
The Long-Acting Echinocandin, Rezafungin, Prevents Pneumocystis Pneumonia and Eliminates Pneumocystis from the Lungs in Prophylaxis and Murine Treatment Models


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
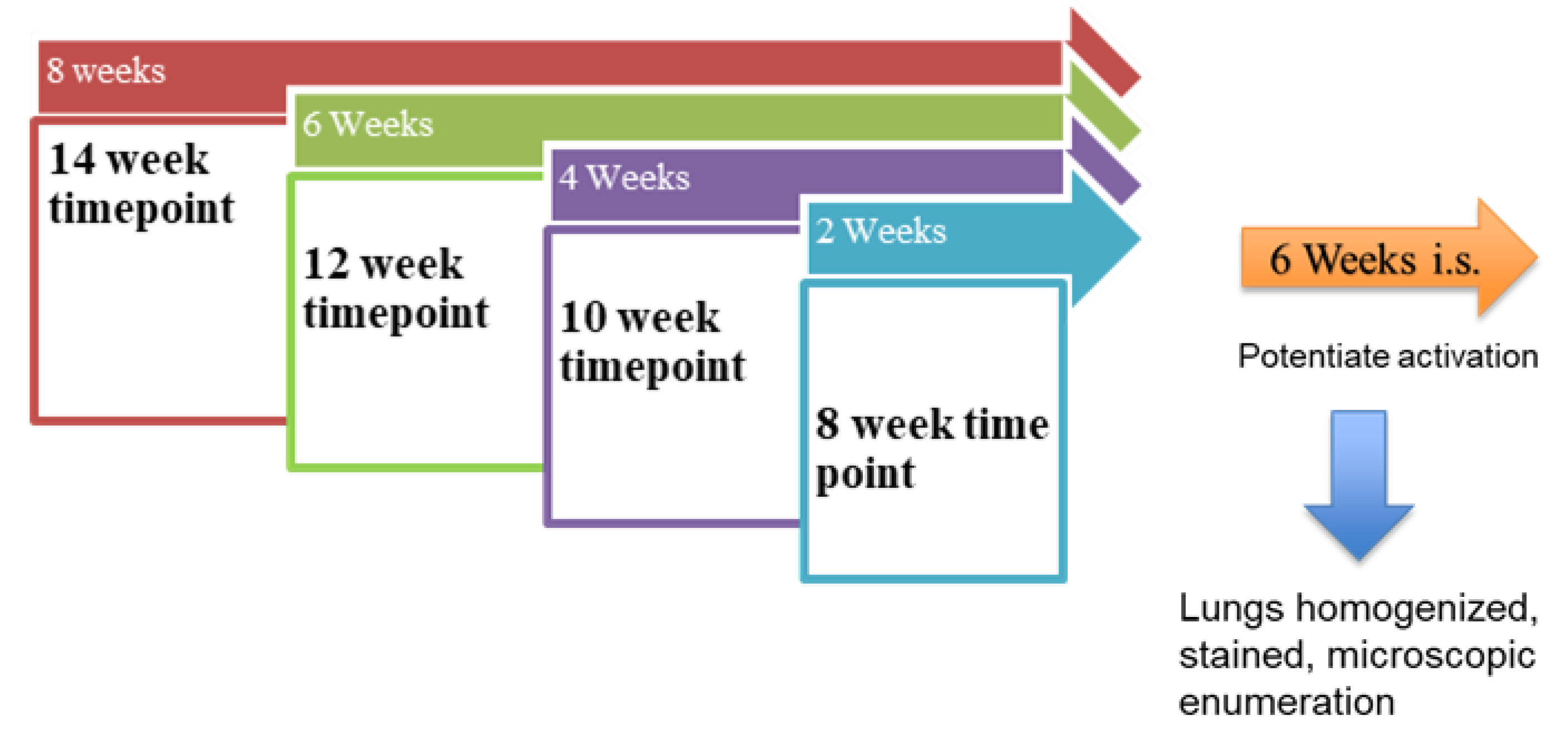
2.1. PCP Prophylaxis Mouse Model
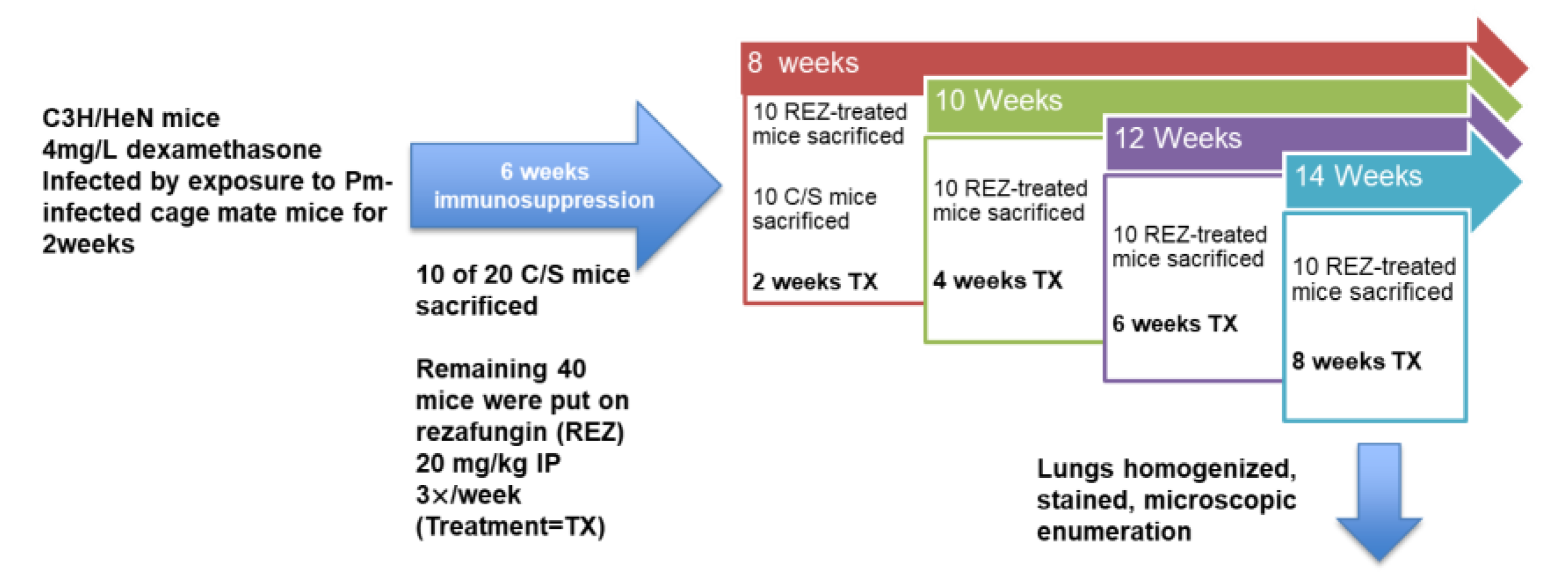
2.2. PCP Treatment Mouse Model
2.3. Statistical Analysis
3. Results
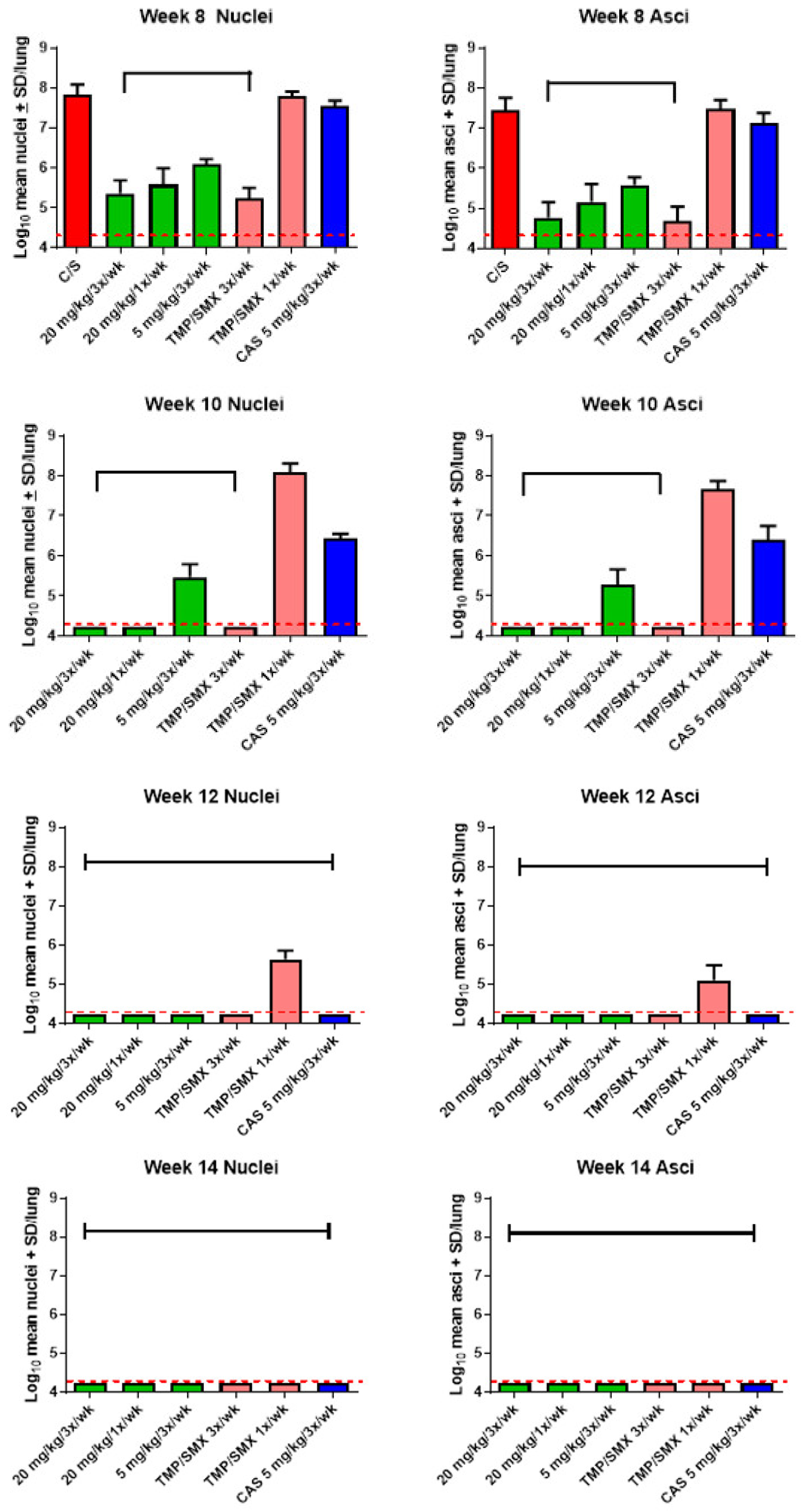
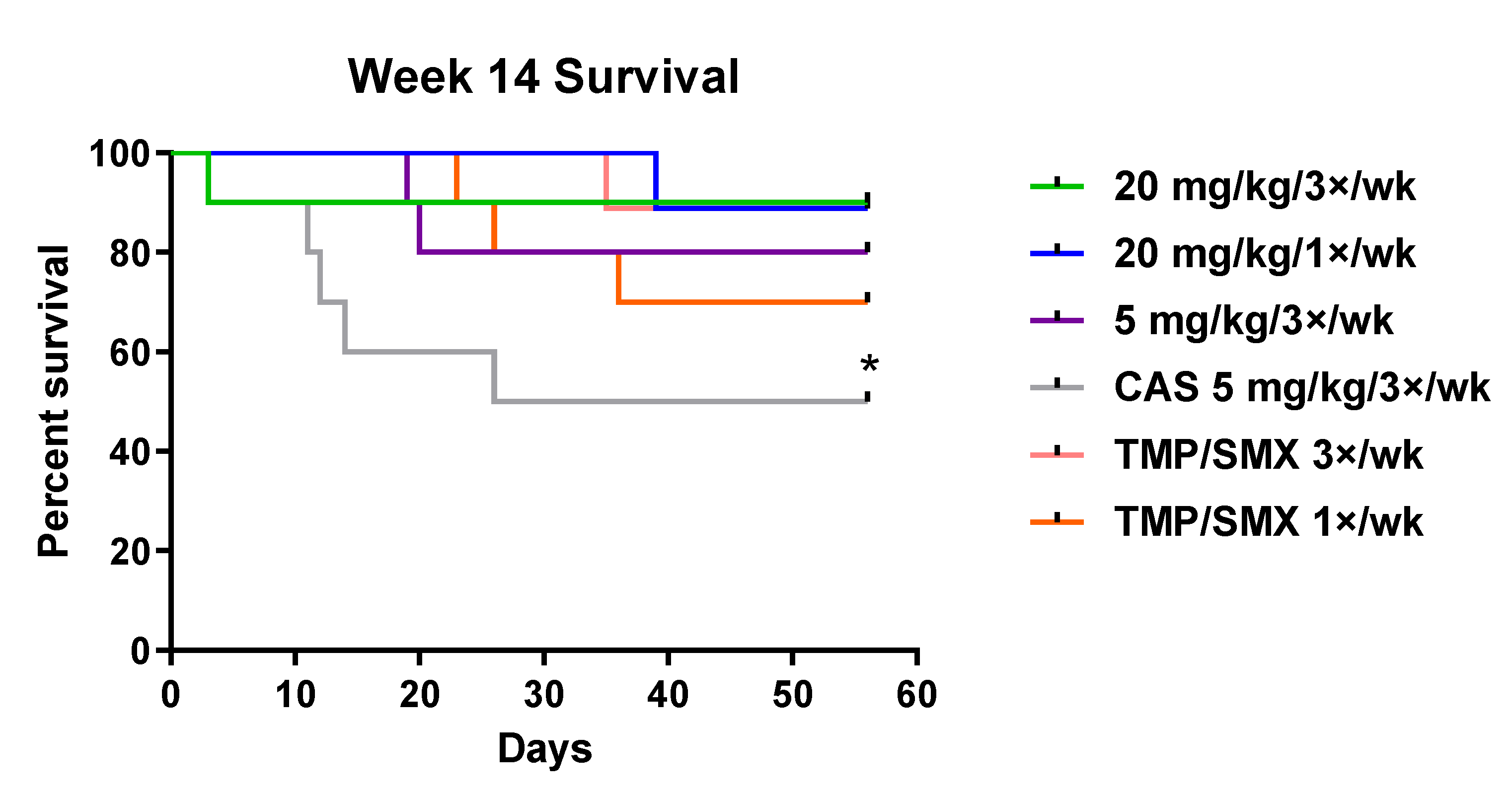
3.1. PCP Prophylaxis Mouse Model
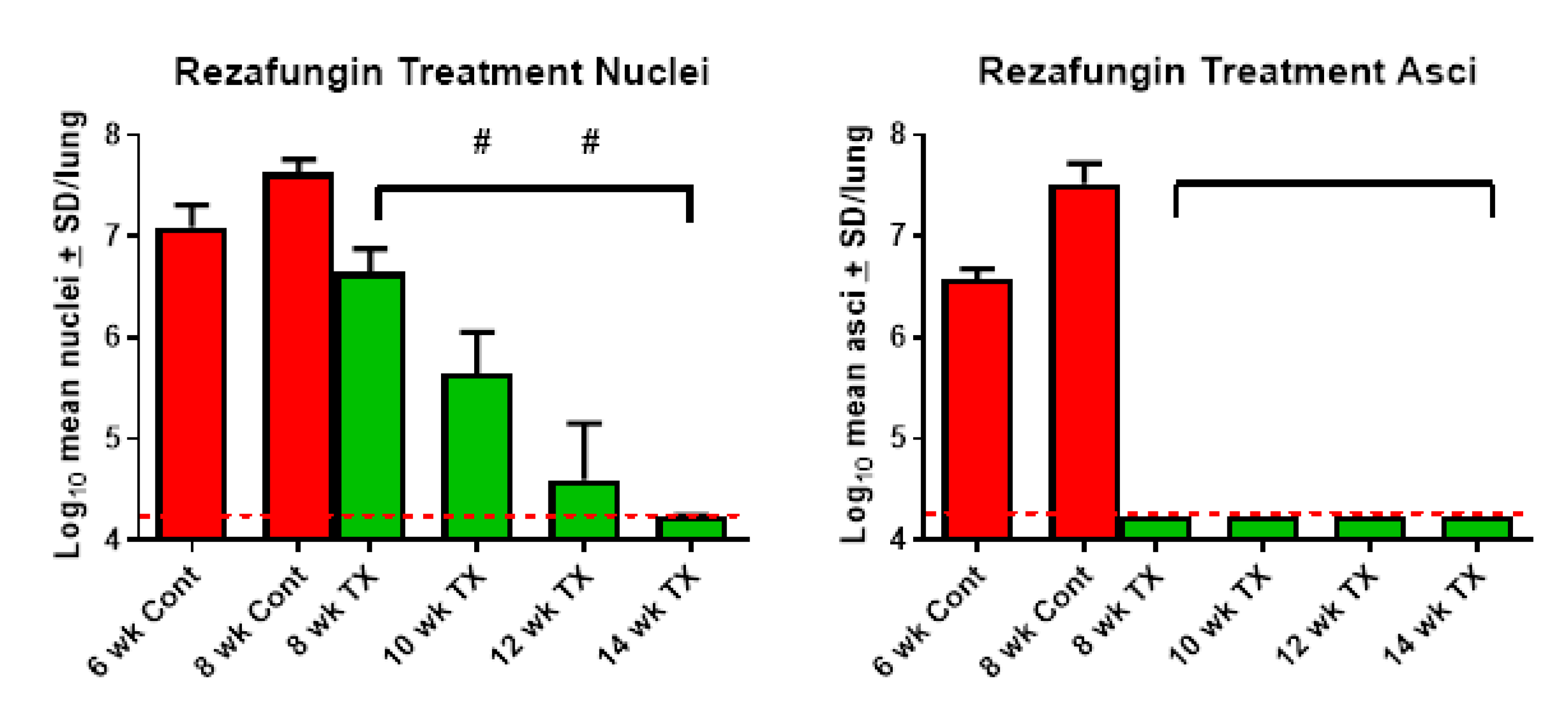
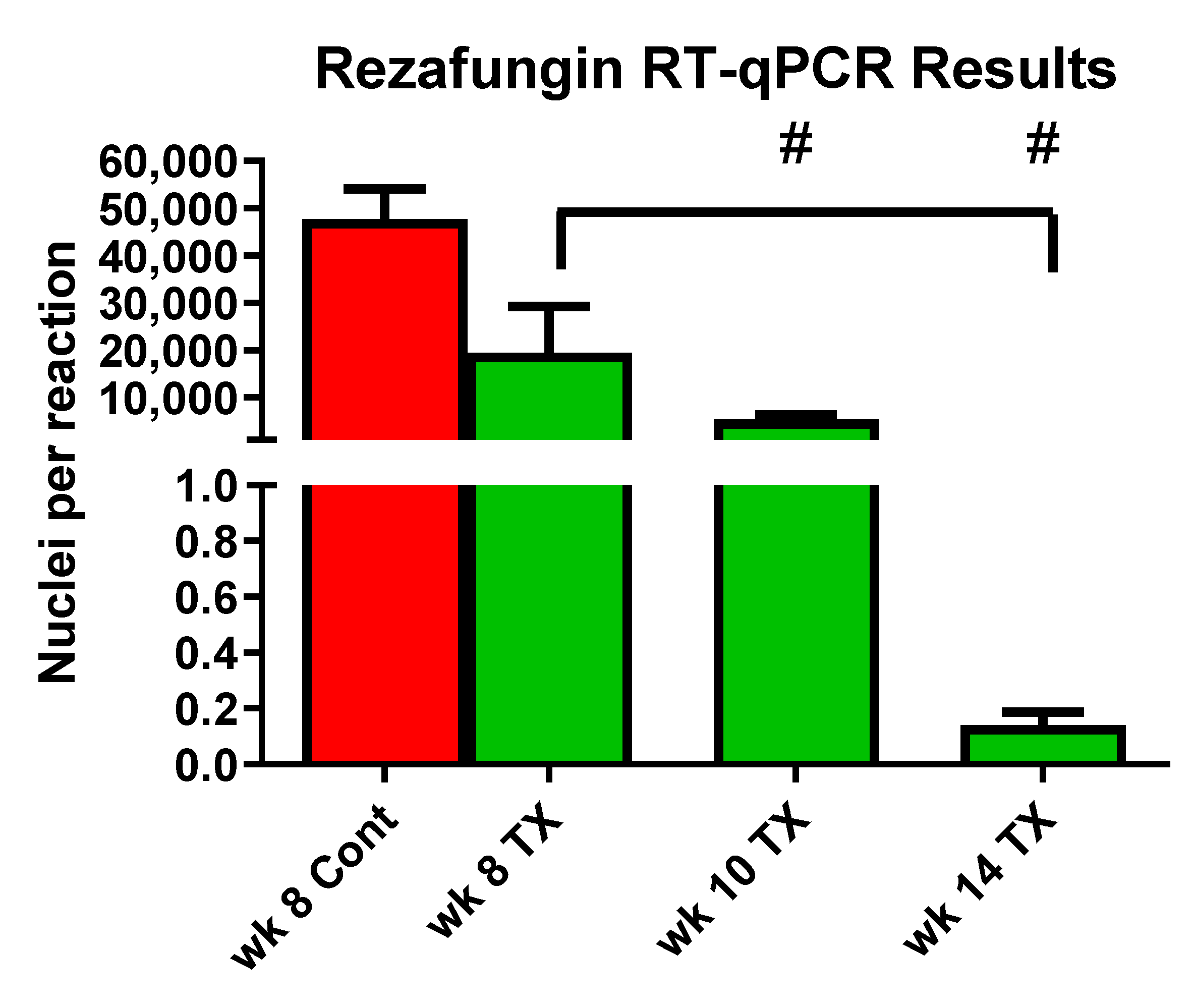
3.2. PCP Treatment Mouse Model
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brakemeier, S.; Pfau, A.; Zukunft, B.; Budde, K.; Nickel, P. Prophylaxis and treatment of Pneumocystis jirovecii pneumonia after solid organ transplantation. Pharmacol. Res. 2018, 134, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Cordonnier, C.; Cesaro, S.; Maschmeyer, G.; Einsele, H.; Donnelly, J.P.; Alanio, A.; Hauser, P.M.; Lagrou, K.; Melchers, W.J.; Helweg-Larsen, J.; et al. Pneumocystis jirovecii pneumonia: Still a concern in patients with haematological malignancies and stem cell transplant recipients. J. Antimicrob. Chemother. 2016, 71, 2379–2385. [Google Scholar] [PubMed] [Green Version]
- Fishman, J.A.; Gans, H. Pneumocystis jiroveci in solid organ transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13587. [Google Scholar] [CrossRef]
- Salzer, H.J.F.; Schafer, G.; Hoenigl, M.; Gunther, G.; Hoffmann, C.; Kalsdorf, B.; Alanio, A.; Lange, C. Clinical, Diagnostic, and Treatment Disparities between HIV-Infected and Non-HIV-Infected Immunocompromised Patients with Pneumocystis jirovecii Pneumonia. Respiration 2018, 96, 52–65. [Google Scholar] [CrossRef]
- Sokulska, M.; Kicia, M.; Wesolowska, M.; Hendrich, A.B. Pneumocystis jirovecii—From a commensal to pathogen: Clinical and diagnostic review. Parasitol. Res. 2015, 114, 3577–3585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redhead, S.A.; Cushion, M.T.; Frenkel, J.K.; Stringer, J.R. Pneumocystis and Trypanosoma cruzi: Nomenclature and typifications. J. Eukaryot. Microbiol. 2006, 53, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Truong, J.; Ashurst, J.V. Pneumocystis jirovecii Pneumonia; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Delliere, S.; Gits-Muselli, M.; Bretagne, S.; Alanio, A. Outbreak-Causing Fungi: Pneumocystis jirovecii. Mycopathologia 2020, 185, 783–800. [Google Scholar] [CrossRef] [PubMed]
- Cilloniz, C.; Dominedo, C.; Alvarez-Martinez, M.J.; Moreno, A.; Garcia, F.; Torres, A.; Miro, J.M. Pneumocystis pneumonia in the twenty-first century: HIV-infected versus HIV-uninfected patients. Expert Rev. Anti. Infect. Ther. 2019, 17, 787–801. [Google Scholar] [CrossRef] [PubMed]
- Tabanor, J.A.; Lakshminarayanan, S. Do patients on biologic drugs for rheumatic disease need PCP prophylaxis? Cleve. Clin. J. Med. 2019, 86, 449–453. [Google Scholar] [CrossRef]
- Kanj, A.; Samhouri, B.; Abdallah, N.; Chehab, O.; Baqir, M. Host Factors and Outcomes in Hospitalizations for Pneumocystis jirovecii Pneumonia in the United States. Mayo Clin. Proc. 2021, 96, 400–407. [Google Scholar] [CrossRef]
- Maertens, J.; Cesaro, S.; Maschmeyer, G.; Einsele, H.; Donnelly, J.P.; Alanio, A.; Hauser, P.M.; Lagrou, K.; Melchers, W.J.; Helweg-Larsen, J.; et al. ECIL guidelines for preventing Pneumocystis jirovecii pneumonia in patients with haematological malignancies and stem cell transplant recipients. J. Antimicrob. Chemother. 2016, 71, 2397–2404. [Google Scholar] [PubMed] [Green Version]
- Redjoul, R.; Robin, C.; Foulet, F.; Leclerc, M.; Beckerich, F.; Cabanne, L.; di Blasi, R.; Pautas, C.; Toma, A.; Botterel, F.; et al. Pneumocystis jirovecii pneumonia prophylaxis in allogeneic hematopoietic cell transplant recipients: Can we always follow the guidelines? Bone Marrow Transpl. 2019, 54, 1082–1088. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.I.; Hwang, S.; Park, G.C.; Namgoong, J.M.; Jung, D.H.; Song, G.W.; Ha, T.Y.; Moon, D.B.; Kim, K.H.; Ahn, C.S.; et al. Clinical outcomes of Pneumocystis carinii pneumonia in adult liver transplant recipients. Transplant. Proc. 2013, 45, 3057–3060. [Google Scholar] [CrossRef] [PubMed]
- Iriart, X.; Belval, T.C.; Fillaux, J.; Esposito, L.; Lavergne, R.A.; Cardeau-Desangles, I.; Roques, O.; del Bello, A.; Cointault, O.; Lavayssiere, L.; et al. Risk factors of Pneumocystis pneumonia in solid organ recipients in the era of the common use of posttransplantation prophylaxis. Am. J. Transpl. 2015, 15, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.H.; Partovi, N.; Levy, R.D.; Shapiro, R.J.; Yoshida, E.M.; Greanya, E.D. Pneumocystis pneumonia in solid organ transplant recipients: Not yet an infection of the past. Transpl. Infect. Dis. 2012, 14, 519–525. [Google Scholar] [CrossRef]
- Utsunomiya, M.; Dobashi, H.; Odani, T.; Saito, K.; Yokogawa, N.; Nagasaka, K.; Takenaka, K.; Soejima, M.; Sugihara, T.; Hagiyama, H.; et al. An open-label, randomized controlled trial of sulfamethoxazole-trimethoprim for Pneumocystis prophylaxis: Results of 52-week follow-up. Rheumatol. Adv. Pract. 2020, 4, rkaa029. [Google Scholar] [CrossRef]
- Wiederhold, N.P.; Locke, J.B.; Daruwala, P.; Bartizal, K. Rezafungin (CD101) demonstrates potent in vitro activity against Aspergillus, including azole-resistant Aspergillus fumigatus isolates and cryptic species. J. Antimicrob. Chemother. 2018, 73, 3063–3067. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Carvalhaes, C.; Messer, S.A.; Rhomberg, P.R.; Castanheira, M. Activity of a Long-Acting Echinocandin, Rezafungin, and Comparator Antifungal Agents Tested against Contemporary Invasive Fungal Isolates (SENTRY Program, 2016 to 2018). Antimicrob. Agents Chemother. 2020, 64, e00099-20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toth, Z.; Forgacs, L.; Locke, J.B.; Kardos, G.; Nagy, F.; Kovacs, R.; Szekely, A.; Borman, A.M.; Majoros, L. In vitro activity of rezafungin against common and rare Candida species and Saccharomyces cerevisiae. J. Antimicrob. Chemother. 2019, 74, 3505–3510. [Google Scholar] [CrossRef] [Green Version]
- Cushion, M.T.; Collins, M.S.; Locke, J.B.; Ong, V.; Bartizal, K. Novel Once-Weekly Echinocandin Rezafungin (CD101) Prevention and Treatment of Pneumocystis Biofilms; European Group for Bone and Marrow Transplantation: Lisbon, Portugal, 2018. [Google Scholar]
- Miesel, L.; Cushion, M.T.; Ashbaugh, A.; Lopez, S.R.; Ong, V. Efficacy of Rezafungin in Prophylactic Mouse Models of Invasive Candidiasis, Aspergillosis, and Pneumocystis Pneumonia. Antimicrob. Agents Chemother. 2021, 65, e01992-20. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Perlin, D.S. Review of the Novel Echinocandin Antifungal Rezafungin: Animal Studies and Clinical Data. J. Fungi 2020, 6, 192. [Google Scholar] [CrossRef] [PubMed]
- Ham, Y.Y.; Lewis, J.S., 2nd; Thompson, G.R., 3rd. Rezafungin: A novel antifungal for the treatment of invasive candidiasis. Future Microbiol. 2021, 16, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Sofjan, A.K.; Mitchell, A.; Shah, D.N.; Nguyen, T.; Sim, M.; Trojcak, A.; Beyda, N.D.; Garey, K.W. Rezafungin (CD101), a next-generation echinocandin: A systematic literature review and assessment of possible place in therapy. J. Glob. Antimicrob. Resist. 2018, 14, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.S.; Liu, C.E.; Lin, S.P.; Lee, C.H.; Yang, C.J.; Lin, C.Y.; Tang, H.J.; Lee, Y.C.; Lin, Y.C.; Lee, Y.T.; et al. Taiwan, Echinocandins as alternative treatment for HIV-infected patients with Pneumocystis pneumonia. AIDS 2019, 33, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-S.; Yang, J.-J.; Lee, N.-Y.; Chen, G.-J.; Ko, W.-C.; Sun, H.-Y.; Hung, C.-C. Treatment of Pneumocystis jirovecii pneumonia in HIV-infected patients: A review. Expert Rev. Anti-Infect. Ther. 2017, 15, 873–892. [Google Scholar] [CrossRef]
- Cushion, M.T.; Linke, M.J.; Ashbaugh, A.; Sesterhenn, T.; Collins, M.S.; Lynch, K.; Brubaker, R.; Walzer, P.D. Echinocandin treatment of pneumocystis pneumonia in rodent models depletes cysts leaving trophic burdens that cannot transmit the infection. PLoS ONE 2010, 5, e8524. [Google Scholar] [CrossRef] [PubMed]
- Cushion, M.T. Stealth and opportunism: Alternative lifestyles of species in the fungal genus Pneumocystis. Mol. Genet. Genom. MGG 2010, 64, 431–452. [Google Scholar]
- Hauser, P.M.; Cushion, M.T. Is sex necessary for the proliferation and transmission of Pneumocystis? PLoS Pathog. 2018, 14, e1007409. [Google Scholar] [CrossRef]
- Whipple, B.; Agar, J.; Zhao, J.; Pearce, D.A.; Kovács, A.D. The acidified drinking water-induced changes in the behavior and gut microbiota of wild-type mice depend on the acidification mode. Sci. Rep. 2021, 11, 2877. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.S.; Cushion, M.T. Standardization of an in vitro drug screening assay by use of cryopreserved and characterized Pneumocystis carinii populations. J. Eukaryot. Microbiol. Suppl. 2001, 48, 178S–179S. [Google Scholar] [CrossRef]
- Andes, D.; Diekema, D.J.; Pfaller, M.A.; Bohrmuller, J.; Marchillo, K.; Lepak, A. In vivo comparison of the pharmacodynamic targets for echinocandin drugs against Candida species. Antimicrob. Agents Chemother. 2010, 54, 2497–2506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merck & Co., Inc. Cancidas Prescribing Information; Merck & Co., Inc.: Kenilworth, NJ, USA, 2001. [Google Scholar]
- Lepak, A.J.; Zhao, M.; VanScoy, B.; Ambrose, P.G.; Andes, D.R. Pharmacodynamics of a Long-Acting Echinocandin, CD101, in a Neutropenic Invasive-Candidiasis Murine Model Using an Extended-Interval Dosing Design. Antimicrob. Agents Chemother. 2018, 62, e02154-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruan, S.; Tate, C.; Lee, J.J.; Ritter, T.; Kolls, J.K.; Shellito, J.E. Local delivery of the viral interleukin-10 gene suppresses tissue inflammation in murine Pneumocystis carinii infection. Infect. Immun. 2002, 70, 6107–6113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cushion, M.T.; Ashbaugh, A.; Hendrix, K.; Linke, M.J.; Tisdale, N.; Sayson, S.G.; Porollo, A. Gene Expression of Pneumocystis murina after Treatment with Anidulafungin Results in Strong Signals for Sexual Reproduction, Cell Wall Integrity, and Cell Cycle Arrest, Indicating a Requirement for Ascus Formation for Proliferation. Antimicrob. Agents Chemother. 2018, 62, e02513-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, D.J.; Seo, S.K.; Brown, J.M.; Papanicolaou, G.A. Echinocandin prophylaxis in patients undergoing haematopoietic cell transplantation and other treatments for haematological malignancies. J. Antimicrob. Chemother. 2018, 73, i60–i72. [Google Scholar] [CrossRef] [PubMed]
- Brüggemann, R.J.M.; Alffenaar, J.-W.C.; Blijlevens, N.M.A.; Billaud, E.M.; Kosterink, J.G.W.; Verweij, P.E.; Burger, D.M.; Saravolatz, L.D. Clinical Relevance of the Pharmacokinetic Interactions of Azole Antifungal Drugs with Other Coadministered Agents. Clin. Infect. Dis. 2009, 48, 1441–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Lang, G.; Chen, Y.; Hu, C.; Guo, Y.; Tao, R.; Dong, X.; Zhu, B. A Pilot Study of Echinocandin Combination with Trimethoprim/Sulfamethoxazole and Clindamycin for the Treatment of AIDS Patients with Pneumocystis Pneumonia. J. Immunol. Res. 2019, 2019, 8105075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, G.; Chen, M.; Zhang, S.; Zhou, H.; Ji, X.; Cai, J.; Lou, T.; Cui, W.; Zhang, N. Efficacy of caspofungin combined with trimethoprim/sulfamethoxazole as first-line therapy to treat non-HIV patients with severe pneumocystis pneumonia. Exp. Med. 2018, 15, 1594–1601. [Google Scholar] [CrossRef] [PubMed]
- Tian, Q.; Si, J.; Jiang, F.; Xu, R.; Wei, B.; Huang, B.; Li, Q.; Jiang, Z.; Zhao, T. Caspofungin combined with TMP/SMZ as a first-line therapy for moderate-to-severe PCP in patients with human immunodeficiency virus infection. HIV Med. 2021, 22, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Sandison, T.; Ong, V.; Lee, J.; Thye, D. Safety and Pharmacokinetics of CD101 IV, a Novel Echinocandin, in Healthy Adults. Antimicrob. Agents Chemother. 2017, 61, e01627-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, G.R.; Soriano, A.; Skoutelis, A.; Vazquez, J.A.; Honore, P.M.; Horcajada, J.P.; Spapen, H.; Bassetti, M.; Ostrosky-Zeichner, L.; Das, A.F.; et al. Rezafungin versus Caspofungin in a Phase 2, Randomized, Double-Blind Study for the Treatment of Candidemia and Invasive Candidiasis—The STRIVE Trial. In Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America; The Infectious Diseases Society of America: Arlington, VA, USA, 2020. [Google Scholar]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cushion, M.T.; Ashbaugh, A. The Long-Acting Echinocandin, Rezafungin, Prevents Pneumocystis Pneumonia and Eliminates Pneumocystis from the Lungs in Prophylaxis and Murine Treatment Models. J. Fungi 2021, 7, 747. https://doi.org/10.3390/jof7090747
Cushion MT, Ashbaugh A. The Long-Acting Echinocandin, Rezafungin, Prevents Pneumocystis Pneumonia and Eliminates Pneumocystis from the Lungs in Prophylaxis and Murine Treatment Models. Journal of Fungi. 2021; 7(9):747. https://doi.org/10.3390/jof7090747
Chicago/Turabian StyleCushion, Melanie T., and Alan Ashbaugh. 2021. "The Long-Acting Echinocandin, Rezafungin, Prevents Pneumocystis Pneumonia and Eliminates Pneumocystis from the Lungs in Prophylaxis and Murine Treatment Models" Journal of Fungi 7, no. 9: 747. https://doi.org/10.3390/jof7090747