
How to Improve Healthcare for Patients with Multimorbidity and Polypharmacy in Primary Care: A Pragmatic Cluster-Randomized Clinical Trial of the MULTIPAP Intervention

 , , ,
, , ,  , , , , , , , , , , , and add
Show full author list
, , , , , , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Methods
2.2. Recruitment
2.3. Randomization and Masking
2.4. Intervention
2.5. Outcomes
2.6. Sample Size
2.7. Statistical Analysis
2.8. Role of the Funding Source
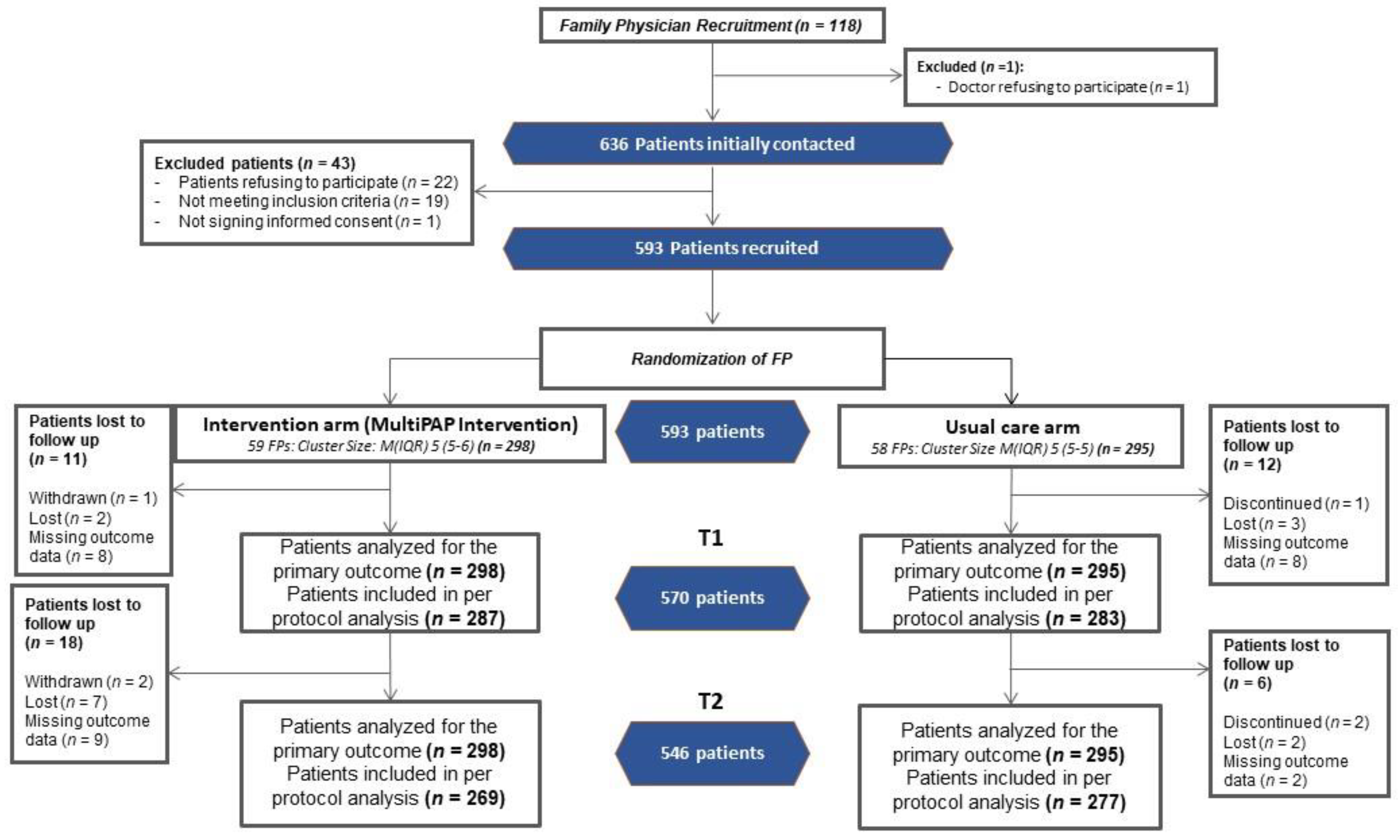
3. Results
3.1. Characteristics of the Study Participants
3.2. Primary Outcomes
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Academy of Medical Sciences. Multimorbidity: A Priority for Global Health Research; The Academy of Medical Sciences: London, UK, 2018. [Google Scholar]
- Valderas, J.M.; Gangannagaripalli, J.; Nolte, E.; Boyd, C.M.; Roland, M.; Sarria-Santamera, A.; Jones, E.; Rijken, M. Quality of care assessment for people with multimorbidity. J. Intern. Med. 2019, 285, 289–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prados-Torres, A.; Poblador-Plou, B.; Gimeno-Miguel, A.; Calderón-Larrañaga, A.; Poncel-Falcó, A.; Gimeno-Feliú, L.A.; González-Rubio, F.; Laguna-Berna, C.; Marta-Moreno, J.; Clerencia-Sierra, M.; et al. Cohort Profile: The Epidemiology of Chronic Diseases and Multimorbidity. The EpiChron Cohort Study. Int. J. Epidemiol. 2018, 47, 382–384f. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad Consumo y Bienestar Social. Encuesta Nacional de Salud España 2017; Ministerio de Sanidad Consumo y Bienestar Social: Madrid, Spain, 2018.
- Fortin, M.; Bravo, G.; Hudon, C.; Lapointe, L.; Almirall, J.; Dubois, M.F.; Vanasse, A. Relationship between multimorbidity and health-related quality of life of patients in primary care. Qual. Life Res. 2006, 15, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Calderon-Larranaga, A.; Poblador-Plou, B.; Gonzalez-Rubio, F.; Gimeno-Feliu, L.A.; Abad-Diez, J.M.; Prados-Torres, A.; Calderón-Larrañaga, A.; Poblador-Plou, B.; González-Rubio, F.; Gimeno-Feliu, L.A.; et al. Multimorbidity, polypharmacy, referrals, and adverse drug events: Are we doing things well? Br. J. Gen. Pract. 2012, 62, e821–e826. [Google Scholar] [CrossRef] [Green Version]
- Marengoni, A.; Angleman, S.; Melis, R.; Mangialasche, F.; Karp, A.; Garmen, A.; Meinow, B.; Fratiglioni, L. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 2011, 10, 430–439. [Google Scholar] [CrossRef]
- Zullo, A.R.; Gray, S.L.; Holmes, H.M.; Marcum, Z.A. Screening for Medication Appropriateness in Older Adults. Clin. Geriatr. Med. 2018, 34, 39–54. [Google Scholar] [CrossRef]
- Klarin, I.; Wimo, A.; Fastbom, J. The association of inappropriate drug use with hospitalisation and mortality: A population-based study of the very old. Drugs Aging 2005, 22, 69–82. [Google Scholar] [CrossRef]
- Munson, J.C.; Bynum, J.P.W.; Bell, J.-E.; Cantu, R.; McDonough, C.; Wang, Q.; Tosteson, T.D.; Tosteson, A.N.A. Patterns of Prescription Drug Use Before and After Fragility Fracture. JAMA Intern. Med. 2016, 176, 1531. [Google Scholar] [CrossRef]
- Leelakanok, N.; Holcombe, A.L.; Lund, B.C.; Gu, X.; Schweizer, M.L. Association between polypharmacy and death: A systematic review and meta-analysis. J. Am. Pharm. Assoc. 2017, 57, 729–738.e10. [Google Scholar] [CrossRef]
- O’Mahony, D.; Gallagher, P.F.; Lavan, A.H.; Gallagher, P.F.; O’Mahony, D.; O’Mahony, D.; Gallagher, P.F.; Lavan, A.H. Methods to reduce prescribing errors in elderly patients with multimorbidity. Clin. Interv. Aging 2016, 11, 857–866. [Google Scholar] [CrossRef] [Green Version]
- Spinewine, A.; Schmader, K.E.; Barber, N.; Hughes, C.; Lapane, K.L.; Swine, C.; Hanlon, J.T. Appropriate prescribing in elderly people: How well can it be measured and optimised? Lancet 2007, 370, 173–184. [Google Scholar] [CrossRef]
- Patterson, S.M.; Hughes, C.; Kerse, N.; Cardwell, C.R.; Bradley, M.C. Interventions to improve the appropriate use of polypharmacy for older people. Cochrane Database Syst. Rev. 2012, 5, CD008165. [Google Scholar] [CrossRef] [Green Version]
- Rankin, A.; Cadogan, C.A.; Patterson, S.M.; Kerse, N.; Cardwell, C.R.; Bradley, M.C.; Ryan, C.; Hughes, C. Interventions to improve the appropriate use of polypharmacy for older people. Cochrane Database Syst. Rev. 2018, 106, CD008165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muth, C.; Uhlmann, L.; Haefeli, W.E.; Rochon, J.; Van Den Akker, M.; Perera, R.; Güthlin, C.; Beyer, M.; Oswald, F.; Valderas, J.M.; et al. Effectiveness of a complex intervention on Prioritising Multimedication in Multimorbidity (PRIMUM) in primary care: Results of a pragmatic cluster randomised controlled trial. BMJ Open 2018, 8, e017740. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M.; Wallace, E.; O’Dowd, T.; Fortin, M. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database Syst. Rev. 2016, 3, CD006560. [Google Scholar] [CrossRef] [PubMed]
- Salisbury, C.; Man, M.S.; Bower, P.; Guthrie, B.; Chaplin, K.; Gaunt, D.M.; Brookes, S.; Fitzpatrick, B.; Gardner, C.; Hollinghurst, S.; et al. Management of multimorbidity using a patient-centred care model: A pragmatic cluster-randomised trial of the 3D approach. Lancet 2018, 392, 41–50. [Google Scholar] [CrossRef]
- Muth, C.; van den Akker, M.; Blom, J.W.; Mallen, C.D.; Rochon, J.; Schellevis, F.G.; Becker, A.; Beyer, M.; Gensichen, J.; Kirchner, H.; et al. The Ariadne principles: How to handle multimorbidity in primary care consultations. BMC Med. 2014, 12, 223. [Google Scholar] [CrossRef]
- Muth, C.; Blom, J.W.; Smith, S.M.; Johnell, K.; Gonzalez-Gonzalez, A.I.; Nguyen, T.S.; Brueckle, M.-S.; Cesari, M.; Tinetti, M.E.; Valderas, J.M. Evidence supporting the best clinical management of patients with multimorbidity and polypharmacy: A systematic guideline review and expert consensus. J. Intern. Med. 2018, 285, 272–288. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence. Multimorbidity: Clinical Assessment and Management, 1st ed.; National Institute for Health and Care Excellence: London, UK, 2016; p. 63. ISBN 978-1-4731-2065-5. [Google Scholar]
- Bower, P. Better management of multimorbidity: A critical look at the “Ariadne principles”. BMC Med. 2014, 12, 222. [Google Scholar] [CrossRef] [Green Version]
- Prados-Torres, A.; del Cura-González, I.; Prados-Torres, J.D.; Leiva-Fernández, F.; López-Rodríguez, J.A.; Calderón-Larrañaga, A.; Muth, C. Multimorbilidad en medicina de familia y los principios Ariadne. Un enfoque centrado en la persona. Atención Primaria 2017, 49, 300–307. [Google Scholar] [CrossRef]
- O’Halloran, J.; Miller, G.C.; Britt, H. Defining chronic conditions for primary care with ICPC-2. Fam. Pract. 2004, 21, 381–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prados-Torres, A.; del Cura-González, I.; Prados-Torres, D.; López-Rodríguez, J.A.; Leiva-Fernández, F.; Calderón-Larrañaga, A.; López-Verde, F.; Gimeno-Feliu, L.A.L.A.; Escortell-Mayor, E.; Pico-Soler, V.; et al. Effectiveness of an intervention for improving drug prescription in primary care patients with multimorbidity and polypharmacy: Study protocol of a cluster randomized clinical trial (Multi-PAP project). Implement. Sci. 2017, 12, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perera, R.; Heneghan, C.; Yudkin, P. Graphical method for depicting randomised trials of complex interventions. BMJ 2007, 334, 127–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, C.; Wallace, E.; Kyle, L.; Cullen, W.; Smith, S.M.; Kyne, L.; Cullen, W.; Smith, S.M. Training doctors to manage patients with multimorbidity: A systematic review. J. Comorbidity 2016, 2016, 85–94. [Google Scholar] [CrossRef]
- Leiva-Fernández, F.; Prados-Torres, J.D.; Prados-Torres, A.; Del-Cura-González, I.; Castillo-Jimena, M.; López-Rodríguez, J.A.; Rogero-Blanco, M.E.; López-Verde, F.; Bujalance-Zafra, M.J.; Pico-Soler, M.V.; et al. Training primary care professionals in multimorbidity management: Educational assessment of the eMULTIPAP course. Mech. Ageing Dev. 2020, 192, 111354. [Google Scholar] [CrossRef]
- Mills, T.; Lawton, R.; Sheard, L. Advancing complexity science in healthcare research: The logic of logic models. BMC Med. Res. Methodol. 2019, 19, 55. [Google Scholar] [CrossRef] [Green Version]
- Hanlon, J.T.; Weinberger, M.; Samsa, G.P.; Schmader, K.E.; Uttech, K.M.; Lewis, I.K.; Cowper, P.A.; Landsman, P.B.; Cohen, H.J.; Feussner, J.R. A randomized, controlled trial of a clinical pharmacist intervention to improve inappropriate prescribing in elderly outpatients with polypharmacy. Am. J. Med. 1996, 100, 428–437. [Google Scholar] [CrossRef]
- Pednekar, P.P.; Ágh, T.; Malmenäs, M.; Raval, A.D.; Bennett, B.M.; Borah, B.J.; Hutchins, D.S.; Manias, E.; Williams, A.F.; Hiligsmann, M.; et al. Methods for Measuring Multiple Medication Adherence: A Systematic Review–Report of the ISPOR Medication Adherence and Persistence Special Interest Group. Value Health 2019, 22, 139–156. [Google Scholar] [CrossRef] [Green Version]
- Samsa, G.P.; Hanlon, J.T.; Schmader, K.E.; Weinberger, M.; Clipp, E.C.; Uttech, K.M.; Lewis, I.K.; Landsman, P.B.; Cohen, H.J. A summated score for the medication appropriateness index: Development and assessment of clinimetric properties including content validity. J. Clin. Epidemiol. 1994, 47, 891–896. [Google Scholar] [CrossRef]
- van der Cammen, T.J.M.; Rajkumar, C.; Onder, G.; Sterke, C.S.; Petrovic, M. Drug cessation in complex older adults: Time for action. Age Ageing 2014, 43, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Herdman, M.; Badia, X.; Berra, S. EuroQol-5D: A simple alternative for measuring health-related quality of life in primary care. Aten. Primaria 2001, 28, 425–430. [Google Scholar] [CrossRef] [Green Version]
- NHS England Statistical Bulletin. Overall Patient Experience Scores 2014: Adult Inpatient Survey Update. 2015. Available online: https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2015/05/Bulletin_2014IP_Final.pdf (accessed on 19 April 2022).
- Otero López, M.J.; Codina Jané, C.; Tamés Alonso, M.J.; Pérez Encinas, M. Medication errors: Standarizing the terminology and taxomany. Ruiz Jarabo 2000 grand results. Farm. Hosp. Organo Of. Expr. Cient. Soc. Esp. Farm. Hosp. 2003, 27, 137–149. [Google Scholar]
- Morisky, D.E.; Green, L.W.; Levine, D.M. Concurrent and predictive validity of a self-reported measure of medication adherence. Med. Care 1986, 24, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Krisch, L.; Mahlknecht, A.; Bauer, U.; Nestler, N.; Hempel, G.; Osterbrink, J.; Flamm, M. The challenge to define a relevant change in medication appropriateness index score in older adults—An approach. Br. J. Clin. Pharmacol. 2020, 86, 398–399. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, J.T.; Schmader, K.E. The medication appropriateness index at 20: Where it started, where it has been, and where it may be going. Drugs Aging 2013, 30, 893–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, G.; Gulliford, M.C.; Ukoumunne, O.C.; Eldridge, S.; Chinn, S.; Campbell, M.J. Patterns of intra-cluster correlation from primary care research to inform study design and analysis. J. Clin. Epidemiol. 2004, 57, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Müller, B.S.; Uhlmann, L.; Ihle, P.; Stock, C.; Von Buedingen, F.; Beyer, M.; Gerlach, F.M.; Perera, R.; Valderas, J.M.; Glasziou, P.; et al. Development and internal validation of prognostic models to predict negative health outcomes in older patients with multimorbidity and polypharmacy in general practice. BMJ Open 2020, 10, e039747. [Google Scholar] [CrossRef]
- Schmader, K.E.; Hanlon, J.T.; Landsman, P.B.; Samsa, G.P.; Lewis, I.K.; Weinberger, M. Inappropriate prescribing and health outcomes in elderly veteran outpatients. Ann. Pharmacother. 1997, 31, 529–533. [Google Scholar] [CrossRef]
- Allison, P.D. Change Scores as Dependent Variables in Regression Analysis. Sociol. Methodol. 1990, 20, 93. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013; ISBN 9781134742707. [Google Scholar]
- Romskaug, R.; Skovlund, E.; Straand, J.; Molden, E.; Kersten, H.; Pitkala, K.H.; Lundqvist, C.; Wyller, T.B. Effect of Clinical Geriatric Assessments and Collaborative Medication Reviews by Geriatrician and Family Physician for Improving Health-Related Quality of Life in Home-Dwelling Older Patients Receiving Polypharmacy: A Cluster Randomized Clinical Trial. JAMA Intern. Med. 2020, 180, 181–189. [Google Scholar] [CrossRef]
- Lopez-Rodriguez, J.A.; Rogero-Blanco, E.; Aza-Pascual-Salcedo, M.; Lopez-Verde, F.; Pico-Soler, V.; Leiva-Fernandez, F.; Daniel Prados-Torres, J.; Prados-Torres, A.; Cura-Gonzalez, I. Potentially inappropriate prescriptions according to explicit and implicit criteria in patients with multimorbidity and polypharmacy. MULTIPAP: A cross-sectional study. PLoS ONE 2020, 15, e0237186. [Google Scholar] [CrossRef] [PubMed]
- Kouladjian O’Donnell, L.; Gnjidic, D.; Sawan, M.; Reeve, E.; Kelly, P.J.; Chen, T.F.; Bell, J.S.; Hilmer, S.N. Impact of the Goal-directed Medication Review Electronic Decision Support System on Drug Burden Index: A cluster-randomised clinical trial in primary care. Br. J. Clin. Pharmacol. 2021, 87, 1499–1511. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Naik, A.D.; Dindo, L.; Costello, D.M.; Esterson, J.; Geda, M.; Rosen, J.; Hernandez-Bigos, K.; Smith, C.D.; Ouellet, G.M.; et al. Association of Patient Priorities-Aligned Decision-Making with Patient Outcomes and Ambulatory Health Care Burden among Older Adults with Multiple Chronic Conditions: A Nonrandomized Clinical Trial. JAMA Intern. Med. 2019, 179, 1688–1697. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.; Smith, A.; Gibbons, C.; Alonso, J.; Valderas, J. The National Institutes of Health Patient-Reported Outcomes Measurement Information System (PROMIS): A view from the UK. Patient Relat. Outcome Meas. 2018, 9, 345–352. [Google Scholar] [CrossRef] [Green Version]
- Mavaddat, N.; Valderas, J.M.; van der Linde, R.; Khaw, K.T.; Kinmonth, A.L. Association of self-rated health with multimorbidity, chronic disease and psychosocial factors in a large middle-aged and older cohort from general practice: A cross-sectional study. BMC Fam. Pract. 2014, 15, 185. [Google Scholar] [CrossRef] [Green Version]
- Goodman, R.A.; Posner, S.F.; Huang, E.S.; Parekh, A.K.; Koh, H.K. Defining and measuring chronic conditions: Imperatives for research, policy, program, and practice. Prev. Chronic Dis. 2013, 10, 120239. [Google Scholar] [CrossRef] [Green Version]
- Foguet-Boreu, Q.; Violan, C.; Roso-Llorach, A.; Rodriguez-Blanco, T.; Pons-Vigués, M.; Muñoz-Pérez, M.A.; Pujol-Ribera, E.; Valderas, J.M. Impact of multimorbidity: Acute morbidity, area of residency and use of health services across the life span in a region of south Europe. BMC Fam. Pract. 2014, 15, 55. [Google Scholar] [CrossRef] [Green Version]
- Barrio Cortes, J.; Suárez Fernández, C.; Bandeira de Oliveira, M.; Beca Martínez, M.T.; Lozano Hernández, C.; Del Cura-González, I. Utilización de los servicios de salud de Atención Primaria en los pacientes crónicos según nivel de riesgo. Rev. Esp. Salud Publica 2019, 93, e201909082. [Google Scholar]
- Loudon, K.; Treweek, S.; Sullivan, F.; Donnan, P.; Thorpe, K.E.; Zwarenstein, M. The PRECIS-2 tool: Designing trials that are fit for purpose. BMJ 2015, 350, h2147. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Raina, P.; Beyene, J.; Thabane, L. Comparison of population-averaged and cluster-specific models for the analysis of cluster randomized trials with missing binary outcomes: A simulation study. BMC Med. Res. Methodol. 2013, 13, 9. [Google Scholar] [CrossRef] [Green Version]
- Speidel, M.; Drechsler, J.; Sakshaug, J.W. Biases in multilevel analyses caused by cluster-specific fixed-effects imputation. Behav. Res. Methods 2018, 50, 1824–1840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díaz-Ordaz, K.; Kenward, M.G.; Cohen, A.; Coleman, C.L.; Eldridge, S. Are missing data adequately handled in cluster randomised trials? A systematic review and guidelines. Clin. Trials 2014, 11, 590–600. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | Control | Intervention | |
|---|---|---|---|
| Physician characteristics | n = 117 | n = 58 | n = 59 |
| Sex (female) | 77 (65.8%) | 41 (70.7%) | 36 (61.0%) |
| Age of the professional, mean (SD) | 52.1 (6.8) | 52.4 (6.8) | 51.8 (6.8) |
| Years in the professional position, mean (SD) | 18.3 (3.4) | 18.2 (3.7) | 18.3 (3.0) |
| 1–14 years | 12 (10.3%) | 4 (6.9%) | 8 (13.6%) |
| 15–19 years | 27 (23.1%) | 17 (29.3%) | 10 (16.9%) |
| 20 or more years | 78 (66.7%) | 37 (63.8%) | 41 (69.5%) |
| Postgraduate tutor | 75 (64.1%) | 40 (69.0%) | 35 (59.3%) |
| Patient characteristics | n = 593 | n = 295 | n = 298 |
| Sex (Female) | 331 (55.8%) | 172 (58.3%) | 159 (53.4%) |
| Age, mean (SD) | 69.7 (2.7) | 69.9 (2.7) | 69.6 (2.7) |
| Spanish nationality | 583 (98.3%) | 290 (98.3%) | 293 (98.3%) |
| Marital status | |||
| Single | 23 (3.9%) | 12 (4.1%) | 11 (3.7%) |
| Married | 447 (75.4%) | 224 (75.9%) | 223 (74.8%) |
| Separated | 29 (4.9%) | 13 (4.4%) | 16 (5.4%) |
| Widower | 94 (15.9%) | 46 (15.6%) | 48 (16.1%) |
| Level of studies | |||
| Did not complete primary studies | 279 (47.0%) | 142 (48.1%) | 137 (46.0%) |
| Completed primary studies | 196 (33.1%) | 104 (35.3%) | 92 (30.9%) |
| Bachelor or higher | 118 (19.9%) | 49 (16.6%) | 69 (23.2%) |
| Social class * | |||
| Supervisor, middle-management and director | 234 (39.5%) | 113 (38.3%) | 121 (40.6%) |
| Skilled primary sector | 217 (36.6%) | 108 (36.6%) | 109 (36.6%) |
| Unskilled | 142 (23.9%) | 74 (25.1%) | 68 (22.8%) |
| Monthly income | |||
| ≤1050 euro | 170 (28.7%) | 88 (29.8%) | 82 (27.5%) |
| 1051–2250 euro | 342 (57.7%) | 163 (55.3%) | 179 (60.1%) |
| ≥2251 euro | 59 (9.9%) | 29 (9.8%) | 30 (10.1%) |
| Unknown | 22 (3.7%) | 15 (5.1%) | 7 (2.3%) |
| Home size (m2), mean (SD) | 93.5 (42.9) | 93.3 (48.6) | 93.8 (36.4) |
| Number of cohabitants, mean (SD) | 2.3 (0.7) | 2.3 (0.6) | 2.3 (0.7) |
| Functional Social support +, mean (SD) | 43.7(8.8) | 43.7 (8.14) | 43.6 (19.3) |
| Number of diseases, median (IQR) | 5.0 (4.0, 7.0) | 5.0 (4.0, 6.0) | 5.0 (4.0, 7.0) |
| Number of drugs, median (IQR) | 7.0 (6.0, 9.0) | 7.0 (5.0, 8.0) | 7.0 (6.0, 9.0) |
| Non-adherence (Medication Assessment Questionnaire) | 242 (40.8%) | 105 (35.6%) | 137 (46.0%) |
| EuroQoL 5D-5 L, mean utilities (SD) | 0.8 (0.2) | 0.8 (0.2) | 0.8 (0.2) |
| EuroQoL VAS, mean (SD) | 65.5 (20.5) | 65.2 (19.4) | 65.9 (21.6) |
| Patient summated MAI score, mean (SD) | 17.5 (16.8) | 16.4 (14.6) | 18.6 (18.6) |
| Primary Outcome (6 Months) | Control Group | Intervention Group | Adjusted Difference (95% CI) | p-Value |
|---|---|---|---|---|
| Difference in MAI (1) T1-T0 mean (SD) (n) | 1.08 (0.41) (295) | 3.43 (0.84) (298) | −2.42 * (from −4.27 to −0.59) | 0.009 |
| Secondary outcomes (12 months) (1) | ||||
| Difference in MAI T3-T0 mean (SD) (n) | 1.19 (8.4) (277) | 4.6 (11.1) (269) | −3.40 * (from −5.45 to −1.34) | 0.001 |
| Quality of life | ||||
| EQ-VAS (visual analogue scale) mean (SD) (n) | 64.97 (19.75) (280) | 68.18 (20.57) (272) | 2.94 * (from −1.39 to 7.28) | 0.18 |
| EQ-5D-5 L (index) mean (SD) (n) | 0.780 (0.182) (280) | 0.763 (0.213) (272) | −0.006 * (from −0.034 to 0.022) | 0.68 |
| Treatment adherence | ||||
| Medication Assessment Questionnaire | 71/280 (25.4%) | 73/272 (26.8%) | −0.048 ‡ (from −0.65 to 0.56) | 0.87 |
| Medication safety | ||||
| Absolute incidence of adverse drug reactions | 1 (1–1) (291) | 1 (1–2) (290) | 0.49 † (from −0.12 to 1.11) | 0.11 |
| Patient perception of shared decision making | ||||
| NHS questionnaire (3) | 259/275 (94.2%) | 250/264 (94.7%) | 0.09 ‡ (from −0.91 to 1.10) | 0.85 |
| CollaboRATE (5) | 218/275 (79.3%) | 211/264 (79.9%) | 0.03 ‡ (from −0.67 to 0.74) | 0.92 |
| Use of health services | ||||
| Hospital admissions (IQR) (n) | 1 (1–2) (280) | 1 (0–1) (272) | −0.14 † (from −0.57 to 0.30) | 0.52 |
| Visits to emergency services (IQR) (n) | 1 (1–2) (280) | 1 (1–3) (272) | 0.18 † (from −0.06 to 0.41) | 0.14 |
| Number of FP consultations (n) | 7 (4–10) (280) | 7 (4–11) (272) | 0.07 † (from −0.11 to 0.25) | 0.44 |
| Number of primary-care nurse consultations (n) | 4 (2–7) (280) | 4 (2–8) (272) | 0.10 † (from −0.15 to 0.35) | 0.43 |
| Coefficients | 95% CI | p Value | |
|---|---|---|---|
| Receiving intervention (yes) | 1.78 | 0.29 to 3.29 | <0.001 |
| Baseline summated MAI Score | 0.29 | 0.25 to 0.33 | 0.02 |
| Living alone (yes) | −1.59 | −3.08 to −0.11 | 0.03 |
| Functional social support * | 0.07 | 0.01 to 0.14 | 0.03 |
| Number of drugs 5–6 Drugs | ref | ||
| 7–9 Drugs | −1.44 | −2.76 to −0.12 | 0.03 |
| ≥10 Drugs | −0.94 | −2.76 to 0.86 | 0.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
del Cura-González, I.; López-Rodríguez, J.A.; Leiva-Fernández, F.; Gimeno-Miguel, A.; Poblador-Plou, B.; López-Verde, F.; Lozano-Hernández, C.; Pico-Soler, V.; Bujalance-Zafra, M.J.; Gimeno-Feliu, L.A.; et al. How to Improve Healthcare for Patients with Multimorbidity and Polypharmacy in Primary Care: A Pragmatic Cluster-Randomized Clinical Trial of the MULTIPAP Intervention. J. Pers. Med. 2022, 12, 752. https://doi.org/10.3390/jpm12050752
del Cura-González I, López-Rodríguez JA, Leiva-Fernández F, Gimeno-Miguel A, Poblador-Plou B, López-Verde F, Lozano-Hernández C, Pico-Soler V, Bujalance-Zafra MJ, Gimeno-Feliu LA, et al. How to Improve Healthcare for Patients with Multimorbidity and Polypharmacy in Primary Care: A Pragmatic Cluster-Randomized Clinical Trial of the MULTIPAP Intervention. Journal of Personalized Medicine. 2022; 12(5):752. https://doi.org/10.3390/jpm12050752
Chicago/Turabian Styledel Cura-González, Isabel, Juan A. López-Rodríguez, Francisca Leiva-Fernández, Antonio Gimeno-Miguel, Beatriz Poblador-Plou, Fernando López-Verde, Cristina Lozano-Hernández, Victoria Pico-Soler, Mª Josefa Bujalance-Zafra, Luis A. Gimeno-Feliu, and et al. 2022. "How to Improve Healthcare for Patients with Multimorbidity and Polypharmacy in Primary Care: A Pragmatic Cluster-Randomized Clinical Trial of the MULTIPAP Intervention" Journal of Personalized Medicine 12, no. 5: 752. https://doi.org/10.3390/jpm12050752