LincRNA-p21 Levels Relates to Survival and Post-Operative Radiotherapy Benefit in Rectal Cancer Patients

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Samples
2.2. RNA Extraction from Tissue
2.3. Statistical Analyses
3. Results
3.1. Patients
3.2. LincRNA-p21 Expression Levels
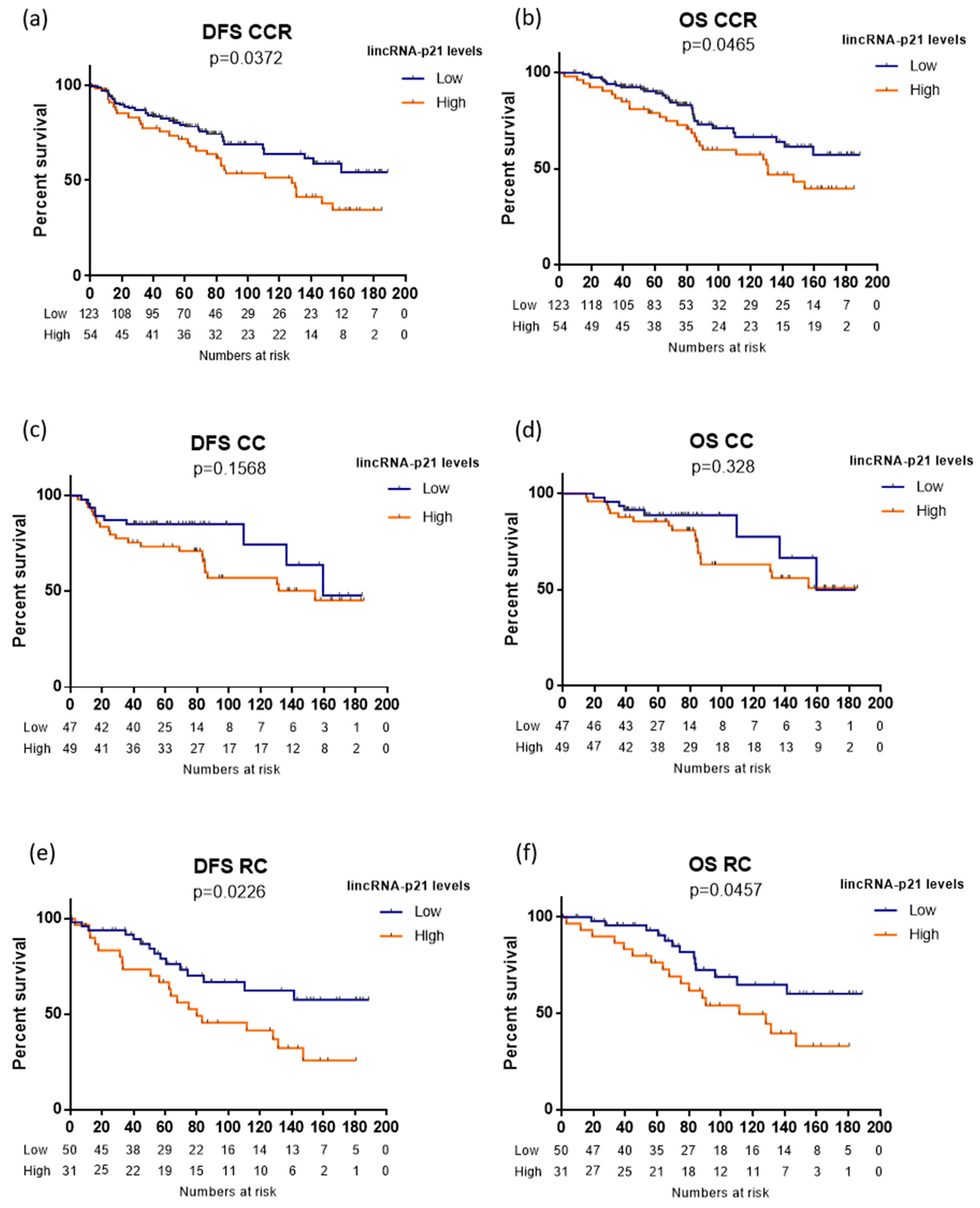
3.3. LincRNA-p21 Expression and Survival
3.4. LincRNA-p21 is an Independent Prognosis Marker in CRC
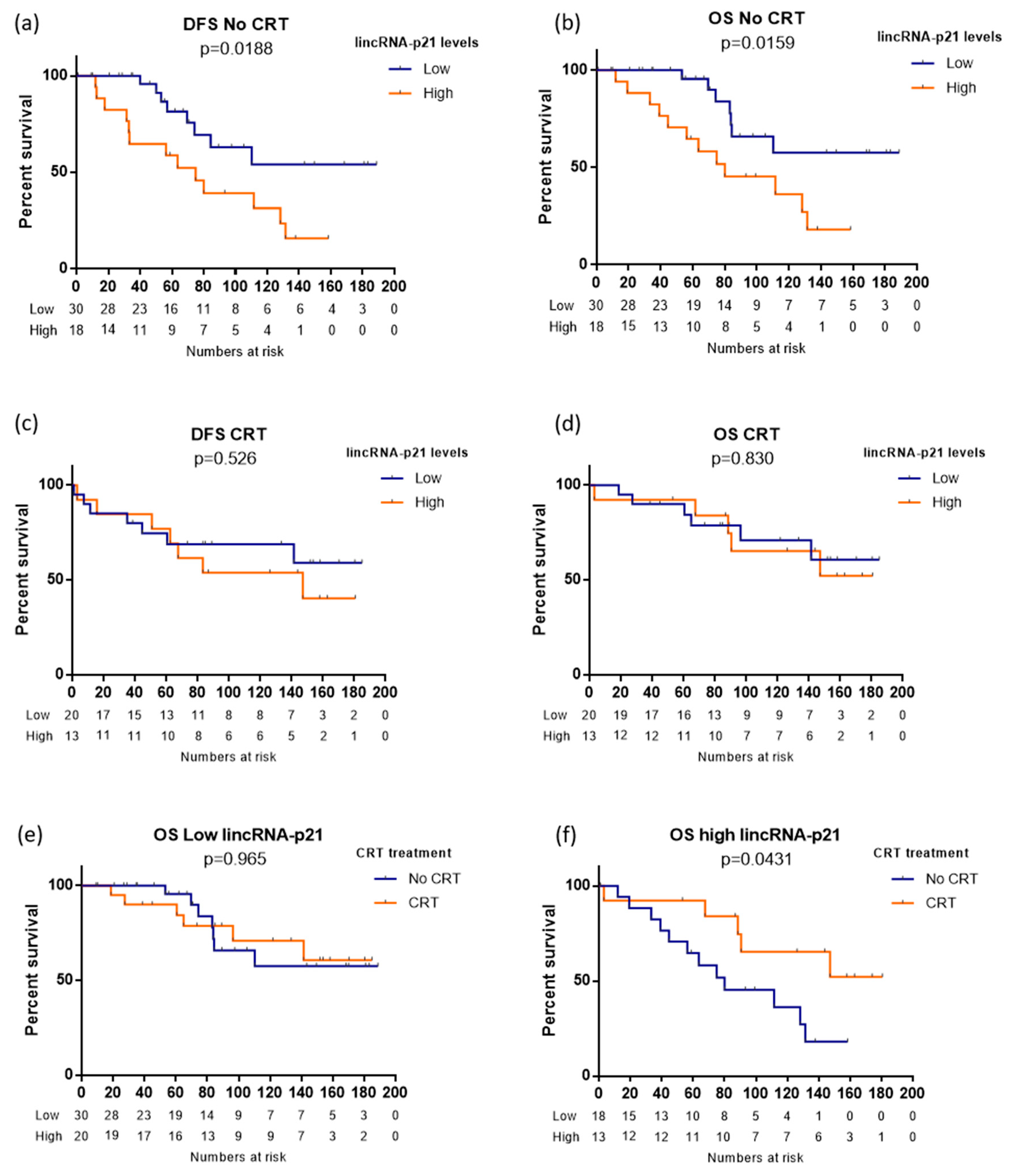
3.5. LincRNA-p21 and Chemoradiotherapy in Rectal Cancer
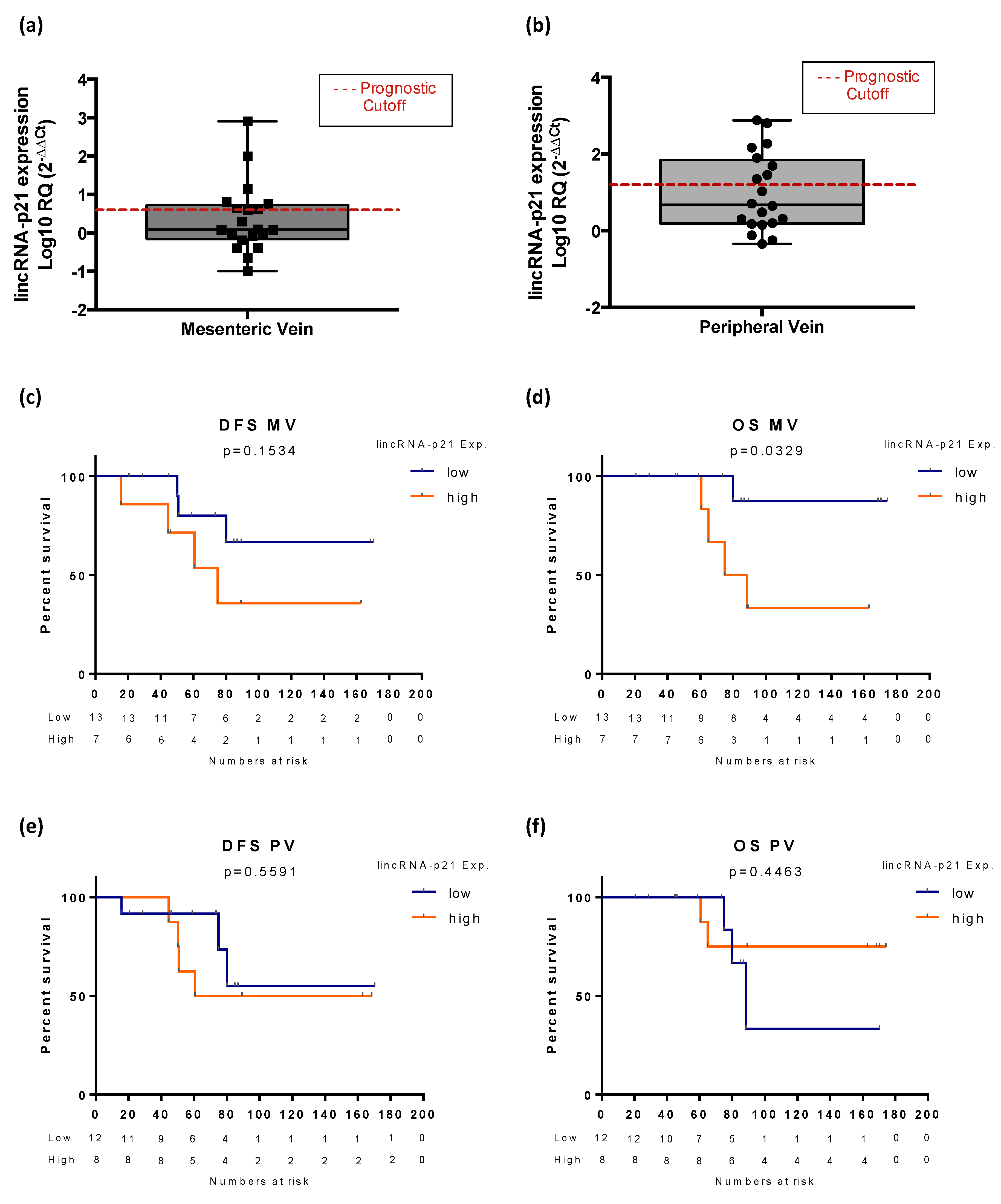
3.6. Exploratory Analysis of LincRNA-p21 Expression in Plasma Samples
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CC | Colon cancer |
| CI | Confidence intervals |
| CRC | Colorectal cancer |
| CT | Chemotherapy |
| CTR | Chemoradiotherapy |
| DFS | Disease-free survival |
| HR | Hazard ratios |
| MDPI | Multidisciplinary Digital Publishing Institute |
| MV | Mesenteric vein |
| NT | Normal tissue |
| OS | Overall survival |
| PV | Peripheral vein |
| RC | Rectal cancer |
| TT | Tumor tissue |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamas, K.; Walenkamp, A.; de Vries, E.; van Vugt, M.; Beets-Tan, R.; van Etten, B.; de Groot, D.; Hospers, G. Rectal and colon cancer: Not just a different anatomic site. Cancer Treat. Rev. 2015, 41, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Labianca, R.; Nordlinger, B.; Beretta, G.; Mosconi, S.; Mandalà, M.; Cervantes, A.; Arnold, D.; ESMO Guidelines Working Group. Early colon cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24 (Suppl. 6), vi64–vi72. [Google Scholar] [CrossRef] [PubMed]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D. Rectal cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28 (Suppl. 4), iv22–iv40. [Google Scholar] [CrossRef]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [Green Version]
- Jia, M.; Jiang, L.; Wang, Y.D.; Huang, J.Z.; Yu, M.; Xue, H.Z. lincRNA-p21 inhibits invasion and metastasis of hepatocellular carcinoma through Notch signaling-induced epithelial–mesenchymal transition. Hepatol. Res. 2016, 46, 1137–1144. [Google Scholar] [CrossRef]
- Djebali, S.; Davis, C.A.; Merkel, A.; Dobin, A.; Lassmann, T.; Mortazavi, A.; Tanzer, A.; Lagarde, J.; Lin, W.; Schlesinger, F. Landscape of transcription in human cells. Nature 2012, 489, 101–108. [Google Scholar] [CrossRef]
- Wilusz, J.E.; Sunwoo, H.; Spector, D.L. Long noncoding RNAs: Functional surprises from the RNA world. Genes Dev. 2009, 23, 1494–1504. [Google Scholar] [CrossRef] [Green Version]
- Gutschner, T.; Diederichs, S. The hallmarks of cancer: A long non-coding RNA point of view. RNA Biol. 2012, 9, 703–719. [Google Scholar] [CrossRef] [Green Version]
- Galamb, O.; Barták, B.K.; Kalmár, A.; Nagy, Z.B.; Szigeti, K.A.; Tulassay, Z.; Igaz, P.; Molnár, B. Diagnostic and prognostic potential of tissue and circulating long non-coding RNAs in colorectal tumors. World J. Gastroenterol. 2019, 25, 5026. [Google Scholar] [CrossRef]
- Necsulea, A.; Soumillon, M.; Warnefors, M.; Liechti, A.; Daish, T.; Zeller, U.; Baker, J.C.; Grützner, F.; Kaessmann, H. The evolution of lncRNA repertoires and expression patterns in tetrapods. Nature 2014, 505, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Washietl, S.; Kellis, M.; Garber, M. Evolutionary dynamics and tissue specificity of human long noncoding RNAs in six mammals. Genome Res. 2014, 24, 616–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, X.; Hu, Z.; Feng, Y.; Hu, X.; Yuan, J.; Zhao, S.D.; Zhang, Y.; Yang, L.; Shan, W.; He, Q. Comprehensive genomic characterization of long non-coding RNAs across human cancers. Cancer Cell 2015, 28, 529–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baassiri, A.; Nassar, F.; Mukherji, D.; Shamseddine, A.; Nasr, R.; Temraz, S. Exosomal non coding RNA in LIQUID biopsies as a promising biomarker for colorectal cancer. Int. J. Mol. Sci. 2020, 21, 1398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.-J.; Wang, X.; Song, Y.-X.; Zhao, J.-H.; Sun, J.-X.; Shi, J.-X.; Wu, Z.-H.; Wang, Z.-N. Circulating noncoding RNAs have a promising future acting as novel biomarkers for colorectal cancer. Dis. Markers 2019, 4, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Huarte, M.; Guttman, M.; Feldser, D.; Garber, M.; Koziol, M.J.; Kenzelmann-Broz, D.; Khalil, A.M.; Zuk, O.; Amit, I.; Rabani, M. A large intergenic noncoding RNA induced by p53 mediates global gene repression in the p53 response. Cell 2010, 142, 409–419. [Google Scholar] [CrossRef] [Green Version]
- Hall, J.; Messenger, Z.; Tam, H.; Phillips, S.; Recio, L.; Smart, R. Long noncoding RNA lincRNA-p21 is the major mediator of UVB-induced and p53-dependent apoptosis in keratinocytes. Cell Death Dis. 2015, 6, e1700. [Google Scholar] [CrossRef]
- Ning, Y.; Yong, F.; Haibin, Z.; Hui, S.; Nan, Z.; Guangshun, Y. LincRNA-p21 activates endoplasmic reticulum stress and inhibits hepatocellular carcinoma. Oncotarget 2015, 6, 28151. [Google Scholar] [CrossRef] [Green Version]
- Yang, F.; Zhang, H.; Mei, Y.; Wu, M. Reciprocal regulation of HIF-1α and lincRNA-p21 modulates the Warburg effect. Mol. Cell 2014, 53, 88–100. [Google Scholar] [CrossRef] [Green Version]
- Meng, S.-S.; Xu, X.-P.; Chang, W.; Lu, Z.-H.; Huang, L.-L.; Xu, J.-Y.; Liu, L.; Qiu, H.-B.; Yang, Y.; Guo, F.-M. LincRNA-p21 promotes mesenchymal stem cell migration capacity and survival through hypoxic preconditioning. Stem Cell Res. Ther. 2018, 9, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Wang, G.; Li, Z.; Zhao, Q.; Zhu, Y.; Zhao, C.; Li, X.; Ma, Z.; Li, X.; Zhang, Y. LincRNA-p21 enhances the sensitivity of radiotherapy for human colorectal cancer by targeting the Wnt/β-catenin signaling pathway. Oncol. Rep. 2014, 31, 1839–1845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhai, H.; Fesler, A.; Schee, K.; Fodstad, Ø.; Flatmark, K.; Ju, J. Clinical significance of long intergenic noncoding RNA-p21 in colorectal cancer. Clin. Colorectal Cancer 2013, 12, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Camp, R.L.; Dolled-Filhart, M.; Rimm, D.L. X-tile: A new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin. Cancer Res. 2004, 10, 7252–7259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaleshi, V.; Irani, S.; Alebouyeh, M.; Mirfakhraie, R.; Aghdaei, A.H. Association of lncRNA-p53 regulatory network (lincRNA-p21, lincRNA-ROR and MALAT1) and p53 with the clinicopathological features of colorectal primary lesions and tumors. Oncol. Lett. 2020, 19, 3937–3949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castellano, J.J.; Navarro, A.; Viñolas, N.; Marrades, R.M.; Moises, J.; Cordeiro, A.; Saco, A.; Muñoz, C.; Fuster, D.; Molins, L. LincRNA-p21 impacts prognosis in resected non–small cell lung cancer patients through angiogenesis regulation. J. Thorac. Oncol. 2016, 11, 2173–2182. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ruan, Y.; Wang, X.; Zhao, W.; Jiang, Q.; Jiang, C.; Zhao, Y.; Xu, Y.; Sun, F.; Zhu, Y. Long intragenic non-coding RNA linc RNA-p21 suppresses development of human prostate cancer. Cell Prolif. 2017, 50, e12318. [Google Scholar] [CrossRef] [Green Version]
- Peng, W.; Wu, J.; Feng, J. LincRNA-p21 predicts favorable clinical outcome and impairs tumorigenesis in diffuse large B cell lymphoma patients treated with R-CHOP chemotherapy. Clin. Exp. Med. 2017, 17, 1–8. [Google Scholar] [CrossRef]
- Yang, W.; Yu, H.; Shen, Y.; Liu, Y.; Yang, Z.; Sun, T. MiR-146b-5p overexpression attenuates stemness and radioresistance of glioma stem cells by targeting HuR/lincRNA-p21/β-catenin pathway. Oncotarget 2016, 7, 41505. [Google Scholar] [CrossRef] [Green Version]
- Monzo, M.; Santasusagna, S.; Moreno, I.; Martinez, F.; Hernáez, R.; Muñoz, C.; Castellano, J.J.; Moreno, J.; Navarro, A. Exosomal microRNAs isolated from plasma of mesenteric veins linked to liver metastases in resected patients with colon cancer. Oncotarget 2017, 8, 30859. [Google Scholar] [CrossRef]
- Santasusagna, S.; Moreno, I.; Navarro, A.; Rodenas, F.M.; Hernandez, R.; Castellano, J.J.; Munoz, C.; Monzo, M. Prognostic impact of miR-200 family members in plasma and exosomes from tumor-draining versus peripheral veins of colon cancer patients. Oncology 2018, 95, 309–318. [Google Scholar] [CrossRef]
- Castellano, J.J.; Marrades, R.M.; Molins, L.; Viñolas, N.; Moises, J.; Canals, J.; Han, B.; Li, Y.; Martinez, D.; Monzó, M. Extracellular vesicle lincRNA-p21 expression in tumor-draining pulmonary vein defines prognosis in NSCLC and modulates endothelial cell behavior. Cancers 2020, 12, 734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dragomir, M.; Chen, B.; Calin, G.A. Exosomal lncRNAs as new players in cell-to-cell communication. Transl. Cancer Res. 2018, 7 (Suppl. 2), S243. [Google Scholar] [CrossRef] [PubMed]
- Sole, C.; Arnaiz, E.; Manterola, L.; Otaegui, D.; Lawrie, C.H. The Circulating Transcriptome as a Source of Cancer Liquid Biopsy Biomarkers. Semin. Cancer Biol. 2019, 58, 100–108. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value | All CRC Patients (n = 177) | Colon Cancer (n = 96) | Rectal Cancer (n = 81) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N (%) | DFS | OS | N (%) | DFS | OS | N (%) | DFS | OS | ||
| Sex | Male | 103 (58.2) | 0.644 | 0.311 | 52 (54.2) | 0.473 | 0.928 | 51 (63) | 0.081 | 0.111 |
| Female | 74 (41.8) | 44 (45.8) | 30 (37) | |||||||
| Age (years) | ≤65 | 59 (33.3) | 0.002 | 0.001 | 31 (32.3) | 0.02 | 0.012 | 28 (34.6) | 0.024 | 0.002 |
| >65 | 118 (66.7) | 65 (67.7) | 53 (65.4) | |||||||
| ECOG PS * | 0 | 8 (4.5) | 0.041 | 0.017 | 6 (6.3) | 0.017 | 0.013 | 2 (2.5) | 0.405 | 0.292 |
| 1 | 148 (84.2) | 79 (82.3) | 70 (86.4) | |||||||
| 2 | 20 (11.3) | 11 (11.5) | 9 (11.1) | |||||||
| T | 1 | 11 (6.2) | 0.467 | 0.266 | 3 (3.1) | 0.373 | 0.446 | 8 (9.9) | 0.761 | 0.391 |
| 2 | 36 (20.3) | 10 (10.4) | 26 (32.1) | |||||||
| 3 | 112 (63.3) | 68 (70.8) | 44 (54.3) | |||||||
| 4 | 18 (10.2) | 15 (15.6) | 3 (3.7) | |||||||
| N | 0 | 120 (67.8) | 0.233 | 0.418 | 63 (65.6) | 0.385 | 0.344 | 57 (70.4) | 0.659 | 0.858 |
| 1 | 40 (22.6) | 25 (26) | 15 (18.5) | |||||||
| 2 | 17 (9.6) | 8 (8.3) | 9 (11.1) | |||||||
| Stage | I | 37 (20.9) | 0.314 | 0.554 | 10 (10.4) | 0.258 | 0.353 | 27 (33.4) | 0.763 | 0.994 |
| II | 83 (46.9) | 53 (55.2) | 30 (37) | |||||||
| III | 57 (32.2) | 33 (34.4) | 24 (29.6) | |||||||
| Previous polyp | Yes | 40 (22.6) | 0.311 | 0.179 | 26 (27.1) | 0.142 | 0.03 | 14 (17.3) | 0.915 | 0.896 |
| No | 137 (77.4) | 70 (72.9) | 67 (82.7) | |||||||
| Mucin secretion | Yes | 33 (18.6) | 0.534 | 0.129 | 27 (28.1) | 0.691 | 0.292 | 75 (92.6) | 0.152 | 0.054 |
| No | 144 (81.4) | 69 (71.9) | 6 (7.4) | |||||||
| Relapse | Yes | 33 (18.6) | --- | --- | 17 (17.7) | --- | --- | 16 (19.8) | --- | --- |
| No | 144 (81.4) | 79 (82.3) | 65 (80.2) | |||||||
| DFS | OS | ||||
|---|---|---|---|---|---|
| Factor | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| CRC patients | Advanced age | 1.043 (1.016–1.071) | 0.02 | 1.075 (1.042–1.110) | p < 0.001 |
| Stage III | 1.379 (0.687–2.769) | 0.367 | 1.435 (0.676–3.046) | 0.348 | |
| No adjuvant treatment | 0.778 (0.339–1.785) | 0.554 | 0.658 (0.258–1.678) | 0.380 | |
| ECOG PS (0) | 0.274 (0.056–1.341) | 0.110 | 0.408 (0.081–2.046) | 0.276 | |
| High lincRNA-p21 | 1.747 (1.074–2.841) | 0.025 | 1.884 (1.104–3.217) | 0.020 | |
| RC Patients | Advanced age | 1.032 (0.996–1.069) | 0.087 | 1.064 (1.017–1.113) | 0.007 |
| Male | 0.570 (0.290–1.119) | 0.102 | - | - | |
| Mucin secretion | - | - | 2.468 (0.833–7.317) | 0.103 | |
| Stage III | 0.769 (0.148–4.013) | 0.756 | 0.606 (0.095–3.861) | 0.596 | |
| No adjuvant treatment | 0.924 (0.409–2.090) | 0.850 | 0.996 (0.423–2.345) | 0.992 | |
| High lincRNA-p21 | 1.986 (1.013–3.895) | 0.046 | 1.318(0.562–3.091) | 0.562 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Castellano, J.J.; Moreno, I.; Martínez-Rodenas, F.; Hernandez, R.; Canals, J.; Diaz, T.; Han, B.; Muñoz, C.; Biete, A.; et al. LincRNA-p21 Levels Relates to Survival and Post-Operative Radiotherapy Benefit in Rectal Cancer Patients. Life 2020, 10, 172. https://doi.org/10.3390/life10090172
Li Y, Castellano JJ, Moreno I, Martínez-Rodenas F, Hernandez R, Canals J, Diaz T, Han B, Muñoz C, Biete A, et al. LincRNA-p21 Levels Relates to Survival and Post-Operative Radiotherapy Benefit in Rectal Cancer Patients. Life. 2020; 10(9):172. https://doi.org/10.3390/life10090172
Chicago/Turabian StyleLi, Yan, Joan J. Castellano, Isabel Moreno, Francisco Martínez-Rodenas, Raquel Hernandez, Jordi Canals, Tania Diaz, Bing Han, Carmen Muñoz, Albert Biete, and et al. 2020. "LincRNA-p21 Levels Relates to Survival and Post-Operative Radiotherapy Benefit in Rectal Cancer Patients" Life 10, no. 9: 172. https://doi.org/10.3390/life10090172