1. Introduction
Psoriasis is a chronic inflammatory and immune-mediated disease characterized by cutaneous and systemic manifestations, and affecting 1–3% of the population in Western Europe [
1]. Compared with the general population, psoriatic patients have an increased risk of developing other chronic diseases as comorbidities, including cardiovascular diseases (CVDs). CVDs are one of the most common comorbidities in psoriatic patients, and this may affect the severity of the disease and decrease both the quality of life and the lifespan of psoriatic patients [
2].
A combination of several exogenous and endogenous factors, including genetic predisposition, is well documented in the etiology and progression of both psoriasis and CVD [
3,
4,
5,
6,
7]. The presence of systemic inflammation in combination with metabolic abnormalities might explain the high incidence of CVD in psoriatic patients [
2,
8].
Genetic and genome-wide association studies have recently allowed for the identification of a common genetic background of psoriasis and concomitant cardiovascular risk factors, suggesting pleiotropic mechanisms of interactions involving pro-inflammatory pathways [
6]. However, other factors besides genetic background may explain the prevalence of CVD in psoriasis patients.
Gut microbiome dysbiosis is considered as a triggering factor for psoriasis onset as it may promote chronic systemic inflammation. Dysbiosis may indeed contribute to the increase in bacteria promoting the production of harmful compounds involved in the inflammatory response, with a central role in the systemic inflammation of several diseases [
9,
10].
Significant alterations of the gut microbiome composition were found in psoriatic patients compared with healthy controls, mainly including a reduction in
Bacteroidetes and increase in
Firmicutes phyla [
9].
Cumulative evidence has also demonstrated that the gut microbiome may have a role in the development and maintenance of CVD [
11,
12]. Compared with healthy controls, patients with CVD showed a peculiar gut microbiome profile, including a reduction in
Bacteroidetes and increase in
Proteobacteria phyla [
13].
Despite the established role of the gut microbiome composition in the development and maintenance of both psoriasis and CVD, a possible link between the gut microbiome composition and the occurrence of CVD in psoriatic patients is still unknown.
In this study, we characterized and compared the gut microbiome composition in psoriatic patients with and without CVD to investigate whether gut dysbiosis might influence the occurrence of CVD in psoriatic patients, with possible clinical relevance.
2. Materials and Methods
A cohort of 28 psoriatic patients, including 17 cases with CVD and 11 cases without CVD, were diagnosed and enrolled at the Psoriasis Center of Policlinico “Umberto I”, Sapienza University of Rome. All patients involved in this study signed an informed consent form with a detailed description of the study protocol, approved by the local ethics committee of Sapienza University of Rome (protocol 873/13). The study was performed according to the principles of the Declaration of Helsinki.
The main personal and clinical-pathological data including sex, age at enrollment and at diagnosis, duration of the disease, body mass index (BMI), type and degree of psoriasis, and anti-psoriatic biological treatment were collected for all patients.
For each case, fecal samples were obtained within 24 h of production and were stored at −20 °C in sterile containers until use. To reduce possible biases due to environmental effects on the microbiome composition, the study enrolled Caucasian individuals from the same geographic area (Lazio, Italy), all of whom had a similar diet and had not received probiotics or antibiotics in the 6 months prior to recruitment. Fecal bacterial DNA was extracted using the commercially available InviMag Stool DNA Kit/KF96 (Invitek Molecular, Berlin, Germany) and analyzed by 16s rRNA gene sequencing on the Illumina MiSeq platform. The sequencing data were processed using QIIME2 version 2019.1 and DADA2 software, and the details including raw and clean data per sample and number of reads passing quality filters were as previously reported [
10]. The operational taxonomic units (OTUs) per sample were generated after the filtering by quality and length and purification from chimeric sequences; the rarefaction analysis was performed on the OTU table in order to normalize samples at the minimum number of reads, as previously described [
10]. The sequencing data are available upon reasonable request to the corresponding author.
Bioinformatics analyses were performed to determine the diversity in the gut microbiome composition of psoriatic patients with and without CVD.
Taxonomy was assigned using the Greengenes v.13-8 database and the differential microbial abundance between the two groups was performed using the DeSeq2 package of R/Bioconductor, as previously described [
10].
Statistical analysis of the clinical-pathological features in the case series was performed using the Wilcoxon rank-sum test for numerical variables, and the χ2 test for categorical variables. Results were considered statistically significant at p ≤ 0.05.
3. Results and Discussion
The personal and clinical-pathological data of the 28 psoriatic patients included in the study are shown in
Table 1.
Psoriatic patients with CVD were significantly older at enrollment (
p = 0.001) and at diagnosis (
p = 0.049) and had a significantly higher BMI (
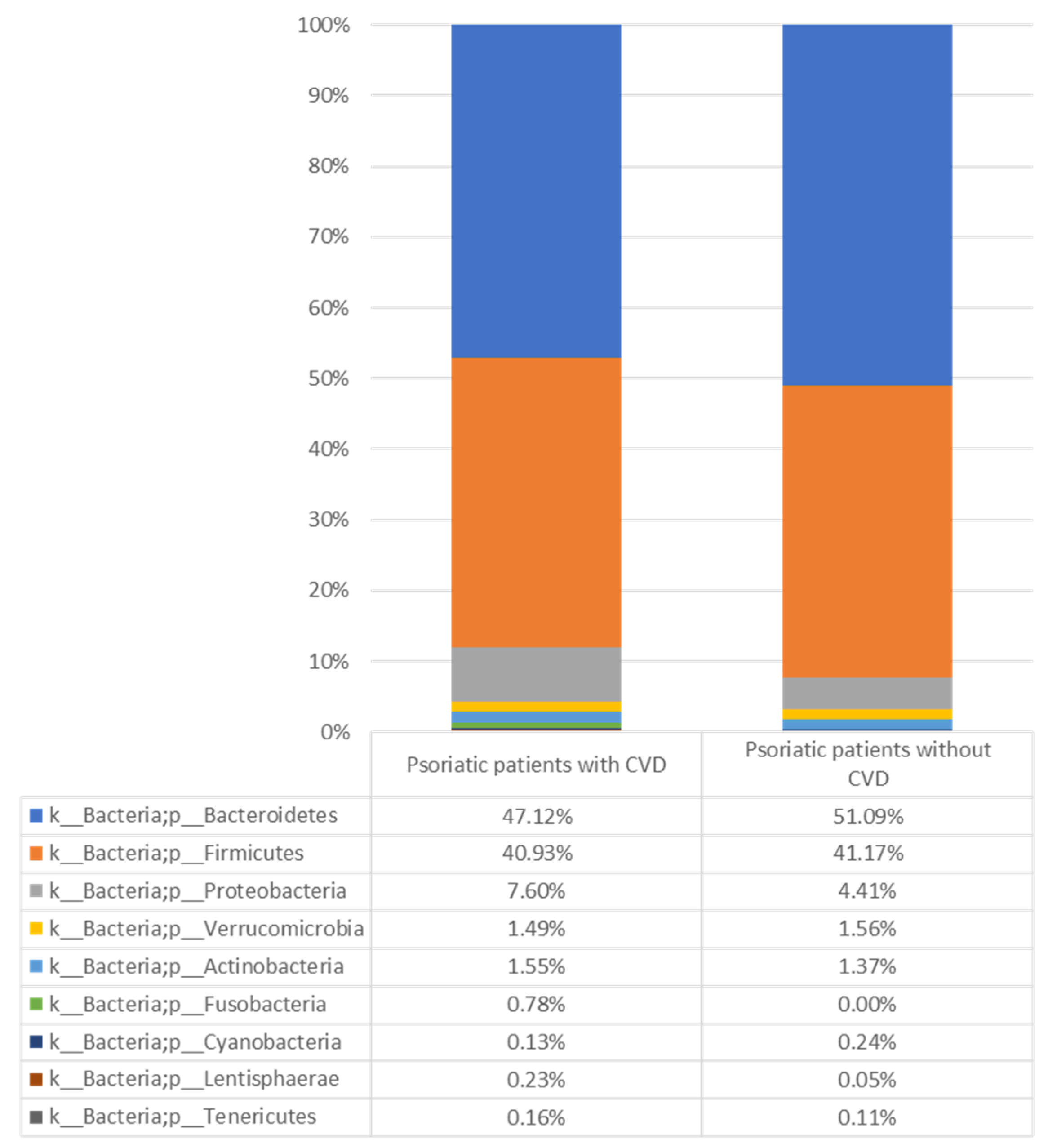
p = 0.003) compared with psoriatic patients without CVD. Among psoriatic patients with and without CVD, five and four cases, respectively, were undergoing biological therapy. We subsequently examined the gut microbiome composition of psoriatic patients with and without CVD, analyzing the abundance of specific bacterial groups at various taxonomic levels. At the phylum level, we observed a significantly higher abundance of
Proteobacteria, known to promote a status of systemic inflammation [
13] in psoriatic patients with CVD, compared with those without CVD (
p = 0.045) (
Figure 1 and
Supplementary Figure S1).
Notably, an increased abundance of Proteobacteria was previously reported in patients with coronary artery disease [
13]. Our findings suggest that a higher abundance of Proteobacteria in psoriatic patients with CVD might contribute to inflammatory processes related to both psoriasis and CVD by means of increasing the production of inflammatory cytokines. In addition, we observed a significantly higher proportion of the family
Barnesiellaceae, the genera
Coprococcus and
Phascolarctobacterium, and the species
Bacteroides ovatus in psoriatic patients with CVD (
Table 2).
A higher abundance of
Barnesiellaceae and
Phascolarctobacterium, known to produce elevated quantities of short-chain fatty acids associated with both hypercholesterolemia and hypertriglyceridemia, was previously reported in CVD patients compared with healthy controls [
12,
14]. Our findings suggest that a higher prevalence of
Barnesiellaceae and
Phascolarctobacterium might be considered as risk factors for developing CVD in psoriatic patients.
Previous studies showed controversial associations of
Barnesiellaceae and
Phascolarctobacterium with metabolic status (measured as BMI), as some studies reported higher levels in higher BMI patients, and others reported an inverse correlation [
15,
16,
17,
18]. These contrasting results may be due to other additional features that may act as confounding factors. In our series, psoriatic patients with CVD were significantly older and had a significantly higher BMI compared with psoriatic patients without CVD. Given the relatively small number of patients analyzed, we cannot rule out the possible effects of age and BMI as confounding factors for the observed associations. On the other hand, our observations may hint at a possible link between gut microbiome composition and metabolic factors, for example, a high BMI, suggesting a possible concurrent role of gut microbiome alterations and traditional cardiovascular risk factors in psoriatic patients.
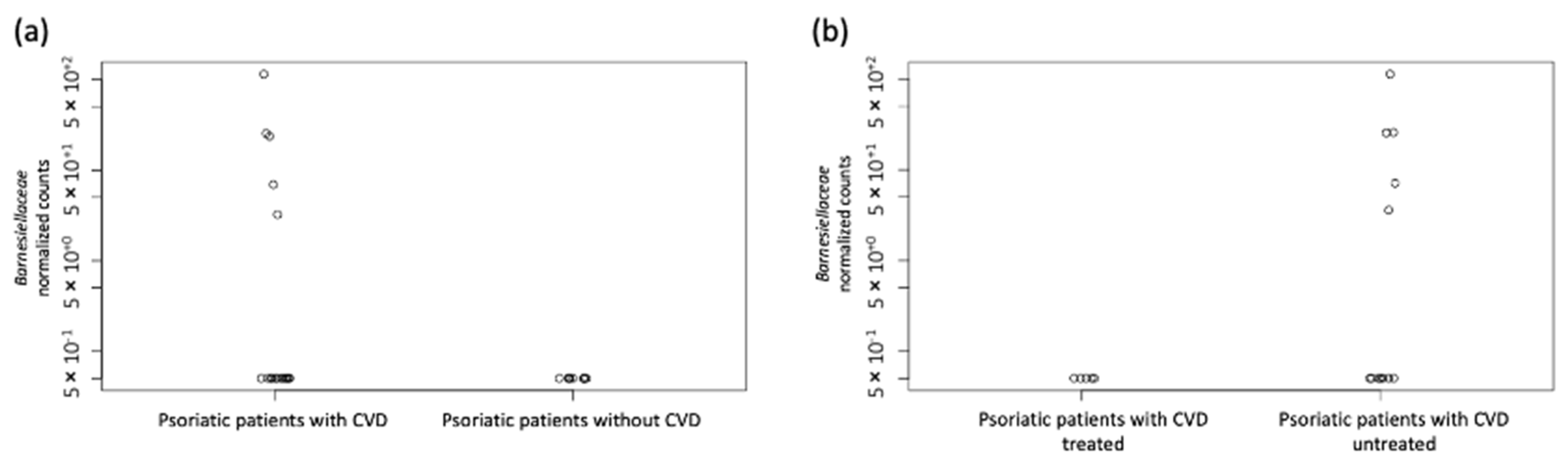
Among psoriatic patients with CVD, patients undergoing biological therapy had a lower abundance of the family
Barnesiellaceae (
p = 7.79 × 10
−11) and showed abundance levels comparable to those found in psoriatic patients without CVD (
Figure 2a,b).
Whether biological treatment may affect the gut microbiome, with a possible impact on cardiovascular comorbidities in psoriatic patients, deserves to be further validated in a larger cohort of patients.
The order
Clostridiales and the species
Alistipes finegoldii and
Roseburia faecis were found significantly more abundant in psoriatic patients without CVD (
Table 2).
Alistipes finegoldii and
Roseburia faecis were suggested as playing a role in improving obesity [
12] and in producing butyrate with vasodilatory properties [
14], respectively. Our findings suggest that these bacteria might positively impact traditional cardiovascular risk factors in psoriatic patients.
This study has a few limitations. First, it is a pilot study on a small cohort of patients; thus, it was not possible to exclude the possible influence of confounding factors for the observed associations. On the other hand, the analyzed cohort was collected through stringent inclusion criteria in order to minimize environmental biases. Another possible limitation is represented by data analysis. It is well known that microbiome data analysis is a computational challenge, and a standardization of the best pipeline is currently lacking. The analysis pipeline, whose results are shown here, is based on evidence from previous results and evidence from recent methodological comparisons [
10,
19].
Further studies using multiple functional and computational approaches are needed to confirm our observations regarding the gut microbiome dysbiosis and the possible functional relationship among dysregulated taxa in the risk of CVD in psoriatic patients.
4. Conclusions
This study highlighted differences in the gut microbiome composition in psoriatic patients with and without CVD and suggested that gut microbiome dysbiosis may be associated with an increased risk of CVD in psoriatic patients, in addition to traditional cardiovascular risk factors (i.e., high BMI), with possible clinical implications in the management of psoriasis and its associated comorbidities. Furthermore, our findings hinted at a possible impact of biological therapy on the gut microbiome composition, an observation which deserves further validation. Thus, preventive and therapeutic strategies aimed at restoring the gut microbiome symbiosis might potentially represent useful approaches in the management of psoriasis and its associated comorbidities. Further studies on larger cohorts of patients will provide more insights regarding the impact of biological drugs on gut microbiome composition and on bacteria that could play an important role for the host’s cardiovascular health, in terms of treatment and prevention of associated diseases.
Supplementary Materials
The following supporting information can be downloaded at:
https://www.mdpi.com/article/10.3390/jpm12071118/s1, Figure S1: Relative abundance (%) of the gut microbes identified at phylum level represented by stacked bars of each subject (1–28) from each group of psoriatic patients with and without CVD (1–17 and 18–28, respectively).
Author Contributions
Conceptualization, L.O. and A.G.R.; data curation, V.V., V.S., A.B., F.M., M.R., S.G. and G.P.; formal analysis, V.V., V.S. and M.R.; funding acquisition, L.O.; investigation, V.V. and V.S.; methodology, V.V., V.S., A.B., F.M., M.R. and S.G.; project administration, L.O. and A.G.R.; supervision, L.O. and A.G.R.; writing—original draft, V.V., V.S., L.O. and A.G.R.; writing—review and editing, all authors. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Fondazione AIRC (Associazione Italiana Ricerca sul Cancro) under IG 2018 grant number ID. 21389 to L.O.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Sapienza University of Rome (Protocol code 887/13).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors wish to thank all the patients who participated in our study. V.V. is supported by FIRC-AIRC (triennial fellowship “Carlo Zanotti”). V.S. is supported by the Fondazione Umberto Veronesi. A.B. contributed to this paper as a recipient of the Ph.D. program of Molecular Medicine of Sapienza, University of Rome.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Parisi, R.; Iskandar, I.Y.K.; Kontopantelis, E.; Augustin, M.; Griffiths, C.E.M.; Ashcroft, D.M.; Global Psoriasis Atlas. National, regional, and worldwide epidemiology of psoriasis: Systematic analysis and modelling study. BMJ 2020, 369, m1590. [Google Scholar] [CrossRef] [PubMed]
- Woo, Y.R.; Park, C.J.; Kang, H.; Kim, J.E. The Risk of Systemic Diseases in Those with Psoriasis and Psoriatic Arthritis: From Mechanisms to Clinic. Int. J. Mol. Sci. 2020, 21, 7041. [Google Scholar] [CrossRef] [PubMed]
- Richetta, A.G.; Silvestri, V.; Giancristoforo, S.; Rizzolo, P.; D’Epiro, S.; Graziano, V.; Mattozzi, C.; Navazio, A.S.; Campoli, M.; D’Amico, C.; et al. A-1012G Promoter Polymorphism of Vitamin D Receptor Gene Is Associated with Psoriasis Risk and Lower Allele-Specific Expression. DNA Cell Biol. 2014, 33, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Coto-Segura, P.; Coto, E.; Mas-Vidal, A.; Morales, B.; Alvarez, V.; Díaz, M.; Alonso, B.; Santos-Juanes, J. Influence of endothelial nitric oxide synthase polymorphisms in psoriasis risk. Arch. Dermatol. Res. 2011, 303, 445–449. [Google Scholar] [CrossRef] [Green Version]
- Newhouse, S.J.; Wallace, C.; Dobson, R.; Mein, C.; Pembroke, J.; Farrall, M.; Clayton, D.; Brown, M.; Samani, N.; Dominiczak, A.; et al. Haplotypes of the WNK1 gene associate with blood pressure variation in a severely hypertensive population from the British Genetics of Hypertension study. Hum. Mol. Genet. 2005, 14, 1805–1814. [Google Scholar] [CrossRef] [PubMed]
- Purzycka-Bohdan, D.; Kisielnicka, A.; Bohdan, M.; Szczerkowska-Dobosz, A.; Sobalska-Kwapis, M.; Nedoszytko, B.; Nowicki, R.J. Analysis of the Potential Genetic Links between Psoriasis and Cardiovascular Risk Factors. Int. J. Mol. Sci. 2021, 22, 9063. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Li, Y.; Zuo, X.-B.; Tang, H.-Y.; Tang, X.-F.; Gao, J.-P.; Sheng, Y.-J.; Yin, X.-Y.; Zhou, F.-S.; Zhang, C.; et al. Identification of a Missense Variant in LNPEP that Confers Psoriasis Risk. J. Investig. Dermatol. 2014, 134, 359–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masson, W.; Lobo, M.; Molinero, G. Psoriasis and Cardiovascular Risk: A Comprehensive Review. Adv. Ther. 2020, 37, 2017–2033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sikora, M.; Stec, A.; Chrabaszcz, M.; Knot, A.; Waskiel-Burnat, A.; Rakowska, A.; Olszewska, M.; Rudnicka, L. Gut Microbiome in Psoriasis: An Updated Review. Pathogens 2020, 9, 463. [Google Scholar] [CrossRef] [PubMed]
- Valentini, V.; Silvestri, V.; Marraffa, F.; Greco, G.; Bucalo, A.; Grassi, S.; Gagliardi, A.; Mazzotta, A.; Ottini, L.; Richetta, A.G. Gut microbiome profile in psoriatic patients treated and untreated with biologic therapy. J. Dermatol. 2021, 48, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Sikora, M.; Kiss, N.; Stec, A.; Giebultowicz, J.; Samborowska, E.; Jazwiec, R.; Dadlez, M.; Olszewska, M.; Rudnicka, L. Trimethylamine N-Oxide, a Gut Microbiota-Derived Metabolite, Is Associated with Cardiovascular Risk in Psoriasis: A Cross-Sectional Pilot Study. Dermatol. Ther. 2021, 11, 1277–1289. [Google Scholar] [CrossRef] [PubMed]
- Dan, X.; Mushi, Z.; Baili, W.; Han, L.; Enqi, W.; Huanhu, Z.; Shuchun, L. Differential Analysis of Hypertension-Associated Intestinal Microbiota. Int. J. Med. Sci. 2019, 16, 872–881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Alcoholado, L.; Castellano-Castillo, D.; Jordán-Martínez, L.; Moreno-Indias, I.; Cardila-Cruz, P.; Elena, D.; Muñoz-Garcia, A.J.; Queipo-Ortuño, M.I.; Jimenez-Navarro, M. Role of Gut Microbiota on Cardio-Metabolic Parameters and Immunity in Coronary Artery Disease Patients with and without Type-2 Diabetes Mellitus. Front. Microbiol. 2017, 8, 1936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mushtaq, N.; Hussain, S.; Zhang, S.; Yuan, L.; Li, H.; Ullah, S.; Wang, Y.; Xu, J. Molecular characterization of alterations in the intestinal microbiota of patients with grade 3 hypertension. Int. J. Mol. Med. 2019, 44, 513–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, C.-M.; Huang, W.-C.; Weng, S.-L.; Tseng, H.-C.; Liang, C.; Wang, W.-C.; Yang, T.; Yang, T.-L.; Weng, C.-T.; Chang, T.-H.; et al. Systematic Analysis of the Association between Gut Flora and Obesity through High-Throughput Sequencing and Bioinformatics Approaches. BioMed Res. Int. 2014, 2014, 906168. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.; Harrington, J.M.; Millar, S.R.; Perry, I.J.; O’Toole, P.W.; Phillips, C.M. Gut Microbiota Associations with Metabolic Health and Obesity Status in Older Adults. Nutrients 2020, 12, 2364. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Chen, R.; McCormick, K.L.; Zhang, Y.; Lin, X.; Yang, X. The role of the gut microbiota on the metabolic status of obese children. Microb. Cell Factories 2021, 20, 53. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Andreu-Sánchez, S.; Kuipers, F.; Fu, J. Gut microbiome and bile acids in obesity-related diseases. Best Pract. Res. Clin. Endocrinol. Metab. 2021, 35, 101493. [Google Scholar] [CrossRef] [PubMed]
- Calgaro, M.; Romualdi, C.; Waldron, L.; Risso, D.; Vitulo, N. Assessment of statistical methods from single cell, bulk RNA-seq, and metagenomics applied to microbiome data. Genome Biol. 2020, 21, 191. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 


{kind=link}
{kind=link}