
Finetuned Super-Resolution Generative Adversarial Network (Artificial Intelligence) Model for Calcium Deblooming in Coronary Computed Tomography Angiography


Abstract
:1. Introduction
2. Materials and Methods
2.1. ESRGAN Model Finetuning
2.2. Finetuned Real-ESRGAN Model Performance Evaluation
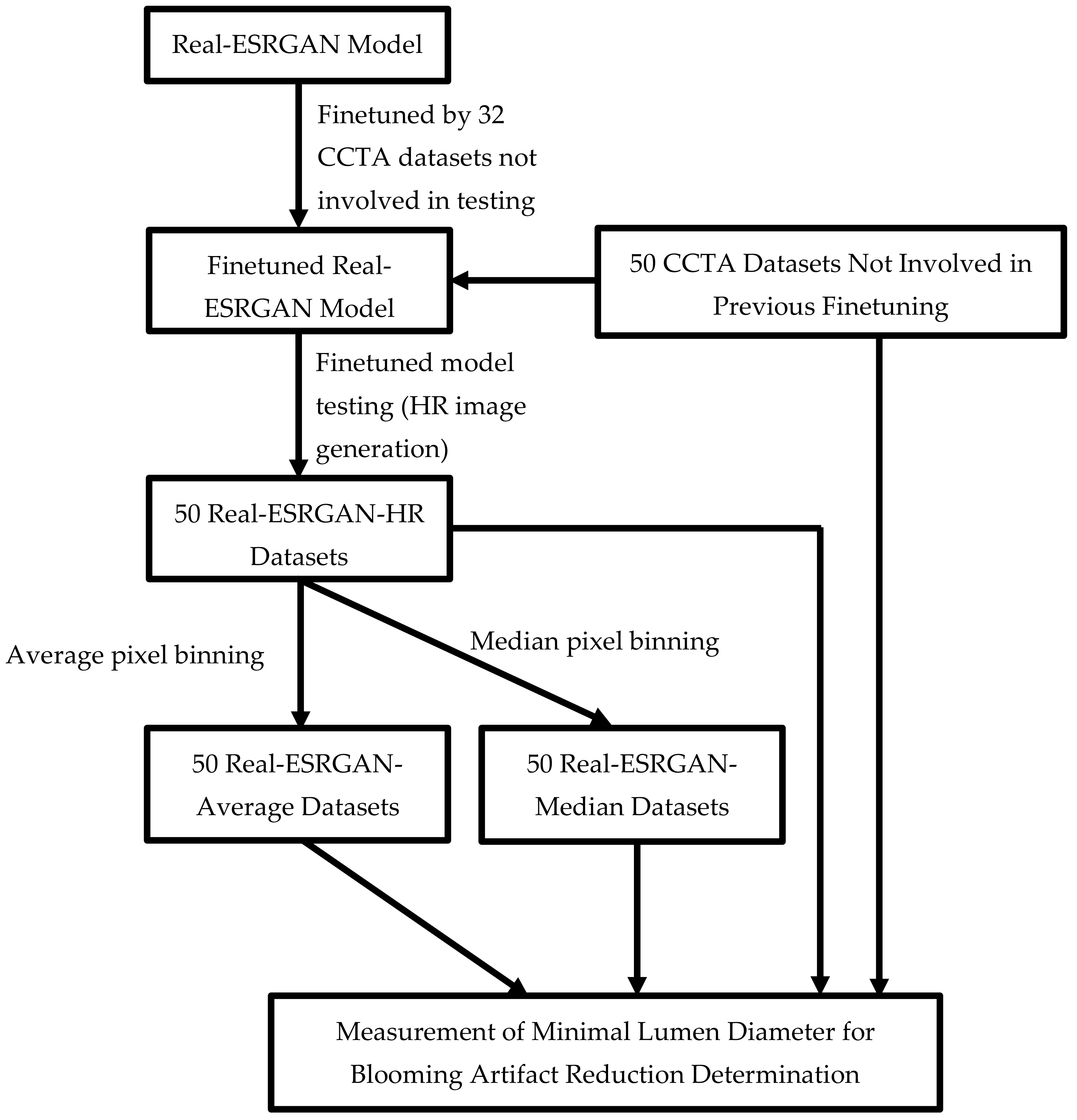
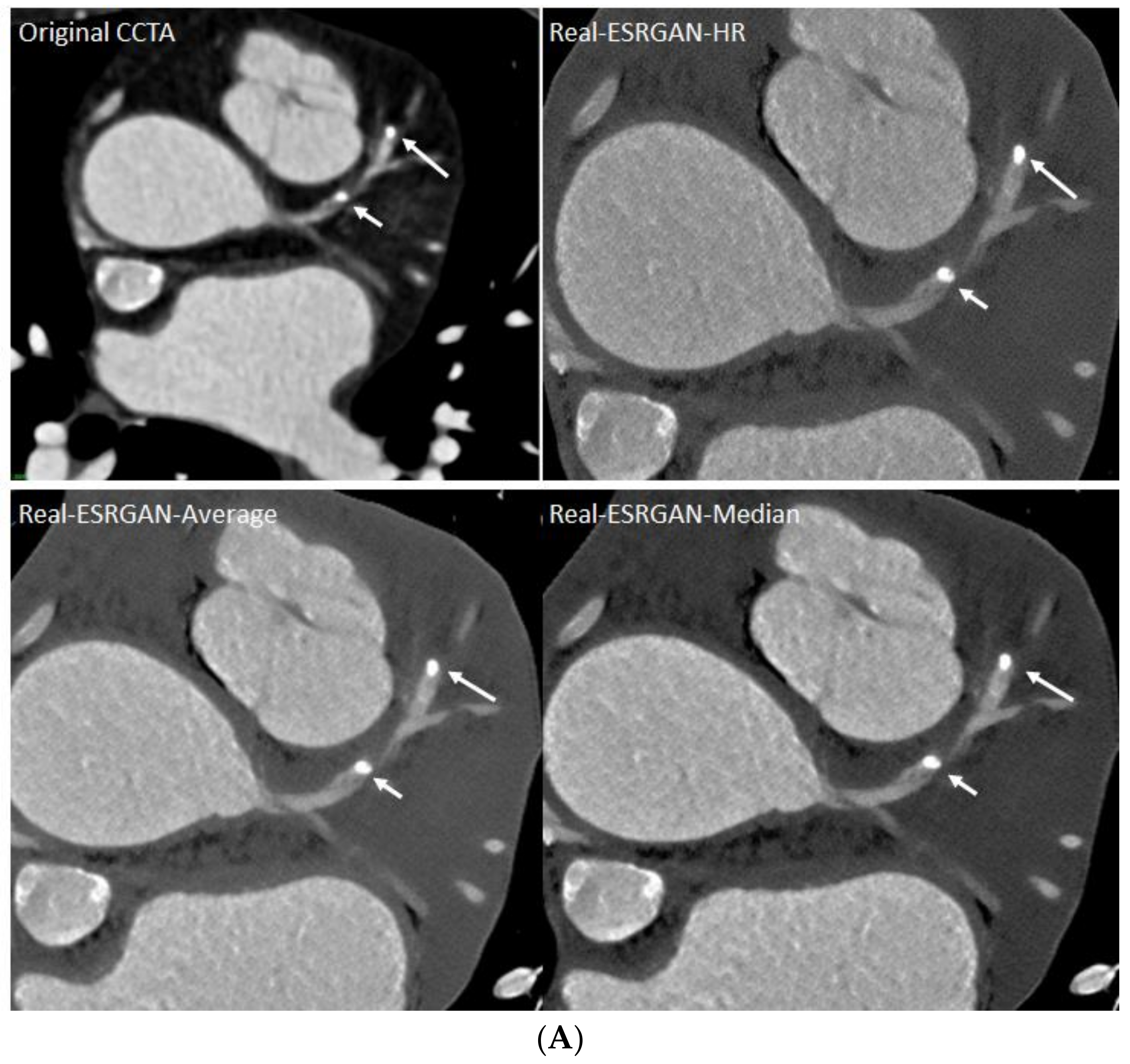
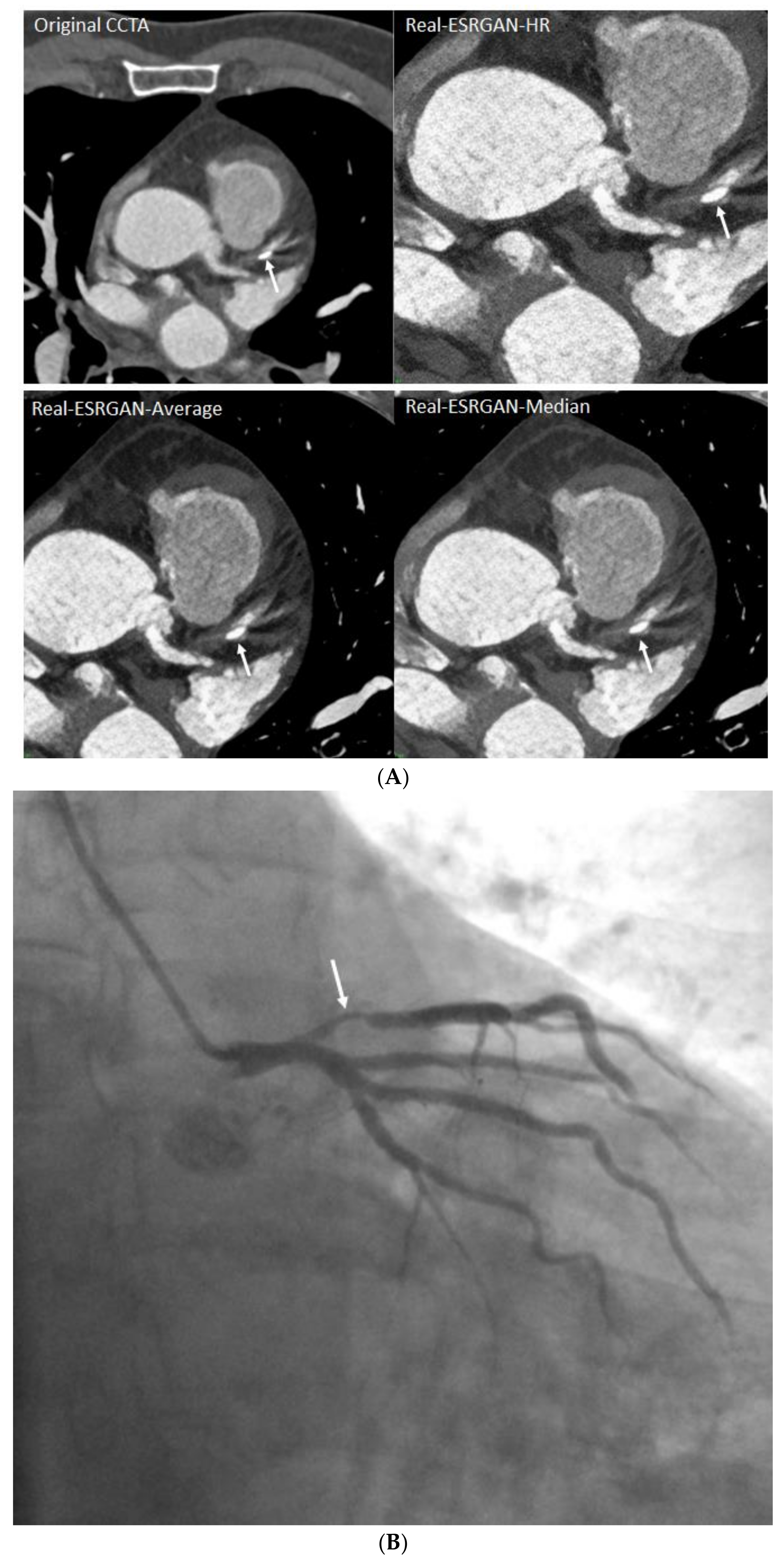
- Generation of two other CCTA datasets with an image size of 512 × 512 pixels based on the high-resolution images (Real-ESRGAN-HR) (2048 × 2048 pixels) through average (Real-ESRGAN-Average) and median (pixel) binning (Real-ESRGAN-Median) approaches for further image noise reduction.
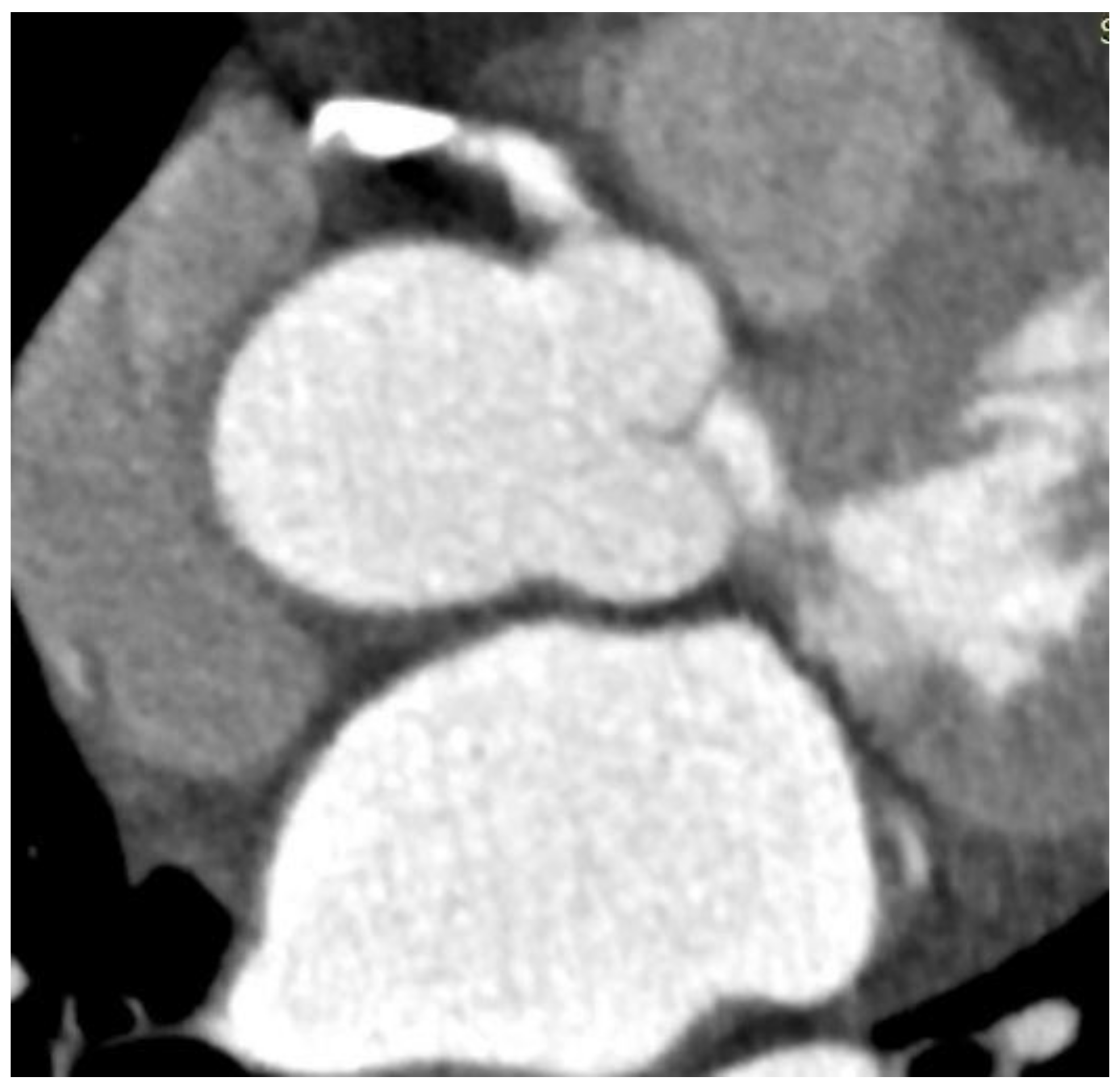
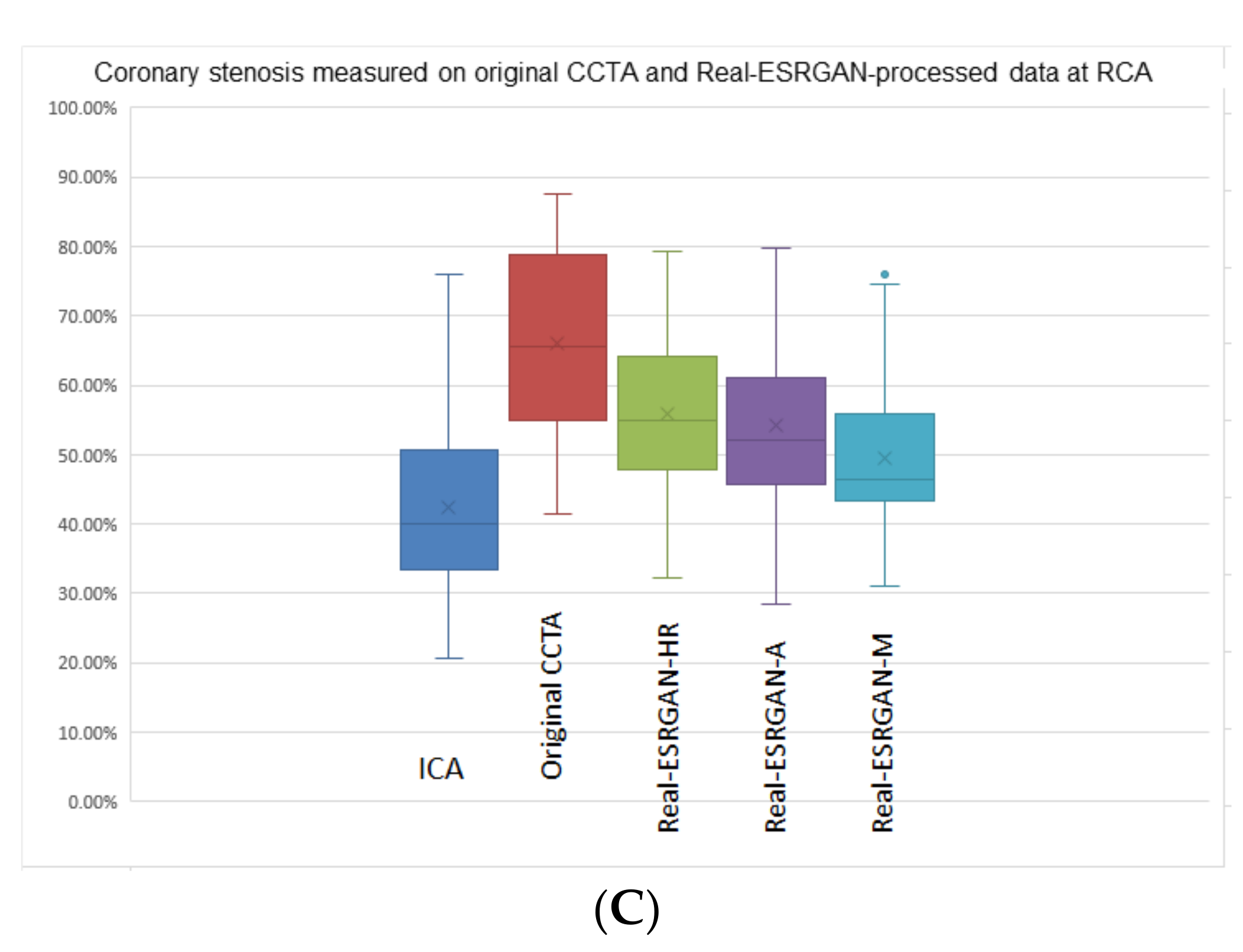
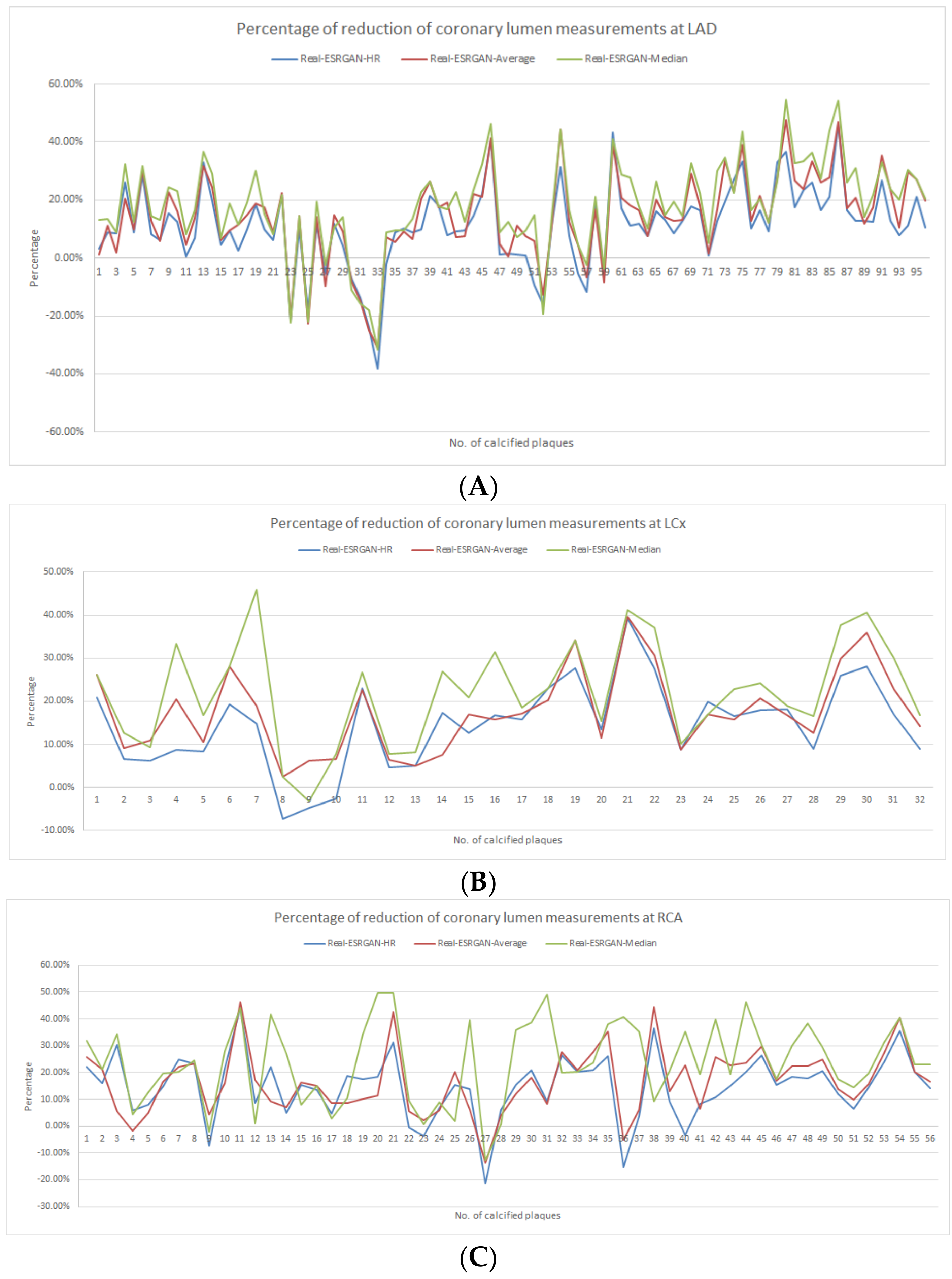
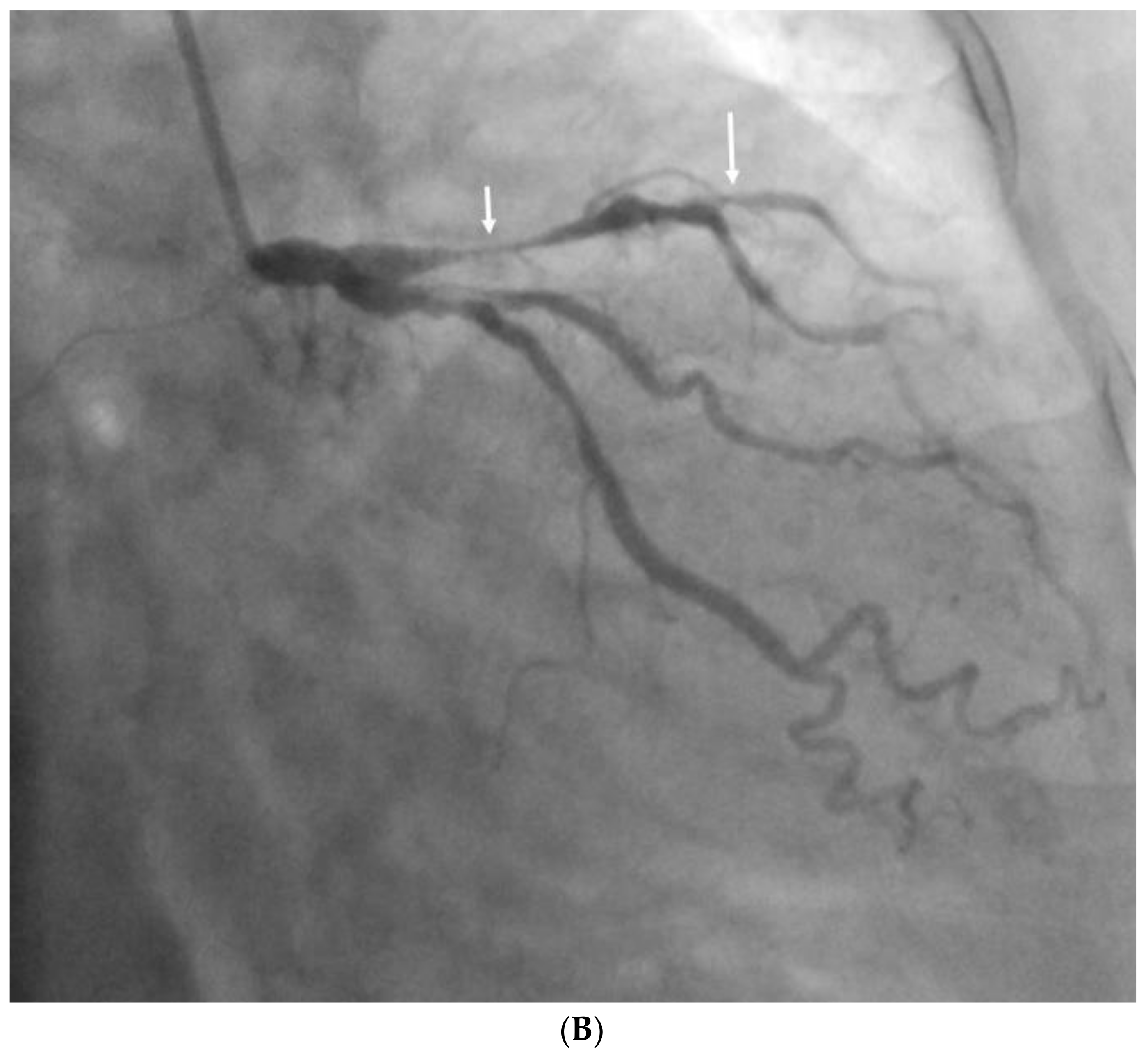
- Measurements of minimal lumen diameter (MLD) at each calcified plaque lesion of three main coronary arteries, left anterior descending (LAD), left circumflex (LCx) and right coronary artery (RCA) for the 200 datasets (50 original CCTA, 50 Real-ESRGAN-HR, 50 Real-ESRGAN-Average and 50 Real-ESRGAN-Median datasets) by a single researcher (with experience of more than 20 years in CCTA image interpretation) for three times per lesion with average value taking as the final. The MLD was measured at the narrowest part of each coronary lumen (the most extensively calcified area) to determine the degree of stenosis on the original CCTA and Real-ESRGAN-processed images with measurements on ICA as the reference to calculate the diagnostic value.
- Determination of blooming artifact reduction by using Formula (1) below.

2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kianoush, S.; Al Rifai, M.; Cainzos-Achirica, M.; Umapathi, P.; Graham, G.; Blumenthal, R.S.; Nasir, K.; Blaha, M.J. An Update on the Utility of Coronary Artery Calcium Scoring for Coronary Heart Disease and Cardiovascular Disease Risk Prediction. Curr. Atheroscler. Rep. 2016, 18, 13. [Google Scholar] [CrossRef] [PubMed]
- Al Rifai, M.; McEvoy, J.W.; Nasir, K.; Rumberger, J.; Feldman, D.; Budoff, M.J.; Blaha, M.J. Traditional cardiovascular disease risk factors associated with one-year all-cause mortality among those with coronary artery calcium scores ≥400. Atherosclerosis 2015, 241, 495–497. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Ng, C.K.C. Artificial intelligence (enhanced super-resolution generative adversarial network) for calcium deblooming in coronary computed tomography angiography: A feasibility study. Diagnostics 2022, 12, 991. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Ng, C.K.C. High calcium scores in coronary CT angiography: Effects of image post-processing on visualization and measurement of coronary lumen diameter. J. Med. Imaging Health Inform. 2015, 5, 110–116. [Google Scholar] [CrossRef]
- Sun, Z.; Ng, C.K.C.; Xu, L.; Fan, Z.; Lei, J. Coronary CT angiography in heavily calcified coronary arteries: Improvement of coronary lumen visualization and coronary stenosis assessment with image postprocessing methods. Medicine 2015, 94, e2148. [Google Scholar] [CrossRef]
- Kalisz, K.; Buethe, J.; Saboo, S.S.; Abbara, S.; Halliburton, S.; Rajiah, P. Artifacts at cardiac CT: Physics and solutions. RadioGraphics 2016, 36, 2064–2083. [Google Scholar] [CrossRef]
- Yi, Y.; Xu, C.; Xu, M.; Yan, J.; Li, Y.-Y.; Wang, J.; Yang, S.-J.; Guo, Y.-B.; Wang, Y.; Li, Y.-M.; et al. Diagnostic improvements of deep learning–based image reconstruction for assessing calcification-related obstructive coronary artery disease. Front. Cardiovasc. Med. 2021, 8, 758793. [Google Scholar] [CrossRef]
- Church, K.W.; Yuan, X.; Guo, S.; Wu, Z.; Yang, Y.; Chen, Z. Emerging trends: Deep nets for poets. Nat. Lang. Eng. 2021, 27, 631–645. [Google Scholar] [CrossRef]
- Church, K.W.; Chen, Z.; Ma, Y. Emerging trends: A gentle introduction to fine-tuning. Nat. Lang. Eng. 2021, 27, 763–778. [Google Scholar] [CrossRef]
- Han, X.; Zhang, Z.; Ding, N.; Gu, Y.; Liu, X.; Huo, Y.; Qiu, J.; Yao, Y.; Zhang, A.; Zhang, L.; et al. Pre-trained models: Past, present and future. AI Open 2021, 2, 225–250. [Google Scholar] [CrossRef]
- Wang, Y.; Wu, C.; Herranz, L.; van de Weijer, J.; Gonzalez-Garcia, A.; Raducanu, B. Transferring GANs: Generating images from limited data. In Proceedings of the European Conference on Computer Vision (ECCV) Workshops, Munich, Germany, 8–14 September 2018. [Google Scholar] [CrossRef]
- Kim, H.E.; Cosa-Linan, A.; Santhanam, N.; Jannesari, M.; Maros, M.E.; Ganslandt, T. Transfer learning for medical image classification: A literature review. BMC Med. Imaging 2022, 22, 69. [Google Scholar] [CrossRef]
- Wang, X.; Xie, L.; Dong, C.; Shan, Y. Real-ESRGAN: Training real-world blind super-resolution with pure synthetic data. In Proceedings of the 2021 IEEE/CVF International Conference on Computer Vision Workshops (ICCVW), Montreal, BC, Canada, 11–17 October 2021; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA, 2021; pp. 1905–1914. [Google Scholar] [CrossRef]
- Wang, X.; Yu, K.; Wu, S.; Gu, J.; Liu, Y.; Dong, C.; Qiao, Y.; Loy, C.C. ESRGAN: Enhanced super-resolution generative ad-versarial networks. In Proceedings of the European Conference on Computer Vision (ECCV) Workshops, Munich, Germany, 8–14 September 2018. [Google Scholar] [CrossRef]
- Lee, H.; Martin, S.; Burt, J.R.; Bagherzadeh, P.S.; Rapaka, S.; Gray, H.N.; Leonard, T.J.; Schwemmer, C.; Schoepf, U.J. Machine learning and coronary artery calcium scoring. Curr. Cardiol. Rep. 2020, 22, 90. [Google Scholar] [CrossRef]
- Wang, W.; Wang, H.; Chen, Q.; Zhou, Z.; Wang, R.; Zhang, N.; Chen, Y.; Sun, Z.; Xu, L. Coronary artery calcium score quantification using a deep-learning algorithm. Clin. Radiol. 2019, 75, 237.e11–237.e16. [Google Scholar] [CrossRef]
- Han, D.; Liu, J.; Sun, Z.; Cui, Y.; He, Y.; Yang, Z. Deep learning analysis in coronary computed tomographic angiography imaging for the assessment of patients with coronary artery stenosis. Comput. Methods Programs Biomed. 2020, 196, 105651. [Google Scholar] [CrossRef]
- Liu, C.Y.; Tang, C.X.; Zhang, X.L.; Chen, S.; Xie, Y.; Zhang, X.Y.; Qiao, H.Y.; Zhou, C.S.; Xu, P.P.; Lu, M.J.; et al. Deep learning powered coronary CT angiogrphy for detecting obstructive coronary artery disease: The effect of reader experience, calcification and image quality. Eur. J. Radiol. 2021, 142, 109835. [Google Scholar] [CrossRef]
- Sandstedt, M.; Henriksson, L.; Janzon, M.; Nyberg, G.; Engvall, J.; De Geer, J.; Alfredsson, J.; Persson, A. Evaluation of an AI-based, automatic coronary artery calcium scoring software. Eur. Radiol. 2019, 30, 1671–1678. [Google Scholar] [CrossRef]
- Zreik, M.; van Hamersvelt, R.W.; Wolterink, J.M.; Leiner, T.; Viergever, M.A.; Isgum, I. A recurrent CNN for automatic de-tection and classification of coronary artery plaque and stenosis in coronary CT angiography. IEEE. Trans. Med. Imaging. 2019, 38, 1588–1598. [Google Scholar] [CrossRef]
- Dey, D.; Cheng, V.Y.; Slomka, P.J.; Nakazato, R.; Ramesh, A.; Gurudevan, S.; Germano, G.; Berman, D.S. Automated 3-dimensional quantification of noncalcified and calcified coronary plaque from coronary CT angiography. J. Cardiovasc. Comput. Tomogr. 2009, 3, 372–382. [Google Scholar] [CrossRef]
- Litjens, G.; Ciompi, F.; Wolterink, J.M.; de Vos, B.D.; Leiner, T.; Teuwen, J.; Isgum, I. State-of-the art deep learning in cardio-vascular image analysis. JACC Cardiovasc. Imaging. 2019, 12, 1549–1565. [Google Scholar] [CrossRef]
- Wu, H.; Lu, X.; Lei, B.; Wen, Z. Automated left ventricular segmentation from cardiac magnetic resonance images via adver-sarial learning with multi-stage pose estimation network and co-discriminator. Med. Image. Anal. 2021, 68, 101891. [Google Scholar] [CrossRef]
- Wolterink, J.M.; Leiner, T.; Viergever, M.A.; Isgum, I. Generative adversarial networks for noise reduction in low-dose CT. IEEE Trans. Med Imaging 2017, 36, 2536–2545. [Google Scholar] [CrossRef]
- Van Velzen, S.G.M.; de Vos, B.D.; Noothout, J.M.H.; Verkooijen, H.M.; Viergever, M.A.; Isgum, I. Generative models for re-producible coronary calcium scoring. J. Med. Imaging 2022, 9, 52406. [Google Scholar] [CrossRef]
- Singh, A.; Kwiecinski, J.; Cadet, S.; Killekar, A.; Tzolos, E.; Williams, M.C.; Dweck, M.R.; Newby, D.E.; Dey, D.; Slomka, P.J. Automated nonlinear registration of coronary PET to CT angiography using pseudo-CT generated from PET with generative adversarial networks. J. Nucl. Cardiol. 2022. [Google Scholar] [CrossRef]
- Inage, H.; Tomizawa, N.; Otsuka, Y.; Aoshima, C.; Kawaguchi, Y.; Takamura, K.; Matsumori, R.; Kamo, Y.; Nozaki, Y.; Takahashi, D.; et al. Use of a deep-learning-based lumen extraction method to detect significant stenosis on coronary computed tomography angiography in patients with severe coronary calcification. Egypt. Heart J. 2022, 74, 43. [Google Scholar] [CrossRef]
- Schork, N.J. Artificial intelligence and personalized medicine. Cancer Treat. Res. 2019, 178, 265–283. [Google Scholar] [CrossRef]
- Ng, C.K.C. Artificial intelligence for radiation dose optimization in pediatric radiology: A systematic review. Children 2022, 9, 1044. [Google Scholar] [CrossRef]
- Kleinfelder, T.R.; Ng, C.K.C. Effects of image postprocessing in digital radiography to detect wooden, soft tissue foreign bodies. Radiol. Technol. 2022, 93, 544–554. Available online: https://pubmed.ncbi.nlm.nih.gov/35790309/ (accessed on 25 July 2022).
- Petri, S.A.; Ng, C.K.C. Comparison of the performance of computed radiography and direct radiography in glass soft tissue foreign body visualisation. S. Afr. Radiogr. 2018, 56, 18–25. Available online: https://sar.org.za/index.php/sar/article/view/458 (accessed on 25 July 2022).
- Yazici, Y.; Foo, C.S.; Winkler, S.; Yap, K.H.; Chandrasekhar, V. Empirical analysis of overfitting and mode drop in GAN training. In Proceedings of the 2020 IEEE International Conference on Image Processing (ICIP), Abu Dhabi, United Arab Emirates, 25–28 October 2020. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Coronary Arteries/No. Plaques | TP | FP | TN | FN | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | PLR | NLR | AUC |
|---|---|---|---|---|---|---|---|---|---|---|---|
| LAD | |||||||||||
| Original CCTA | 19 | 60 | 17 | 0 | 100 (82.3, 100) | 22.1 (13.4, 32.9) | 24.1 (21.9, 26.3) | 100 | 1.28 (1.13, 1.44) | 0.00 | 0.69 (0.57, 0.82) |
| Real-ESRGAN-HR | 18 | 51 | 26 | 1 | 94.7 (73.9, 99.8) | 33.8 (23.4, 45.4) | 26.1 (22.5, 29.9) | 96.3 (78.9, 99.4) | 1.43 (1.18, 1.73) | 0.16 (0.02, 1.08) | 0.68 (0.56, 0.80) |
| Real-ESRGAN-Average | 17 | 47 | 30 | 2 | 89.5 (66.8, 98.7) | 38.9 (28.0, 50.7) | 26.6 (22.2, 31.4) | 93.7 (79.7, 98.3) | 1.47 (1.16, 1.86) | 0.27 (0.07, 1.03) | 0.69 (0.57, 0.80) |
| Real-ESRGAN-Median | 17 | 37 | 40 | 2 | 89.5 (66.9, 98.7) | 51.9 (40.3, 63.5) | 31.5 (25.8, 37.8) | 95.2 (84.1, 98.7) | 1.86 (1.41, 2.46) | 0.20 (0.05, 0.77) | 0.73 (0.62, 0.85) |
| LCx | |||||||||||
| Original CCTA | 8 | 21 | 3 | 0 | 100 (63.1, 100) | 12.5 (2.6, 32.4) | 27.6 (24.7, 30.7) | 100 | 1.14 (0.98, 1.33) | 0.00 | 0.67 (0.48, 0.86) |
| Real-ESRGAN-HR | 8 | 13 | 11 | 0 | 100 (63.1, 100) | 45.8 (25.6, 67.2) | 38.1 (29.9, 47.1) | 100 | 1.85 (1.28, 2.67) | 0.00 | 0.67 (0.48, 0.86) |
| Real-ESRGAN-Average | 7 | 13 | 11 | 1 | 87.5 (47.3 99.7) | 45.8 (25.5, 67.2) | 35.0 (25.5, 45.8) | 91.7 (62.6, 98.6) | 1.62 (1.03, 2.54) | 0.27 (0.04, 1.79) | 0.66 (0.47, 0.85) |
| Real-ESRGAN-Median | 7 | 9 | 15 | 1 | 87.5 (47.3, 99.7) | 62.5 (40.6, 81.2) | 43.8 (30.3, 58.1) | 93.7 (70.0, 98.9) | 2.33 (1.31, 4.16) | 0.20 (0.03, 1.28) | 0.72 (0.55, 0.89) |
| RCA | |||||||||||
| Original CCTA | 16 | 33 | 7 | 0 | 100 (79.4, 100) | 17.5 (7.3, 32.8) | 32.7 (29.6, 35.9) | 100 | 1.21 (1.05, 1.39) | 0.00 | 0.76 (0.64, 0.89) |
| Real-ESRGAN-HR | 16 | 20 | 20 | 0 | 100 (79.4, 100) | 50.0 (33.8, 66.2) | 44.4 (36.9, 52.2) | 100 | 2.00 (1.47, 2.73) | 0.00 | 0.84 (0.73, 0.94) |
| Real-ESRGAN-Average | 15 | 16 | 24 | 1 | 93.7 (69.8, 99.8) | 60.0 (43.3, 75.1) | 48.4 (38.6, 58.3) | 96.0 (77.9, 99.4) | 2.34 (1.57, 3.50) | 0.10 (0.02, 0.71) | 0.85 (0.75, 0.95) |
| Real-ESRGAN-Median | 13 | 8 | 32 | 3 | 81.3 (54.4, 95.9) | 80.0 (64.4, 90.9) | 61.9 (45.6, 75.9) | 91.4 (79.2, 96.7) | 4.06 (2.09, 7.88) | 0.23 (0.08, 0.66) | 0.73 (0.58, 0.89) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, Z.; Ng, C.K.C. Finetuned Super-Resolution Generative Adversarial Network (Artificial Intelligence) Model for Calcium Deblooming in Coronary Computed Tomography Angiography. J. Pers. Med. 2022, 12, 1354. https://doi.org/10.3390/jpm12091354
Sun Z, Ng CKC. Finetuned Super-Resolution Generative Adversarial Network (Artificial Intelligence) Model for Calcium Deblooming in Coronary Computed Tomography Angiography. Journal of Personalized Medicine. 2022; 12(9):1354. https://doi.org/10.3390/jpm12091354
Chicago/Turabian StyleSun, Zhonghua, and Curtise K. C. Ng. 2022. "Finetuned Super-Resolution Generative Adversarial Network (Artificial Intelligence) Model for Calcium Deblooming in Coronary Computed Tomography Angiography" Journal of Personalized Medicine 12, no. 9: 1354. https://doi.org/10.3390/jpm12091354