
Eight Weeks Unsupervised Pulmonary Rehabilitation in Previously Hospitalized of SARS-CoV-2 Infection

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
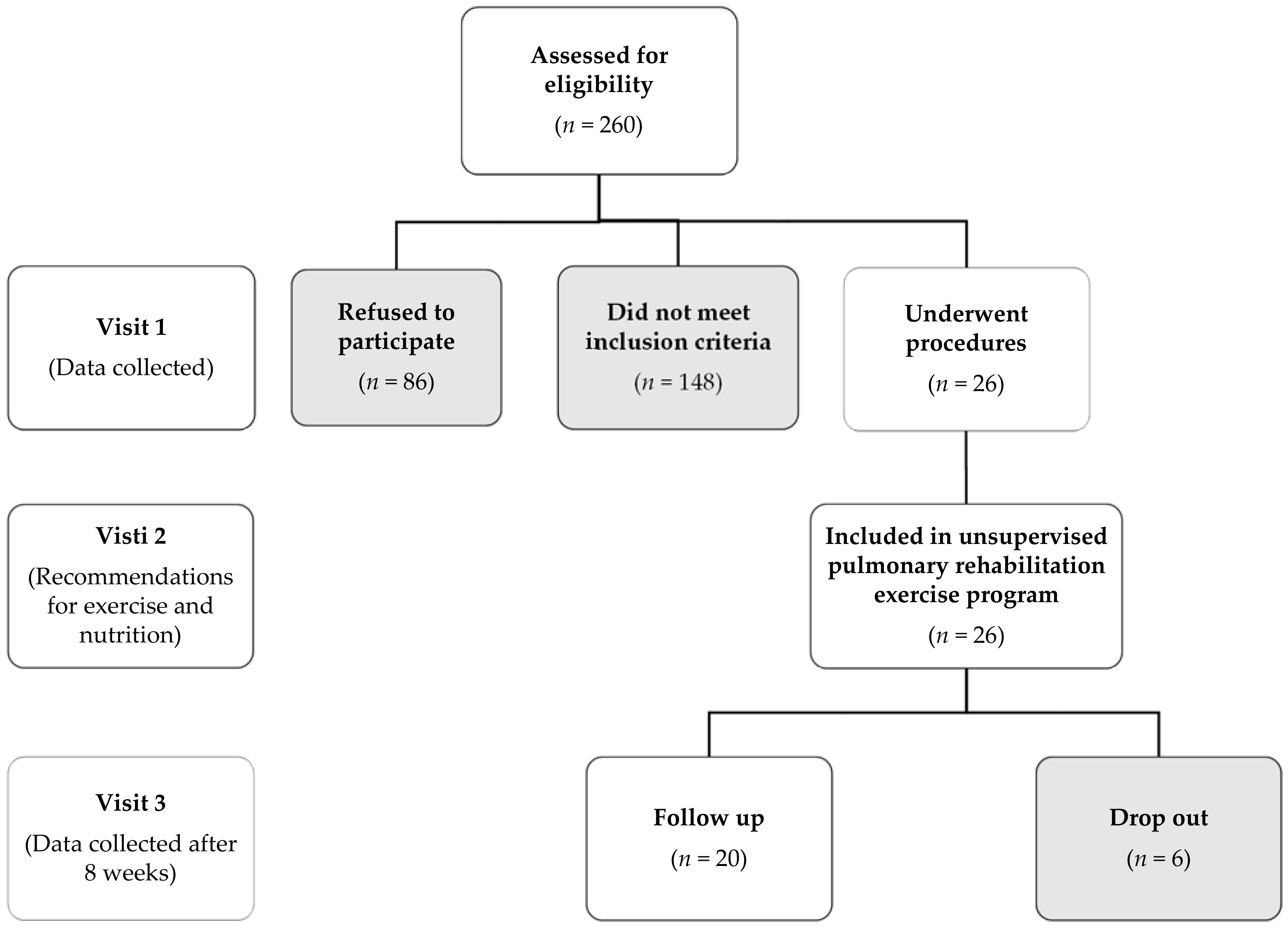
2.1. Study Population
- patients no longer require oxygen,
- their fever has resolved for a consecutive 48-h period without any medication to reduce their fever or
- stable patients even though they still require supplemental oxygen supposing oximetry self-monitoring due to limited hospital resources according to NIH discharge criteria for COVID-19 patients and Hellenic guidance for COVID-19 pneumonia diagnosis.
Study Ethics
2.2. Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Oronsky, B.; Larson, C.; Hammond, T.C.; Oronsky, A.; Kesari, S.; Lybeck, M.; Reid, T.R. A Review of Persistent Post-COVID Syndrome (PPCS). Clin. Rev. Allergy Immunol. 2021, 20, 1–9. [Google Scholar]
- Carf, A.; Bernabei, R.; Landi, F.; Gemelli against COVID-19 Post-Acute Care Study Group. Persistent symptoms in patients afer acute COVID-19. J. Am. Med. Assoc. 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Kim, S.S.; Lindsell, C.J.; Billig Rose, E.; Shapiro, N.I.; Files, D.C.; Gibbs, K.W.; Erickson, H.L.; Steingrub, J.S.; Smithline, H.A.; et al. Symptom Duration and Risk Factors for Delayed Return to Usual Health Among Outpatients with COVID-19 in a Multistate Health Care Systems Network—United States, March–June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2021, 370, m3026. [Google Scholar]
- Wade, D.T. Rehabilitation after COVID-19: An evidence-based approach. Clin. Med. 2020, 20, 359–365. [Google Scholar] [CrossRef]
- Hill, N.S. Pulmonary rehabilitation. Proc. Am. Thorac. Soc. 2006, 3, 66–74. [Google Scholar] [CrossRef]
- Dechman, G.; Hernandez, P.; Camp, P.G. Exercise prescription practices in pulmonary rehabilitation programs. Can. J. Respir. Crit. Care Sleep Med. 2017, 1, 77–83. [Google Scholar] [CrossRef]
- Wang, T.J.; Chau, B.; Lui, M.; Lam, G.T.; Lin, N.; Humbert, S. Physical Medicine and Rehabilitation and Pulmonary Rehabilitation for COVID-19. Am. J. Phys. Med. Rehabil. 2020, 99, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Desveaux, L.; Janaudis-Ferreira, T.; Goldstein, R.; Brooks, D. An international comparison of pulmonary rehabilitation: A systematic review. COPD 2015, 12, 144–153. [Google Scholar] [CrossRef]
- Stavrou, V.; Griziotis, M.; Raptis, D.; Bardaka, F.; Karetsi, E.; Kiritsis, A.; Daniil, Z.; Tsarouhas, K.; Triposkiadis, F.; Gourgoulianis, K.I.; et al. Eight Weeks of Pulmonary Rehabilitation in Patients with Pulmonary Embolism: A Preliminary Report. Proceedings 2019, 25, 37. [Google Scholar] [CrossRef] [Green Version]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Castillo-Rodríguez, A.; Onetti-Onetti, W.; Sousa Mendes, R.; Luis Chinchilla-Minguet, J. Relationship between Leg Strength and Balance and Lean Body Mass. Benefits for Active Aging. Sustainability 2020, 12, 2380. [Google Scholar] [CrossRef] [Green Version]
- Stavrou, V.T.; Astara, K.; Daniil, Z.; Gourgoulianis, K.I.; Kalabakas, K.; Karagiannis, D.; Basdekis, G. The reciprocal association between fitness indicators and sleep quality in the context of recent sport injury. Int. J. Environ. Res. Public Health 2020, 17, 4810. [Google Scholar] [CrossRef]
- Stavrou, V.T.; Astara, K.; Tourlakopoulos, K.N.; Daniil, Z.; Gourgoulianis, K.I.; Kalabakas, K.; Karagiannis, D.; Basdekis, G. Sleep Quality’s Effect on Vigilance and Perceptual Ability in Adolescent and Adult Athletes. J. Sports Med. 2021, 2021, 5585573. [Google Scholar] [CrossRef]
- Holt, G.R. Declaration of Helsinki—The World’s Document of Conscience and Responsibility. South Med. J. 2014, 107, 407. [Google Scholar] [CrossRef]
- European Union Law. Available online: https://eur-lex.europa.eu/eli/reg/2016/679/oj (accessed on 15 January 2021).
- Norton, K.; Whittingham, N.; Carter, L.; Kerr, D.; Gore, C.; Marfell-Jones, M. Measurement techniques in anthropometry. In Anthropometrica; Norton, K., Olds, T., Eds.; University of New South Wales Press: Sydney, Austria, 1996; pp. 25–50. [Google Scholar]
- World Health Organization. Waist Circumference and Waist-Hip Ratio. Report of a WHO Expert Consultation. 2008. Available online: http://apps.who.int/iris/bitstream/handle/10665/44583/9789241501491_eng.pdf;jsessionid=EFEE9ECDDE018A9A204DB6B342903860?sequence=1 (accessed on 12 March 2021).
- Mosteller, R.D. Simplified Calculation of Body Surface Area. N. Engl. J. Med. 1987, 317, 1098. [Google Scholar]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Stavrou, V.T.; Vavougios, G.D.; Astara, K.; Siachpazidou, D.I.; Papayianni, E.; Gourgoulianis, K.I. The 6-minute walk test and anthropometric characteristics as assessment tools in patients with Obstructive Sleep Apnea Syndrome. A preliminary report during the pandemic. J. Pers. Med. 2021, 11, 563. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Borg, E.; Borg, G.; Larsson, K.; Letzter, M.; Sundblad, B.M. An index for breathlessness and leg fatigue. Scand. J. Med. Sci. Sports 2010, 20, 644–650. [Google Scholar] [CrossRef]
- Ross, R.M.; Murthy, J.N.; Wollak, I.D.; Jackson, A.S. The six minute walk test accurately estimates mean peak oxygen uptake. BMC Pulm. Med. 2010, 10, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romagnolo, D.F.; Selmin, O.I. Mediterranean Diet and Prevention of Chronic Diseases. Nutr. Today 2017, 52, 208–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- De Lorenzo, R.; Conte, C.; Lanzani, C.; Benedetti, F.; Roveri, L.; Mazza, M.G.; Brioni, E.; Giacalone, G.; Canti, V.; Sofia, V.; et al. Residual clinical damage after COVID-19: A retrospective and prospective observational cohort study. PLoS ONE 2020, 15, e0239570. [Google Scholar] [CrossRef]
- Fagard, R.H.; Cornelissen, V.A. Effect of exercise on blood pressure control in hypertensive patients. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 12–17. [Google Scholar] [CrossRef]
- Claire, M.N.; Rochester, C.L. Exercise Training Modalities for People with Chronic Obstructive Pulmonary Disease. COPD 2019, 16, 378–389. [Google Scholar]
- Liu, X.C.; Pan, L.; Hu, Q.; Dong, W.P.; Yan, J.H.; Dong, L. Effects of yoga training in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis. J. Thorac. Dis. 2014, 6, 795–802. [Google Scholar]
- Lakka, T.A.; Bouchard, C. Physical activity, obesity and cardiovascular diseases. Handb. Exp. Pharmacol. 2005, 170, 137–163. [Google Scholar]
- Manna, P.; Jain, S.K. Obesity, Oxidative Stress, Adipose Tissue Dysfunction, and the Associated Health Risks: Causes and Therapeutic Strategies. Metab. Syndr. Relat. Disord. 2015, 13, 423–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenhalgh, T.; Knight, M.; Inda-Kim, M.; Fulop, N.J.; Leach, J.; Vindrola-Padros, C. Remote management of covid-19 using home pulse oximetry and virtual ward support. BMJ 2021, 372, n677. [Google Scholar] [CrossRef] [PubMed]
- Wagner, P.D. Ventilation-perfusion matching during exercise. Chest 1992, 101 (Suppl. 5), 192S–198S. [Google Scholar] [CrossRef] [Green Version]
- Casaburi, R.; ZuWallack, R. Pulmonary rehabilitation for management of chronic obstructive pulmonary disease. N. Engl. J. Med. 2009, 360, 1329–1335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Partinen, M. Sleep research in 2020: COVID-19-related sleep disorders. Lancet Neurol. 2021, 20, 15–17. [Google Scholar] [CrossRef]
- Voitsidis, P.; Gliatas, I.; Bairachtari, V.; Papadopoulou, K.; Papageorgiou, G.; Parlapani, E.; Syngelakis, M.; Holeva, V.; Diakogiannis, I. Insomnia during the COVID-19 pandemic in a Greek population. Psychiatry Res. 2020, 289, 113076. [Google Scholar] [CrossRef]
- Stavrou, V.; Karetsi, E.; Daniil, Z.; Gourgoulianis, K.I. 4 weeks exercise in obstructive sleep apnea syndrome patient with type 2 diabetes mellitus and without continuous positive airway pressure treatment: A case report. Sleep Med. Res. 2019, 10, 54–57. [Google Scholar] [CrossRef] [Green Version]
- Goërtz, Y.M.J.; Van Herck, M.; Delbressine, J.M.; Vaes, A.W.; Meys, R.; Machado, F.V.C.; Houben-Wilke, S.; Burtin, C.; Posthuma, R.; Franssen, F.M.E.; et al. Persistent symptoms 3 months after a SARS-CoV-2 infection: The post-COVID-19 syndrome? ERJ Open Res. 2020, 6, 00542–02020. [Google Scholar] [CrossRef]
- Maspero, C.; Abate, A.; Cavagnetto, D.; El Morsi, M.; Fama, A.; Farronato, M. Available Technologies, Applications and Benefits of Teleorthodontics. A Literature Review and Possible Applications during the COVID-19 Pandemic. J. Clin. Med. 2020, 9, 1891. [Google Scholar] [CrossRef]
- Althouse, A.D. Adjust for Multiple Comparisons? It’s Not That Simple. Ann. Thorac. Surg. 2016, 101, 1644–1645. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.; Genest, J.; Gotto, A.M.; Kastelein, J.J., Jr.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G.; et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N. Engl. J. Med. 2008, 20, 2195–2207. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | |
|---|---|
| Age, yrs | 64.1 ± 9.9 |
| Gender, (Male %) | 75 |
| Smokers, % | 10 |
| COPD, % | 10 |
| Hypertension, % | 65 |
| Diabetes mellitus, % | 20 |
| CVD, % | 10 |
| Length of hospitalization days | 15.1 ± 14.8 |
| Intensive care unit admission, % | 20 |
| Weeks | Warm-Up/Recovery | Walking | Yoga Breathing | Strength | |||||
|---|---|---|---|---|---|---|---|---|---|
| Exercise Type | Sets/ Repetitions (and/or s) | Intensity of HR peak (%) | Borg Scale CR10 (L/D) | Exercise Type | Sets/ Repetitions (and/or s) | Exercise Type | Sets/ Repetitions | Resistance | |
| 1st | a, b, c | a = 2/6 rep; b = 2/20 s; c = 2/15 s | 75 | 2/3 | a, b, c | 3/10 rep | a, b | 2/12 | a = 1.5 kg; b = body weight |
| 2nd | 80 | 3/3 | a, b, c | 4/12 rep | a, b, c | 2/12 | a = 1.5 kg; b, c = body weight | ||
| 3rd | 85 | 4/4 | a, b, c, d | 3/12 rep | a, b, c | 3/12 | a = 1.5 kg; b, c = body weight | ||
| 4th | 90 | 4/5 | a, b, c, h | 3/12 rep | a, b, c, d | 2/12 | a = 1.5 kg; b, c, d = body weight | ||
| 5th | 95 | 5/5 | e, f, g | 3/10 s | a, b, c, d | 3/12 | a = 1.5 kg; b, c, d = body weight | ||
| 6th | 100 | 5/6 | a, b, c, h | 4/12 | a, b, c, d, e | 2/12 | a = 1.5 kg; b, c, d = body weight; e = 2 kg | ||
| 7th | 105 | 6/6 | a, b, c, h–e, f, g | 3/12 rep–4/15 s | a, b, c, d, e | 3/12 | a = 1.5 kg; b, c, d = body weight; e = 2 kg | ||
| 8th | 110 | 6/6 | a, b, c, h–e, f, g | 3/12 rep–4/15 s | a, b, c, d, e | 3/16 | a = 1.5 kg; b, c, d = body weight; e = 2 kg | ||
| Baseline | Post Uns-PR | p Value | |
|---|---|---|---|
| Body Mass Index, kg/m2 | 30.3 ± 4.3 | 30.1 ± 4.4 | 0.030 |
| Body Surface Area, m2 | 2.1 ± 0.3 | 2.1 ± 0.3 | 0.110 |
| Body fat, % | 32.2 ± 9.4 | 29.5 ± 8.2 | 0.003 |
| Visceral fat, score | 14.0 ± 4.4 | 13.3 ± 4.2 | 0.021 |
| Muscle mass, kg | 30.1 ± 4.6 | 34.6 ± 7.4 | 0.030 |
| RMR, kcal/day | 1725.3 ± 174.7 | 1739.3 ± 202.9 | 0.490 |
| Neck circumference, cm | 39.9 ± 3.4 | 37.8 ± 4.2 | 0.006 |
| WHR | 102.6 ± 10.6 | 101.9 ± 9.4 | 0.917 |
| Δchest, % | 4.2 ± 2.3 | 6.0 ± 1.9 | 0.002 |
| Δarm, % | 3.7 ± 2.9 | 3.1 ± 2.2 | 0.398 |
| Δthigh, % | 5.0 ± 4.6 | 3.4 ± 2.5 | 0.270 |
| Δcalf, % | 3.2 ± 2.8 | 3.4 ± 3.3 | 0.809 |
| Handgrip, kg | 31.9 ± 10.2 | 33.2 ± 9.8 | 0.117 |
| 30 s Sit to Stand | |||
| Repetitions/30 s | 11.4 ± 3.2 | 14.1 ± 2.7 | <0.001 |
| ΔHR, bpm | 23.9 ± 11.2 | 24.3 ± 15.0 | 0.903 |
| ΔSpO2, % | 1.7 ± 1.3 | 1.5 ± 2.3 | 0.025 |
| FEV1, % of predicted | 84.1 ± 18.0 | 88.2 ± 17.4 | 0.235 |
| FVC, % of predicted | 84.8 ± 15.7 | 88.6 ± 14.7 | 0.214 |
| DLCO, % of predicted | 73.6 ± 11.2 | 75.7 ± 11.5 | 0.437 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stavrou, V.T.; Tourlakopoulos, K.N.; Vavougios, G.D.; Papayianni, E.; Kiribesi, K.; Maggoutas, S.; Nikolaidis, K.; Fradelos, E.C.; Dimeas, I.; Daniil, Z.; et al. Eight Weeks Unsupervised Pulmonary Rehabilitation in Previously Hospitalized of SARS-CoV-2 Infection. J. Pers. Med. 2021, 11, 806. https://doi.org/10.3390/jpm11080806
Stavrou VT, Tourlakopoulos KN, Vavougios GD, Papayianni E, Kiribesi K, Maggoutas S, Nikolaidis K, Fradelos EC, Dimeas I, Daniil Z, et al. Eight Weeks Unsupervised Pulmonary Rehabilitation in Previously Hospitalized of SARS-CoV-2 Infection. Journal of Personalized Medicine. 2021; 11(8):806. https://doi.org/10.3390/jpm11080806
Chicago/Turabian StyleStavrou, Vasileios T., Konstantinos N. Tourlakopoulos, George D. Vavougios, Eirini Papayianni, Katerina Kiribesi, Stavros Maggoutas, Konstantinos Nikolaidis, Evangelos C. Fradelos, Ilias Dimeas, Zoe Daniil, and et al. 2021. "Eight Weeks Unsupervised Pulmonary Rehabilitation in Previously Hospitalized of SARS-CoV-2 Infection" Journal of Personalized Medicine 11, no. 8: 806. https://doi.org/10.3390/jpm11080806