
Long-Term Follow-Up of 12 Patients Treated with Bilateral Pallidal Stimulation for Tardive Dystonia

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
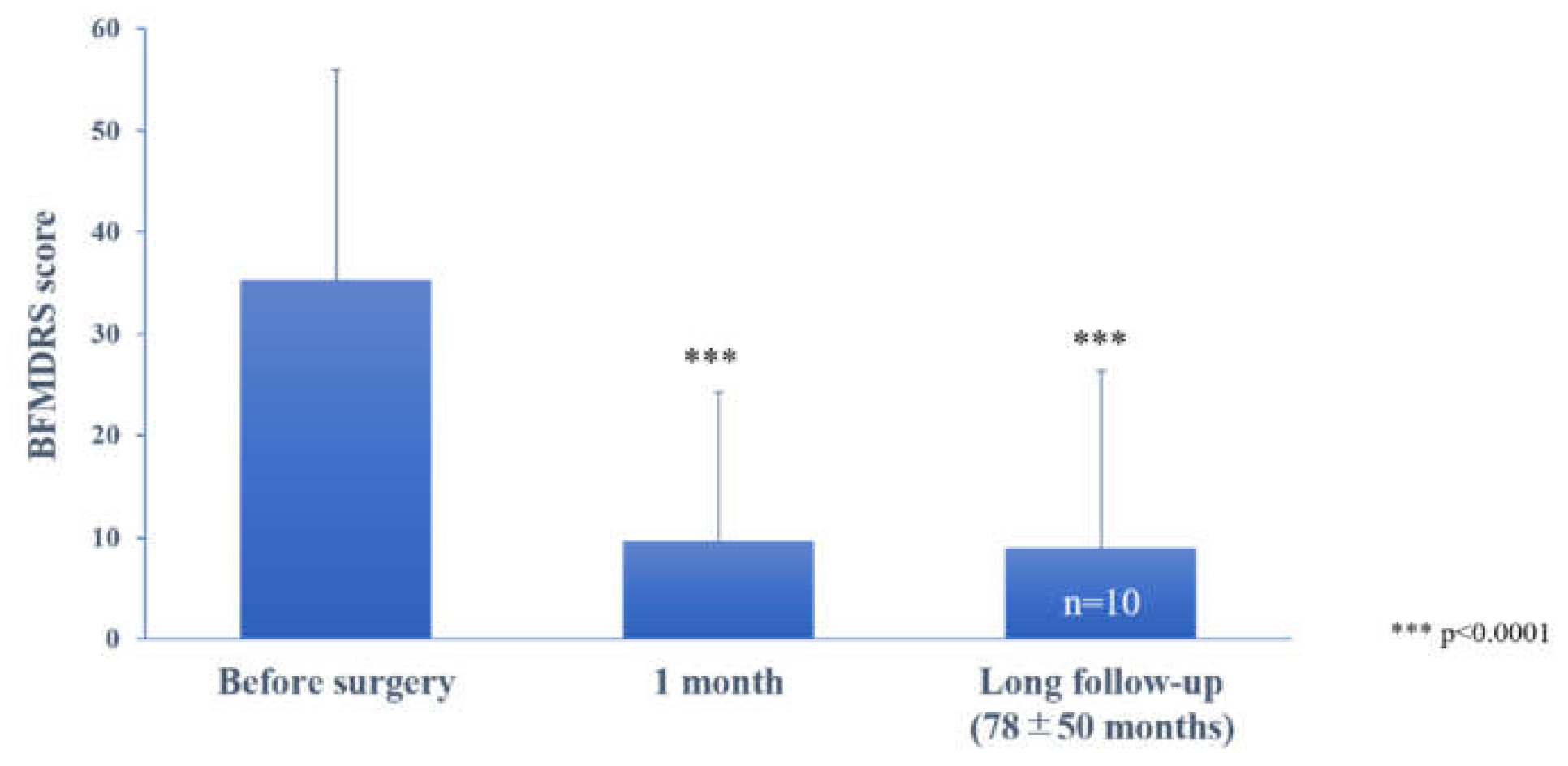
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burke, R.E.; Fahn, S.; Jankovic, J.; Marsden, C.D.; Lang, A.E.; Gollomp, S.; Ilson, J. Tardive dystonia: Late-onset and persistent dystonia caused by antipsychotic drugs. Neurology 1982, 32, 1335. [Google Scholar] [CrossRef] [PubMed]
- Aderibigbe, Y.A.; Jampala, V.C.; Mathews, T. The current status of tardive dystonia. Biol. Psychiatry 1999, 45, 715–730. [Google Scholar]
- Morigaki, R.; Mure, H.; Kaji, R.; Nagahiro, S.; Goto, S. Therapeutic Perspective on Tardive Syndrome with Special Reference to Deep Brain Stimulation. Front. Psychiatry 2016, 7, 207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lerner, P.P.; Miodownik, C.; Lerner, V. Tardive dyskinesia (syndrome): Current concept and modern approaches to its management. Psychiatry Clin. Neurosci. 2015, 69, 321–334. [Google Scholar] [CrossRef] [Green Version]
- Franzini, A.; Marras, C.; Ferroli, P.; Zorzi, G.; Bugiani, O.; Romito, L.; Broggi, G. Long-term high-frequency bilateral pallidal stimulation for neuroleptic-induced tardive dystonia. J. Neurosurg. 2005, 102, 721–725. [Google Scholar] [CrossRef]
- Kiriakakis, V.; Bhatia, K.P.; Quinn, N.P.; Marsden, C.D. The natural history of tardive dystonia. A long-term follow-up study of 107 cases. Brain 1998, 121, 2053–2066. [Google Scholar] [CrossRef] [Green Version]
- Lerner, V.; Miodownik, C. Motor Symptoms of Schizophrenia: Is Tardive Dyskinesia a Symptom or Side Effect? A Modern Treatment. Curr. Psychiatry Rep. 2011, 13, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Ostrem, J.L.; Starr, P.A. Treatment of dystonia with deep brain stimulation. Neurotherapeutics 2008, 5, 320–330. [Google Scholar] [CrossRef] [PubMed]
- Starr, P.A.; Turner, R.S.; Rau, G.; Lindsey, N.; Heath, S.; Volz, M.; Ostrem, J.L.; Marks, W.J. Microelectrode-guided implantation of deep brain stimulators into the globus pallidus internus for dystonia: Techniques, electrode locations, and outcomes. J. Neurosurg. 2006, 104, 488–501. [Google Scholar] [CrossRef] [PubMed]
- Vidailhet, M.; Vercueil, L.; Houeto, J.-L.; Krystkowiak, P.; Benabid, A.-L.; Cornu, P.; Lagrange, C.; Du Montcel, S.T.; Dormont, D.; Grand, S.; et al. Bilateral Deep-Brain Stimulation of the Globus Pallidus in Primary Generalized Dystonia. N. Engl. J. Med. 2005, 352, 459–467. [Google Scholar] [CrossRef] [Green Version]
- Kupsch, A.; Benecke, R.; Müller, J.; Trottenberg, T.; Schneider, G.-H.; Poewe, W.; Eisner, W.; Wolters, A.; Müller, J.-U.; Deuschl, G.; et al. Pallidal Deep-Brain Stimulation in Primary Generalized or Segmental Dystonia. N Engl. J. Med. 2006, 355, 1978–1990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kefalopoulou, Z.; Paschali, A.; Markaki, E.; Vassilakos, P.; Ellul, J.; Constantoyannis, C. A double-blind study on a patient with tardive dyskinesia treated with pallidal deep brain stimulation. Acta Neurol. Scand. 2009, 119, 269–273. [Google Scholar] [CrossRef]
- Magariños-Ascone, C.; Regidor, I.; Gómez-Galán, M.; Cabañes-Martínez, L.; Figueiras-Méndez, R. Deep brain stimulation in the globus pallidus to treat dystonia: Electrophysiological characteristics and 2 years’ follow-up in 10 patients. Neuroscience 2008, 152, 558–571. [Google Scholar] [CrossRef]
- Sako, W.; Goto, S.; Shimazu, H.; Murase, N.; Matsuzaki, K.; Tamura, T.; Mure, H.; Tomogane, Y.; Arita, N.; Yoshikawa, H.; et al. Bilateral deep brain stimulation of the globus pallidus internus in tardive dystonia. Mov. Disord. 2008, 23, 1929–1931. [Google Scholar] [CrossRef] [PubMed]
- Sako, W.; Morigaki, R.; Mizobuchi, Y.; Tsuzuki, T.; Ima, H.; Ushio, Y.; Nagahiro, S.; Kaji, R.; Goto, S. Bilateral pallidal deep brain stimulation in primary Meige syndrome. Park. Relat. Disord. 2011, 17, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Damier, P.; Thobois, S.; Witjas, T.; Cuny, E.; Derost, P.; Raoul, S.; Mertens, P.; Peragut, J.-C.; Lemaire, J.-J.; Burbaud, P.; et al. Bilateral Deep Brain Stimulation of the Globus Pallidus to Treat Tardive Dyskinesia. Arch. Gen. Psychiatry 2007, 64, 170–176. [Google Scholar] [CrossRef] [Green Version]
- Andrews, C.; Aviles-Olmos, I.; Hariz, M.; Foltynie, T. Which patients with dystonia benefit from deep brain stimulation? A metaregression of individual patient outcomes. J. Neurol. Neurosurg. Psychiatry 2010, 81, 1383–1389. [Google Scholar] [CrossRef] [Green Version]
- Alterman, R.L.; Miravite, J.; Weisz, D.; Shils, J.L.; Bressman, S.B.; Tagliati, M. Sixty hertz pallidal deep brain stimulation for primary torsion dystonia. Neurology 2007, 69, 681–688. [Google Scholar] [CrossRef]
- Kupsch, A.; Klaffke, S.; Meissner, W.; Arnold, G.; Schneider, G.H.; Maier-Hauff, K.; Trottenberg, T. The effects of frequency in pallidal deep brain stimulation for primary dystonia. J. Neurol. 2003, 250, 1201–1205. [Google Scholar] [CrossRef]
- Moro, E.; Piboolnurak, P.; Arenovich, T.; Hung, S.W.; Poon, Y.-Y.; Lozano, A.M. Pallidal stimulation in cervical dystonia: Clinical implications of acute changes in stimulation parameters. Eur. J. Neurol. 2009, 16, 506–512. [Google Scholar] [CrossRef]
- Coubes, P.; Cif, L.; El Fertit, H.; Hemm, S.; Vayssiere, N.; Serrat, S.; Picot, M.C.; Tuffery, S.; Claustres, M.; Echenne, B.; et al. Electrical stimulation of the globus pallidus internus in patients with primary generalized dystonia: Long-term results. J. Neurosurg. 2004, 101, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Vercueil, L.; Houeto, J.L.; Krystkowiak, P.; Lagrange, C.; Cassim, F.; Benazzouz, A.; Pidoux, B.; Destée, A.; Agid, Y.; Cornu, P.; et al. Effects of pulse width variations in pallidal stimulation for primary generalized dystonia. J. Neurol. 2007, 254, 1533–1537. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient Number | Age at Surgery | Gender | Age at TD Onset | Underlying Psychiatric Disease and Onset Age | Suspected Drugs | Drug Exposure (Years) | Duration Between TD Onset and DBS (Years) | Region on Dystonia |
|---|---|---|---|---|---|---|---|---|
| 1 | 48 | F | 46 | Depression, 40 | Sulpiride | 2 | 2 | Eye, mouth, neck. |
| 2 | 48 | F | 47 | Bipolar disorder, 40 | Tiapride | 6 | 1 | Neck, bilateral arms, left leg. |
| 3 | 30 | M | 29 | Schizophrenia, 28 | Risperidone | 1 | 0.5 | Left arm, trunk, right leg. |
| 4 | 47 | F | 40 | Panic disorder, 31 | Perphenazine | 5 | 7 | Neck, trunk. |
| 5 | 39 | M | 39 | Depression, 36 | Perphenazine | 0.5 | 0.5 | Neck, right arm, right leg. |
| 6 | 55 | M | NA | Anxiety neurosis, 51 | Haloperidol | 4 | NA | |
| 7 | 42 | M | 41 | Depression, 33 | Sulpiride | 7 | 1 | Neck, mouth, bilateral arms. |
| 8 | 30 | F | 19 | Schizophrenia, 15 | Risperidone Haloperidol | 14 | 11 | Eye, mouth, neck, bilateral legs. |
| 9 | 25 | M | 19 | Schizophrenia, 14 | Risperidone Haloperidol | 11 | 6 | Neck, trunk, bilateral legs. |
| 10 | 69 | M | 59 | Bipolar disorder, 37 | Aripiprazole Quetiapine | 32 | 10 | Neck, trunk |
| 11 | 55 | F | 44 | Schizophrenia, 43 | Risperidone Haloperidol | 10 | 9 | Eye, mouth, neck, trunk |
| 12 | 49 | M | 48 | Schizophrenia, 31 | Risperidone | 17 | 1 | Neck, mouth, bilateral arms. |
| Patient Number | BFMDRS Baseline | BFMDRS 1 Month after DBS | Improvement Rate at 1 Month (%) | BFMDRS at Last Follow-Up | Improvement Rate at Last Follow-Up (%) | Postoperative Follow-Up Time (Months) | Stimulation Parameters with Best Response Amplitude/Frequency (Hz)/Pulse width (μs) |
|---|---|---|---|---|---|---|---|
| 1 | 26 | NA | NA | 3 | 88.5 | 50 | Bilateral 3(+)2(−) 4.4V/60/450 |
| 2 | 21 | 8 | 61.9 | 2 | 90.5 | 88 | Rt. Case(+) 1(−) 2.0V/130/450 Lt. Case(+)2(−) 2.5V/130/450 |
| 3 | 19 | 4 | 78.9 | 2 | 89.5 | 107 | Rt. Case(+)2(−) 2.8V/130/450 Lt. Case(+)2(−) 2.5V/130/450 |
| 4 | 32 | 0 | 100.0 | 4 | 87.5 | 186 | Rt. Case(+)0(−)1(−)2(−) 1.6V/130/450 Lt. Case(+)1(−)2(−) 1.8V/130/450 |
| 5 | 12 | 1 | 91.7 | 3.5 | 70.8 | 127 | Bilateral Case(+)1(−) 2.0V/130/60 |
| 6 | 75 | 9 | 88.0 | 9 | 88.0 | 3 | NA |
| 7 | 35 | 7.5 | 78.6 | 7 | 80.0 | 72 | Rt. Case(+)1(−) 2.5V/60/450 Lt. Case(+)1(−) 2.5V/60/360 |
| 8 | 26 | 1 | 96.2 | 3 | 88.5 | 24 | Bilateral Case(+)2(−) 4.2 mA/130/60 |
| 9 | 29.5 | 1 | 96.6 | 1 | 96.6 | 56 | Rt. Case(+)1(−) 3.5V/60/450 Lt. Case(+)1(−) 3.8V/60/450 |
| 10 | 51 | 45 | 11.8 | 45 | 11.8 | 6 | Bilateral Case(+)1(−) 3.5 mA/60/450 |
| 11 | 74 | 26 | 64.9 | 55 | 25.7 | 46 | Bilateral Case(+)1(−)2(−) 3.0/60/180 |
| 12 | 23 | 3 | 87.0 | 3 | 87.0 | 24 | Rt. Case(+)1(−)2(−) 4.1 mA/90/400 Lt. Case(+)2(−)4.4 mA/90/450 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koyama, H.; Mure, H.; Morigaki, R.; Miyamoto, R.; Miyake, K.; Matsuda, T.; Fujita, K.; Izumi, Y.; Kaji, R.; Goto, S.; et al. Long-Term Follow-Up of 12 Patients Treated with Bilateral Pallidal Stimulation for Tardive Dystonia. Life 2021, 11, 477. https://doi.org/10.3390/life11060477
Koyama H, Mure H, Morigaki R, Miyamoto R, Miyake K, Matsuda T, Fujita K, Izumi Y, Kaji R, Goto S, et al. Long-Term Follow-Up of 12 Patients Treated with Bilateral Pallidal Stimulation for Tardive Dystonia. Life. 2021; 11(6):477. https://doi.org/10.3390/life11060477
Chicago/Turabian StyleKoyama, Hiroshi, Hideo Mure, Ryoma Morigaki, Ryosuke Miyamoto, Kazuhisa Miyake, Taku Matsuda, Koji Fujita, Yuishin Izumi, Ryuji Kaji, Satoshi Goto, and et al. 2021. "Long-Term Follow-Up of 12 Patients Treated with Bilateral Pallidal Stimulation for Tardive Dystonia" Life 11, no. 6: 477. https://doi.org/10.3390/life11060477