
Progression-Free Survival Prediction in Patients with Nasopharyngeal Carcinoma after Intensity-Modulated Radiotherapy: Machine Learning vs. Traditional Statistics


Abstract
:
1. Background
2. Results
2.1. Patient Characteristics
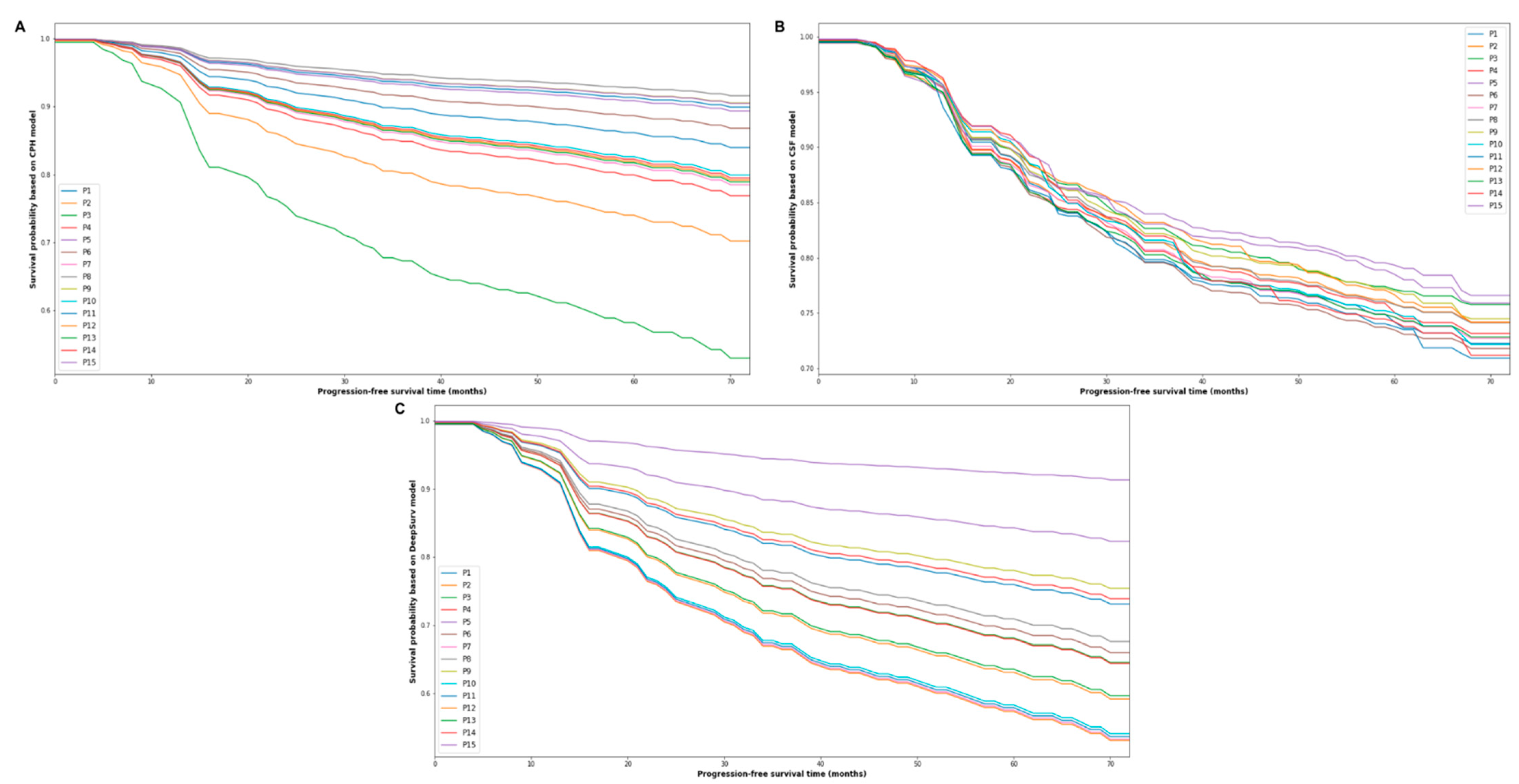
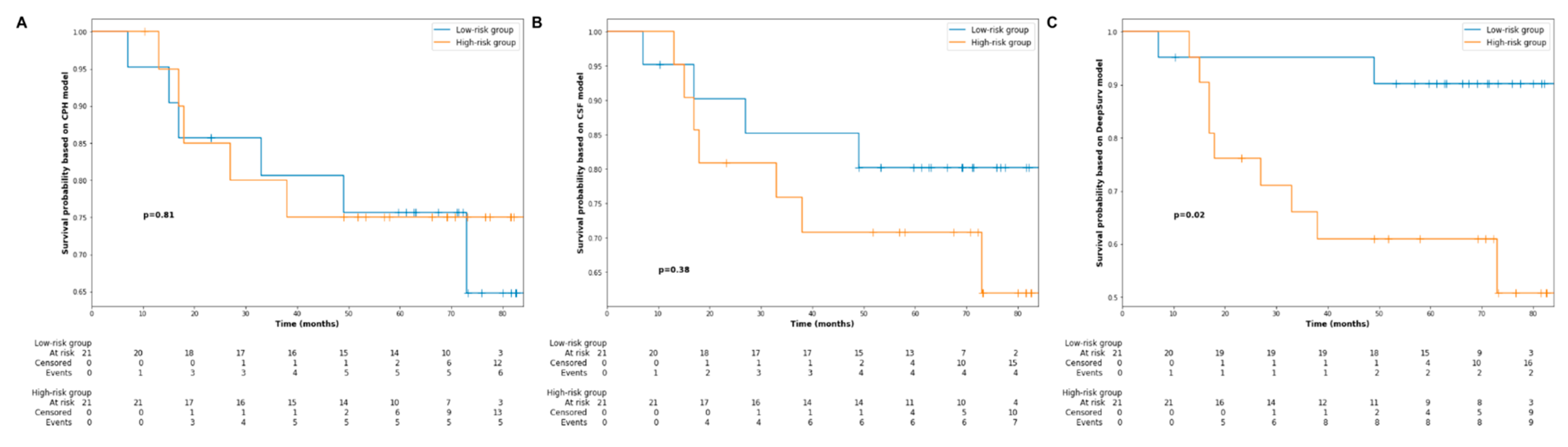
2.2. Survival Analysis
2.3. Univariate and Multivariate Analyses Based on CPH Model
2.4. Performance Comparison
3. Discussion
4. Materials and Methods
4.1. Study Cohort and Data
4.2. Treatment Protocol
4.3. Follow-Up and Statistical Analysis
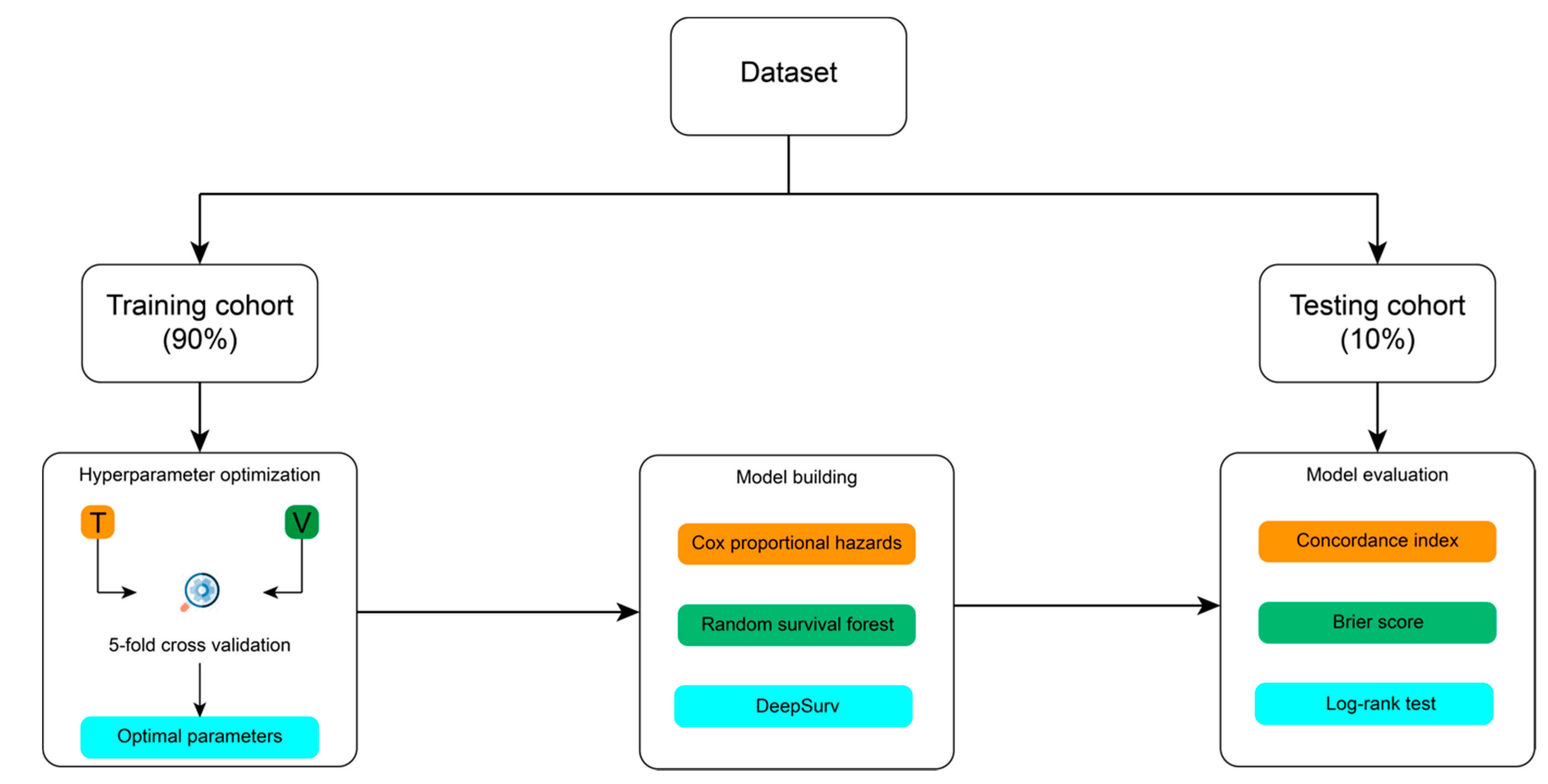
4.4. Modelling Process
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, Y.-P.; Chan, A.T.; Le, Q.-T.; Blanchard, P.; Sun, Y.; Ma, J. Nasopharyngeal carcinoma. Lancet 2019, 394, 64–80. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Co, J.; Mejia, M.B.; Dizon, J.M. Evidence on effectiveness of intensity-modulated radiotherapy versus 2-dimensional radiotherapy in the treatment of nasopharyngeal carcinoma: Meta-analysis and a systematic review of the literature. Head Neck 2016, 38, E2130–E2142. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Mo, Z.; Du, W.; Wang, Y.; Liu, L.; Wei, Y. Intensity-modulated radiation therapy versus 2D-RT or 3D-CRT for the treatment of nasopharyngeal carcinoma: A systematic review and meta-analysis. Oral Oncol. 2015, 51, 1041–1046. [Google Scholar] [CrossRef] [PubMed]
- Peng, G.; Wang, T.; Yang, K.Y.; Zhang, S.; Zhang, T.; Li, Q.; Han, J.; Wu, G. A prospective, randomized study comparing outcomes and toxicities of intensity-modulated radiotherapy vs. conventional two-dimensional radiotherapy for the treatment of nasopharyngeal carcinoma. Radiother. Oncol. 2012, 104, 286–293. [Google Scholar] [CrossRef]
- Yang, J.; Han, J.; He, J.; Duan, B.; Gou, Q.; Ai, P.; Liu, L.; Li, Y.; Ren, K.; Wang, F.; et al. Real-World Cost-Effectiveness Analysis of Gemcitabine and Cisplatin Compared to Docetaxel and Cisplatin Plus Fluorouracil Induction Chemotherapy in Locoregionally Advanced Nasopharyngeal Carcinoma. Front. Oncol. 2020, 10, 2923. [Google Scholar] [CrossRef]
- Lee, A.W.; Ng, W.T.; Chan, L.L.; Hung, W.M.; Chan, C.C.; Sze, H.C.; Chan, O.S.; Chang, A.T.; Yeung, R.M. Evolution of treatment for nasopharyngeal cancer–success and setback in the intensity-modulated radiotherapy era. Radiother. Oncol. 2014, 110, 377–384. [Google Scholar] [CrossRef]
- Linardatos, P.; Papastefanopoulos, V.; Kotsiantis, S. Explainable ai: A review of machine learning interpretability methods. Entropy 2021, 23, 18. [Google Scholar] [CrossRef] [PubMed]
- Iwatate, Y.; Hoshino, I.; Yokota, H.; Ishige, F.; Itami, M.; Mori, Y.; Chiba, S.; Arimitsu, H.; Yanagibashi, H.; Nagase, H.; et al. Radiogenomics for predicting p53 status, PD-L1 expression, and prognosis with machine learning in pancreatic cancer. Br. J. Cancer 2020, 123, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Boeri, C.; Chiappa, C.; Galli, F.; De Berardinis, V.; Bardelli, L.; Carcano, G.; Rovera, F. Machine Learning techniques in breast cancer prognosis prediction: A primary evaluation. Cancer Med. 2020, 9, 3234–3243. [Google Scholar] [CrossRef]
- Alabi, R.O.; Elmusrati, M.; Sawazaki-Calone, I.; Kowalski, L.P.; Haglund, C.; Coletta, R.D.; Mäkitie, A.A.; Salo, T.; Almangush, A.; Leivo, I. Comparison of supervised machine learning classification techniques in prediction of locoregional recurrences in early oral tongue cancer. Int. J. Med. Inform. 2020, 136, 104068. [Google Scholar] [CrossRef] [PubMed]
- Mourad, M.; Moubayed, S.; Dezube, A.; Mourad, Y.; Park, K.; Torreblanca-Zanca, A.; Torrecilla, J.S.; Cancilla, J.C.; Wang, J. Machine Learning and feature Selection Applied to SeeR Data to Reliably Assess thyroid cancer prognosis. Sci. Rep. 2020, 10, 5176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimitriou, N.; Arandjelović, O.; Harrison, D.J.; Caie, P.D. A principled machine learning framework improves accuracy of stage II colorectal cancer prognosis. NPJ Digit. Med. 2018, 1, 52. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; Zhan, X.; Xiang, S.; Johnson, T.S.; Helm, B.; Yu, C.Y.; Zhang, J.; Salama, P.; Rizkalla, M.; Han, Z.; et al. SALMON: Survival analysis learning with multi-omics neural networks on breast cancer. Front. Genet. 2019, 10, 166. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; Johnson, T.S.; Han, Z.; Helm, B.; Cao, S.; Zhang, C.; Salama, P.; Rizkalla, M.; Yu, C.Y.; Cheng, J.; et al. Deep learning-based cancer survival prognosis from RNA-seq data: Approaches and evaluations. BMC Med. Genom. 2020, 13, 41. [Google Scholar] [CrossRef] [Green Version]
- Akcay, M.; Etiz, D.; Celik, O.; Ozen, A. Evaluation of Prognosis in Nasopharyngeal Cancer Using Machine Learning. Technol. Cancer Res. Treat. 2020, 19, 1533033820909829. [Google Scholar] [CrossRef]
- Zhang, L.; Wu, X.; Liu, J.; Zhang, B.; Mo, X.; Chen, Q.; Fang, J.; Wang, F.; Li, M.; Chen, Z.; et al. MRI-based deep-learning model for distant metastasis-free survival in locoregionally advanced nasopharyngeal carcinoma. J. Magn. Reson. Imaging 2021, 53, 167–178. [Google Scholar] [CrossRef]
- Du, R.; Lee, V.H.; Yuan, H.; Lam, K.-O.; Pang, H.H.; Chen, Y.; Lam, E.Y.; Khong, P.-L.; Lee, A.W.; Kwong, D.L.; et al. Radiomics model to predict early progression of nonmetastatic nasopharyngeal carcinoma after intensity modulation radiation therapy: A multicenter study. Radiol. Artif. Intell. 2019, 1, e180075. [Google Scholar] [CrossRef]
- Li, S.; Wang, K.; Hou, Z.; Yang, j.; Ren, w.; Gao, S.; Meng, F.; Wu, P.; Liu, B.; Liu, J.; et al. Use of radiomics combined with machine learning method in the recurrence patterns after intensity-modulated radiotherapy for nasopharyngeal carcinoma: A preliminary study. Front. Oncol. 2018, 8, 648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.; He, X.; Ouyang, F.; Gu, D.; Dong, Y.; Zhang, L.; Mo, X.; Huang, W.; Tian, J.; Zhang, S.; et al. Radiomic machine-learning classifiers for prognostic biomarkers of advanced nasopharyngeal carcinoma. Cancer Lett. 2017, 403, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for some traditional and novel measures. Epidemiol. (Camb. Mass) 2010, 21, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Li, Y.; Li, X.; Cao, X.; Xiang, Y.; Xia, W.; Li, J.; Gao, M.; Sun, Y.; Liu, K.; et al. An interpretable machine learning prognostic system for locoregionally advanced nasopharyngeal carcinoma based on tumor burden features. Oral Oncol. 2021, 118, 105335. [Google Scholar] [CrossRef]
- Richter, A.N.; Khoshgoftaar, T.M. A review of statistical and machine learning methods for modeling cancer risk using structured clinical data. Artif. Intell. Med. 2018, 90, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Rajula, H.S.R.; Verlato, G.; Manchia, M.; Antonucci, N.; Fanos, V. Comparison of Conventional Statistical Methods with Machine Learning in Medicine: Diagnosis, Drug Development, and Treatment. Medicina 2020, 56, 455. [Google Scholar] [CrossRef]
- Xue, X.; Xie, X.; Gunter, M.; Rohan, T.E.; Wassertheil-Smoller, S.; Ho, G.Y.F.; Cirillo, D.; Yu, H.; Strickler, H.D. Testing the proportional hazards assumption in case-cohort analysis. BMC Med Res. Methodol. 2013, 13, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nasejje, J.B.; Mwambi, H.; Dheda, K.; Lesosky, M. A comparison of the conditional inference survival forest model to random survival forests based on a simulation study as well as on two applications with time-to-event data. BMC Med Res. Methodol. 2017, 17, 115. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.N.; Dankowski, T.; Ziegler, A. Unbiased split variable selection for random survival forests using maximally selected rank statistics. Stat. Med. 2017, 36, 1272–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katzman, J.L.; Shaham, U.; Cloninger, A.; Bates, J.; Jiang, T.; Kluger, Y. DeepSurv: Personalized treatment recommender system using a Cox proportional hazards deep neural network. BMC Med Res. Methodol. 2018, 18, 2. [Google Scholar] [CrossRef] [PubMed]
- Ching, T.; Zhu, X.; Garmire, L.X. Cox-nnet: An artificial neural network method for prognosis prediction of high-throughput omics data. PLoS Comput. Biol. 2018, 14, e1006076. [Google Scholar] [CrossRef]
- Giunchiglia, E.; Nemchenko, A.; van der Schaar, M. (Eds.) RNN-SURV: A Deep Recurrent Model for Survival Analysis. In International Conference on Artificial Neural Networks; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Fabris, A.; Bruschi, M.; Santucci, L.; Candiano, G.; Granata, S.; Gassa, A.D.; Antonucci, N.; Petretto, A.; Ghiggeri, G.M.; Gambaro, G.; et al. Proteomic-based research strategy identified laminin subunit alpha 2 as a potential urinary-specific biomarker for the medullary sponge kidney disease. Kidney Int. 2017, 91, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Ngiam, K.Y.; Khor, W. Big data and machine learning algorithms for health-care delivery. Lancet Oncol. 2019, 20, e262–e273. [Google Scholar] [CrossRef]
- Vock, D.M.; Wolfson, J.; Bandyopadhyay, S.; Adomavicius, G.; Johnson, P.E.; Vazquez-Benitez, G.; O’Connor, P.J. Adapting machine learning techniques to censored time-to-event health record data: A general-purpose approach using inverse probability of censoring weighting. J. Biomed. Inform. 2016, 61, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Stephane Fotso and Others. PySurvival: Open Source Package for Survival Analysis Modeling. 2019. Available online: https://www.pysurvival.io/ (accessed on 11 August 2021).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n | % |
|---|---|---|
| Age (years) | ||
| Median | 48 | |
| Range | 17–82 | |
| Sex | ||
| Male | 293 | 71.1 |
| Female | 119 | 28.9 |
| WHO histological subtypes | ||
| Type 2 (non-keratinizing squamous cell carcinoma) | 36 | 8.7 |
| Type 3 (undifferentiated or poorly differentiated carcinoma) | 376 | 91.3 |
| Tumor classification a | ||
| T1 | 76 | 18.4 |
| T2 | 135 | 32.8 |
| T3 | 125 | 30.4 |
| T4 | 76 | 18.4 |
| Nodal classification a | ||
| N0 | 43 | 10.4 |
| N1 | 147 | 35.7 |
| N2 | 163 | 39.6 |
| N3 | 59 | 14.3 |
| TNM stage a | ||
| I | 8 | 1.9 |
| II | 80 | 19.4 |
| III | 125 | 30.4 |
| IV | 199 | 48.3 |
| Radiation dose | ||
| ≤66 gray | 163 | 39.6 |
| >66 gray | 249 | 60.4 |
| Radiotherapy duration (days) | ||
| Median | 44 | |
| Range | 33–61 | |
| Neoadjuvant chemotherapy | ||
| Yes | 120 | 29.1 |
| No | 292 | 70.9 |
| Concurrent chemoradiotherapy | ||
| Yes | 296 | 71.9 |
| No | 116 | 28.1 |
| Adjuvant chemotherapy | ||
| Yes | 25 | 6.1 |
| No | 387 | 93.9 |
| Variable | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age | 1.00 (0.99–1.02) | 0.76 | 1.01 (1.00–1.03) | 0.16 |
| Sex | 0.79 (0.49–1.27) | 0.33 | 0.93 (0.59–1.47) | 0.75 |
| WHO histological subtypes | 0.69 (0.37–1.30) | 0.25 | 0.83 (0.45–1.54) | 0.56 |
| Tumor classification | 1.37 (1.11–1.68) | <0.005 | 1.59 (1.19–2.14) | <0.005 |
| Nodal classification | 1.53 (1.19–1.96) | <0.005 | 1.74 (1.34–2.26) | <0.005 |
| Radiation dose | 1.00 (1.00–1.00) | 0.06 | 1.00 (1.00–1.00) | 0.81 |
| Radiotherapy duration | 1.00 (0.95–1.06) | 0.92 | 0.96 (0.90–1.02) | 0.16 |
| Neoadjuvant chemotherapy | 1.69 (1.01–2.83) | 0.05 | 1.04 (0.60–1.79) | 0.89 |
| Concurrent chemoradiotherapy | 1.48 (0.90–2.43) | 0.12 | 1.00 (0.60–1.69) | 0.99 |
| Adjuvant chemotherapy | 0.52 (0.16–1.65) | 0.27 | 0.28 (0.08–0.94) | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oei, R.W.; Lyu, Y.; Ye, L.; Kong, F.; Du, C.; Zhai, R.; Xu, T.; Shen, C.; He, X.; Kong, L.; et al. Progression-Free Survival Prediction in Patients with Nasopharyngeal Carcinoma after Intensity-Modulated Radiotherapy: Machine Learning vs. Traditional Statistics. J. Pers. Med. 2021, 11, 787. https://doi.org/10.3390/jpm11080787
Oei RW, Lyu Y, Ye L, Kong F, Du C, Zhai R, Xu T, Shen C, He X, Kong L, et al. Progression-Free Survival Prediction in Patients with Nasopharyngeal Carcinoma after Intensity-Modulated Radiotherapy: Machine Learning vs. Traditional Statistics. Journal of Personalized Medicine. 2021; 11(8):787. https://doi.org/10.3390/jpm11080787
Chicago/Turabian StyleOei, Ronald Wihal, Yingchen Lyu, Lulu Ye, Fangfang Kong, Chengrun Du, Ruiping Zhai, Tingting Xu, Chunying Shen, Xiayun He, Lin Kong, and et al. 2021. "Progression-Free Survival Prediction in Patients with Nasopharyngeal Carcinoma after Intensity-Modulated Radiotherapy: Machine Learning vs. Traditional Statistics" Journal of Personalized Medicine 11, no. 8: 787. https://doi.org/10.3390/jpm11080787