Assessment Methods in the Context of the Evaluation of Marketing Authorisation Applications of Medicinal Products for Human Use; European Medicines Agency: London, UK, 2008.
- U.S. Food and Drug Administration (FDA). Benefit-Risk Assessment in Drug Regulatory Decision-Making; U.S. Food and Drug Administration: Washinton, DC, USA, 2018.
- European Medicines Agency (EMA). Guideline on Safety and Efficacy Follow-Up—Risk Management of Advanced Therapy Medicinal Products; European Medicines Agency: London, UK, 2008.
- Andrade, E.L.; Bento, A.F.; Cavalli, J.; Oliveira, S.K.; Freitas, C.S.; Marcon, R.; Schwanke, R.C.; Siqueira, J.M.; Calixto, J.B. Non-Clinical Studies Required for New Drug Development—Part I: Early in Silico and in Vitro Studies, New Target Discovery and Validation, Proof of Principles and Robustness of Animal Studies. Braz. J. Med. Biol. Res. 2016, 49, e5644. [Google Scholar] [CrossRef] [Green Version]
- Sashegyi, A.; Felli, J.; Noel, R. Benefit-Risk Assessment in Pharmaceutical Research and Development; Chapman and Hall/CRC Biostatistics Series; CRC Press, Taylor and Francis Group: Boca Raton, FL, USA, 2014; Volume 13. [Google Scholar] [CrossRef]
- Pane, J.; Francisca, R.D.C.; Verhamme, K.M.C.; Orozco, M.; Viroux, H.; Rebollo, I.; Sturkenboom, M.C.J.M. EU Postmarket Surveillance Plans for Medical Devices. Pharmacoepidemiol. Drug Saf. 2019, 28, 1155–1165. [Google Scholar] [CrossRef] [Green Version]
- Mt-Isa, S.; Tzoulaki, I.; Callreus, T.; Micaleff, A.; Ashby, D. Weighing Benefit-Risk of Medicines: Concepts and Approaches. Drug Discov. Today Technol. 2011, 8, 29–35. [Google Scholar] [CrossRef]
- McAuslane, N.; Leong, J.; Liberti, L.; Walker, S. The Benefit-Risk Assessment of Medicines. Ther. Innov. Regul. Sci. 2017, 51, 635–644. [Google Scholar] [CrossRef]
- Leong, J.; Walker, S.; Salek, S. A Practical Approach to Communicating Benefit-Risk Decisions of Medicines to Stakeholders. Front. Pharmacol. 2015, 6, 99. [Google Scholar] [CrossRef] [Green Version]
- International Organization for Standardization (ISO). ISO 9001:2015—Qality Management Systems-Requirements; ISO: Geneva, Switzerland, 2015. [Google Scholar]
- International Organization for Standardization (ISO). ISO 13485:2016 Medical Devices-Quality Management Systems; ISO: Geneva, Switzerland, 2016. [Google Scholar]
- Geremia, F. Quality Aspects for Medical Devices, Quality System and Certification Process. Microchem. J. 2018, 136, 300–306. [Google Scholar] [CrossRef]
- International Organization for Standardization (ISO). ISO 14971:2007 Medical Devices-Application of Risk Management to Medical Devices; ISO: Geneva, Switzerland, 2007. [Google Scholar]
- Bos, P.M.J.; Gottardo, S.; Scott-Fordsm, J.J.; van Tongeren, M.; Semenzin, E.; Fernandes, T.F.; Hristozov, D.; Hund-Rinke, K.; Hunt, N.; Irfan, M.A.; et al. The MARINA Risk Assessment Strategy: A Flexible Strategy for Efficient Information Collection and Risk Assessment of Nanomaterials. Int. J. Environ. Res. Public Health 2015, 12, 15007–15021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seltenrich, N. Nanosilver: Weighling the Risks and Benefits. Environ. Health Perspect. 2013, 121, 220–225. [Google Scholar] [CrossRef]
- Organisation for Economic Co-operation and Development (OECD). Physical-Chemical Decision Framework to Inform Decisions for Risk Assessment of Manufactured Nanomaterials; OECD: Paris, France, 2019.
- Mühlbacher, A.C.; Juhnke, C.; Beyer, A.R.; Garner, S. Patient-Focused Benefit-Risk Analysis to Inform Regulatory Decisions: The European Union Perspective. Value Health 2016, 19, 734–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Product | Life Cycle Stages | Tasks/Activities | Exposure Route | Target |
|---|---|---|---|---|
| ATMP | Synthesis of NBMs | Weighing operations Mixing operations Purification Collection and sorting Packing/re-packing | Inhalation Dermal | Workers in medical research labs |
| Product manufacturing | Dissolution preparation Sampling Packing/re-packing In vitro and In vivo testing Cleaning and maintenance Waste management Collection and sorting Packing/re-packing | Inhalation Dermal | Workers in medical research labs Workers in pharma industry Facility maintenance staff | |
| Use | Flask filling and mixing operation Syringe filling (1–60 mL) Maintenance of drug preparation devices Waste management | Inhalation Dermal | Health care workers Home healthcare workers Waste management workers | |
| End of Life | Handling patient excreta Spills treatments Waste management | Inhalation Dermal | Health care workers Waste management workers | |
| MD | Synthesis of NBMs | Weighing operations Mixing operations Purification Collection and sorting Packing/re-packing | Inhalation Dermal | Workers in medical research labs |
| Product manufacturing | NBMs dosage Injection molding Machining and abrasion Mixing operations Film coatings Collection and sorting Packing/re-packing | Inhalation Dermal | Workers in medical research labs Workers in pharma industry Facility maintenance staff | |
| Use | Drilling of tooth Polishing and sanding Application in the body Waste management | Inhalation Dermal | Health care workers Home healthcare workers Waste management workers | |
| End of Life | Handling patient excreta Waste management | Dermal | Waste management workers |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giubilato, E.; Cazzagon, V.; Amorim, M.J.B.; Blosi, M.; Bouillard, J.; Bouwmeester, H.; Costa, A.L.; Fadeel, B.; Fernandes, T.F.; Fito, C.; et al. Risk Management Framework for Nano-Biomaterials Used in Medical Devices and Advanced Therapy Medicinal Products. Materials 2020, 13, 4532. https://doi.org/10.3390/ma13204532
Giubilato E, Cazzagon V, Amorim MJB, Blosi M, Bouillard J, Bouwmeester H, Costa AL, Fadeel B, Fernandes TF, Fito C, et al. Risk Management Framework for Nano-Biomaterials Used in Medical Devices and Advanced Therapy Medicinal Products. Materials. 2020; 13(20):4532. https://doi.org/10.3390/ma13204532
Chicago/Turabian StyleGiubilato, Elisa, Virginia Cazzagon, Mónica J. B. Amorim, Magda Blosi, Jacques Bouillard, Hans Bouwmeester, Anna Luisa Costa, Bengt Fadeel, Teresa F. Fernandes, Carlos Fito, and et al. 2020. "Risk Management Framework for Nano-Biomaterials Used in Medical Devices and Advanced Therapy Medicinal Products" Materials 13, no. 20: 4532. https://doi.org/10.3390/ma13204532