
Testing Practices for Fungal Respiratory Infections and SARS-CoV-2 among Infectious Disease Specialists, United States

 , , and
, , and 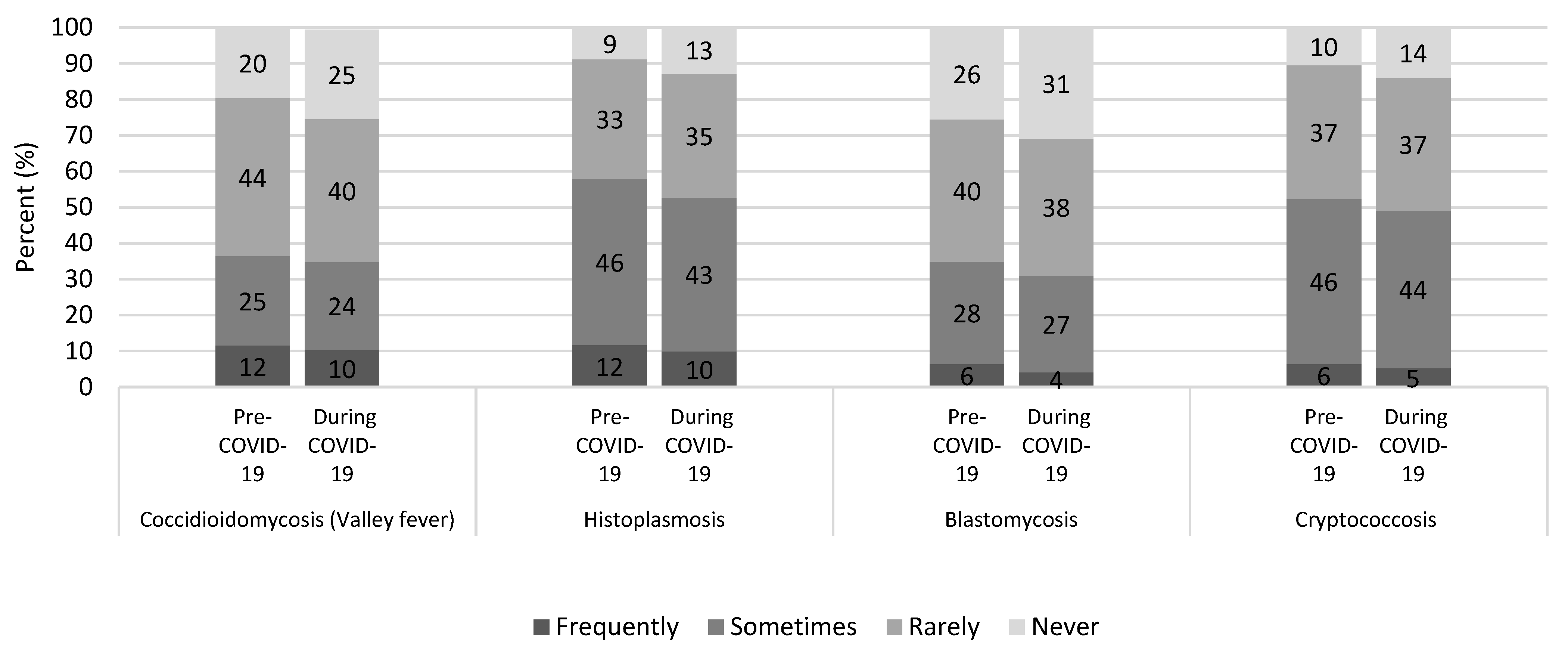{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Disclaimer
References
- CDC. Fungal Diseases and COVID-19. 2020. Available online: https://www.cdc.gov/fungal/covid-fungal.html (accessed on 10 May 2021).
- Beer, K.D.; Jackson, B.R.; Chiller, T.; Verweij, P.E.; Van de Veerdonk, F.L.; Wauters, J. Does Pulmonary Aspergillosis Complicate Coronavirus Disease 2019? Crit. Care Explor. 2020, 2, e0211. [Google Scholar] [CrossRef] [PubMed]
- John, T.M.; Jacob, C.N.; Kontoyiannis, D.P. When Uncontrolled Diabetes Mellitus and Severe COVID-19 Converge: The Perfect Storm for Mucormycosis. J. Fungi 2021, 7, 298. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.S.; Heidari, A.; Civelli, V.F.; Sharma, R.; Clark, C.S.; Munoz, A.D.; Ragland, A.S.; Johnson, R.H. The Coincidence of 2 Epidemics, Coccidioidomycosis and SARS-CoV-2: A Case Report. J. Investig. Med. High Impact Case Rep. 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Messina, F.A.; Marin, E.; Caceres, D.H.; Romero, M.; Depardo, R.; Priarone, M.M.; Rey, L.; Vázquez, M.; Verweij, P.E.; Chiller, T.M.; et al. Coronavirus Disease 2019 (COVID-19) in a Patient with Disseminated Histoplasmosis and HIV-A Case Report from Argentina and Literature Review. J. Fungi 2020, 6, 275. [Google Scholar] [CrossRef] [PubMed]
- Khatib, M.Y.; Ahmed, A.A.; Shaat, S.B.; Mohamed, A.S.; Nashwan, A.J. Cryptococcemia in a Patient with COVID-19: A case report. Clin. Case Rep. 2020, 9, 853–855. [Google Scholar] [CrossRef] [PubMed]
- Howard, M.; Heller, H.M.; Gonzalez, R.G.; Edlow, B.L.; Ard, K.L.; Gogakos, T. Case 40-2020: A 24-Year-Old Man with Headache and Covid-19. N. Engl. J. Med. 2020, 383, 2572–2580. [Google Scholar] [CrossRef]
- Chang, C.C.; Senining, R.; Kim, J.; Goyal, R. An Acute Pulmonary Coccidioidomycosis Coinfection in a Patient Presenting with Multifocal Pneumonia With COVID-19. J. Investig. Med. High Impact Case Rep. 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, M.; Mutti, M.F.; Barletta, J.A.; Falak, A.; Cuatz, D.; Sisto, A.; Ragusa, M.; Fernandez Claros, N.O.; Rolón, M.J. COVID-19 associated with AIDS-related disseminated histoplasmosis: A case report. Int. J. STD AIDS 2020, 31, 1222–1224. [Google Scholar] [CrossRef] [PubMed]
- Basso, R.P.; Poester, V.R.; Benelli, J.L.; Stevens, D.A.; Zogbi, H.E.; Vasconcellos, I.; Comarú Pasqualotto, A.; Orzechowski Xavier, M.O. COVID-19-Associated Histoplasmosis in an AIDS Patient. Mycopathologia 2020, 186, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Benedict, K.; Li, Y.; Molinari, N.A.M.; Jackson, B.R. Healthcare Providers’ Testing Practices for Coccidioidomycosis and Histoplasmosis in Patients with Community-Acquired Pneumonia—United States, 2020. Open Forum Infect. Dis. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Pillai, S.K.; Beekmann, S.E.; Santibanez, S.; Polgreen, P.M. The Infectious Diseases Society of America Emerging Infections Network: Bridging the Gap Between Clinical Infectious Diseases and Public Health. Clin. Infect. Dis. 2014, 58, 991–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention (Atlanta, GA, USA). Infectious disease physicians’ reported testing frequency for coccidioidomycosis, histoplasmosis, blastomycosis, and cryptococcosis among patients with signs and symptoms of community-acquired pneumonia, before and during the COVID-19 pandemic, United States, by disease and region. 2021. [Google Scholar]
- Stasiak, C.E.S.; Nigri, D.H.; Cardoso, F.R.; de Almeida Rezende de Mattos, R.S.; Martins, P.A.G.; Carvalho, A.R.S.; de Almeida, S.A.; Rodrigues, R.S.; Rosado-de-Castro, P.H. Case report: Incidental Finding of COVID-19 Infection after PET/CT Imaging in a Patient with Diagnosis of Histoplasmosis and Recurring Fever. Am. J. Trop. Med. Hygiene 2021, 104, 1651–1654. [Google Scholar] [CrossRef] [PubMed]
- CDC. Burden of Fungal Diseases in the United States. 2020. Available online: https://www.cdc.gov/fungal/cdc-and-fungal/burden.html (accessed on 10 May 2021).
- Salmanton-García, J.; Sprute, R.; Stemler, J.; Bartoletti, M.; Dupont, D.; Valerio, M.; Garcia-Vidal, C.; Falces-Romero, I.; Machado, M.; de la Villa, S.; et al. COVID-19–Associated Pulmonary Aspergillosis. Emerg. Infect. Dis. 2021, 27, 1077–1086. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, S.R.; Toda, M.; Benedict, K.; Caceres, D.H.; Litvintseva, A.P. Endemic and Other Dimorphic Mycoses in the Americas. J. Fungi 2021, 7, 151. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benedict, K.; Williams, S.; Beekmann, S.E.; Polgreen, P.M.; Jackson, B.R.; Toda, M. Testing Practices for Fungal Respiratory Infections and SARS-CoV-2 among Infectious Disease Specialists, United States. J. Fungi 2021, 7, 605. https://doi.org/10.3390/jof7080605
Benedict K, Williams S, Beekmann SE, Polgreen PM, Jackson BR, Toda M. Testing Practices for Fungal Respiratory Infections and SARS-CoV-2 among Infectious Disease Specialists, United States. Journal of Fungi. 2021; 7(8):605. https://doi.org/10.3390/jof7080605
Chicago/Turabian StyleBenedict, Kaitlin, Samantha Williams, Susan E. Beekmann, Philip M. Polgreen, Brendan R. Jackson, and Mitsuru Toda. 2021. "Testing Practices for Fungal Respiratory Infections and SARS-CoV-2 among Infectious Disease Specialists, United States" Journal of Fungi 7, no. 8: 605. https://doi.org/10.3390/jof7080605