
Efficacy and Failure Patterns of Early SBRT to the Primary Tumor in Advanced EGFR-Mutation-Positive Lung Cancer with EFGR-TKI Treatment: A Prospective, Single Arm, Phase II Study
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Treatment
2.3. Assessments
2.4. Endpoints
2.5. Statistical Analysis
3. Results
3.1. Patients
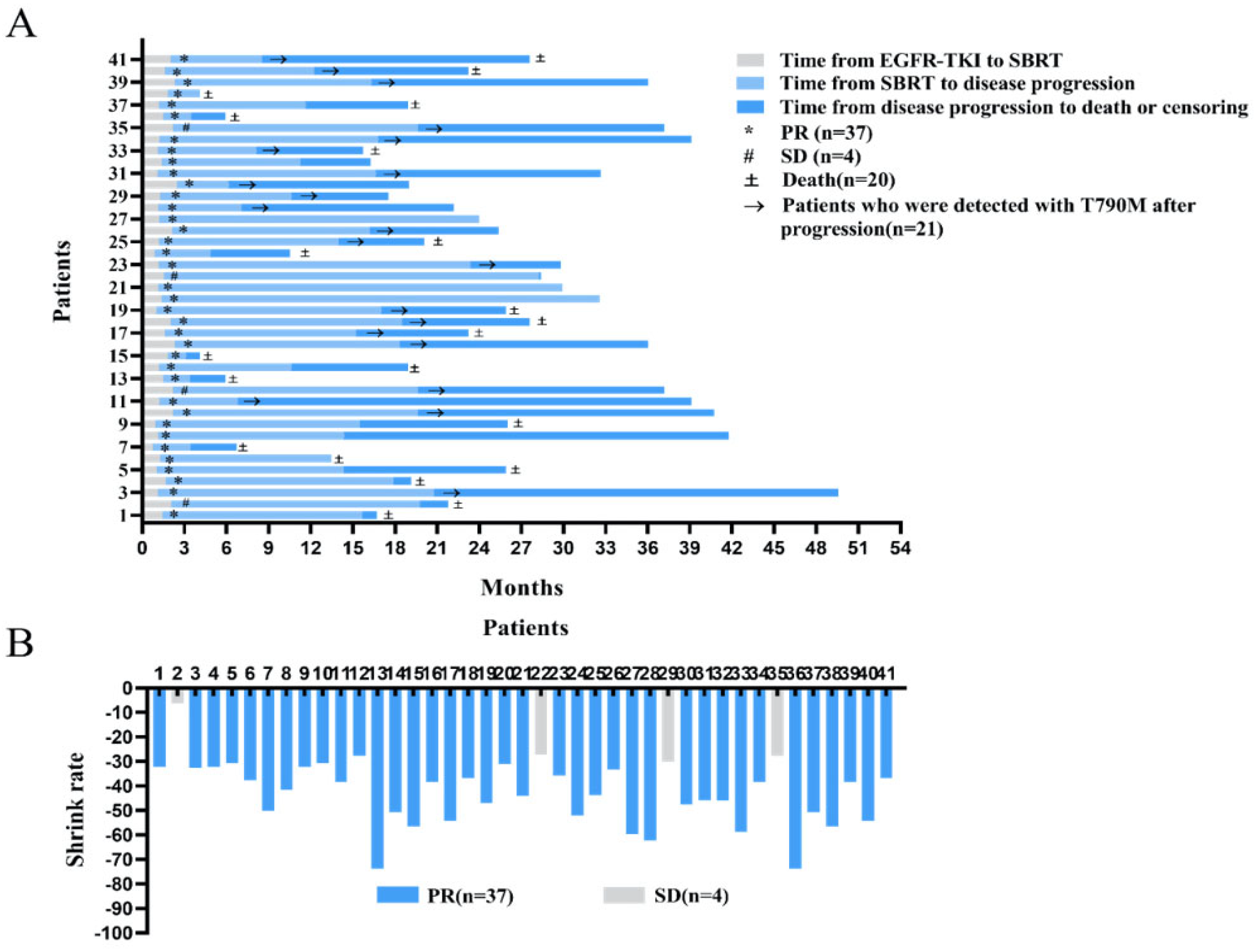
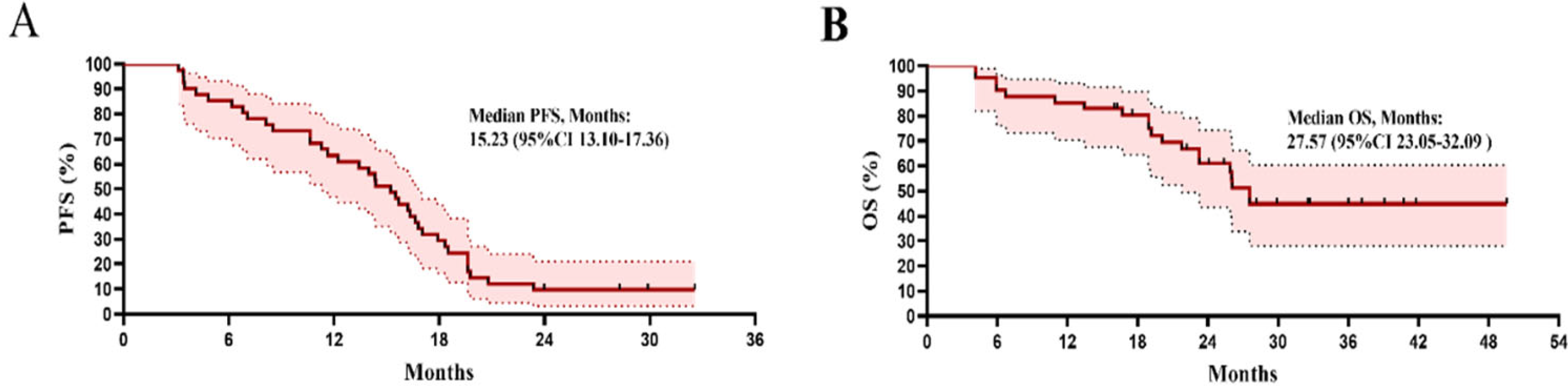
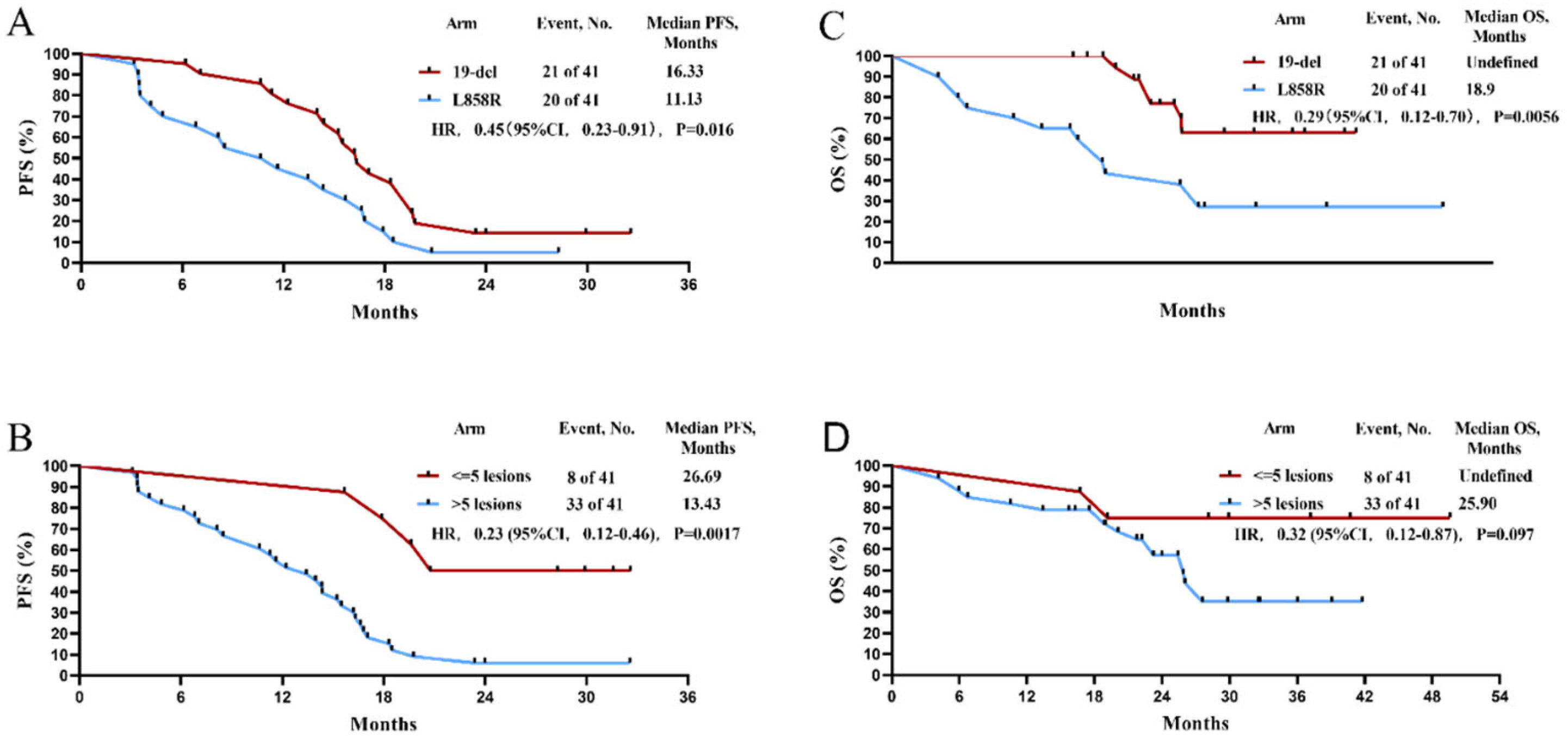
3.2. Efficacy
3.3. Safety
3.4. Patterns of Failure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Ye, M.; Wu, X.; Lv, D.; Kong, F.; Yang, H. P1.15-32 Real World EGFR Mutation Profile from 1699 Non-Small Cell Lung Cancer Patients in Eastern China. J. Thorac. Oncol. 2018, 13, S625–S626. [Google Scholar] [CrossRef] [Green Version]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. Non-Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2022, 20, 497–530. [Google Scholar] [CrossRef] [PubMed]
- Mitsudomi, T.; Morita, S.; Yatabe, Y.; Negoro, S.; Okamoto, I.; Tsurutani, J.; Seto, T.; Satouchi, M.; Tada, H.; Hirashima, T.; et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): An open label, randomised phase 3 trial. Lancet Oncol. 2010, 11, 121–128. [Google Scholar] [CrossRef]
- Zhong, W.Z.; Chen, K.N.; Chen, C.; Gu, C.D.; Wang, J.; Yang, X.N.; Mao, W.M.; Wang, Q.; Qiao, G.B.; Cheng, Y.; et al. Erlotinib Versus Gemcitabine Plus Cisplatin as Neoadjuvant Treatment of Stage IIIA-N2 EGFR-Mutant Non-Small-Cell Lung Cancer (EMERGING-CTONG 1103): A Randomized Phase II Study. J. Clin. Oncol. 2019, 37, 2235–2245. [Google Scholar] [CrossRef]
- Zhong, W.-Z.; Zhou, Q.; Wu, Y.-L. The resistance mechanisms and treatment strategies for EGFR -mutant advanced non-small-cell lung cancer. Oncotarget 2017, 8, 71358. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Wang, J.; Zhang, G.; Li, Y.; Lin, L.; Yang, H.; Zhou, J.; Zhang, L.; Lv, D. Detection of plasma T790M mutation after the first generation EGFR-TKI resistance of non-small cell lung cancer in the real world. J. Thorac. Dis. 2020, 12, 550–557. [Google Scholar] [CrossRef]
- Patel, S.H.; Rimner, A.; Foster, A.; Zhang, Z.; Woo, K.M.; Yu, H.A.; Riely, G.J.; Wu, A.J. Patterns of initial and intracranial failure in metastatic EGFR-mutant non-small cell lung cancer treated with erlotinib. Lung Cancer 2017, 108, 109–114. [Google Scholar] [CrossRef]
- Al-Halabi, H.; Sayegh, K.; Digamurthy, S.R.; Niemierko, A.; Piotrowska, Z.; Willers, H.; Sequist, L.V. Pattern of Failure Analysis in Metastatic EGFR-Mutant Lung Cancer Treated with Tyrosine Kinase Inhibitors to Identify Candidates for Consolidation Stereotactic Body Radiation Therapy. J. Thorac. Oncol. 2015, 10, 1601–1607. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Zheng, X.; Huang, H.; Wu, K.; Wang, B.; Chen, X.; Ma, S. Afatinib increases sensitivity to radiation in non-small cell lung cancer cells with acquired EGFR T790M mutation. Oncotarget 2015, 6, 5832–5845. [Google Scholar] [CrossRef]
- Chang, J.Y.; Senan, S.; Paul, M.A.; Mehran, R.J.; Louie, A.V.; Balter, P.; Groen, H.J.; McRae, S.E.; Widder, J.; Feng, L.; et al. Stereotactic ablative radiotherapy versus lobectomy for operable stage I non-small-cell lung cancer: A pooled analysis of two randomised trials. Lancet Oncol. 2015, 16, 630–637. [Google Scholar] [CrossRef] [Green Version]
- Scotti, V.; Bruni, A.; Francolini, G.; Perna, M.; Vasilyeva, P.; Loi, M.; Simontacchi, G.; Viggiano, D.; Lanfranchi, B.; Gonfiotti, A.; et al. Stereotactic Ablative Radiotherapy as an Alternative to Lobectomy in Patients with Medically Operable Stage I NSCLC: A Retrospective, Multicenter Analysis. Clin. Lung Cancer 2019, 20, e53–e61. [Google Scholar] [CrossRef] [PubMed]
- Cuccia, F.; Mazzola, R.; Figlia, V.; Giaj-Levra, N.; Nicosia, L.; Ricchetti, F.; Rigo, M.; Attina, G.; Vitale, C.; Pastorello, E.; et al. Stereotactic body radiotherapy for pulmonary oligometastases: A monoinstitutional analysis of clinical outcomes and potential prognostic factors. Strahlenther. Onkol. 2022, 198, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Figlia, V.; Mazzola, R.; Cuccia, F.; Alongi, F.; Mortellaro, G.; Cespuglio, D.; Cucchiara, T.; Iacoviello, G.; Valenti, V.; Molino, M.; et al. Hypo-fractionated stereotactic radiation therapy for lung malignancies by means of helical tomotherapy: Report of feasibility by a single-center experience. Radiol. Med. 2018, 123, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.M.; Ten Haken, R.K.; Schipper, M.; Frey, K.A.; Hayman, J.; Gross, M.; Ramnath, N.; Hassan, K.A.; Matuszak, M.; Ritter, T.; et al. Effect of Midtreatment PET/CT-Adapted Radiation Therapy with Concurrent Chemotherapy in Patients with Locally Advanced Non-Small-Cell Lung Cancer: A Phase 2 Clinical Trial. JAMA Oncol. 2017, 3, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Wujanto, C.; Vellayappan, B.; Siva, S.; Louie, A.V.; Guckenberger, M.; Slotman, B.J.; Onishi, H.; Nagata, Y.; Liu, M.; Lo, S.S. Stereotactic Body Radiotherapy for Oligometastatic Disease in Non-small Cell Lung Cancer. Front. Oncol. 2019, 9, 1219. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): A randomised, phase 2, open-label trial. Lancet 2019, 393, 2051–2058. [Google Scholar] [CrossRef]
- Kissel, M.; Martel-Lafay, I.; Lequesne, J.; Faivre, J.C.; Le Pechoux, C.; Stefan, D.; Barraux, V.; Loiseau, C.; Grellard, J.M.; Danhier, S.; et al. Stereotactic ablative radiotherapy and systemic treatments for extracerebral oligometastases, oligorecurrence, oligopersistence and oligoprogression from lung cancer. BMC Cancer 2019, 19, 1237. [Google Scholar] [CrossRef]
- Wei, H.; Zhou, X.; Yang, H.; Gong, Y.; Wang, J.; Xu, Y.; Zhou, L.; Xue, J.; Zou, B.; Zhang, Y.; et al. Stereotactic body radiotherapy to the primary lung lesion improves the survival of the selected patients with non-oligometastatic NSCLC harboring EGFR activating mutation with first-line EGFR-TKIs: A real-world study. J. Cancer Res. Clin. Oncol. 2022, 148, 2589–2598. [Google Scholar] [CrossRef]
- Zheng, L.; Wang, Y.; Xu, Z.; Yang, Q.; Zhu, G.; Liao, X.Y.; Chen, X.; Zhu, B.; Duan, Y.; Sun, J. Concurrent EGFR-TKI and Thoracic Radiotherapy as First-Line Treatment for Stage IV Non-Small Cell Lung Cancer Harboring EGFR Active Mutations. Oncologist 2019, 24, 1031-e612. [Google Scholar] [CrossRef]
- Wang, X.S.; Bai, Y.F.; Verma, V.; Yu, R.L.; Tian, W.; Ao, R.; Deng, Y.; Xia, J.L.; Zhu, X.Q.; Liu, H.; et al. Randomized Trial of First-Line Tyrosine Kinase Inhibitor with or without Radiotherapy for Synchronous Oligometastatic EGFR-Mutated NSCLC. J. Natl. Cancer Inst. 2022, djac015. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Dong, Q.; Wang, W.; Tang, X.; Meng, Y.; Kong, F.; Yang, H. P2.01-124 SIB-IMRT in Symptomatic Brain Metastases for NSCLC: A Randomized Controlled Study of WBRT Comparing 25Gy and 30Gy. J. Thorac. Oncol. 2018, 13, S712–S713. [Google Scholar] [CrossRef] [Green Version]
- Tang, X.; Shen, Y.; Meng, Y.; Hou, L.; Zhou, C.; Yu, C.; Jia, H.; Wang, W.; Ren, G.; Cai, J.; et al. Radiation-induced lung damage in patients treated with stereotactic body radiotherapy after EGFR-TKIs: Is there any difference from stereotactic body radiotherapy alone? Ann. Palliat. Med. 2021, 10, 2832–2842. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Xia, B.; Xie, R.; Xu, X.; Zhang, M.; Wu, K.; Wang, B.; Ma, S. Timing in combination with radiotherapy and patterns of disease progression in non-small cell lung cancer treated with EGFR-TKI. Lung Cancer 2020, 140, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Fukuhara, T.; Furuya, N.; Watanabe, K.; Sugawara, S.; Iwasawa, S.; Tsunezuka, Y.; Yamaguchi, O.; Okada, M.; Yoshimori, K.; et al. Erlotinib plus bevacizumab versus erlotinib alone in patients with EGFR-positive advanced non-squamous non-small-cell lung cancer (NEJ026): Interim analysis of an open-label, randomised, multicentre, phase 3 trial. Lancet Oncol. 2019, 20, 625–635. [Google Scholar] [CrossRef]
- Yu, H.A.; Sima, C.S.; Huang, J.; Solomon, S.B.; Rimner, A.; Paik, P.; Pietanza, M.C.; Azzoli, C.G.; Rizvi, N.A.; Krug, L.M.; et al. Local therapy with continued EGFR tyrosine kinase inhibitor therapy as a treatment strategy in EGFR-mutant advanced lung cancers that have developed acquired resistance to EGFR tyrosine kinase inhibitors. J. Thorac. Oncol. 2013, 8, 346–351. [Google Scholar] [CrossRef] [Green Version]
- Xu, Q.; Liu, H.; Meng, S.; Jiang, T.; Li, X.; Liang, S.; Ren, S.; Zhou, C. First-line continual EGFR-TKI plus local ablative therapy demonstrated survival benefit in EGFR-mutant NSCLC patients with oligoprogressive disease. J. Cancer 2019, 10, 522–529. [Google Scholar] [CrossRef]
- Xu, Q.; Zhou, F.; Liu, H.; Jiang, T.; Li, X.; Xu, Y.; Zhou, C. Consolidative Local Ablative Therapy Improves the Survival of Patients with Synchronous Oligometastatic NSCLC Harboring EGFR Activating Mutation Treated with First-Line EGFR-TKIs. J. Thorac. Oncol. 2018, 13, 1383–1392. [Google Scholar] [CrossRef] [Green Version]
- Bi, N.; Wang, L.; Xu, K.; Ge, H.; E, M.; Zhang, L.; Cao, J.; Zhang, X.; Xia, B.; Zhao, L.; et al. Real-world treatment patterns and clinical outcomes in EGFR-mutant unresectable locally advanced NSCLC (LA-NSCLC): A retrospective multicenter study of 367 patients. J. Clin. Oncol. 2020, 38, 9047. [Google Scholar] [CrossRef]
- Campo, M.; Al-Halabi, H.; Khandekar, M.; Shaw, A.T.; Sequist, L.V.; Willers, H. Integration of Stereotactic Body Radiation Therapy with Tyrosine Kinase Inhibitors in Stage IV Oncogene-Driven Lung Cancer. Oncologist 2016, 21, 964–973. [Google Scholar] [CrossRef]
- Wu, T.H.; Hsiue, E.H.; Lee, J.H.; Lin, C.C.; Liao, W.Y.; Ho, C.C.; Shih, J.Y.; Yu, C.J.; Yang, J.C. Best Response According to RECIST During First-line EGFR-TKI Treatment Predicts Survival in EGFR Mutation-positive Non-Small-cell Lung Cancer Patients. Clin. Lung Cancer 2018, 19, e361–e372. [Google Scholar] [CrossRef] [PubMed]
- Peng, P.; Chen, Y.; Han, G.; Meng, R.; Zhang, S.; Liao, Z.; Zhang, Y.; Gong, J.; Xiao, C.; Liu, X.; et al. MA01.09 Concomitant SBRT and EGFR-TKI Versus EGFR-TKI Alone for Oligometastatic NSCLC: A Multicenter, Randomized Phase II Study. J. Thorac. Oncol. 2019, 14, S250–S251. [Google Scholar] [CrossRef]
- Nosaki, K.; Satouchi, M.; Kurata, T.; Yoshida, T.; Okamoto, I.; Katakami, N.; Imamura, F.; Tanaka, K.; Yamane, Y.; Yamamoto, N.; et al. Re-biopsy status among non-small cell lung cancer patients in Japan: A retrospective study. Lung Cancer 2016, 101, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.H.; Hsu, K.H.; Tseng, J.S.; Chen, K.C.; Hsu, C.H.; Su, K.Y.; Chen, J.J.W.; Chen, H.W.; Yu, S.L.; Yang, T.Y.; et al. The Association of Acquired T790M Mutation with Clinical Characteristics after Resistance to First-Line Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitor in Lung Adenocarcinoma. Cancer Res. Treat. 2018, 50, 1294–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Y.; He, Y.; Li, W.; Zhang, H.L.; Zhou, Q.; Wang, B.; Liu, C.; Walding, A.; Saggese, M.; Huang, X.; et al. Osimertinib Versus Comparator EGFR TKI as First-Line Treatment for EGFR-Mutated Advanced NSCLC: FLAURA China, A Randomized Study. Target Oncol. 2021, 16, 165–176. [Google Scholar] [CrossRef]
- Guo, T.; Ni, J.; Yang, X.; Li, Y.; Li, Y.; Zou, L.; Wang, S.; Liu, Q.; Chu, L.; Chu, X.; et al. Pattern of Recurrence Analysis in Metastatic EGFR-Mutant NSCLC Treated with Osimertinib: Implications for Consolidative Stereotactic Body Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 62–71. [Google Scholar] [CrossRef]
- Gavralidis, A.; Gainor, J.F. Immunotherapy in EGFR-Mutant and ALK-Positive Lung Cancer: Implications for Oncogene-Driven Lung Cancer. Cancer J. 2020, 26, 517–524. [Google Scholar] [CrossRef]
- Peng, S.; Wang, R.; Zhang, X.; Ma, Y.; Zhong, L.; Li, K.; Nishiyama, A.; Arai, S.; Yano, S.; Wang, W. EGFR-TKI resistance promotes immune escape in lung cancer via increased PD-L1 expression. Mol. Cancer 2019, 18, 165. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number of Subjects | |
|---|---|---|
| Age | Median, range (years) | 66 (46–75) |
| >66 | 23 | |
| ≤66 | 18 | |
| Sex | Female | 18 |
| Male | 23 | |
| Smoke history | Yes | 16 |
| No | 25 | |
| ECOG PS | 0 | 15 |
| 1 | 26 | |
| Mutation type | L858R | 20 |
| 19-del | 21 | |
| T | T1–2 | 13 |
| T3–4 | 28 | |
| N | N0–1 | 9 |
| N2–3 | 32 | |
| M | 0 | 7 |
| 1 | 34 | |
| Lesions | 1–5 | 1 |
| >5 | 33 | |
| Stage | III | 7 |
| IV | 34 | |
| Initial metastasis | Lung | 20 |
| Brain | 6 | |
| Bone | 21 | |
| Liver | 4 | |
| Adrenal glands | 1 | |
| Regional lymph nodes | 35 | |
| Distant lymph nodes | 1 | |
| Others | 15 |
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | Grade 5 | All (%) | |
|---|---|---|---|---|---|---|
| Radiation pneumonitis | 27 | 8 | 0 | 0 | 0 | 35 (85.37) |
| Radiation esophagitis | 0 | 0 | 0 | 0 | 0 | 0 (0.00) |
| Transaminase increased | 8 | 13 | 0 | 0 | 0 | 21 (51.22) |
| Renal insufficiency | 6 | 0 | 0 | 0 | 0 | 6 (14.63) |
| Rash | 14 | 2 | 0 | 0 | 0 | 16 (39.02) |
| Diarrhea | 4 | 0 | 0 | 0 | 0 | 4 (9.76) |
| Paronychia | 1 | 1 | 0 | 0 | 0 | 2 (4.88) |
| Hypokalemia | 2 | 0 | 0 | 0 | 0 | 2 (4.88) |
| Nausea and vomiting | 1 | 0 | 0 | 0 | 0 | 1 (2.44) |
| Sites of Initial Failure | All Patients (n = 33) | Patients with OF (n = 7) | Patients with NF (n = 22) | Patients with ONF (n = 4) | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| Brain | 11 | 33.33 | 0 | 0 | 10 | 45.45 | 1 | 25 |
| Bone | 12 | 36.36 | 0 | 0 | 9 | 40.90 | 3 | 75 |
| Liver | 2 | 6.06 | 0 | 0 | 2 | 9.09 | 0 | 0 |
| Lung | 19 | 57.58 | 7 | 100 | 8 | 36.36 | 4 | 100 |
| Regional lymph nodes | 3 | 9.09 | 0 | 0 | 0 | 0 | 3 | 75 |
| Others | 4 | 12.12 | 0 | 0 | 1 | 4.55 | 3 | 75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, Y.; Xu, H.; Raynor, W.Y.; Ding, J.; Lin, L.; Zhou, C.; Wang, W.; Meng, Y.; Wu, X.; Chen, X.; et al. Efficacy and Failure Patterns of Early SBRT to the Primary Tumor in Advanced EGFR-Mutation-Positive Lung Cancer with EFGR-TKI Treatment: A Prospective, Single Arm, Phase II Study. Life 2022, 12, 1954. https://doi.org/10.3390/life12121954
Shi Y, Xu H, Raynor WY, Ding J, Lin L, Zhou C, Wang W, Meng Y, Wu X, Chen X, et al. Efficacy and Failure Patterns of Early SBRT to the Primary Tumor in Advanced EGFR-Mutation-Positive Lung Cancer with EFGR-TKI Treatment: A Prospective, Single Arm, Phase II Study. Life. 2022; 12(12):1954. https://doi.org/10.3390/life12121954
Chicago/Turabian StyleShi, Yangyang, Hailing Xu, William Y. Raynor, Jiapei Ding, Ling Lin, Chao Zhou, Wei Wang, Yinnan Meng, Xiaomai Wu, Xiaofeng Chen, and et al. 2022. "Efficacy and Failure Patterns of Early SBRT to the Primary Tumor in Advanced EGFR-Mutation-Positive Lung Cancer with EFGR-TKI Treatment: A Prospective, Single Arm, Phase II Study" Life 12, no. 12: 1954. https://doi.org/10.3390/life12121954