
Occupational Histoplasmosis: Epidemiology and Prevention Measures

 , ,
, ,
Abstract
:1. Introduction
2. General Epidemiology
3. Histoplasma in the Environment
4. Activities, Settings, and Jobs Associated With Histoplasmosis
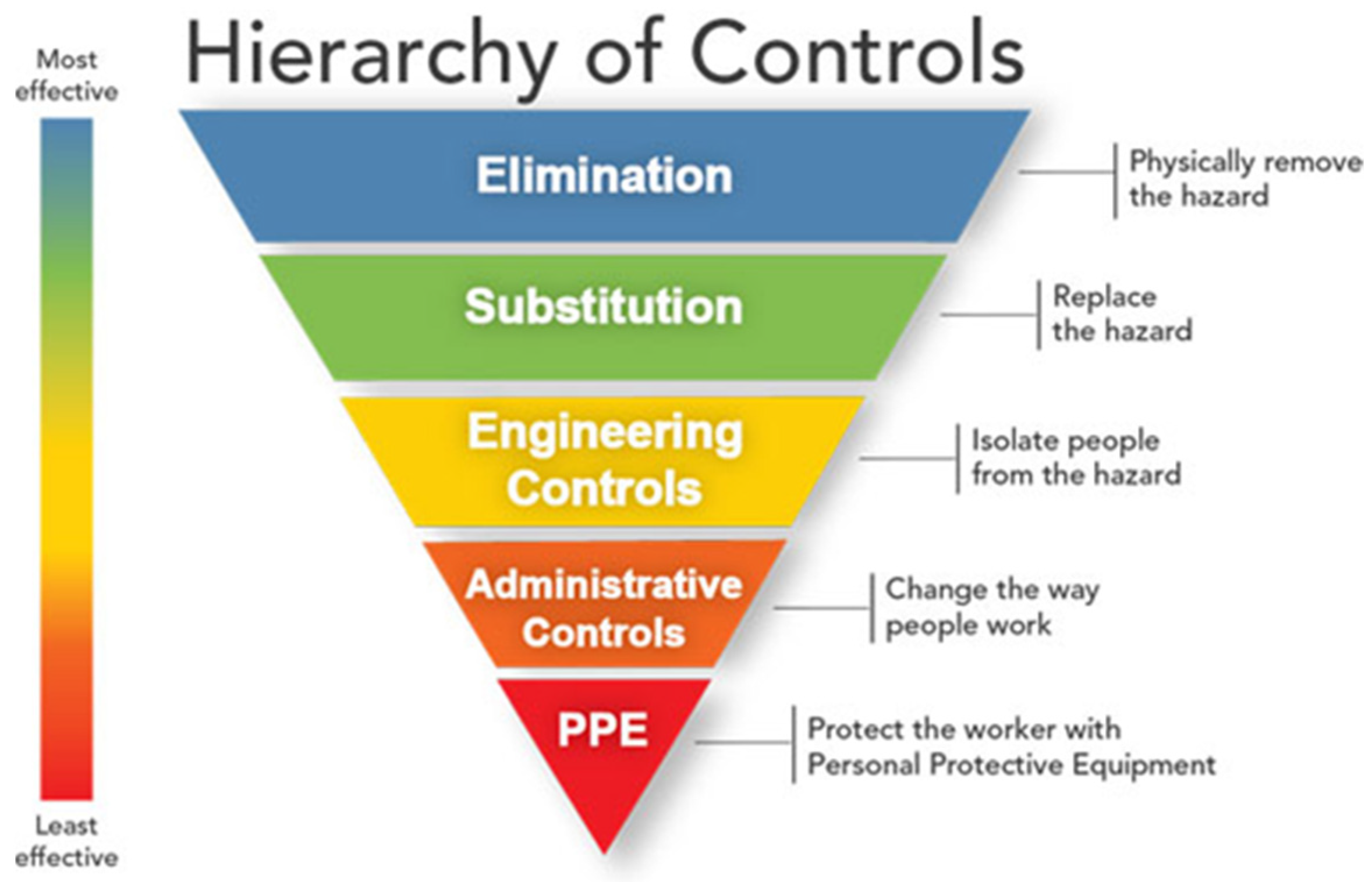
5. Preventing Histoplasma Exposures in the Workplace
5.1. Elimination/Engineering Controls
5.1.1. Excluding Bats or Birds from a Building
5.1.2. Controlling Dust Generation and Aerosolized Dust
5.1.3. Disposing of Waste
5.1.4. Disinfecting Potentially Contaminated Material
5.2. Administrative Controls
5.2.1. Posting Health Risk Warnings
5.2.2. Hazard Communication and Training
5.3. Personal Protective Equipment
- the level of risk for histoplasmosis while performing the job;
- the required assigned protection factor [73]. The assigned protection factor is the level of workplace protection that each class of respirators is expected to provide to employees when the employer implements a continuing, effective respiratory protection program;
- the advantages and disadvantages of each respirator class that provide the required assigned protection factor.
6. Laboratory-Acquired Histoplasmosis
7. Public Health Implications
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Darling, S.T. A Protozoön General Infection Producing Pseudotubercles in the Lungs and Focal Necroses in the Liver, Spleen and Lymphnodes. JAMA 1906, 46, 1283–1285. [Google Scholar] [CrossRef] [Green Version]
- Linder, K.A.; Kauffman, C.A. Current and New Perspectives in the Diagnosis of Blastomycosis and Histoplasmosis. J. Fungi 2021, 7, 12. [Google Scholar] [CrossRef]
- Rodrigues, A.M.; Beale, M.A.; Hagen, F.; Fisher, M.C.; Terra, P.P.D.; de Hoog, S.; Brilhante, R.S.N.; de Aguiar Cordeiro, R.; de Souza Collares Maia Castelo-Branco, D.; Rocha, M.F.G.; et al. The Global Epidemiology of Emerging Histoplasma species in Recent Years. Stud. Mycol. 2020, 97, 100095. [Google Scholar] [CrossRef]
- Dukik, K.; Muñoz, J.F.; Jiang, Y.; Feng, P.; Sigler, L.; Stielow, J.B.; Freeke, J.; Jamalian, A.; Gerrits van den Ende, B.; McEwen, J.G.; et al. Novel Taxa of Thermally Dimorphic Systemic Pathogens in the Ajellomycetaceae (Onygenales). Mycoses 2017, 5, 296–309. [Google Scholar] [CrossRef] [Green Version]
- Shen, Q.; Rappleye, C.A. Differentiation of the Fungus Histoplasma capsulatum into a Pathogen of Phagocytes. Curr. Opin. Microbiol. 2017, 40, 1–7. [Google Scholar] [CrossRef]
- Nielsen, G.E.; Evans, R.E. A Study of the Sporulation of Histoplasma capsulatum. J. Bacteriol. 1954, 68, 261–264. [Google Scholar] [CrossRef] [Green Version]
- Anderson, K.L.; Marcus, S. Sporulation Characteristics of Histoplasma capsulatum. Mycopathol. Mycol. Appl. 1968, 36, 179–187. [Google Scholar] [CrossRef]
- Deepe, G.S., Jr. Outbreaks of Histoplasmosis: The Spores Set Sail. PLoS Pathog. 2018, 14, e1007213. [Google Scholar] [CrossRef] [PubMed]
- Min, K.; Neiman, A.M.; Konopka, J.B. Fungal Pathogens: Shape-Shifting Invaders. Trends Microbiol. 2020, 28, 922–933. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, N.; Kubat, R.C.; Poplin, V.; Adenis, A.A.; Denning, D.W.; Wright, L.; McCotter, O.; Schwartz, I.S.; Jackson, B.R.; Chiller, T.; et al. Re-drawing the Maps for Endemic Mycoses. Mycopathologia 2020, 185, 843–865. [Google Scholar] [PubMed]
- Benedict, K.; Mody, R.K. Epidemiology of Histoplasmosis Outbreaks, United States, 1938–2013. Emerg. Infect. Dis. 2016, 22, 370–378. [Google Scholar] [CrossRef] [Green Version]
- Manos, N.E.; Ferebee, S.H.; Kerschbaum, W.F. Geographic Variation in the Prevalence of Histoplasmin Sensitivity. Dis. Chest. 1956, 29, 649–668. [Google Scholar] [CrossRef] [Green Version]
- Cano, M. The Epidemiology of Histoplasmosis: A Review. Semin. Respir. Infect. 2001, 16, 109–118. [Google Scholar] [CrossRef]
- Hage, C.A.; Knox, K.S.; Wheat, L.J. Endemic Mycoses: Overlooked Causes of Community Acquired Pneumonia. Respir. Med. 2012, 106, 769–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benedict, K.; McCracken, S.; Signs, K.; Ireland, M.; Amburgey, V.; Serrano, J.A.; Christophe, N.; Gibbons-Burgener, S.; Hallyburton, S.; Warren, K.A.; et al. Enhanced Surveillance for Histoplasmosis—9 States, 2018–2019. Open Forum Infect. Dis. 2020, 7, ofaa343. [Google Scholar] [CrossRef] [PubMed]
- McKinsey, D.S.; McKinseym, J.P. Pulmonary Histoplasmosis. Semin. Respir. Crit. Care Med. 2011, 32, 735–744. [Google Scholar] [CrossRef]
- Marukutira, T.; Huprikar, S.; Azie, N.; Quan, S.-P.; Meier-Kriesche, U.; Horn, D. Clinical Characteristics and Outcomes in 303 HIV-Infected Patients with Invasive Fungal Infections: Data from the Prospective Antifungal Therapy Alliance Registry, a Multicenter, Observational Study. HIV AIDS Res. Palliat. Care 2014, 6, 39–47. [Google Scholar]
- Cuellar-Rodriguez, J.; Avery, R.K.; Lard, M.; Budev, M.; Gordon, S.M.; Shrestha, N.K.; van Duin, D.; Oethinger, M.; Mawhorter, S.D. Histoplasmosis in Solid Organ Transplant Recipients: 10 Years of Experience at a Large Transplant Center in an Endemic Area. Clin. Infect. Dis. 2009, 49, 710–716. [Google Scholar] [CrossRef] [Green Version]
- Edwards, L.B.; Acquaviva, F.A.; Livesay, V.T.; Cross, F.W.; Palmer, C.E. An Atlas of Sensitivity to Tuberculin, PPD-B, and Histoplasmin in the United States. Am. Rev. Respir. Dis. 1969, 99 (Suppl. 1), 132. [Google Scholar]
- Palmer, C.E. Geographic Differences in Sensitivity to Histoplasmin among Student Nurses. Public Health Rep. 1946, 61, 475–487. [Google Scholar] [CrossRef]
- Benedict, K.; Thompson, G.R., 3rd; Deresinski, S.; Chiller, T. Mycotic Infections Acquired outside Areas of Known Endemicity, United States. Emerg. Infect. Dis. 2015, 21, 1935–1941. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Toda, M.; Benedict, K.; Caceres, D.H.; Litvintseva, A.P. Endemic and Other Dimorphic Mycoses in The Americas. J. Fungi 2021, 7, 151. [Google Scholar] [CrossRef] [PubMed]
- Gómez, L.F.; Torres, I.P.; Jiménez-A, M.D.P.; McEwen, J.G.; de Bedout, C.; Peláez, C.A.; Acevedo, M.; Taylor, M.L.; Arango, M. Detection of Histoplasma capsulatum in Organic Fertilizers by Hc100 Nested Polymerase Chain Reaction and Its Correlation with the Physicochemical and Microbiological Characteristics of the Samples. Am. J. Trop. Med. Hyg. 2018, 98, 1303–1312. [Google Scholar]
- Gómez Londoño, L.F.; Pérez León, L.C.; McEwen Ochoa, J.G.; Zuluaga Rodriguez, A.; Pelaez Jaramillo, C.A.; Acevedo Ruiz, J.N.; Taylor, M.L.; Arango Arteaga, M.; Jimenez Alzate, M.P. Capacity of Histoplasma capsulatum to Survive the Composting Process. Appl. Environ. Soil Sci. 2019, 2019, 5038153. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, P.A.; Jackson, B.R.; Haselow, D.; Fields, V.; Ireland, M.; Austin, C.; Signs, K.; Fialkowski, V.; Patel, R.; Ellis, P.; et al. Multistate Epidemiology of Histoplasmosis, United States, 2011–2014. Emerg. Infect. Dis. 2018, 24, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Grayston, J.T.; Furcolow, M.L. The Occurrence of Histoplasmosis in Epidemics; Epidemiological Studies. Am. J. Public Health Nations Health 1953, 43, 665–676. [Google Scholar] [CrossRef] [PubMed]
- Lehan, P.H.; Furcolow, M.L. Epidemic Histoplasmosis. J. Chronic Dis. 1957, 5, 489–503. [Google Scholar] [CrossRef]
- Idstrom, L.; Rosenberg, B. Primary Atypical Pneumonia. Bull. US Army Med. Dep. 1944, 81, 88–92. [Google Scholar]
- Cain, J.C.; Devins, E.J.; Downing, J.E. An Unusual Pulmonary Disease. Arch. Intern. Med. 1947, 79, 626–641. [Google Scholar] [CrossRef]
- Parrott, T., Jr.; Taylor, G.; Poston, M.A.; Smith, D.T. An Epidemic of Histoplasmosis in Warrenton, North Carolina. South Med. J. 1955, 48, 1147–1150. [Google Scholar] [CrossRef]
- Feldman, H.A.; Sabin, A. Pneumonitis of Unknown Etiology in a Group of Men Exposed to Pigeon Excreta. J. Clin. Investig. 1948, 27, 533. [Google Scholar]
- Englert, E., Jr.; Phillips, A.W. Acute Diffuse Pulmonary Granulomatosis in Bridge Workers. Am. J. Med. 1953, 15, 733–740. [Google Scholar] [CrossRef]
- Cullen, J.H.; Hazen, E.; Scholdager, R. Two Cases of Histoplasmosis Acquired in Felling a Decayed Tree in the Mohawk Valley. N. Y. State J. Med. 1956, 56, 3507–3510. [Google Scholar] [PubMed]
- Centers for Disease Control and Prevention. Epidemiological reports—Histoplasmosis. In Morb. Mortal. Wkly. Rep.; 30 November 1956. Available online: https://stacks.cdc.gov/view/cdc/895 (accessed on 25 June 2021).
- Centers for Disease Control and Prevention. Epidemiological reports—Histoplasmosis. In Morb. Mortal. Wkly. Rep.; 1956. Available online: https://stacks.cdc.gov/view/cdc/1365 (accessed on 25 June 2021).
- Wilcox, K.R., Jr.; Waisbren, B.A.; Martin, J. The Walworth, Wisconsin, Epidemic of Histoplasmosis. Ann. Intern. Med. 1958, 49, 388–418. [Google Scholar]
- Centers for Disease Control and Prevention. Histoplasmosis—Lexington, Kentucky. Morb. Mortal. Wkly. Rep. 1961, 10, 2–8. [Google Scholar]
- D’Alessio, D.J.; Heeren, R.H.; Hendricks, S.L.; Ogilvie, P.; Furcolow, M.L. A Starling Roost as the Source of Urban Epidemic Histoplasmosis in an Area of Low Incidence. Am. Rev. Respir. Dis. 1965, 92, 725–731. [Google Scholar] [PubMed]
- Younglove, R.M.; Terry, R.M.; Rose, N.J.; Martin, R.J.; Schnurrenberger, P.R. An Outbreak of Histoplasmosis in Illinois Associated with Starlings. Ill. Med. J. 1968, 134, 259–263. [Google Scholar]
- Chick, E.W.; Bauman, D.S.; Lapp, N.L.; Morgan, W.K. A Combined Field and Laboratory Epidemic of Histoplasmosis. Isolation from Bat Feces in West Virginia. Am. Rev. Respir. Dis. 1972, 105, 968–971. [Google Scholar]
- Centers for Disease Control and Prevention. Morb. Mortal. Wkly. Rep. 1972, 21, 231–236.
- Handzel, S.; Jessamine, A.G. Imported Histoplasmosis from Puerto Rico. Can. J. Public Health 1975, 66, 393–395. [Google Scholar]
- Dean, A.G.; Bates, J.H.; Sorrels, C.; Sorrels, T.; Germany, W.; Ajello, L.; Kaufman, L.; McGrew, C.; Fitts, A. An Outbreak of Histoplasmosis at an Arkansas Courthouse, with Five Cases of Probable Reinfection. Am. J. Epidemiol. 1978, 108, 36–46. [Google Scholar]
- Sorley, D.L.; Levin, M.L.; Warren, J.W.; Flynn, J.P.G.; Gerstenblith, J. Bat-associated Histoplasmosis in Maryland Bridge Workers. Am. J. Med. 1979, 67, 623–626. [Google Scholar] [CrossRef]
- CDC. Histoplasmosis—Northern Louisiana. MMWR Morb. Mortal. Wkly. Rep. 1977, 26, 375. [Google Scholar]
- Jones, T.F.; Swinger, G.L.; Craig, A.S.; McNeil, M.M.; Kaufman, L.; Schaffner, W. Acute Pulmonary Histoplasmosis in Bridge Workers: A Persistent Problem. Am. J. Med. 1999, 106, 480–482. [Google Scholar] [CrossRef]
- Bartlett, P.C.; Vonbehren, L.A.; Tewari, R.P.; Martin, R.J.; Eagleton, L.; Isaac, M.J.; Kulkarni, P.S. Bats in the Belfry: An Outbreak of Histoplasmosis. Am. J. Public Health 1982, 72, 1369–1372. [Google Scholar] [CrossRef] [Green Version]
- Waldman, R.J.; England, A.C.; Tauxe, R.; Kline, T.; Weeks, R.J.; Ajello, L.; Kaufman, L.; Wentworth, B.; Fraser, D.W. A Winter Outbreak of Acute Histoplasmosis in Northern Michigan. Am. J. Epidemiol. 1983, 117, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Schoenberger, C.I.; Weiner, J.H.; Mayo, F.J.; Spellman, J.; Waltersdorff, R.G. Acute Pulmonary Histoplasmosis Outbreak Following Home Renovation. Md. Med. J. 1988, 37, 457–460. [Google Scholar]
- Ramirez, J. Acute Pulmonary Histoplasmosis: Newly Recognized Hazard of Marijuana Plant Hunters. Am. J. Med. 1990, 88, 60N–62N. [Google Scholar]
- Stobierski, M.G.; James Hospedales, C.; Hall, W.N.; Robinson-Dunn, B.; Hoch, D.; Sheill, D.A. Outbreak of Histoplasmosis among Employees in a Paper Factory—Michigan, 1993. J. Clin. Microbiol. 1996, 34, 1220–1223. [Google Scholar] [CrossRef] [Green Version]
- Hajjeh, R.W.D.; Kaufman, L.; Padhye, A.; McNeil, M. An outbreak of acute histoplasmosis in a correctional center in Virginia. In Proceedings of the Program and Abstracts of the 35th Interscience Conference on Antimicrobial Agents and Chemotherapy, American Society for Microbiology, San Francisco, CA, USA, 17–20 September 1995. [Google Scholar]
- CDC. Histoplasmosis—Kentucky, 1995. MMWR Morb. Mortal. Wkly. Rep. 1995, 44, 701–703. [Google Scholar]
- Huhn, G.D.; Austin, C.; Carr, M.; Heyer, D.; Boudreau, P.; Gilbert, G.; Eimen, T.; Lindsley, M.D.; Cali, S.; Conover, C.S.; et al. Two Outbreaks of Occupationally Acquired Histoplasmosis: More than Workers at Risk. Environ. Health Perspect. 2005, 113, 585–589. [Google Scholar] [CrossRef] [Green Version]
- CDC. Outbreak of Histoplasmosis among Industrial Plant Workers—Nebraska, 2004. Morb. Mortal. Wkly. Rep. 2004, 53, 1020–1022. [Google Scholar]
- Fournier, M.; Quinlisk, P.; Garvey, A. Histoplasmosis infections associated with a demolition site—Iowa, 2008. In Proceedings of the 59th Annual Epidemic Intelligence Service Conference, Atlanta, GA, USA, 20–24 April 2008. [Google Scholar]
- Trivedi, K.; Miramontes, R.; Dufficy, D.; Park, B.; Galeazzi, C.; Sharp, K.; Soyemi, K.; Miramontes, R.; Henkels, T.; Chiller, T. Histoplasmosis outbreak related to construction at a state facility—Iowa 2008. In Proceedings of the Joint 48th Interscience Conference on Antimicrobial Agents and Chemotherapy and 46th Annual Meeting of the Infectious Diseases Society of America, Washington, DC, USA, 25–28 October 2008. [Google Scholar]
- Grant, Y.; Harlacher, V.; Austin, C. Histoplasmosis infection among temporary laborers—Illinois, August–September 2011. In Proceedings of the 61st Annual Epidemic Intelligence Service Conference, Atlanta, GA, USA, 16–20 April 2012. [Google Scholar]
- Centers for Disease Control and Prevention. Histoplasmosis Outbreak among Day Camp Attendees—Nebraska, June 2012. Morb. Mortal. Wkly. Rep. 2012, 61, 747–748. [Google Scholar]
- Arwady, M.; Vallabhaneni, S.; Tsai, V.; Smith, R.; Park, B.; Conover, C. Febrile Illness at a State Correctional Facility—Illinois, 2013; IDweek: Philadelphia, PA, USA, 2014. [Google Scholar]
- Su, C.P.; de Perio, M.A.; Cummings, K.J.; McCague, A.B.; Luckhaupt, S.E.; Sweeney, M.H. Case Investigations of Infectious Diseases Occurring in Workplaces, United States, 2006–2015. Emerg. Infect. Dis. 2019, 25, 397–405. [Google Scholar] [CrossRef]
- Armstrong, P.A.; Beard, J.D.; Bonilla, L.; Arboleda, N.; Lindsley, M.D.; Chae, S.R.; Castillo, D.; Nuñez, R.; Chiller, T.; de Perio, M.A.; et al. Outbreak of Severe Histoplasmosis among Tunnel Workers-Dominican Republic, 2015. Clin. Infect. Dis. 2018, 66, 1550–1557. [Google Scholar] [CrossRef]
- Raterman, S.M. Methods of control. In Fundamentals of Industrial Hygiene, Plog B ed.; National Safety Council: Itasca, IL, USA, 2000; pp. 585–605. [Google Scholar]
- DePerno, C.S. Animal damage control. In 2020 N.C. Agricultural Chemicals Manual; North Carolina Department of Forestry and Environmental Resources: Raleigh, NC, USA, 2020. [Google Scholar]
- Bat Conservation International, Inc. Exclusion Experts Promote Pest Control Industry Changes. Bats 1996, 14, 10–11. [Google Scholar]
- Williams, D.E.; Corrigan, R.M. Pigeons (rock doves). In Prevention and Control of Wildlife Damage; University of Nebraska–Lincoln: Lincoln, NE, USA, 1994. Available online: https://agri.nv.gov/uploadedFiles/agrinvgov/Content/Protection/Resource_Protection/Pigeon.pdf (accessed on 1 May 2021).
- Tuttle, M.D. America’s Neighborhood Bats; University of Texas Press: Austin, TX, USA, 2005. [Google Scholar]
- Morse, D.L.; Gordon, M.A.; Matte, T.; Eadie, G. An Outbreak of Histoplasmosis in a Prison. Am. J. Epidemiol. 1985, 122, 253–261. [Google Scholar] [CrossRef]
- Bartlett, P.C.; Weeks, R.J.; Ajello, L. Decontamination of Histoplasma capsulatum-infested Bird Roost in Illinois. Arch. Environ. Health 1982, 37, 221–223. [Google Scholar] [CrossRef]
- Tosh, F.E.; Weeks, R.J.; Pfeiffer, F.R.; Hendricks, S.L.; Greer, D.L.; Chin, T.D.Y. The use of formalin to kill Histoplasma capsulatum at an epidemic site. Am. J. Epidemiol. 1967, 85, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agency for Toxic Substances and Disease Registry. Toxicological Profile for Formaldehyde; U.S. Department of Health and Human Services, Public Health Service: Atlanta, GA, USA, 1999. Available online: https://www.atsdr.cdc.gov/toxprofiles/tp111.pdf (accessed on 25 June 2021).
- Occupational Safety and Health Administration. Hazard Communication Standard, 29 CFR 1910.1200. Available online: https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.1200 (accessed on 25 June 2021).
- Occupational Safety and Health Administration. Respiratory Protection Standard, 29 CFR 1910.134. Available online: https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134 (accessed on 25 June 2021).
- Deepe, G.S., Jr. Chapter 254: Histoplasma capsulatum. In Principles and Practices of Infectious Diseases, 5th ed.; Mandell, G.L., Bennett, J.E., Dolin, R., Eds.; Churchill Livingstone: Philadelphia, PA, USA, 2000; pp. 2718–2733. [Google Scholar]
- Wheat, L.J. Chapter 3: Histoplasmosis. In Fungal Diseases of the Lung, 3rd ed.; Sarosi, G.A., Davies, S.F., Eds.; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2000; pp. 31–46. [Google Scholar]
- Brousseau, L.M.; Shaffer, R. NIOSH Science Blog: Do We Need to Challenge Respirator Filters With Biological Aerosols? Available online: https://blogs.cdc.gov/niosh-science-blog/2014/04/02/respirator-filter-testing/ (accessed on 3 May 2021).
- Lenhart, S.W. Recommendations for Protecting Workers from Histoplasma capsulatum Exposure during Bat Guano Removal from a Church’s Attic. Appl. Occup. Environ. Hyg. 1994, 9, 230–236. [Google Scholar]
- USAEHA. Managing health hazards associated with bird and bat excrement. In U.S. Army Environmental Hygiene Agency Technical Guide 142; U. S. Army Environmental Hygiene Agency: Aberdeen Proving Ground, MD, USA, 1992. [Google Scholar]
- Sulkin, S.E.; Pike, R.M. Survey of Laboratory-Acquired Infections. Am. J. Public Health 1951, 41, 769–781. [Google Scholar] [CrossRef] [Green Version]
- Sewell, D.L. Laboratory-Associated Infections and Biosafety. Clin. Microbiol. Rev. 1995, 8, 389–405. [Google Scholar] [CrossRef] [PubMed]
- Spicknall, C.G.; Ryan, R.W.; Cain, A. Laboratory-Acquired Histoplasmosis. N. Engl. J. Med. 1956, 254, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Hanel, E. Laboratory-Acquired Mycoses; Department of the Army: Fort Detrick, MD, USA, 1967; Volume 28. [Google Scholar]
- Tosh, F.E.; Balhuizen, J.; Yates, J.L.; Brasher, C.A. Primary Cutaneous Histoplasmosis: Report of a Case. Arch. Intern. Med. 1964, 114, 118–119. [Google Scholar] [CrossRef] [PubMed]
- Gugnani, H.C.; Randhawa, H.S. Laboratory-Acquired Fungal Infections, A Review. Arch. Microbiol. Immunol. 2020, 4, 51–56. [Google Scholar] [CrossRef]
- De Perio, M.A.; Materna, B.L.; Sondermeyer Cooksey, G.L.; Vugia, D.J.; Su, C.P.; Luckhaupt, S.E.; McNary, J.; Wilken, J.A. Occupational Coccidioidomycosis Surveillance and Recent Outbreaks in California. Med. Mycol. 2019, 57 (Suppl. 1), S41–S45. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Occupational Safety and Health. Collecting and Using Industry and Occupation Data. Available online: https://www.cdc.gov/niosh/topics/coding/default.html (accessed on 27 May 2021).


{kind=link}
| Ref | Location | Month and Year | No. Cases | Activities and Setting | Type of Workers Affected |
|---|---|---|---|---|---|
| [26,27] | Plattsburg, New York | November 1938 | 23 | Demolition and shoveling bird droppings from the roof of a school building | Works Progress Administration workers |
| [28] | Camp Crowder, Missouri | May 1943 | 40 | Cleaning abandoned chicken coops, homes, and barns | Army members |
| [29] | Camp Gruber, Oklahoma | March 1944 | 27 | Entering an abandoned storm cellar and chopping wood | Army members |
| [30] | Warrenton, North Carolina | May 1947 | 7 | Church renovation | Carpenters and a contractor |
| [31] | Cincinnati, Ohio | July 1947 | 12 | Exposure to bird droppings at an abandoned water tower | Not specified |
| [32] | Anne Arundel County or Calvert County, Maryland | August 1951 | 2 | Scraping bird/bat droppings off bridges | Bridge workers |
| [26] | Mandan, North Dakota | February 1952 | 4 | Demolishing a school building and removing bird droppings | Railroad workers |
| [33] | Johnstown, New York | November 1954 | 2 | Cutting down a decayed tree | Lumberjacks |
| [34] | North Carolina | 1956 | 2 | House renovation | Not specified |
| [35] | Southwestern Minnesota | 1956 | 5 | Church renovation | Workers who cleaned and installed new window wells |
| [36] | Walworth, Wisconsin | August 1956 | 19 | Excavation for water and sewer lines while constructing a new house | Construction workers |
| [37] | Lexington, Kentucky | October 1960 | 7 | Removing bird droppings at a water tower | Not specified |
| [38] | Mason City, Iowa | August–September 1962 | 28 | Clearing trees and bushes at a bird roosting site | Workers who cleared vegetation |
| [39] | Northwest Illinois | June 1967 | 12 | House renovation | Construction workers |
| [40] | Jane Lew, West Virginia | March 1968 | 4 | Building renovation and digging for gas lines | Maintenance crew, investigators, and laboratory workers |
| [41] | Jacksonville, Texas | March 1971 | 2 | Bulldozing a blackbird roost | City workers |
| [42] | Aquas Buenas Caves, Puerto Rico | May 1973 | 4 | Digging for fossils in a cave | Students and teachers |
| [43] | Hot Springs, Arkansas | July 1975 | 68 | Clearing bird droppings from courthouse roof | Construction workers and office workers |
| [44] | Southern Maryland | November 1977 | 13 | Scraping bat droppings from a bridge | Bridge workers and epidemiologists |
| [45] | Bossier Parish, Louisiana | September 1977 | 6 | Clearing bamboo from a bird roosting site | Temporary laborers |
| [46] | Tennessee | September 1977 | 2 | Cleaning bat droppings from a bridge | Bridge workers |
| [47] | Pittsfield, Illinois | April 1980 | 29 | Disruption of bat droppings during renovation of a school building | Heating/ventilation worker and school employees |
| [48] | Rogers City, Michigan | January 1980 | 138 | Exposure to a pulley stored in a bird nesting area | Limestone quarry workers |
| [49] | Rockville, Maryland | January 1987 | 13 | Renovation of a bat-infested house | Construction workers |
| [50] | Lares, Puerto Rico | September 1987 | 4 | Uprooting marijuana plants | Police officers |
| [51] | Muskegon County, Michigan | October 1993 | 44 | Sweeping bird droppings from roof at a pulp paper factory | Factory workers |
| [52] | 30 miles west of Richmond, Virginia | June 1994 | 72 | Moving a pile of dirt and debris | Prison employees and inmates |
| [53] | Eastern Kentucky | June 1995 | 19 | Disruption of bat guano during demolition of abandoned building | Demolition workers |
| [54] | Macon County, Illinois | May 2001 | 6 | Moving soil and clearing trees at a landfill | Landfill workers |
| [54] | Iroquois County, Illinois | August 2003 | 5 | Bridge repair | Bridge workers |
| [55] | Blair, Nebraska | January 2004 | 108 | Removal of contaminated soil excavated during a previous histoplasmosis outbreak | Agricultural processing plant workers |
| [56] | Des Moines, Iowa | November 2007 | 55 | Construction and renovation at a state facility building | Construction workers and office workers |
| [57] | Iowa | October 2008 | 23 | Demolishing a bat-infested attic | Construction workers |
| [58] | McLean County, Illinois | August–September 2011 | 8 | Disrupting bat droppings during building restoration | Temporary laborers |
| [59] | Douglas County, Nebraska | June 2012 | 36 | Cleaning bat droppings from a campsite | Camp counselors |
| [60] | Danville, Illinois | August 2013 | 85 | Removal of trees where birds roosted | Prison employees and inmates |
| Hierarchy of Controls | Prevention Measure |
|---|---|
| Elimination | Excluding bats or birds from a building |
| Engineering controls | Controlling dust generation and aerosolized dust Disposing of waste |
| Administrative controls | Developing site safety plan Posting health risk warnings Hazard communication and training |
| Personal protective equipment (PPE) | NIOSH-approved respirators Other PPE: eye protection, gloves, protective clothing, shoe/boot coverings |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Perio, M.A.; Benedict, K.; Williams, S.L.; Niemeier-Walsh, C.; Green, B.J.; Coffey, C.; Di Giuseppe, M.; Toda, M.; Park, J.-H.; Bailey, R.L.; et al. Occupational Histoplasmosis: Epidemiology and Prevention Measures. J. Fungi 2021, 7, 510. https://doi.org/10.3390/jof7070510
de Perio MA, Benedict K, Williams SL, Niemeier-Walsh C, Green BJ, Coffey C, Di Giuseppe M, Toda M, Park J-H, Bailey RL, et al. Occupational Histoplasmosis: Epidemiology and Prevention Measures. Journal of Fungi. 2021; 7(7):510. https://doi.org/10.3390/jof7070510
Chicago/Turabian Stylede Perio, Marie A., Kaitlin Benedict, Samantha L. Williams, Christine Niemeier-Walsh, Brett J. Green, Christopher Coffey, Michelangelo Di Giuseppe, Mitsuru Toda, Ju-Hyeong Park, Rachel L. Bailey, and et al. 2021. "Occupational Histoplasmosis: Epidemiology and Prevention Measures" Journal of Fungi 7, no. 7: 510. https://doi.org/10.3390/jof7070510