
Risk of Ischemic Heart Disease Associated with Primary Dysmenorrhea: A Population-Based Retrospective Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
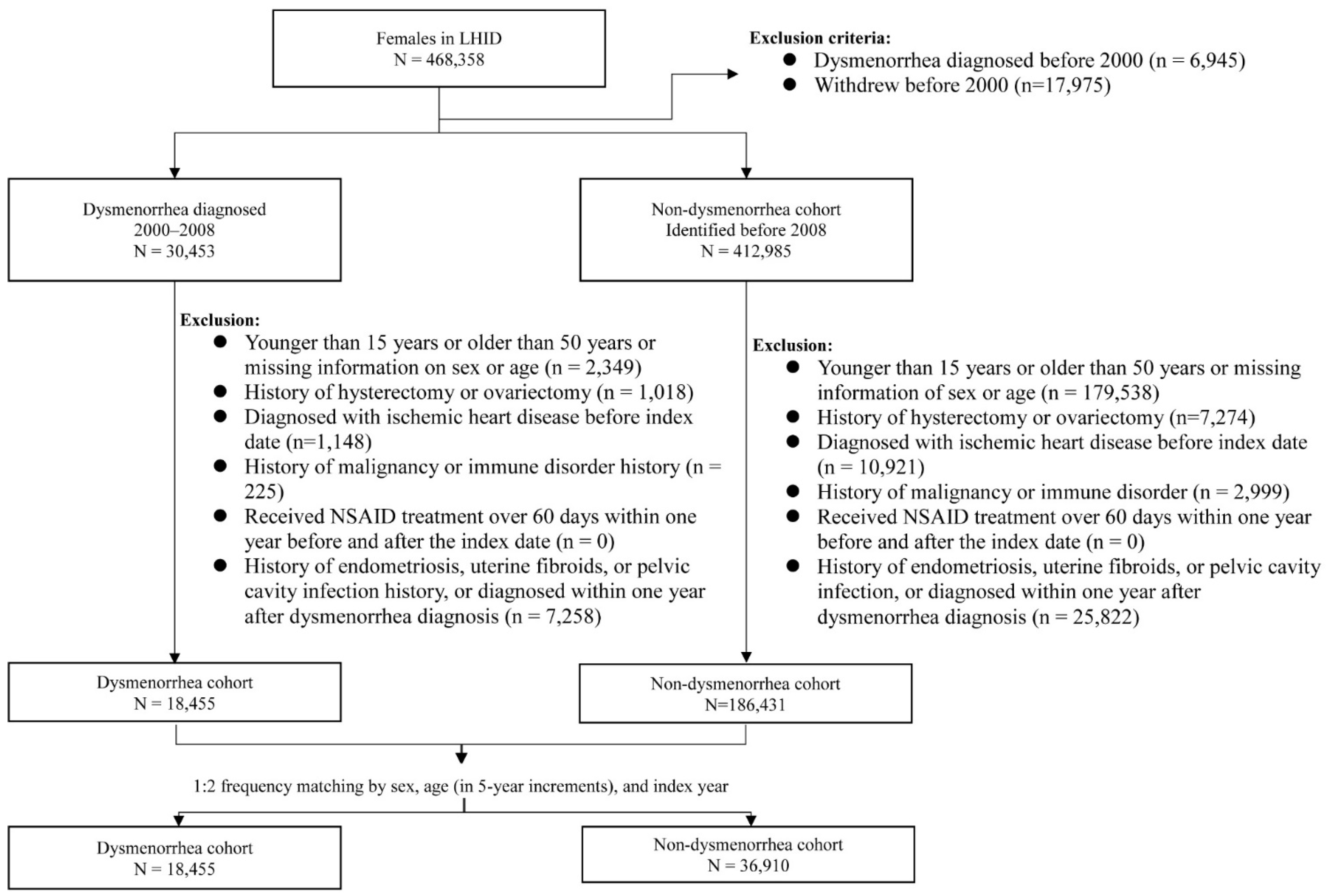
2.2. Study Cohorts
2.3. Baseline Comorbidity, Medicine Use, and Outcome
2.4. Statistical Analysis
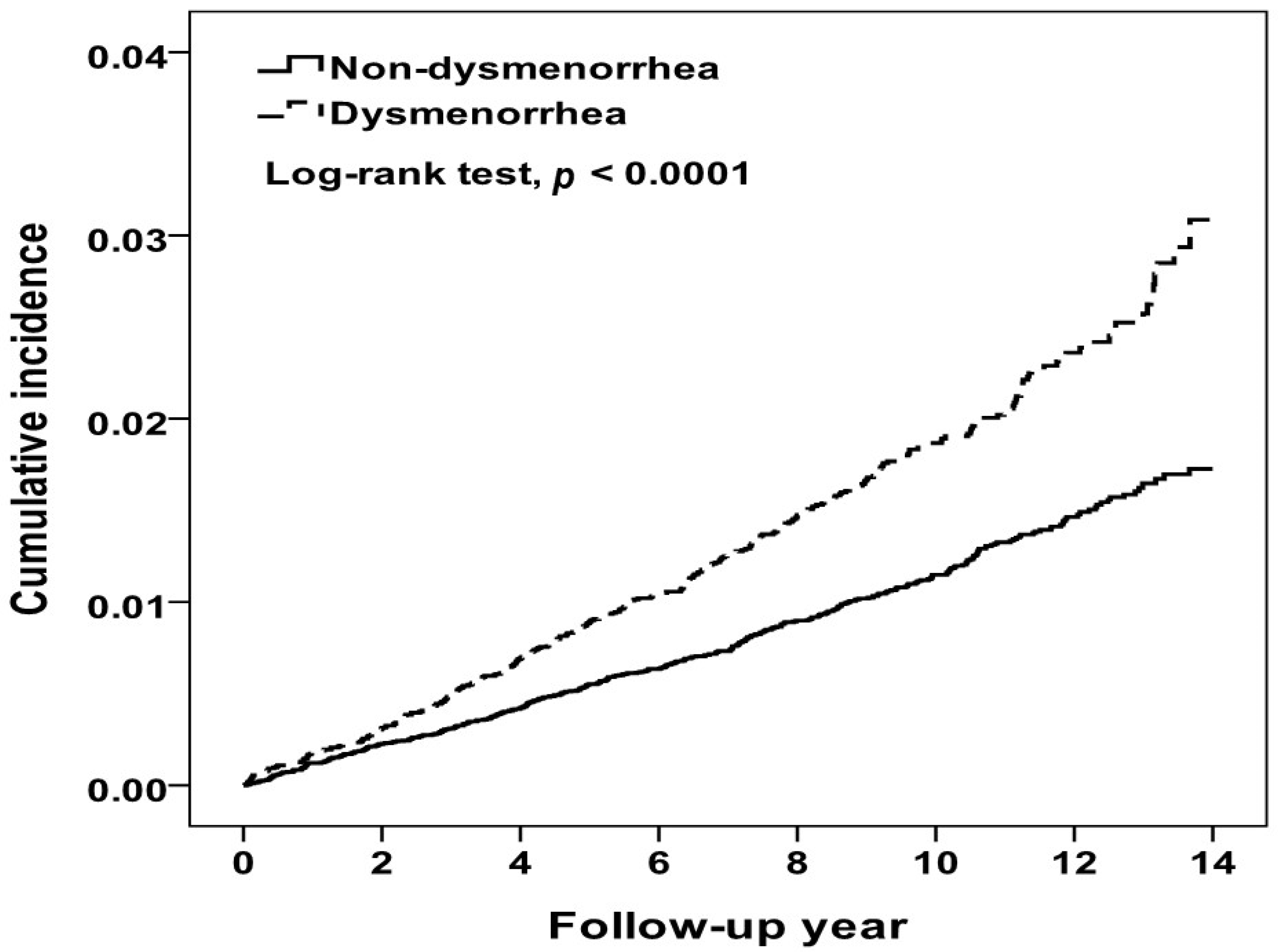
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 9 June 2022).
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Ahmad, F.B.; Anderson, R.N. The Leading Causes of Death in the US for 2020. JAMA 2021, 325, 1829–1830. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Brown, J.C.; Gerhardt, T.E.; Kwon, E. Risk Factors For Coronary Artery Disease. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Mehilli, J.; Presbitero, P. Coronary artery disease and acute coronary syndrome in women. Heart 2020, 106, 487–492. [Google Scholar] [CrossRef]
- Neumann, J.T.; Goßling, A.; Sörensen, N.A.; Blankenberg, S.; Magnussen, C.; Westermann, D. Sex-Specific Outcomes in Patients with Acute Coronary Syndrome. J. Clin. Med. 2020, 9, 2124. [Google Scholar] [CrossRef]
- Vaccarino, V.; Parsons, L.; Every, N.R.; Barron, H.V.; Krumholz, H.M. Sex-based differences in early mortality after myocardial infarction. National Registry of Myocardial Infarction 2 Participants. N. Engl. J. Med. 1999, 341, 217–225. [Google Scholar] [CrossRef]
- Davis, M.; Diamond, J.; Montgomery, D.; Krishnan, S.; Eagle, K.; Jackson, E. Acute coronary syndrome in young women under 55 years of age: Clinical characteristics, treatment, and outcomes. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2015, 104, 648–655. [Google Scholar] [CrossRef]
- Bugiardini, R.; Manfrini, O.; Cenko, E. Female sex as a biological variable: A review on younger patients with acute coronary syndrome. Trends Cardiovasc. Med. 2019, 29, 50–55. [Google Scholar] [CrossRef]
- Lichtman, J.H.; Lorenze, N.P.; D’Onofrio, G.; Spertus, J.A.; Lindau, S.T.; Morgan, T.M.; Herrin, J.; Bueno, H.; Mattera, J.A.; Ridker, P.M.; et al. Variation in recovery: Role of gender on outcomes of young AMI patients (VIRGO) study design. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 684–693. [Google Scholar] [CrossRef] [PubMed]
- Davies, R.E.; Rier, J.D. Gender Disparities in CAD: Women and Ischemic Heart Disease. Curr. Atheroscler. Rep. 2018, 20, 51. [Google Scholar] [CrossRef] [PubMed]
- Schuit, S.C.; Oei, H.H.; Witteman, J.C.; Geurts van Kessel, C.H.; van Meurs, J.B.; Nijhuis, R.L.; van Leeuwen, J.P.; de Jong, F.H.; Zillikens, M.C.; Hofman, A.; et al. Estrogen receptor alpha gene polymorphisms and risk of myocardial infarction. JAMA 2004, 291, 2969–2977. [Google Scholar] [CrossRef] [PubMed]
- Querio, G.; Geddo, F.; Antoniotti, S.; Gallo, M.P.; Penna, C. Sex and Response to Cardioprotective Conditioning Maneuvers. Front. Physiol. 2021, 12, 667961. [Google Scholar] [CrossRef] [PubMed]
- Wood, C.; Larsen, L.; Williams, R. Menstrual characteristics of 2,343 women attending the Shepherd Foundation. Aust. N. Z. J. Obstet. Gynaecol. 1979, 19, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Latthe, P.; Mignini, L.; Gray, R.; Hills, R.; Khan, K. Factors predisposing women to chronic pelvic pain: Systematic review. BMJ 2006, 332, 749–755. [Google Scholar] [CrossRef] [PubMed]
- Ferries-Rowe, E.; Corey, E.; Archer, J.S. Primary Dysmenorrhea: Diagnosis and Therapy. Obstet. Gynecol. 2020, 136, 1047–1058. [Google Scholar] [CrossRef]
- Harlow, S.D.; Ephross, S.A. Epidemiology of menstruation and its relevance to women’s health. Epidemiol. Rev. 1995, 17, 265–286. [Google Scholar] [CrossRef]
- Parker, M.A.; Sneddon, A.E.; Arbon, P. The menstrual disorder of teenagers (MDOT) study: Determining typical menstrual patterns and menstrual disturbance in a large population-based study of Australian teenagers. BJOG Int. J. Obstet. Gynaecol. 2010, 117, 185–192. [Google Scholar] [CrossRef]
- Karout, S.; Soubra, L.; Rahme, D.; Karout, L.; Khojah, H.M.J.; Itani, R. Prevalence, risk factors, and management practices of primary dysmenorrhea among young females. BMC Women’s Health 2021, 21, 392. [Google Scholar] [CrossRef]
- Chiou, M.H.; Wang, H.H. Predictors of dysmenorrhea and self-care behavior among vocational nursing school female students. J. Nurs. Res. 2008, 16, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.F.; Lin, Y.H. Selection and efficacy of self-management strategies for dysmenorrhea in young Taiwanese women. J. Clin. Nurs. 2011, 20, 1018–1025. [Google Scholar] [CrossRef] [PubMed]
- Palmer, D. “To help a million sick, you must kill a few nurses”: Nurses’ occupational health, 1890–1914. Nurs. Hist. Rev. 2012, 20, 14–45. [Google Scholar] [CrossRef] [PubMed]
- De Sanctis, V.; Soliman, A.T.; Daar, S.; Di Maio, S.; Elalaily, R.; Fiscina, B.; Kattamis, C. Prevalence, attitude and practice of self-medication among adolescents and the paradigm of dysmenorrhea self-care management in different countries. Acta Biomed. 2020, 91, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Kho, K.A.; Shields, J.K. Diagnosis and Management of Primary Dysmenorrhea. JAMA 2020, 323, 268–269. [Google Scholar] [CrossRef]
- Fang, L.; Gu, C.; Liu, X.; Xie, J.; Hou, Z.; Tian, M.; Yin, J.; Li, A.; Li, Y. Metabolomics study on primary dysmenorrhea patients during the luteal regression stage based on ultra performance liquid chromatography coupled with quadrupoletimeofflight mass spectrometry. Mol. Med. Rep. 2017, 15, 1043–1050. [Google Scholar] [CrossRef]
- Raina, J.K.; Sharma, M.; Panjaliya, R.K.; Dogra, V.; Bakaya, A.; Kumar, P. Association of ESR1 (rs2234693 and rs9340799), CETP (rs708272), MTHFR (rs1801133 and rs2274976) and MS (rs185087) polymorphisms with Coronary Artery Disease (CAD). BMC Cardiovasc. Disord. 2020, 20, 340. [Google Scholar] [CrossRef]
- Castellon, X.; Bogdanova, V. Chronic Inflammatory Diseases and Endothelial Dysfunction. Aging Dis. 2016, 7, 81–89. [Google Scholar] [CrossRef]
- Barcikowska, Z.; Rajkowska-Labon, E.; Grzybowska, M.E.; Hansdorfer-Korzon, R.; Zorena, K. Inflammatory Markers in Dysmenorrhea and Therapeutic Options. Int. J. Environ. Res. Public Health 2020, 17, 1191. [Google Scholar] [CrossRef]
- Chen, L.; Liu, T.; Zhao, X. Inferring anatomical therapeutic chemical (ATC) class of drugs using shortest path and random walk with restart algorithms. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 2228–2240. [Google Scholar] [CrossRef]
- von Hafe, M.; Neves, J.S.; Vale, C.; Borges-Canha, M.; Leite-Moreira, A. The impact of thyroid hormone dysfunction on ischemic heart disease. Endocr. Connect. 2019, 8, R76–R90. [Google Scholar] [CrossRef] [PubMed]
- Saeed, A.; Rana, K.F.; Warriach, Z.I.; Tariq, M.A.; Malik, B.H. Association of Migraine and Ischemic Heart Disease: A Review. Cureus 2019, 11, e5719. [Google Scholar] [CrossRef] [PubMed]
- Bisciglia, A.; Pasceri, V.; Irini, D.; Varveri, A.; Speciale, G. Risk Factors for Ischemic Heart Disease. Rev. Recent Clin. Trials 2019, 14, 86–94. [Google Scholar] [CrossRef]
- Xu, H.; Li, P.H.; Barrow, T.M.; Colicino, E.; Li, C.; Song, R.; Liu, H.; Tang, N.J.; Liu, S.; Guo, L.; et al. Obesity as an effect modifier of the association between menstrual abnormalities and hypertension in young adult women: Results from Project ELEFANT. PLoS ONE 2018, 13, e0207929. [Google Scholar] [CrossRef] [PubMed]
- Sharghi, M.; Mansurkhani, S.M.; Larky, D.A.; Kooti, W.; Niksefat, M.; Firoozbakht, M.; Behzadifar, M.; Azami, M.; Servatyari, K.; Jouybari, L. An update and systematic review on the treatment of primary dysmenorrhea. JBRA Assist. Reprod. 2019, 23, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, I.; Póvoa, A.M. Primary Dysmenorrhea: Assessment and Treatment. Rev. Bras. Ginecol. Obstet. 2020, 42, 501–507. [Google Scholar] [CrossRef]
- Bally, M.; Dendukuri, N.; Rich, B.; Nadeau, L.; Helin-Salmivaara, A.; Garbe, E.; Brophy, J.M. Risk of acute myocardial infarction with NSAIDs in real world use: Bayesian meta-analysis of individual patient data. BMJ 2017, 357, j1909. [Google Scholar] [CrossRef]
- Sidney, S.; Siscovick, D.S.; Petitti, D.B.; Schwartz, S.M.; Quesenberry, C.P.; Psaty, B.M.; Raghunathan, T.E.; Kelaghan, J.; Koepsell, T.D. Myocardial infarction and use of low-dose oral contraceptives: A pooled analysis of 2 US studies. Circulation 1998, 98, 1058–1063. [Google Scholar] [CrossRef]
- van Bergen, E.D.P.; Monnikhof, M.; Lafeber, F.; Schutgens, R.E.G.; Mastbergen, S.C.; van Vulpen, L.F.D. The fear for adverse bleeding and cardiovascular events in hemophilia patients using (non-)selective non-steroidal anti-inflammatory drugs: A systematic review reporting on safety. Blood Rev. 2022, 100987. [Google Scholar] [CrossRef]
- McKenna, K.A.; Fogleman, C.D. Dysmenorrhea. Am. Fam. Physician 2021, 104, 164–170. [Google Scholar]
- Shaper, A.G.; Pocock, S.J.; Walker, M.; Phillips, A.N.; Whitehead, T.P.; Macfarlane, P.W. Risk factors for ischaemic heart disease: The prospective phase of the British Regional Heart Study. J. Epidemiol. Community Health 1985, 39, 197–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, P.K.; Wei, J.; Wenger, N.K. Ischemic heart disease in women: A focus on risk factors. Trends Cardiovasc. Med. 2015, 25, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef] [PubMed]
- Kenton, E.J. Access to neurological care for minorities. Arch. Neurol. 1991, 48, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Mercer, B.N.; Koshy, A.; Drozd, M.; Walker, A.M.N.; Patel, P.A.; Kearney, L.; Gierula, J.; Paton, M.F.; Lowry, J.E.; Kearney, M.T.; et al. Ischemic Heart Disease Modifies the Association of Atrial Fibrillation With Mortality in Heart Failure With Reduced Ejection Fraction. J. Am. Heart Assoc. 2018, 7, e009770. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar] [CrossRef]
- Trinh, P.; Hoover, D.R.; Sonnenberg, F.A. Time-of-day changes in physician clinical decision making: A retrospective study. PLoS ONE 2021, 16, e0257500. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Kao Yang, Y.H.; Lai, E.C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef]
- Larki, M.; Salavati, A.; Azmoude, E. The Relationship Between Menstrual Patterns and Menstrual Attitude Dimensions among Women of Reproductive Age: Cross-sectional survey. Sultan Qaboos Univ. Med. J. 2022, 22, 241–246. [Google Scholar] [CrossRef]
- Jacobsen, B.K.; Knutsen, S.F.; Oda, K.; Fraser, G.E. Parity and total, ischemic heart disease and stroke mortality. The Adventist Health Study, 1976–1988. Eur. J. Epidemiol. 2011, 26, 711–718. [Google Scholar] [CrossRef]
- Wu, Y.; Pang, J.; Wang, J.; Wu, J.; Zhang, S.; Zhang, S.; Yao, Y.; Cheng, S.; Tao, Y.; Shen, Z.; et al. Fertility Histories and Heart Disease in Later Life in China. Front. Public Health 2022, 10, 819196. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Shu, X.O.; Gao, Y.T.; Yang, G.; Li, H.; Zheng, W. Pregnancy, childrearing, and risk of stroke in Chinese women. Stroke 2009, 40, 2680–2684. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Non-Dysmenorrhea Cohort (n = 36,910) | Dysmenorrhea Cohort (n = 18,455) | p Value * | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age group (years) | 0.99 | ||||
| 15–29 | 27,666 | 75.0 | 13,833 | 75.0 | |
| 30–39 | 6634 | 18.0 | 3317 | 18.0 | |
| 40–50 | 2610 | 7.07 | 1305 | 7.07 | |
| Mean age, years (SD) | 25.7 | (8.03) | 25.6 | (7.90) | 0.27 |
| Baseline comorbidities | |||||
| Diabetes | 450 | 1.22 | 233 | 1.26 | 0.66 |
| Hypertension | 494 | 1.34 | 253 | 1.37 | 0.75 |
| Hyperlipidemia | 416 | 1.13 | 299 | 1.62 | <0.0001 |
| Arrhythmia | 500 | 1.35 | 433 | 2.35 | <0.0001 |
| Thyroid disease | 1545 | 4.19 | 1068 | 5.79 | <0.0001 |
| Migraine | 610 | 1.65 | 689 | 3.73 | <0.0001 |
| Medicine use | |||||
| NSAID | 180 | 0.49 | 132 | 0.72 | 0.0007 |
| Female hormone use | 32 | 0.09 | 16 | 0.09 | 0.99 |
| Follow-up year, mean (SD) | 9.77 | (2.61) | 9.47 | (2.62) | <0.0001 |
| Variables | Non-Dysmenorrhea Cohort | Dysmenorrhea Cohort | Adjusted HR † | p for Interaction | |||||
|---|---|---|---|---|---|---|---|---|---|
| Event | Person Years | IR † | Event | Person Years | IR † | (95%CI) | p-Value | ||
| Overall | 427 | 360,608 | 1.18 | 338 | 174,747 | 1.93 | 1.60 (1.38–1.85) | <0.0001 | |
| Age group (years) | 0.429 | ||||||||
| 15–29 | 125 | 270,201 | 0.46 | 105 | 131,794 | 0.80 | 1.65 (1.27–2.15) | 0.0002 | |
| 30–39 | 119 | 65,270 | 1.82 | 105 | 31,107 | 3.38 | 1.76 (1.35–2.29) | <0.0001 | |
| 40–50 | 183 | 25,138 | 7.28 | 128 | 11,847 | 10.80 | 1.39 (1.10–1.74) | 0.005 | |
| Diabetes | 0.0002 | ||||||||
| No | 389 | 356,486 | 1.09 | 328 | 172,607 | 1.90 | 1.71 (1.47–1.98) | <0.0001 | |
| Yes | 38 | 4122 | 9.22 | 10 | 2140 | 4.67 | 0.55 (0.27–1.10) | 0.091 | |
| Hypertension | 0.224 | ||||||||
| No | 369 | 356,126 | 1.04 | 302 | 172,580 | 1.75 | 1.66 (1.43–1.94) | <0.0001 | |
| Yes | 58 | 4482 | 12.94 | 36 | 2167 | 16.61 | 1.19 (0.78–1.81) | 0.435 | |
| Hyperlipidemia | 0.083 | ||||||||
| No | 395 | 357,092 | 1.11 | 314 | 172,190 | 1.82 | 1.64 (1.42–1.91) | <0.0001 | |
| Yes | 32 | 3516 | 9.10 | 24 | 2557 | 9.39 | 1.06 (0.62–1.81) | 0.844 | |
| Arrhythmia | 0.568 | ||||||||
| No | 394 | 355,942 | 1.11 | 300 | 170,856 | 1.76 | 1.63 (1.40–1.90) | <0.0001 | |
| Yes | 33 | 4666 | 7.07 | 38 | 3891 | 9.77 | 1.38 (0.86–2.21) | 0.180 | |
| Thyroid disease | 0.461 | ||||||||
| No | 400 | 345,999 | 1.16 | 303 | 164,974 | 1.84 | 1.59 (1.36–1.84) | <0.0001 | |
| Yes | 27 | 14,609 | 1.85 | 35 | 9774 | 3.58 | 1.79 (1.07–2.99) | 0.026 | |
| Migraine | 0.114 | ||||||||
| No | 407 | 355,242 | 1.15 | 315 | 168,561 | 1.87 | 1.64 (1.41–1.90) | <0.0001 | |
| Yes | 20 | 5366 | 3.73 | 23 | 6186 | 3.72 | 1.14 (0.62–2.12) | 0.669 | |
| NSAID | 0.728 | ||||||||
| No | 423 | 358,803 | 1.18 | 332 | 173,423 | 1.91 | 1.60 (1.39–1.85) | <0.0001 | |
| Yes | 4 | 1805 | 2.22 | 6 | 1324 | 4.53 | 1.76 (0.45–6.90) | 0.419 | |
| Hormones | 0.848 | ||||||||
| No | 426 | 360,275 | 1.18 | 337 | 17,459 | 1.93 | 1.60 (1.38–1.85) | <0.0001 | |
| Yes | 1 | 333 | 3.00 | 1 | 158 | 6.33 | 2.24 (0.13–38.6) | 0.580 | |
| Variable | Ischemic Heart Disease | |||||||
| Yes (n = 338) | No (n = 18,117) | Odds Ratio (95% Confidence Interval) | ||||||
| n | % | n | % | Crude | p-Value | Adjusted | p-Value | |
| Age group (years) | ||||||||
| 15–29 | 105 | 31.1 | 13,728 | 75.8 | 1.00 | 1.00 | ||
| 30–40 | 105 | 31.1 | 3212 | 17.7 | 4.27 (3.25–5.62) | <0.0001 | 3.95 (3.00–5.21) | <0.0001 |
| 40–50 | 128 | 37.8 | 1177 | 6.50 | 14.2 (1.09–18.5) | <0.0001 | 11.3 (8.55–15.0) | <0.0001 |
| Baseline comorbidities (yes vs. no) | ||||||||
| Diabetes | 10 | 2.96 | 223 | 1.23 | 2.45 (1.29–4.65) | 0.006 | 0.72 (0.36–1.46) | 0.370 |
| Hypertension | 36 | 10.7 | 217 | 1.20 | 8.93 (6.79–14.2) | <0.0001 | 2.50 (1.64–3.81) | <0.0001 |
| Hyperlipidemia | 24 | 7.10 | 275 | 1.52 | 4.96 (3.22–7.64) | <0.0001 | 1.30 (0.79–2.15) | 0.302 |
| Arrhythmia | 38 | 11.2 | 395 | 2.18 | 5.69 (4.00–8.08) | <0.0001 | 3.30 (2.25–4.86) | <0.0001 |
| Thyroid disease | 35 | 10.4 | 1033 | 5.70 | 1.91 (1.34–2.73) | 0.0004 | 1.17 (0.80–1.71) | 0.407 |
| Migraine | 23 | 6.80 | 666 | 3.68 | 1.91 (1.24–2.94) | 0.003 | 1.26 (0.81–1.98) | 0.308 |
| Medicine use | ||||||||
| NSAID | 6 | 1.78 | 126 | 0.70 | 2.58 (1.13–5.90) | 0.025 | 1.95 (0.81–4.71) | 0.136 |
| Hormones | 1 | 0.30 | 15 | 0.08 | 3.59 (0.47–27.2) | 0.216 | NA | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, C.-H.; Muo, C.-H.; Sung, F.-C.; Yen, P.-S. Risk of Ischemic Heart Disease Associated with Primary Dysmenorrhea: A Population-Based Retrospective Cohort Study. J. Pers. Med. 2022, 12, 1610. https://doi.org/10.3390/jpm12101610
Yeh C-H, Muo C-H, Sung F-C, Yen P-S. Risk of Ischemic Heart Disease Associated with Primary Dysmenorrhea: A Population-Based Retrospective Cohort Study. Journal of Personalized Medicine. 2022; 12(10):1610. https://doi.org/10.3390/jpm12101610
Chicago/Turabian StyleYeh, Chung-Hsin, Chih-Hsin Muo, Fung-Chang Sung, and Pao-Sheng Yen. 2022. "Risk of Ischemic Heart Disease Associated with Primary Dysmenorrhea: A Population-Based Retrospective Cohort Study" Journal of Personalized Medicine 12, no. 10: 1610. https://doi.org/10.3390/jpm12101610