Investigation of Basophil Activation Test for Diagnosing Milk and Egg Allergy in Younger Children

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Specific IgE Measurement
2.3. The Basophil Activation Test
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Diagnostic Performance of the BAT and sIgE
3.3. Diagnostic Performance of the BAT and sIgE for Patients with AD
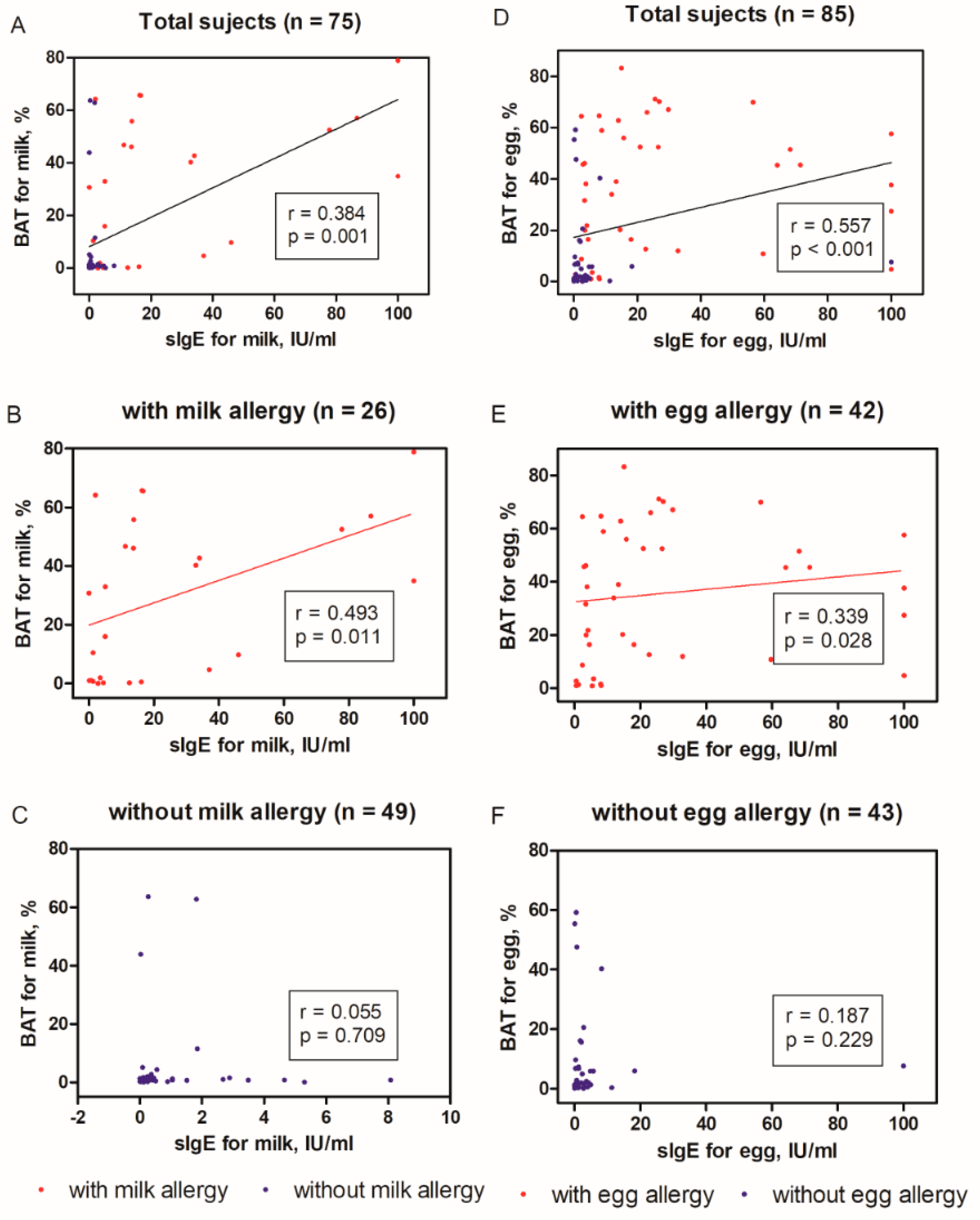
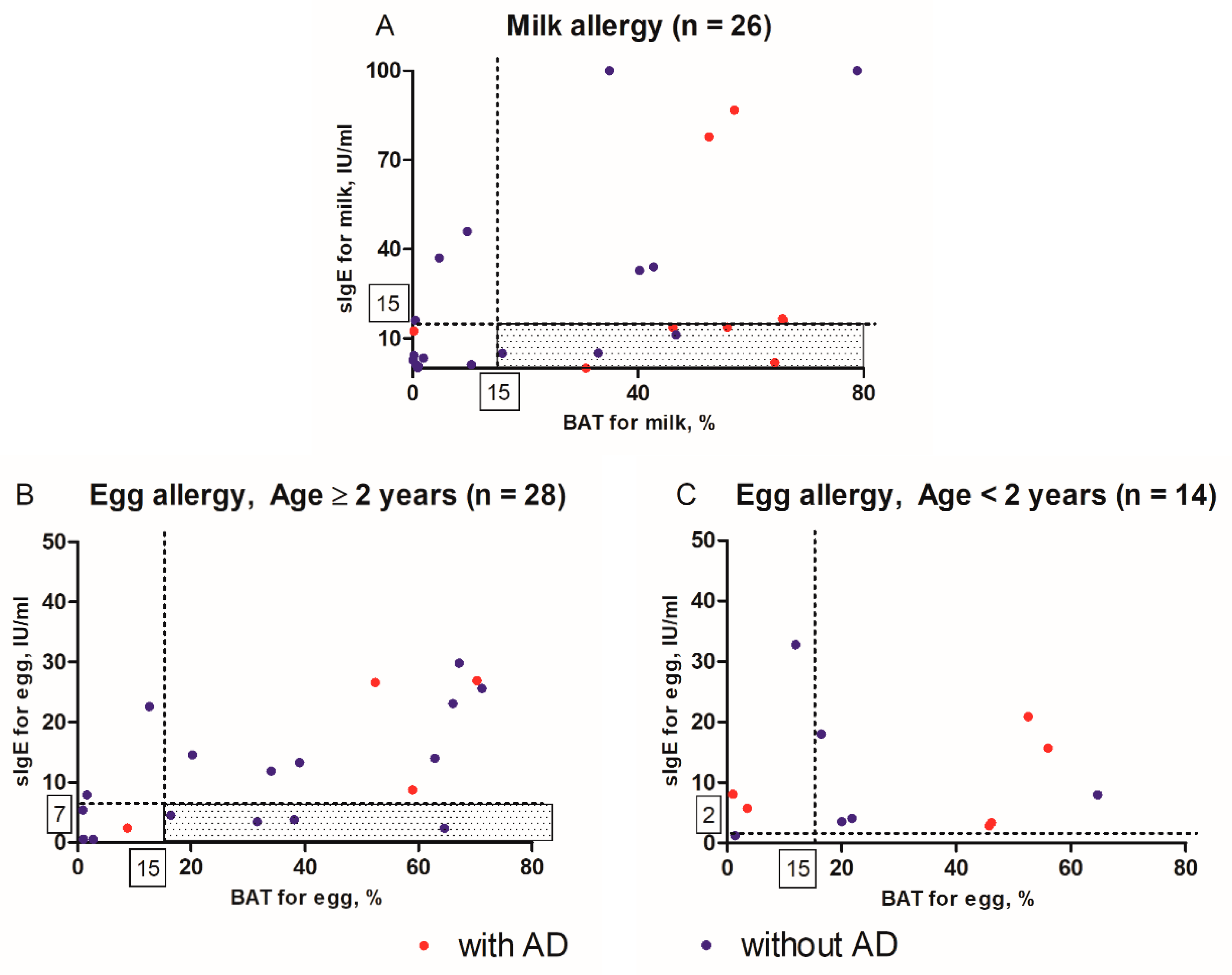
3.4. Distributions of sIgE Levels and Percentages of basophils with the expression of CD63
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cox, A.L.; Nowak-Wegrzyn, A. Innovation in food challenge tests for food allergy. Curr. Allergy Asthma Rep. 2018, 18, 74. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Cox, A.; Nowak-Węgrzyn, A.; Wang, J. Diagnosis of food allergy. Immunol. Allergy Clin. N. Am. 2018, 38, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Sicherer, S.H.; Sampson, H.A. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J. Allergy Clin. Immunol. 2018, 141, 41–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cartledge, N.; Chan, S. Atopic dermatitis and food allergy: A paediatric approach. Curr. Pediatr. Rev. 2018, 14, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Graham, F.; Eigenmann, P.A. Atopic dermatitis and its relation to food allergy. Curr. Opin. Allergy Clin. Immunol. 2020. [Google Scholar] [CrossRef]
- Broeks, S.A.; Brand, P.L. Atopic dermatitis is associated with a fivefold increased risk of polysensitisation in children. Acta Paediatr 2017, 106, 485–488. [Google Scholar] [CrossRef]
- Sampson, H.A.; Mendelson, L.; Rosen, J.P. Fatal and near-fatal anaphylactic reactions to food in children and adolescents. N. Engl. J. Med. 1992, 327, 380–384. [Google Scholar] [CrossRef]
- Commins, S.P.; James, H.R.; Stevens, W.; Pochan, S.L.; Land, M.H.; King, C. Delayed clinical and ex vivo response to mammalian meat in patients with IgE to galactose-alpha-1,3-galactose. J. Allergy Clin. Immunol. 2014, 134, 108–115.e11. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, H.J.; Santos, A.F.; Mayorga, C.; Nopp, A.; Eberlein, B.; Ferrer, M.; Rouzaire, P.; Ebo, D.G.; Sabato, V.; Sanz, M.L.; et al. The clinical utility of basophil activation testing in diagnosis and monitoring of allergic disease. Allergy 2015, 70, 1393–1405. [Google Scholar] [CrossRef]
- Ebo, D.G.; Bridts, C.H.; Mertens, C.H.; Hagendorens, M.M.; Stevens, W.J.; De Clerck, L.S. Analyzing histamine release by flow cytometry (HistaFlow): A novel instrument to study the degranulation patterns of basophils. J. Immunol. Methods 2012, 375, 30–38. [Google Scholar] [CrossRef]
- Ruinemans-Koerts, J.; Schmidt-Hieltjes, Y.; Jansen, A.; Savelkoul, H.F.J.; Plaisier, A.; van Setten, P. The basophil activation test reduces the need for a food challenge test in children suspected of ige-mediated cow’s milk allergy. Clin. Exp. Allergy 2019, 49, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Ocmant, A.; Mulier, S.; Hanssens, L.; Goldman, M.; Casimir, G.; Mascart, F.; Schandene, L. Basophil activation tests for the diagnosis of food allergy in children. Clin. Exp. Allergy 2009, 39, 1234–1245. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Tachimoto, H.; Shukuya, A.; Kurosaka, N.; Yanagida, N.; Utsunomiya, T.; Iguchi, M.; Komata, T.; Imai, T.; Tomikawa, M.; et al. Basophil activation marker cd203c is useful in the diagnosis of hen’s egg and cow’s milk allergies in children. Int. Arch. Allergy Immunol. 2010, 152, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Yanagida, N.; Ebisawa, M. How to diagnose food allergy. Curr. Opin. Allergy Clin. Immunol. 2018, 18, 214–221. [Google Scholar] [CrossRef]
- Santos, A.F.; Shreffler, W.G. Road map for the clinical application of the basophil activation test in food allergy. Clin. Exp. Allergy 2017, 47, 1115–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savage, J.; Johns, C.B. Food allergy: Epidemiology and natural history. Immunol. Allergy Clin. N. Am. 2015, 35, 45–59. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.Y.; Ahn, K.; Kim, J.; Jang, G.C.; Min, T.K.; Yang, H.J.; Pyun, B.Y.; Kwon, J.W.; Sohn, M.H.; Kim, K.W.; et al. A multicenter retrospective case study of anaphylaxis triggers by age in korean children. Allergy Asthma Immunol. Res. 2016, 8, 535–540. [Google Scholar] [CrossRef] [Green Version]
- Scala, G.; Miceli Sopo, S. When are serum specific ige levels positive? J. Allergy Clin. Immunol. 2015, 135, 291–292. [Google Scholar] [CrossRef]
- Nowak-Wegrzyn, A.; Katz, Y.; Mehr, S.S.; Koletzko, S. Non-ige-mediated gastrointestinal food allergy. J. Allergy Clin. Immunol. 2015, 135, 1114–1124. [Google Scholar] [CrossRef]
- Simons, F.E.; Ardusso, L.R.; Bilo, M.B.; El-Gamal, Y.M.; Ledford, D.K.; Ring, J.; Sanchez-Borges, M.; Senna, G.E.; Sheikh, A.; Thong, B.Y. World allergy organization anaphylaxis guidelines: Summary. J. Allergy Clin. Immunol. 2011, 127, 587–593. [Google Scholar] [CrossRef]
- Burks, A.W.; Holgate, S.T.; O’Hehir, R.E.; Bacharier, L.B.; Broide, D.H.; Hershey, G.K.K.; Peebles, R.S., Jr. Middleton’s Allergy e-Book: Principles and Practice; Elsevier Health Sciences: Amsterdam, The Netherlands, 2019. [Google Scholar]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Mousan, G.; Kamat, D. Cow’s milk protein allergy. Clin. Pediatr. (Phila.) 2016, 55, 1054–1063. [Google Scholar] [CrossRef] [PubMed]
- Greiwe, J. Oral food challenges in infants and toddlers. Immunol. Allergy Clin. N. Am. 2019, 39, 481–493. [Google Scholar] [CrossRef]
- Agyemang, A.; Nowak-Wegrzyn, A. Food protein-induced enterocolitis syndrome: A comprehensive review. Clin. Rev. Allergy Immunol. 2019, 57, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Luyt, D.; Ball, H.; Makwana, N.; Green, M.R.; Bravin, K.; Nasser, S.M.; Clark, A.T. Bsaci guideline for the diagnosis and management of cow’s milk allergy. Clin. Exp. Allergy 2014, 44, 642–672. [Google Scholar] [CrossRef] [PubMed]
- Du Toit, G.; Santos, A.; Roberts, G.; Fox, A.T.; Smith, P.; Lack, G. The diagnosis of ige-mediated food allergy in childhood. Pediatr Allergy Immunol. 2009, 20, 309–319. [Google Scholar] [CrossRef]
- Nguyen, T.A.; Leonard, S.A.; Eichenfield, L.F. An update on pediatric atopic dermatitis and food allergies. J. Pediatr. 2015, 167, 752–756. [Google Scholar] [CrossRef]
- Hemmings, O.; Kwok, M.; McKendry, R.; Santos, A.F. Basophil activation test: Old and new applications in allergy. Curr. Allergy Asthma Rep. 2018, 18, 77. [Google Scholar] [CrossRef] [Green Version]
- Sampson, H.A.; Broadbent, K.R.; Bernhisel-Broadbent, J. Spontaneous release of histamine from basophils and histamine-releasing factor in patients with atopic dermatitis and food hypersensitivity. N. Engl. J. Med. 1989, 321, 228–232. [Google Scholar] [CrossRef]
- Ford, L.S.; Bloom, K.A.; Nowak-Wegrzyn, A.H.; Shreffler, W.G.; Masilamani, M.; Sampson, H.A. Basophil reactivity, wheal size, and immunoglobulin levels distinguish degrees of cow’s milk tolerance. J. Allergy Clin. Immunol. 2013, 131, 180–186. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Wang, J.; Leung, N.; Wang, L.X.; Lisann, L.; Sicherer, S.H.; Scurlock, A.M.; Pesek, R.; Perry, T.T.; Jones, S.M.; et al. Correlations between basophil activation, allergen-specific ige with outcome and severity of oral food challenges. Ann. Allergy Asthma Immunol. 2015, 114, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.K.; Hourihane, J.O.; Lieberman, P. Risk multipliers for severe food anaphylaxis. World Allergy Organ. J. 2015, 8, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flow CAST®: Basophil Activation Test, Flow Cytometry [Internet] Schönenbuch, Switzerland: BUHLMANN LABORATORIES AG. Available online: https://www.buhlmannlabs.ch/products-solutions/cellular-allergy/flow-cast/ (accessed on 17 August 2012).
- Depince-Berger, A.E.; Sidi-Yahya, K.; Jeraiby, M.; Lambert, C. Basophil activation test: Implementation and standardization between systems and between instruments. Cytometry A 2017, 91, 261–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Amici, M.; Barocci, F.; Caimmi, S.; Nespoli, L.; Licari, A.; Giuliani, G.; Marseglia, G. Clinical use of basophil activation test in drug, food and hymenoptera venom allergies. Minerva Pediatr. 2019, 71, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Greenhawt, M.; Weiss, C.; Conte, M.L.; Doucet, M.; Engler, A.; Camargo, C.A., Jr. Racial and ethnic disparity in food allergy in the United States: A systematic review. J. Allergy Clin. Immunol. Pract. 2013, 1, 378–386. [Google Scholar] [CrossRef]
- Sampson, H.A. Utility of food-specific IgE concentrations in predicting symptomatic food allergy. J. Allergy Clin. Immunol. 2001, 107, 891–896. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Tested for Milk Allergy (n = 75) | Tested for Egg Allergy (n = 85) | |||
|---|---|---|---|---|
| Children with Milk Allergy (n = 26) | Children without Milk Allergy (n = 49) | Children with Egg Allergy (n = 42) | Children without Egg Allergy (n = 43) | |
| Age, year | 3.0 (2.0–5.2) * | 1.6 (0.9–2.8) | 2.6 (1.4–5.3) † | 1.8 (0.9–2.5) |
| Male, n (%) | 15 (57.7) | 30 (61.2) | 28 (66.7) | 23 (53.5) |
| Total IgE, kU/L | 557 (277–1210) * | 90 (37–280) | 296 (81–907) † | 99 (33–322) |
| Specific IgE for milk or egg, kU/L | 13.10 (2.61–34.85) * | 0.19 (0.09–0.72) | 14.30 (4.01–30.55) † | 1.09 (0.27–3.20) |
| CD63+ basophils for milk or egg, % | 31.8 (1.0–53.3) * | 1.0 (0.5–1.5) | 37.9 (11.7–57.9) † | 1.9 (0.8–6.8) |
| Anaphylaxis, n (%) | 5 (19.2) * | 0 (0) | 6 (14.3) † | 0 (0) |
| Atopic dermatitis, n (%) | 9 (34.6) | 24 (49.0) | 15 (35.7) | 20 (46.5) |
| Family history of allergy, n (%) | 7 (26.9) | 18 (36.7) | 15 (35.7) | 14 (32.6) |
| Other suspected allergic foods ‡ | ||||
| Nuts, n (%) | 6 (23.1) | 7 (14.3) | 5 (11.9) | 5 (11.6) |
| Soybean, n (%) | 1 (3.8) | 2 (4.1) | 1 (2.4) | 2 (4.7) |
| Wheat, n (%) | 4 (15.4) | 4 (8.2) | 6 (14.3) | 3 (7.0) |
| Fruits and vegetables, n (%) | 2 (7.7) | 14 (28.6) | 10 (23.8) | 7 (16.3) |
| Fish, n (%) | 2 (7.7) | 4 (8.2) | 4 (9.5) | 3 (7.0) |
| Crustaceans, n (%) | 1 (3.8) | 4 (8.2) | 2 (4.8) | 3 (7.0) |
| Tested for Milk Allergy (n = 75) | Tested for Egg Allergy (n = 85) | |||
|---|---|---|---|---|
| All (n = 75) | with AD (n = 33) | All (n = 85) | with AD (n = 35) | |
| Age, year | 2.1 (1.1–4.6) | 1.6 (0.8–4.4) | 2.1 (1.1–3.6) | 1.6 (0.8–2.6) |
| Male, n (%) | 45 (60.0) | 19 (57.6) | 51 (60.0) | 21 (60.0) |
| Total IgE, kU/L | 156 (48–655) | 113 (52–706) | 155 (52–604) | 99 (44–557) |
| Anaphylaxis, n (%) | 5 (6.7) | 3 (9.1) | 6 (7.1) | 1 (2.9) |
| Family history of allergy, n (%) | 25 (33.3) | 8 (24.2) | 29 (34.1) | 10 (28.6) |
| Milk or egg allergy, n (%) | 26 (34.7) | 9 (27.3) | 42 (49.4) | 15 (42.9) |
| Specific IgE for milk or egg in milk or egg allergy, kU/L | 13.1 (2.6–34.9) | 13.8 (7.2–47.3) | 14.3 (4.0–30.6) | 15.7 (5.8–64.1) |
| CD63+ basophils for milk or egg in milk or egg allergy, % | 31.8 (0.1–53.3) | 55.8 (38.4–64.9) | 37.9 (11.7–57.9) | 51.5 (45.4–57.6) |
| Diagnosis | Diagnostic Tool | AUC (95% CI) | Comparison of AUCs between (p-Value) | |||
|---|---|---|---|---|---|---|
| sIgE vs. BAT | BAT vs. Combined | sIgE vs. Combined | ||||
| Tested for milk allergy (n = 75) | Milk allergy (n = 26) | sIgE | 0.701 (0.602–0.800) | 0.373 | 0.157 | 0.029 * |
| BAT | 0.758 (0.655–0.860) | |||||
| Combined sIgE and BAT | 0.805 (0.707–0.904) | |||||
| Anaphylaxis (n = 5) | sIgE | 0.790 (0.651–0.929) | 0.949 | 0.784 | 0.991 | |
| BAT | 0.797 (0.532–1.000) | |||||
| Combined sIgE and BAT | 0.791 (0.509–1.000) | |||||
| Tested for egg allergy (n = 85) | Egg allergy (n = 42) | sIgE | 0.777 (0.687–0.866) | 0.989 | 0.830 | 0.781 |
| BAT | 0.776 (0.687–0.865) | |||||
| Combined sIgE and BAT | 0.766 (0.681–0.852) | |||||
| Anaphylaxis (n = 6) | sIgE | 0.624 (0.476–0.772) | 0.661 | 0.867 | 0.705 | |
| BAT | 0.577 (0.367–0.787) | |||||
| Combined sIgE and BAT | 0.561 (0.304–0.818) | |||||
| Diagnosis | Diagnostic Tool | AUC (95% CI) | Comparison of AUCs between (p-Value) | |||
|---|---|---|---|---|---|---|
| sIgE vs. BAT | BAT vs. Combined | sIgE vs. Combined | ||||
| Tested for milk allergy (n = 33) | Milk allergy (n = 9) | sIgE | 0.701 (0.524–0.878) | 0.017 * | 0.317 | 0.026 * |
| BAT | 0.924 (0.807–1.000) | |||||
| Combined sIgE and BAT | 0.903 (0.780–1.000) | |||||
| Tested for egg allergy (n = 35) | Egg allergy (n = 15) | sIgE | 0.850 (0.747–0.953) | 0.768 | 0.712 | 0.146 |
| BAT | 0.825 (0.693–0.957) | |||||
| Combined sIgE and BAT | 0.800 (0.690–0.910) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.H.; Kim, Y.S.; Park, Y.; Kim, S.Y.; Kim, K.W.; Kim, H.S.; Sohn, M.H. Investigation of Basophil Activation Test for Diagnosing Milk and Egg Allergy in Younger Children. J. Clin. Med. 2020, 9, 3942. https://doi.org/10.3390/jcm9123942
Kim YH, Kim YS, Park Y, Kim SY, Kim KW, Kim HS, Sohn MH. Investigation of Basophil Activation Test for Diagnosing Milk and Egg Allergy in Younger Children. Journal of Clinical Medicine. 2020; 9(12):3942. https://doi.org/10.3390/jcm9123942
Chicago/Turabian StyleKim, Yoon Hee, Young Suh Kim, Younhee Park, Soo Yeon Kim, Kyung Won Kim, Hyon Suk Kim, and Myung Hyun Sohn. 2020. "Investigation of Basophil Activation Test for Diagnosing Milk and Egg Allergy in Younger Children" Journal of Clinical Medicine 9, no. 12: 3942. https://doi.org/10.3390/jcm9123942