
Precision Therapy for Invasive Fungal Diseases


1
Antimicrobial Pharmacodynamics and Therapeutics, University of Liverpool, Liverpool L7 8TX, UK
2
Westmead Hospital, Sydney, NSW 2145, Australia
3
Sydney Institute of Infectious Diseases, University of Sydney, Sydney, NSW 2145, Australia
4
Faculty of Medicine and Health, School of Pharmacy, University of Sydney, Sydney, NSW 2006, Australia
5
Department of Pharmacy and Radboud Institute for Health Sciences, Radboudumc and Radboudumc Center for Infectious Diseases, Radboud University Medical Center, 6525 GA Nijmegen, The Netherlands
*
Author to whom correspondence should be addressed.
J. Fungi 2022, 8(1), 18; https://doi.org/10.3390/jof8010018
Submission received: 29 November 2021
/
Revised: 22 December 2021
/
Accepted: 23 December 2021
/
Published: 27 December 2021
(This article belongs to the Special Issue Fungal Infections: From Diagnostics to Treatments)
Abstract
:Invasive fungal infections (IFI) are a common infection-related cause of death in immunocompromised patients. Approximately 10 million people are at risk of developing invasive aspergillosis annually. Detailed study of the pharmacokinetics (PK) and pharmacodynamics (PD) of antifungal drugs has resulted in a better understanding of optimal regimens for populations, drug exposure targets for therapeutic drug monitoring, and establishing in vitro susceptibility breakpoints. Importantly, however, each is an example of a “one size fits all strategy”, where complex systems are reduced to a singularity that ensures antifungal therapy is administered safely and effectively at the level of a population. Clearly, such a notion serves most patients adequately but is completely counter to the covenant at the centre of the clinician–patient relationship, where each patient should know whether they are well-positioned to maximally benefit from an antifungal drug. This review discusses the current therapy of fungal infections and areas of future research to maximise the effectiveness of antifungal therapy at an individual level.
1. Introduction
Invasive fungal infections (IFI) are a common infection-related cause of death in immunocompromised patients. Even with the application of state-of-the-art diagnostic testing and deployment of modern antifungal therapy, the mortality of IFIs remains high [1]. Mortality in real-world settings is generally 20–50% but may be higher in specific contexts [2]. There are continuous threats, such as triazole resistance in Aspergillus spp., multidrug resistant Candida auris, and the emergence of new pathogens (e.g., Emmonsia, Cryptococcus gattii, Exserohilum etc.). Furthermore, invasive fungal diseases are increasingly seen in non-classical settings, such as critically ill patients, and as a complication of influenza, SARS-CoV-1 and SARS-CoV-2 [3].
The clinical pharmacokinetics of antifungal agents are generally well-characterised (Table 1). The pharmacodynamics for most antifungal agents against medically important Candida spp. and Aspergillus spp. are also reasonably well-characterised. This knowledge has resulted in a better understanding of desired regimens for populations, drug exposure targets for therapeutic drug monitoring (TDM), and establishing in vitro susceptibility breakpoints. Importantly, however, each is an example of a “one size fits all strategy”, where complex systems are reduced to a singularity that ensures antifungal therapy is administered safely and effectively at the level of a population. Clearly, such a notion serves most patients adequately but is completely counter to notions of precision therapy at an individual patient level.
This viewpoint discusses the current therapy of fungal infections and areas of future research to maximise the effectiveness of antifungal therapy at an individual level. Reviews and guidelines of antifungal drug therapeutic drug monitoring are published elsewhere [11,15,21,22,23] and will not be considered in detail.
2. Factors Affecting Precision Therapy
Clinical studies used for licensure involve a relatively homogeneous population—a cohort of patients that fulfil typically restrictive inclusion criteria. Patients with suboptimal outcomes that may benefit from a precision approach may only be apparent from post hoc analyses (e.g., patients with central nervous system disease) or from subsequent case reports and/or cohort studies obtained post-licensure. While such evidence is often biased, it helps identify clinical scenarios where a fixed dosing strategy may be inadequate and tailored, or an individualised approach is more appropriate. The following summarises the microbiological, pharmacological and clinical features where precision approaches may be considered.
2.1. Invading Pathogen
The appropriate therapeutic choices and the probability of therapeutic success are dependent on the causative fungal pathogen. The overall therapeutic response to antifungal therapy is generally comparable for different species of Candida and most Aspergillus species, but there are important exceptions. For example, a group of Aspergillus spp.—A. lentulus, A. udagawae, A. viridinutans and A. fischeri—are less susceptible to first-line anti-Aspergillus agents (e.g., amphotericin B, triazoles, echinocandins), thus limiting standard therapeutic choices [24].
Some fungal species display intrinsically reduced susceptibility to licensed antifungal agents. These include species less susceptible to triazoles (e.g., fluconazole versus Candida parapsilosis; fluconazole versus Candida glabrata), echinocandins (e.g., C. parapsilosis, Trichosporon spp., Cryptococcus spp., Geotrichum spp.) and polyenes (e.g., amphotericin B versus A. terreus) [25]. In these cases, accurate speciation enables informed choices about appropriate first-line agent(s).
In vitro susceptibility testing enables further refinement of therapeutic choices and decisions as to whether regimen intensification is a viable strategy. This should be performed by specialised laboratories using standardised techniques with results interpreted according to breakpoints published by the European Committee on Antimicrobial Susceptibility Testing (EUCAST) [26] or the Clinical and Laboratory Standards Institute (CLSI) [27] and potentially considering results from fungal genetic testing. Common resistance mechanisms resulting in reduced susceptibility to antifungal agents are summarised in Table 2.
The effect of the relevant underlying resistance mechanisms (alone and in combination) is generally well-captured by the MIC. PK/PD targets for most of the triazoles against Candida, Aspergillus, and Cryptococcus are well-defined and can guide the likelihood of success with regimen intensification. A higher MIC requires a proportionally higher drug exposure to achieve a comparable therapeutic response. With regard to this, recently, EUCAST (European Committee of Antimicrobial Susceptibility Testing) has re-defined the intermittent susceptibility class to signal regimen intensification, which is required to secure a favourable clinical outcome [39]. The MIC and the associated PK/PD target provides an ability to objectively decide whether the patient is well-positioned to benefit from an antifungal agent.
2.2. Site of Infection
The success of therapy is dependent on the sites of infection. Examples of fungal diseases that are associated with poor clinical outcomes include infections within the central nervous system, endovascular infections, and disseminated disease [2]. Poor outcomes are a result of damage to vital structures and suboptimal partitioning of antifungal agents to the effect site. Bulky disease with significant tissue infarction and necrosis may further compromise drug penetration and make sterilisation with medical therapy alone impossible. Surgical resection may be required to debulk or completely remove acutely infected tissue and should be considered for large lesions that are contiguous and potentially compromise the heart, great vessels, and other mediastinal structures [40]. Suboptimal penetration of antifungal agents into fungal masses inside within pulmonary cavities pathognomonic of chronic pulmonary aspergillosis is associated with the emergence of antifungal resistance.
A high fungal burden may also be an important determinant of therapeutic response. Multifocal disease in a single organ is common (e.g., multiple Aspergillus nodules in the lung), and disseminated disease is probably significantly underdiagnosed. A high fungal burden may increase the probability of a resistant subpopulation being present at the time of treatment initiation and progressively expanding [41,42]. Unsurprisingly, a high fungal burden increases the time of sterilisation in the CSF and bloodstream in cryptococcal meningitis and taloromycosis, respectively [43,44].
2.3. Immunological Status of the Host
There are many factors that are predisposed to invasive fungal diseases. Significant systemic immunocompromise is generally a prerequisite for development of disease (e.g., severe prolonged neutropenia, solid organ transplantation, HIV/AIDS) [45,46]. Increasingly, new biologics, such as inhibitors of tumour necrosis alfa (TNF-α) and interleukin (IL), are recognised as predisposed to histoplasmosis, aspergillosis, and invasive candidiasis [47]. Recently, the introduction of tyrosine kinase inhibitors (TKIs, e.g., ibrutinib indicated for B-cell cancers) has caused a rise of invasive fungal infections [48,49]. During ibrutinib therapy, atypical fungal infections have been reported—disseminated cryptococcosis, extrapulmonary Pneumocystis jirovecii, etc [48]. With the continuous emergence of new biological therapies, disseminated infections with atypical fungi are becoming more frequent, and treatment options are limited. Genetic polymorphism of the immune system has an important role in the development of invasive fungal infections. Polymorphism, deficiency and downregulation of specific genes (e.g., PTX3, CX3CR1, STAT1, STAT3) can suggest risk for fungal infection and potentially help stratify patients into high- and low-risk groups [50].
The main implication of the immunological deficit for the delivery of precision therapy is an objective assessment of the degree of underlying immunosuppression. Regimen intensification (e.g., drug dosing, PK/PD target attainment, combination therapy) may be required to affect a therapeutic response in a profoundly immunosuppressed host.
2.4. PK Variability
The pharmacokinetics of antifungal drugs are typically highly variable because of absorption issues (e.g., food effects, differences between drug formulations), variation in protein binding (resulting in changes in free concentrations), drug–drug interactions and genetic polymorphisms in oxidative metabolism, errors in administration (e.g., crushing of posaconazole tablet [51]), and inflammatory status (in voriconazole therapy [52]). Importantly, however, a significant portion of observed variability remains unexplained [17,53,54,55,56,57,58]. The variability becomes clinically relevant for those agents with a narrow therapeutic index (voriconazole, itraconazole, posaconazole, amphotericin B and 5-flucytosine). In this context, the use of fixed regimens daily (including weight-based regimens) results in too many patients with concentration-dependent clinical failure and toxicity (e.g., voriconazole) [59]. This is the primary argument for routine therapeutic drug monitoring.
Finally, variability in drug exposure may result from poor compliance and a reduced amount of active substance within counterfeit drugs [60]. A thorough overview of the pharmacokinetics of antifungal drugs has been presented in multiple publications and is not discussed further here [17,58,61,62,63,64,65,66,67,68].
3. Delivering Precision Therapy
3.1. Scenario #1. No Cultures Available or Patient Is Culture Negative
This is perhaps the most common clinical scenario. Most patients in this group have significant underlying immunocompromise and possible invasive fungal infection (as defined by EORTC/MSG diagnostic criteria) [69]. Fungal cultures may have been obtained and be negative, or it may not have been possible to obtain deep cultures (e.g., because of thrombocytopenia). In this case, licensed antifungal therapy following international guidelines (e.g., ESCMID, IDSA, ECMM [14,16,70]) should be initially administered and regimens modified using therapeutic drug monitoring (TDM) as an adjunct where relevant. If appropriate, higher loading doses can be considered (e.g., CASPOLOAD study, micafungin in obesity) [71,72]. In addition, genotype-guided dosing has been shown beneficial in voriconazole therapy, where knowing the CYP genotype can help in deciding the initial dose [70,73].
In the absence of any microbiological data, there is no alternative but to use TDM drug exposure targets that have been defined for populations (Table 1). If there are specific clinical concerns (e.g., severe immunocompromised status) and regimen intensification is considered, it may be reasonable to use the top end of the range as the treatment target. In some cases, it may be reasonable to push beyond the upper bound of the target range if safety can be closely monitored and the anticipated toxicity is clinically acceptable. There is increased interest in using advanced computational methods to achieve desired therapeutic targets in a rapidly and optimally precise manner (e.g., model informed precision dosing) [74,75,76,77].
The assessment of the clinical response is notoriously difficult and requires experienced clinical judgement. Clinical signs and symptoms are generally nonspecific and affected (confounded) by multiple comorbidities. Nonspecific biomarkers (e.g., CRP, procalcitonin) may be useful as well as specific biomarkers, such as galactomannan [78]. Radiological resolution is typically slow and may paradoxically worsen, especially upon recovery from neutropenia [79]. Functional imaging with 2-fluorodeoxyglucose positron emission tomography integrated with computer tomography (FDG-PET/CT) may be helpful to define the optimum duration of therapy but it is not widely used due to costs and availability [80,81].
3.2. Scenario #2. Optimising the Antifungal Regimen Using the Organism and MIC
In this scenario, the invading pathogen has been cultured, and an MIC is available. This is commonly seen in candidemia, endemic fungal infections, and cryptococcal meningitis, but remains frustratingly low for mould infections, such as invasive aspergillosis, and infections caused by Mucorales [82,83]. For some fungal genera and species, the correlation between MIC and the clinical outcome is still poorly defined because of a significant impact of the underlying disease and immune status on the therapeutic response.
Standard TDM based on PK–PD targets can be used (Table 1) but are now be embellished by the MIC. However, the PK/PD targets for echinocandins and polyenes are not routinely used to guide dosage adjustment in clinical settings, because of an absence of evidence if this has a quantifiable impact on clinical response and/or safety. Knowledge of the MIC can be used to optimise the use of fluconazole for Candida albicans, where an AUC/MIC of 100 is a well-cited and commonly accepted drug exposure target [10]. The MIC can be used to refine the dosing of voriconazole to treat a range of fungal pathogens. A Cmin/MIC target of 2–5 has been estimated from a large number of fungal infections treated with voriconazole [84] and is useful in deciding treatment options for strains with MICs just beyond the breakpoint.
3.3. Scenario #3. Combining PK with Fungal-Specific Biomarkers
Medical mycology has multiple examples where the response to antifungal therapy can be quantified in real-time using a variety of fungal biomarkers. Galactomannan can be used to follow the course of invasive aspergillosis (especially in murine models). Beta-glucan has prognostic value for invasive aspergillosis and invasive candidiasis. Finally, quantitative fungal cultures of Cryptococcus and Taloromyces in CSF and blood can be used to follow the treatment response of cryptococcal meningitis and talaromycosis, respectively [44,85]. Clearly, such as strategy is limited to the subset of patients that are culture positive or have a positive biomarker.
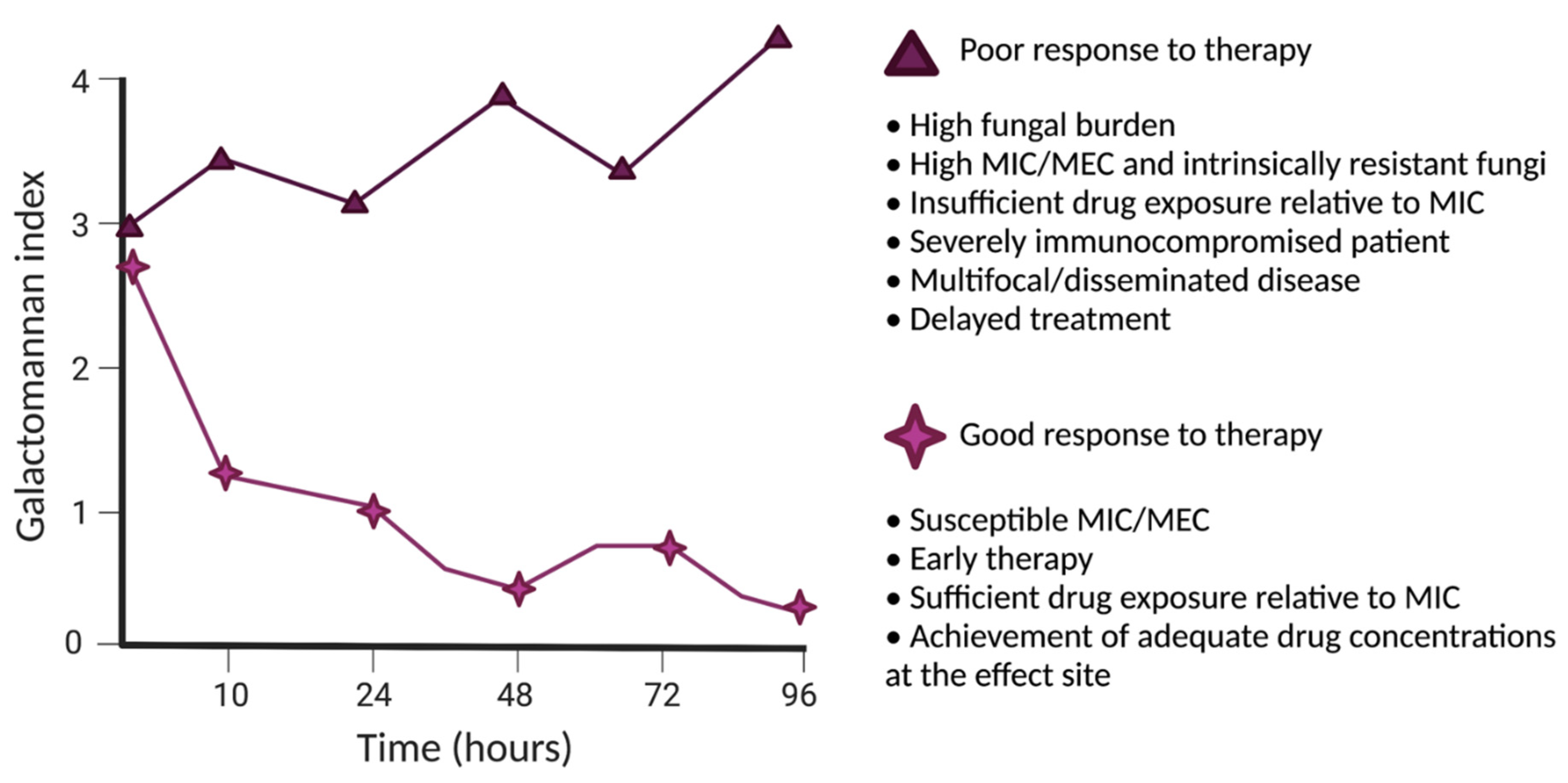
The trajectory of a fungal-specific biomarker may be affected by both the organism and/or host-specific factors (Figure 1, example of biomarker response). The relationship between drug concentrations, fungal growth, and drug-induced antifungal effects can be quantified using PK–PD mathematical models [86,87]. Fungal-specific factors that are relevant include the fungal genera and species, fungal burden, and in vitro susceptibility (as discussed above). Host-specific factors include the nature and specific type of host immunological deficit and determinants of PK variability and drug handling. A successful therapeutic response requires both aspects to be satisfactorily addressed. The use of a biomarker also enables the treating clinician to escape the use of drug exposure targets derived from a population of patients (i.e., the average drug exposure target). Each patient has a specific therapeutic requirement that is based on their own specific circumstances and the properties of the invading pathogen. The balance of that relationship is revealed by the trajectory of the biomarker. A patient who is receiving a seemingly adequate antifungal regimen but has a climbing biomarker clearly needs regimen intensification, a new drug, or a combination of agents. In contrast, a patient whose biomarker settles quickly with treatment might feel more sanguine even if drug exposures are lower than considered ideal from estimates derived from populations.
An integrated approach addresses “true individualised therapy” or truly “precise therapy”. Each patient has their own individual drug exposure target, which is formed from a combination of host- and pathogen-specific factors. The use of both pharmacokinetic and pharmacodynamic data enables patients to understand whether they are well-positioned to maximally benefit from an antifungal drug and guide treatment decisions tailored for that individual.
4. Conclusions
With the increasing number of immunocompromised patients in the world, treatment of fungal infections will become progressively important. Here, we have presented the current approach to the diagnostics and optimisation of therapy and potential future directions. Whole genome sequencing, biomarkers, disease progression modelling, and FDG-PET/CT may all have an important role in the precision dosing of antifungal agents.
Author Contributions
A.-G.M., J.-W.C.A., R.J.B., W.H. contributed equally to the writing and planning of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Schauwvlieghe, A.F.A.D.; Rijnders, B.J.A.; Philips, N.; Verwijs, R.; Vanderbeke, L.; Van Tienen, C.; Lagrou, K.; Verweij, P.E.; Van de Veerdonk, F.L.; Gommers, D.; et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: A retrospective cohort study. Lancet. Respir. Med. 2018, 6, 782–792. [Google Scholar] [CrossRef]
- Bongomin, F.; Gago, S.; Oladele, R.O.; Denning, D.W. Global and Multi-National Prevalence of Fungal Diseases-Estimate Precision. J. Fungi 2017, 3, 57. [Google Scholar] [CrossRef] [PubMed]
- Ghazanfari, M.; Arastehfar, A.; Davoodi, L.; Yazdani Charati, J.; Moazeni, M.; Abastabar, M.; Haghani, I.; Mirzakhani, R.; Mayahi, S.; Fang, W.; et al. Pervasive but Neglected: A Perspective on COVID-19-Associated Pulmonary Mold Infections Among Mechanically Ventilated COVID-19 Patients. Front. Med. 2021, 8, 754. [Google Scholar] [CrossRef]
- Andes, D.; Diekema, D.J.; Pfaller, M.A.; Bohrmuller, J.; Marchillo, K.; Lepak, A. In Vivo Comparison of the Pharmacodynamic Targets for Echinocandin Drugs against Candida Species. Antimicrob. Agents Chemother. 2010, 54, 2497–2506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gumbo, T.; Drusano, G.L.; Liu, W.; Kulawy, R.W.; Fregeau, C.; Hsu, V.; Louie, A. Once-weekly micafungin therapy is as effective as daily therapy for disseminated candidiasis in mice with persistent neutropenia. Antimicrob. Agents Chemother. 2007, 51, 968–974. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.R.; Diekema, D.J.; Pfaller, M.A.; Marchillo, K.; Bohrmueller, J. In vivo pharmacodynamic target investigation for micafungin against Candida albicans and C. glabrata in a neutropenic murine candidiasis model. Antimicrob. Agents Chemother. 2008, 52, 3497–3503. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.; Ambrose, P.G.; Hammel, J.P.; Van Wart, S.A.; Iyer, V.; Reynolds, D.K.; Buell, D.N.; Kovanda, L.L.; Bhavnani, S.M. Use of Pharmacokinetic-Pharmacodynamic Analyses To Optimize Therapy with the Systemic Antifungal Micafungin for Invasive Candidiasis or Candidemia. Antimicrob. Agents Chemother. 2011, 55, 2113–2121. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.; Diekema, D.J.; Pfaller, M.A.; Prince, R.A.; Marchillo, K.; Ashbeck, J.; Hou, J. In vivo pharmacodynamic characterization of anidulafungin in a neutropenic murine candidiasis model. Antimicrob. Agents Chemother. 2008, 52, 539–550. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, K.T.; Ta, P.; Hoang, B.T.; Cheng, S.; Hao, B.; Nguyen, M.H.; Clancy, C.J. Anidulafungin is fungicidal and exerts a variety of postantifungal effects against Candida albicans, C. glabrata, C. parapsilosis, and C. krusei isolates. Antimicrob. Agents Chemother. 2009, 53, 3347–3352. [Google Scholar] [CrossRef] [Green Version]
- Clancy, C.J.; Yu, V.L.; Morris, A.J.; Snydman, D.R.; Nguyen, M.H. Fluconazole MIC and the fluconazole dose/MIC ratio correlate with therapeutic response among patients with Candidemia. Antimicrob. Agents Chemother. 2005, 49, 3171–3177. [Google Scholar] [CrossRef] [Green Version]
- Ashbee, H.R.; Barnes, R.A.; Johnson, E.M.; Richardson, M.D.; Gorton, R.; Hope, W.W. Therapeutic drug monitoring (TDM) of antifungal agents: Guidelines from the British Society for Medical Mycology. J. Antimicrob. Chemother. 2014, 69, 1162–1176. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Tudela, J.L.; Almirante, B.; Rodríguez-Pardo, D.; Laguna, F.; Donnelly, J.P.; Mouton, J.W.; Pahissa, A.; Cuenca-Estrella, M. Correlation of the MIC and dose/MIC ratio of fluconazole to the therapeutic response of patients with mucosal candidiasis and candidemia. Antimicrob. Agents Chemother. 2007, 51, 3599–3604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pai Manjunath, P.; Turpin Robin, S.; Garey Kevin, W. Association of Fluconazole Area under the Concentration-Time Curve/MIC and Dose/MIC Ratios with Mortality in Nonneutropenic Patients with Candidemia. Antimicrob. Agents Chemother. 2007, 51, 35–39. [Google Scholar] [CrossRef] [Green Version]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef]
- Gómez-López, A. Antifungal therapeutic drug monitoring: Focus on drugs without a clear recommendation. Clin. Microbiol. Infect. 2020, 26, 1481–1487. [Google Scholar] [CrossRef]
- Patterson, T.F.; Thompson, G.R., III.; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- Dekkers, B.G.J.; Bakker, M.; van der Elst, K.C.M.; Sturkenboom, M.G.G.; Veringa, A.; Span, L.F.R.; Alffenaar, J.-W.C. Therapeutic Drug Monitoring of Posaconazole: An Update. Curr. Fungal Infect. Rep. 2016, 10, 51–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merck S & DL. Merck, Sharp & Dohme Ltd. Noxafil (Posaconazole)-Summary of Product Characteristics. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000610/WC500037784.pdf (accessed on 24 December 2021).
- Takemoto, K.; Yamamoto, Y.; Ueda, Y. Evaluation of antifungal pharmacodynamic characteristics of AmBisome against Candida albicans. Microbiol. Immunol. 2006, 50, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Perfect, J.R.; Dismukes, W.E.; Dromer, F.; Goldman, D.L.; Graybill, J.R.; Hamill, R.J.; Harrison, T.S.; Larsen, R.A.; Lortholary, O.; Nguyen, M.-H.; et al. Clinical Practice Guidelines for the Management of Cryptococcal Disease: 2010 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2010, 50, 291–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- David, A.; Andres, P.; Oscar, M. Antifungal Therapeutic Drug Monitoring: Established and Emerging Indications. Antimicrob. Agents Chemother. 2009, 53, 24–34. [Google Scholar] [CrossRef] [Green Version]
- John, J.; Loo, A.; Mazur, S.; Walsh, T.J. Therapeutic drug monitoring of systemic antifungal agents: A pragmatic approach for adult and pediatric patients. Expert Opin. Drug Metab. Toxicol. 2019, 15, 881–895. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Baldelli, S.; Märtson, A.-G.; Stocker, S.; Alffenaar, J.-W.; Cattaneo, D.; Marriott, D.J.E. Therapeutic Drug Monitoring of the Echinocandin Antifungal Agents: Is There a Role in Clinical Practice? A Position Statement of the Anti-Infective Drugs Committee of the International Association of Therapeutic Drug Monitoring and Clinical Toxicology. Ther. Drug Monit. 2021, Nov 22. [Google Scholar] [CrossRef]
- Lamoth, F. Aspergillus fumigatus-Related Species in Clinical Practice. Front. Microbiol. 2016, 7, 683. [Google Scholar] [CrossRef] [Green Version]
- Cowen, L.E.; Sanglard, D.; Howard, S.J.; Rogers, P.D.; Perlin, D.S. Mechanisms of Antifungal Drug Resistance. Cold Spring Harb. Perspect. Med. 2014, 5, a019752. [Google Scholar] [CrossRef] [PubMed]
- EUCAST Clinical Breakpoints. Available online: https://www.eucast.org/clinical_breakpoints/ (accessed on 24 November 2021).
- Clinical and Laboratory Standards Institute (CLSI). M100: Antimicrobial Susceptibility Testing Standards. Clin Lab Stand Inst. Available online: https://clsi.org/standards/products/microbiology/documents/m100/ (accessed on 24 December 2021).
- Orozco, A.S.; Higginbotham, L.M.; Hitchcock, C.A.; Parkinson, T.; Falconer, D.; Ibrahim, A.S.; Ghannoum, M.A.; Filler, S.G. Mechanism of fluconazole resistance in Candida krusei. Antimicrob. Agents Chemother. 1998, 42, 2645–2649. [Google Scholar] [CrossRef] [Green Version]
- Ghannoum, M.A.; Rice, L.B. Antifungal Agents: Mode of Action, Mechanisms of Resistance, and Correlation of These Mechanisms with Bacterial Resistance. Clin. Microbiol. Rev. 1999, 12, 501–517. [Google Scholar] [CrossRef] [Green Version]
- vanden Bossche, H.; Marichal, P.; Odds, F.C.; Le Jeune, L.; Coene, M.C. Characterization of an azole-resistant Candida glabrata isolate. Antimicrob. Agents Chemother. 1992, 36, 2602–2610. [Google Scholar] [CrossRef] [Green Version]
- Jenkinson, H.F. Ins and outs of antimicrobial resistance: Era of the drug pumps. J. Dent. Res. 1996, 75, 736–742. [Google Scholar] [CrossRef] [PubMed]
- Douglas, C.M.; D’Ippolito, J.A.; Shei, G.J.; Meinz, M.; Onishi, J.; Marrinan, J.A.; Li, W.; Abruzzo, G.K.; Flattery, A.; Bartizal, K.; et al. Identification of the FKS1 gene of Candida albicans as the essential target of 1,3-beta-D-glucan synthase inhibitors. Antimicrob. Agents Chemother. 1997, 41, 2471–2479. [Google Scholar] [CrossRef] [Green Version]
- Fraser, M.; Borman, A.M.; Thorn, R.; Lawrance, L.M. Resistance to echinocandin antifungal agents in the United Kingdom in clinical isolates of Candida glabrata: Fifteen years of interpretation and assessment. Med. Mycol. 2020, 58, 219–226. [Google Scholar] [CrossRef]
- Slater, J.L.; Howard, S.J.; Sharp, A.; Goodwin, J.; Gregson, L.M.; Alastruey-Izquierdo, A.; Arendrup, M.C.; Warn, P.A.; Perlin, D.S.; Hope, W.W. Disseminated candidiasis caused by Candida albicans with amino acid substitutions in Fks1 at position Ser645 cannot be successfully treated with micafungin. Antimicrob. Agents Chemother. 2011, 55, 3075–3083. [Google Scholar] [CrossRef] [Green Version]
- Carolus, H.; Pierson, S.; Lagrou, K.; Van Dijck, P. Amphotericin B and Other Polyenes-Discovery, Clinical Use, Mode of Action and Drug Resistance. J. Fungi 2020, 6, 321. [Google Scholar] [CrossRef]
- Billmyre, R.B.; Applen Clancey, S.; Li, L.X.; Doering, T.L.; Heitman, J. 5-fluorocytosine resistance is associated with hypermutation and alterations in capsule biosynthesis in Cryptococcus. Nat. Commun. 2020, 11, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florence, C.-L.; Julien, B.; Abdelhak, G.; Christiane, C.; Jean, V.; Thierry, N. Inactivation of the FCY2 Gene Encoding Purine-Cytosine Permease Promotes Cross-Resistance to Flucytosine and Fluconazole in Candida lusitaniae. Antimicrob. Agents Chemother. 2005, 49, 3101–3108. [Google Scholar] [CrossRef] [Green Version]
- Hope, W.; Tabernero, L.; Denning, D.W.; Anderson, M.J. Molecular Mechanisms of Primary Resistance to Flucytosine in Candida albicans. Antimicrob. Agents Chemother. 2004, 48, 4377–4386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EUCAST. ESCMID New definitions of S, I and R from 2019. Available online: https://www.eucast.org/newsiandr/ (accessed on 29 November 2021).
- Pidhorecky, I.; Urschel, J.; Anderson, T. Resection of invasive pulmonary aspergillosis in immunocompromised patients. Ann. Surg. Oncol. 2000, 7, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Stone, N.R.H.; Schwartz, I.S. Identifying the Patients Most Likely to Die from Cryptococcal Meningitis: Time to Move from Recognition to Intervention. Clin. Infect. Dis. 2021, 73, e3083–e3084. [Google Scholar] [CrossRef]
- Lestner, J.; McEntee, L.; Johnson, A.; Livermore, J.; Whalley, S.; Schwartz, J.; Perfect, J.R.; Harrison, T.; Hope, W. Experimental Models of Short Courses of Liposomal Amphotericin B for Induction Therapy for Cryptococcal Meningitis. Antimicrob. Agents Chemother. 2017, 61. [Google Scholar] [CrossRef] [Green Version]
- Stott, K.E.; Le, T.; Nguyen, T.; Whalley, S.; Unsworth, J.; Ly, V.T.; Kolamunnage-Dona, R.; Hope, W. Population Pharmacokinetics and Pharmacodynamics of Itraconazole for Disseminated Infection Caused by Talaromyces marneffei. Antimicrob. Agents Chemother. 2021, 65, e0063621. [Google Scholar] [CrossRef]
- Le, T.; Van Kinh, N.; Cuc, N.T.K.; Tung, N.L.N.; Lam, N.T.; Thuy, P.T.T.; Cuong, D.D.; Phuc, P.T.H.; Vinh, V.H.; Hanh, D.T.H.; et al. A Trial of Itraconazole or Amphotericin B for HIV-Associated Talaromycosis. N. Engl. J. Med. 2017, 376, 2329–2340. [Google Scholar] [CrossRef]
- Firacative, C. Invasive fungal disease in humans: Are we aware of the real impact? Mem. Inst. Oswaldo Cruz 2020, 115, e200430. [Google Scholar] [CrossRef] [PubMed]
- Perfect, J.R. The impact of the host on fungal infections. Am. J. Med. 2012, 125, S39-51. [Google Scholar] [CrossRef]
- Li, X.; Lau, S.K.P.; Woo, P.C.Y. Fungal infection risks associated with the use of cytokine antagonists and immune checkpoint inhibitors. Exp. Biol. Med. 2020, 245, 1104–1114. [Google Scholar] [CrossRef] [PubMed]
- Chamilos, G.; Lionakis, M.S.; Kontoyiannis, D.P. Call for Action: Invasive Fungal Infections Associated With Ibrutinib and Other Small Molecule Kinase Inhibitors Targeting Immune Signaling Pathways. Clin. Infect. Dis. 2018, 66, 140–148. [Google Scholar] [CrossRef] [Green Version]
- Lionakis, M.S.; Dunleavy, K.; Roschewski, M.; Widemann, B.C.; Butman, J.A.; Schmitz, R.; Yang, Y.; Cole, D.E.; Melani, C.; Higham, C.S.; et al. Inhibition of B Cell Receptor Signaling by Ibrutinib in Primary CNS Lymphoma. Cancer Cell 2017, 31, 833–843.e5. [Google Scholar] [CrossRef] [Green Version]
- Naik, B.; Ahmed, S.M.Q.; Laha, S.; Das, S.P. Genetic Susceptibility to Fungal Infections and Links to Human Ancestry. Front. Genet. 2021, 12, 1417. [Google Scholar] [CrossRef] [PubMed]
- Mathew, J.M.; Patrick, M.M.; William, L.M.; Dimitrios, P.K. Serum Levels of Crushed Posaconazole Delayed-Release Tablets. Antimicrob. Agents Chemother. 2021, 63, e02688-18. [Google Scholar] [CrossRef] [Green Version]
- Veringa, A.; ter Avest, M.; Span, L.F.R.; van den Heuvel, E.R.; Touw, D.J.; Zijlstra, J.G.; Kosterink, J.G.W.; van der Werf, T.S.; Alffenaar, J.-W.C. Voriconazole metabolism is influenced by severe inflammation: A prospective study. J. Antimicrob. Chemother. 2017, 72, 261–267. [Google Scholar] [CrossRef]
- van der Elst, K.C.M.; Brouwers, C.H.S.; van den Heuvel, E.R.; van Wanrooy, M.J.P.; Uges, D.R.A.; van der Werf, T.S.; Kosterink, J.G.W.; Span, L.F.R.; Alffenaar, J.-W.C. Subtherapeutic Posaconazole Exposure and Treatment Outcome in Patients With Invasive Fungal Disease. Ther. Drug Monit. 2015, 37, 766–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruggemann, R.J.M.; Alffenaar, J.-W.C.; Blijlevens, N.M.A.; Billaud, E.M.; Kosterink, J.G.W.; Verweij, P.E.; Burger, D.M. Clinical relevance of the pharmacokinetic interactions of azole antifungal drugs with other coadministered agents. Clin. Infect. Dis. 2009, 48, 1441–1458. [Google Scholar] [CrossRef] [Green Version]
- Johnson, L.B.; Kauffman, C.A. Voriconazole: A new triazole antifungal agent. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2003, 36, 630–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purkins, L.; Wood, N.; Ghahramani, P.; Love, E.R.; Eve, M.D.; Fielding, A. Coadministration of voriconazole and phenytoin: Pharmacokinetic interaction, safety, and toleration. Br. J. Clin. Pharmacol. 2003, 56 (Suppl. 1), 37–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geist, M.J.P.; Egerer, G.; Burhenne, J.; Riedel, K.-D.; Mikus, G. Induction of voriconazole metabolism by rifampin in a patient with acute myeloid leukemia: Importance of interdisciplinary communication to prevent treatment errors with complex medications. Antimicrob. Agents Chemother. 2007, 51, 3455–3456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellmann, R.; Smuszkiewicz, P. Pharmacokinetics of antifungal drugs: Practical implications for optimized treatment of patients. Infection 2017, 45, 737–779. [Google Scholar] [CrossRef]
- Luong, M.-L.; Al-Dabbagh, M.; Groll, A.H.; Racil, Z.; Nannya, Y.; Mitsani, D.; Husain, S. Utility of voriconazole therapeutic drug monitoring: A meta-analysis. J. Antimicrob. Chemother. 2016, 71, 1786–1799. [Google Scholar] [CrossRef] [PubMed]
- Kelesidis, T.; Falagas, M.E. Substandard/counterfeit antimicrobial drugs. Clin. Microbiol. Rev. 2015, 28, 443–464. [Google Scholar] [CrossRef] [Green Version]
- Ashley, E.S.D.; Lewis, R.; Lewis, J.S.; Martin, C.; Andes, D. Pharmacology of Systemic Antifungal Agents. Clin. Infect. Dis. 2006, 43, S28–S39. [Google Scholar] [CrossRef] [Green Version]
- Theuretzbacher, U. Pharmacokinetics/pharmacodynamics of echinocandins. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2004, 23, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Stott, K.E.; Hope, W. Pharmacokinetics-pharmacodynamics of antifungal agents in the central nervous system. Expert Opin. Drug Metab. Toxicol. 2018, 14, 803–815. [Google Scholar] [CrossRef]
- Hope, W.W.; Drusano, G.L. Antifungal pharmacokinetics and pharmacodynamics: Bridging from the bench to bedside. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2009, 15, 602–612. [Google Scholar] [CrossRef]
- Chen, L.; Krekels, E.H.J.; Verweij, P.E.; Buil, J.B.; Knibbe, C.A.J.; Brüggemann, R.J.M. Pharmacokinetics and Pharmacodynamics of Posaconazole. Drugs 2020, 80, 671–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasmann, R.E.; Muilwijk, E.W.; Burger, D.M.; Verweij, P.E.; Knibbe, C.A.; Brüggemann, R.J. Clinical Pharmacokinetics and Pharmacodynamics of Micafungin. Clin. Pharmacokinet. 2018, 57, 267–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lempers, V.J.; Brüggemann, R.J. Antifungal therapy: Drug-drug interactions at your fingertips. J. Antimicrob. Chemother. 2016, 71, 285–289. [Google Scholar] [CrossRef] [Green Version]
- Felton, T.; Troke, P.F.; Hope, W.W. Tissue penetration of antifungal agents. Clin. Microbiol. Rev. 2014, 27, 68–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hicks, J.K.; Quilitz, R.E.; Komrokji, R.S.; Kubal, T.E.; Lancet, J.E.; Pasikhova, Y.; Qin, D.; So, W.; Caceres, G.; Kelly, K.; et al. Prospective CYP2C19-Guided Voriconazole Prophylaxis in Patients With Neutropenic Acute Myeloid Leukemia Reduces the Incidence of Subtherapeutic Antifungal Plasma Concentrations. Clin. Pharmacol. Ther. 2020, 107, 563–570. [Google Scholar] [CrossRef]
- Wasmann, R.E.; Smit, C.; Ter Heine, R.; Koele, S.E.; van Dongen, E.P.H.; Wiezer, R.M.J.; Burger, D.M.; Knibbe, C.A.J.; Brüggemann, R.J.M. Pharmacokinetics and probability of target attainment for micafungin in normal-weight and morbidly obese adults. J. Antimicrob. Chemother. 2019, 74, 978–985. [Google Scholar] [CrossRef]
- Bailly, S.; Gautier-Veyret, E.; Lê, M.P.; Bouadma, L.; Andremont, O.; Neuville, M.; Mourvillier, B.; Sonneville, R.; Magalhaes, E.; Lebut, J.; et al. Impact of Loading Dose of Caspofungin in Pharmacokinetic-Pharmacodynamic Target Attainment for Severe Candidiasis Infections in Patients in Intensive Care Units: The CASPOLOAD Study. Antimicrob. Agents Chemother. 2020, 64. [Google Scholar] [CrossRef]
- Patel, J.N.; Hamadeh, I.S.; Robinson, M.; Shahid, Z.; Symanowski, J.; Steuerwald, N.; Hamilton, A.; Reese, E.S.; Plesca, D.C.; Arnall, J.; et al. Evaluation of CYP2C19 Genotype-Guided Voriconazole Prophylaxis After Allogeneic Hematopoietic Cell Transplant. Clin. Pharmacol. Ther. 2020, 107, 571–579. [Google Scholar] [CrossRef]
- Wicha, S.G.; Märtson, A.-G.; Nielsen, E.I.; Koch, B.C.P.; Friberg, L.E.; Alffenaar, J.-W.; Minichmayr, I.K. From Therapeutic Drug Monitoring to Model-Informed Precision Dosing for Antibiotics. Clin. Pharmacol. Ther. 2021, 109, 928–941. [Google Scholar] [CrossRef] [PubMed]
- Autmizguine, J.; Guptill, J.T.; Cohen-Wolkowiez, M.; Benjamin, D.K.J.; Capparelli, E.V. Pharmacokinetics and pharmacodynamics of antifungals in children: Clinical implications. Drugs 2014, 74, 891–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Euteneuer, J.C.; Kamatkar, S.; Fukuda, T.; Vinks, A.A.; Akinbi, H.T. Suggestions for Model-Informed Precision Dosing to Optimize Neonatal Drug Therapy. J. Clin. Pharmacol. 2019, 59, 168–176. [Google Scholar] [CrossRef]
- Hope, W.W.; Vanguilder, M.; Donnelly, J.P.; Blijlevens, N.M.A.; Bruggemann, R.J.M.; Jelliffe, R.W.; Neely, M.N. Software for dosage individualization of voriconazole for immunocompromised patients. Antimicrob. Agents Chemother. 2013, 57, 1888–1894. [Google Scholar] [CrossRef] [Green Version]
- Kovanda, L.L.; Kolamunnage-Dona, R.; Neely, M.; Maertens, J.; Lee, M.; Hope, W.W. Pharmacodynamics of Isavuconazole for Invasive Mold Disease: Role of Galactomannan for Real-Time Monitoring of Therapeutic Response. Clin. Infect. Dis. 2017, 64, 1557–1563. [Google Scholar] [CrossRef]
- Nucci, M.; Nouér, S.A.; Anaissie, E. Distinguishing the Causes of Pulmonary Infiltrates in Patients With Acute Leukemia. Clin. Lymphoma. Myeloma Leuk. 2015, 15, S98–S103. [Google Scholar] [CrossRef] [PubMed]
- Ankrah, A.O.; Span, L.F.R.; Klein, H.C.; de Jong, P.A.; Dierckx, R.A.J.O.; Kwee, T.C.; Sathekge, M.M.; Glaudemans, A.W.J.M. Role of FDG PET/CT in monitoring treatment response in patients with invasive fungal infections. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 174–183. [Google Scholar] [CrossRef] [Green Version]
- Ankrah, A.O.; Klein, H.C.; Span, L.F.R.; de Vries, E.F.J.; Dierckx, R.A.J.O.; Sathekge, M.M.; Glaudemans, A.W.J.M. The Role of PET in Monitoring Therapy in Fungal Infections. Curr. Pharm. Des. 2018, 24, 795–805. [Google Scholar] [CrossRef] [Green Version]
- Maertens, J.A.; Raad, I.I.; Marr, K.A.; Patterson, T.F.; Kontoyiannis, D.P.; Cornely, O.A.; Bow, E.J.; Rahav, G.; Neofytos, D.; Aoun, M.; et al. Isavuconazole versus voriconazole for primary treatment of invasive mould disease caused by Aspergillus and other filamentous fungi (SECURE): A phase 3, randomised-controlled, non-inferiority trial. Lancet 2016, 387, 760–769. [Google Scholar] [CrossRef]
- Marr, K.A.; Schlamm, H.T.; Herbrecht, R.; Rottinghaus, S.T.; Bow, E.J.; Cornely, O.A.; Heinz, W.J.; Jagannatha, S.; Koh, L.P.; Kontoyiannis, D.P.; et al. Combination antifungal therapy for invasive aspergillosis: A randomized trial. Ann. Intern. Med. 2015, 162, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Jeans, A.R.; Howard, S.J.; Al-Nakeeb, Z.; Goodwin, J.; Gregson, L.; Warn, P.A.; Hope, W.W. Combination of voriconazole and anidulafungin for treatment of triazole-resistant Aspergillus fumigatus in an in vitro model of invasive pulmonary aspergillosis. Antimicrob. Agents Chemother. 2012, 56, 5180–5185. [Google Scholar] [CrossRef] [Green Version]
- Le, T.; Ly, V.T.; Thu, N.T.M.; Nguyen, A.; Thanh, N.T.; Chau, N.V.V.; Thwaites, G.; Perfect, J.; Kolamunnage-Dona, R.; Hope, W. Population Pharmacodynamics of Amphotericin B Deoxycholate for Disseminated Infection Caused by Talaromyces marneffei. Antimicrob. Agents Chemother. 2019, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huurneman, L.J.; Neely, M.; Veringa, A.; Docobo Perez, F.; Ramos-Martin, V.; Tissing, W.J.; Alffenaar, J.-W.C.; Hope, W. Pharmacodynamics of Voriconazole in Children: Further Steps along the Path to True Individualized Therapy. Antimicrob. Agents Chemother. 2016, 60, 2336–2342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, R.E.; Wiederhold, N.P.; Klepser, M.E. In Vitro Pharmacodynamics of Amphotericin B, Itraconazole, and Voriconazole against Aspergillus, Fusarium, and Scedosporium spp. Antimicrob. Agents Chemother. 2005, 49, 945–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
A schematic illustrating the use of a biomarker to guide antifungal therapy. The sold stars and triangles depict a favourable and suboptimal response to antifungal therapy, respectively. Figure created with Biorender.com, accessed on 13 December 2021.
Figure 1.
A schematic illustrating the use of a biomarker to guide antifungal therapy. The sold stars and triangles depict a favourable and suboptimal response to antifungal therapy, respectively. Figure created with Biorender.com, accessed on 13 December 2021.


{kind=link}
Table 1.
TDM of antifungal drugs.
| PK and PK/PD Index Targets | References | |
|---|---|---|
| Echinocandins | ||
| Caspofungin | AUC/MIC = 450–1185 a Clinical target undefined | [4] |
| Micafungin | AUC/MIC >285 b >3000 c | [5,6,7] |
| Anidulafungin | AUC/MIC = 123–2033 a Clinical target undefined | [8,9] |
| Triazoles | ||
| Fluconazole | AUC/MIC > 100 d | [10,11,12,13] |
| Itraconazole | Cmin > 1 mg/L d Cmin < 5 mg/L e | [14,15] |
| Posaconazole | Prophylaxis: Cmin > 0.7 mg/L d Treatment: Cmin > 1–1.25 mg/L d AUC/MIC~ 200 f | [14,16,17,18] |
| Voriconazole | Cmin > 1 mg/L d Cmin < 4–6 mg/L e Cmin/MIC = 2–5 g | [11,14,19] |
| Isavuconazole | Clinical target undefined | [15] |
| Amphotericin B | Clinical target undefined Likely considerable differences between formulations | [15,19] |
| 5-flucytosine | Cmax < 100 mg/L e | [15,20] |
TDM, therapeutic drug monitoring; PK, pharmacokinetics; PD, pharmacodynamics; Cmin, trough concentration; AUC, area under the concentration-time curve; Cmax, maximal concentration; MIC, minimal inhibitory concentration; a. Candida glabrata, Candida albicans, Candida tropicalis, Candida parapsilosis in murine models of disseminated candidiasis; b. Candida parapsilosis (invasive candidiasis); c. non-Candida parapsilosis population (invasive candidiasis); d. Efficacy; e. Toxicity; f. Aspergillus spp.; g. determined against invasive infections caused by medically important yeasts and moulds.
Table 2.
Antifungal drugs resistance mechanisms.
| Drug Class | Drug Resistance | References |
|---|---|---|
| Triazoles | Inhibition, low binding affinity of enzyme 14α-demethylase through mutations (Erg11 p, drug target) Overexpression of enzyme 14α-demethylase (drug target) Efflux of antifungals through proteins in the major facilitator and ATP-binding cassette (CDR1-CDR5) superfamilies Genomic changes: loss of heterozygosity, segmental or chromosomal aneuploidies, chromosome copy number increase Combination of different mechanisms | [25,28,29,30,31] |
| Echinocandins | Fks mutations (substitutions of amino acids, Fks encodes the protein β-1, 3-glucan synthase) Not affected by transporters | [25,32,33,34] |
| Polyenes | Much less common than in azoles and echinocandins Mutations in genes involved in ergosterol biosynthesis (ERG genes) Proposed mechanism–decrease of polyene caused oxidative stress | [25,35] |
| 5-flucytosine | FUR1, FCY1, FCY2, UXS1 mutations | [36,37,38] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Märtson, A.-G.; Alffenaar, J.-W.C.; Brüggemann, R.J.; Hope, W. Precision Therapy for Invasive Fungal Diseases. J. Fungi 2022, 8, 18. https://doi.org/10.3390/jof8010018
AMA Style
Märtson A-G, Alffenaar J-WC, Brüggemann RJ, Hope W. Precision Therapy for Invasive Fungal Diseases. Journal of Fungi. 2022; 8(1):18. https://doi.org/10.3390/jof8010018
Chicago/Turabian StyleMärtson, Anne-Grete, Jan-Willem C. Alffenaar, Roger J. Brüggemann, and William Hope. 2022. "Precision Therapy for Invasive Fungal Diseases" Journal of Fungi 8, no. 1: 18. https://doi.org/10.3390/jof8010018
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.