Hyponatremia in Patients with Hematologic Diseases



1
Department of Hematology, Faculty of Medicine, University of Ioannina, Stavros Niarchos Avenue, GR-45110 Ioannina, Greece
2
Department of Internal Medicine, Faculty of Medicine, University of Ioannina, Ioannina, Stavros Niarchos Avenue, GR-45110 Ioannina, Greece
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2020, 9(11), 3721; https://doi.org/10.3390/jcm9113721
Submission received: 24 October 2020
/
Revised: 10 November 2020
/
Accepted: 17 November 2020
/
Published: 19 November 2020
(This article belongs to the Special Issue Hyponatremia: Challenges and Solutions)
Abstract
:Hyponatremia is the most common electrolyte disorder in clinical practice and is associated with increased morbidity and mortality. It is frequently encountered in hematologic patients with either benign or malignant diseases. Several underlying mechanisms, such as hypovolemia, infections, toxins, renal, endocrine, cardiac, and liver disorders, as well as the use of certain drugs appear to be involved in the development or the persistence of hyponatremia. This review describes the pathophysiology of hyponatremia and discusses thoroughly the contributing factors and mechanisms that may be encountered specifically in patients with hematologic disorders. The involvement of the syndrome of inappropriate antidiuretic hormone (SIADH) secretion and renal salt wasting syndrome (RSWS) in the development of hyponatremia in such patients, as well as their differential diagnosis and management, are also presented. Furthermore, the distinction between true hyponatremia and pseudohyponatremia is explained. Finally, a practical algorithm for the evaluation of hyponatremia in hematologic patients, as well as the principles of hyponatremia management, are included in this review.
1. Introduction
Hyponatremia, usually defined as serum sodium concentration < 135 mEq/L, is the most common electrolyte abnormality encountered both in hospitalized patients and in the general population and is associated with increased morbidity and mortality [1,2]. The rapidity and the degree of reduction in serum sodium concentration are the main determinants of the symptoms associated with this electrolyte disorder. In the setting of acute (<48 h) or severe (serum sodium levels < 120 mEq/L) hyponatremia, patients’ symptoms may range from non-specific nausea, vomiting, and headache to life-threatening stupor, coma, seizures, respiratory depression, and death. Chronic moderate (serum sodium levels 120–129 mEq/L) and mild (serum sodium levels 130–134 mEq/L) hyponatremia are usually asymptomatic and have no remarkable findings on a conventional clinical examination. However, individuals with such sodium levels may develop subtle manifestations, e.g., fatigue, cognitive impairment, disorientation and gait disorders, as well as falls, osteoporosis, and fractures [3,4]. The incidence of hyponatremia varies extensively in different studies mainly depending on the definition of hyponatremia and the patient population. Thus, an incidence of 7.2% has been reported in the general population, while it may reach up to 42.6% in hospitalized patients [5].
Hyponatremia may be encountered in several hematological diseases, both benign and malignant [6,7]. In a study including hospitalized children treated for acute lymphoblastic leukemia (ALL), the incidence of hyponatremia (serum sodium levels < 130 mmol/L) on at least 2 out of 3 consecutive days was 11.9% [8]. Moreover, hyponatremia was significantly related both to neurologic complications and the existence of obvious central nervous system leukemia at diagnosis [8]. In another single center analysis of 140 pediatric patients, hyponatremia was observed in 40% of patients following hematopoietic stem cell transplantation (HSCT) [9]. A large retrospective cohort analysis of patients diagnosed with particular cancer types showed that, in patients with lymphoma, the incidence rate of euvolemic and hypervolemic hyponatremia was 395 per 1000 person-years [10]. Of note, one recent experimental study illustrated that low extracellular sodium concentration may promote carcinogenesis in vitro by upregulating molecular pathways involved in oxidative stress, proliferation, and invasion [11].
The importance of recognizing, evaluating, and treating hyponatremia in hematologic patients lies in the fact that it is an independent predictor of unfavorable outcomes both in patients with neoplastic and benign disorders, including lymphomas, sickle cell anemia, hemolytic uremic syndrome, and allogeneic hematopoietic SCT (AlloSCT) [7,10,12,13]. In addition, symptoms of hyponatremia such as fatigue, disorientation, or even falls can be mistakenly attributed to other causes, such as neutropenic sepsis or central nervous system (CNS) involvement in the context of the underlying hematological disease. This review discusses the causes as well as the clinical and pathophysiological aspects of hyponatremia in the spectrum of hematological disorders. The proper treatment of hyponatremia is also presented.
2. Pathophysiology
The two main pathophysiological mechanisms of hyponatremia include either loss of effective solutes (sodium plus potassium) in excess of water or (more often) water retention. Given that the ability for water excretion is sufficient in normal states, retention of water resulting in reduced serum sodium concentration occurs only in the presence of impaired renal excretion of water. Primary polydipsia represents an exception to this rule, in which the disproportionate water intake can overwhelm the normal excretory capacity (acute water intoxication) [14,15].
High serum levels of arginine vasopressin (also known as antidiuretic hormone (ADH)) should be considered as a prerequisite for the development and maintenance of hyponatremia in view of the fundamental role of the suppression of ADH secretion for the renal excretion of any water load. Thus, irrespective of the presence of hypotonicity, almost all causes of hyponatremia (except for low dietary solute intake, renal failure, primary polydipsia, or beer potomania syndrome) are accompanied by increased ADH, mainly due to the syndrome of inappropriate ADH secretion (SIADH) or to effective circulating volume depletion. In fact, a 15% decrease in effective arterial blood volume due to true hypovolemia (e.g., vomiting, diarrhea, osmotic diuresis) or edematous states (e.g., congestive heart failure, nephrotic syndrome, hepatic cirrhosis with ascites) causes a reduction in stretch at the carotid and renal baroreceptors, subsequently increasing ADH excretion and overriding the inhibitory effect of hypotonicity. This emphasizes the greater importance of mechanisms aiming at the maintenance of adequate circulating volume at the expense of osmotic dysregulation and hyponatremia [16].
The volume of ingested water and daily solute intake also play an important role in the development of hyponatremia. Although the kidneys have a great ability to excrete large amounts of water, this is not unlimited even in the case of intact diluting capacity. The daily urine volume (UV) is calculated by the following equation: UV = USL/Uosm, where USL is the urine solute load (in mOsm/day) and Uosm is the urine osmolarity. A normal Western diet provides 600–900 mOsm of solute daily, derived mainly from urea (the metabolic product of proteins) and electrolytes (sodium, potassium, and accompanying anions), which generates an equivalent USL. Thus, at a lowest achievable Uosm (50 mOsm), 18 L of urine will be excreted if solute intake is 900 mOsm/d. On the contrary, only 2 L of urine can be excreted if the intake of solutes is reduced to as low as 100 mOsm/d, an amount not infrequently observed in malnourished patients (tea and toast diet). As a result, if these patients consume more than 2 L of fluids, hyponatremia will ensue [17,18].
3. Causes of Hyponatremia in Hematologic Patients
3.1. Pseudohyponatremia
The first step when evaluating hyponatremia is to exclude the possibility of pseudohyponatremia; this may result from marked hyperlipidemia or hyperproteinemia (the causes of hyperlipidemia or hyperproteinemia in patients with hematologic diseases are shown in Table 1 and discussed below)—conditions that reduce the water content of a given volume of serum. Hence, sodium concentration measured per liter of serum is artifactually decreased (pseudohyponatremia), while sodium concentration in the water phase and serum osmolality are not affected. Electrolytes can be measured via direct or indirect ion-selective electrodes (ISE). Only indirect ISE is related to spurious hyponatremia, as it requires a dilution step [19]. Therefore, the obstacle of pseudohyponatremia may be avoided with direct ISE.
Hypocholesterolemia is the most common lipid abnormality in patients with cancer, including hematologic malignancies [20]. However, hyperlipidemia may also occur. A case of type III hyperlipoproteinemia with xanthomas has been reported in a patient with multiple myeloma (MM) [21]. Furthermore, severe secondary hypercholesterolemia due to cholestasis in a patient who had obstructive jaundice as the initial presentation of non-Hodgkin’s lymphoma (NHL) has been reported [22]. L-asparaginase, an essential agent in treating ALL, induces hypertriglyceridemia, which may be further intensified by the co-administration of steroids [23,24]. Furthermore, all trans retinoic acid (ATRA) used to treat acute promyelocytic leukemia appears to cause dose-dependent hypertriglyceridemia [25]. AlloSCT may also lead to hypercholesterolemia either due to decreased activity of hepatic triglyceride lipase or due to cholestasis induced by chronic graft versus host disease (GvHD) [26,27]. Furthermore, hypertriglyceridemia occurs with hemophagocytic lymphohistiocytosis (HLH) and, in fact, represents one of its diagnostic criteria [28,29].
Importantly, several conditions encountered in hematologic patients are accompanied by nephrotic syndrome and, thus, are probable causes of spurious hyponatremia in the context of hyperlipidemia (Table 1). The main underlying mechanisms of nephrotic syndrome-related hyperlipidemia are the increased hepatic biosynthesis as well as the decreased clearance of cholesterol and major lipoproteins, triggered by the decrease in oncotic pressure due to loss of proteins in urine [30,31,32,33].
Hepatitis B and C viruses (HBV and HCV) are common infections in patients with hemoglobinopathies, such as thalassemias, due to repetitive transfusions [34,35]. These infections have been associated with nephrotic-syndrome- or cholestasis-related hyperlipidemia as well as hypergammaglobulinemia due to chronic liver disease; thus, pseudohyponatremia may occur [36,37]. Monoclonal gammopathy and intravenous immunoglobulin (IVIG) administration have also been associated with spurious hyponatremia [38,39]. In the former, pseudohyponatremia may occur in the setting of severe hyperproteinemia (usually greater than 10 g/dL), given that a 1 g/dL increase in serum protein concentration decreases serum sodium concentration by approximately 0.7 mEq/L [40]. In the latter, both pseudohyponatremia and true hyponatremia may be observed (see below).
It should be emphasized that normal serum sodium levels in the context of hyperproteinemia or hyperlipidemia should raise the suspicion of hypernatremia (pseudonormonatremia). Moreover, in hypoalbuminemic states (e.g., nephrotic syndrome), indirect ISE may overestimate serum sodium concentration up to 10 mEq/L compared with direct ISE [41]. Therefore, in the presence of hyperlipidemias, hyper- and hypoalbuminemia serum sodium levels should be measured with the direct ISE method, while in such cases, it is prudent to measure serum osmolality by an osmometer. The presence of pseudohyponatremia is ascertained when the measured serum osmolality is within normal limits (280–295 mOsm/kg) [19].
3.2. SIADH
SIADH is one of the most common causes of hyponatremia and may be attributed to numerous underlying conditions. Although inappropriate release of ADH is a requirement for this condition, increased intake of liquids also plays an essential role in developing low serum sodium concentrations [42]. When SIADH occurs in the context of malignant hematologic diseases (e.g., lymphomas, leukemia, MM, Waldenström’s macroglobulinemia (WM)), it is mainly ascribed to ectopic ADH secretion or increased interleukin-6 (IL-6) production from malignant cells, as well as to CNS infiltration [43,44,45,46,47,48].
IL-6 induces SIADH by increasing (non-osmotically) the hypothalamic production of ADH [49]. IL-6-mediated SIADH has also been observed in hemophagocytic syndrome [50]. Increased serum levels of lead have also been suggested as an etiologic factor of SIADH in a 5-year-old patient with sickle cell disease, where both hyponatremia and increased levels of ADH were corrected by dimercaprol and calcium ethylenediaminetetraacetic acid (EDTA) chelation treatment [51]. However, it appears more plausible that high levels of IL-6 and stroke due to acute vaso-occlusion play the most important role in SIADH associated with sickle cell disease [52].
SIADH has also been reported in acute intermittent porphyria and post AlloSCT [13,53]. Of note, early presentation of hyponatremia due to SIADH post AlloSCT is insidious and may progress rapidly with fatal outcome [13]. SIADH following AlloSCT or even autoSCT is a relatively infrequent and poorly recognized disorder. Non-specific symptoms of hyponatremia such as nausea, vomiting, and fatigue may be easily attributed to the conditioning regimen prior to transplant. Several risk factors have been implicated in the presentation of SCT-related SIADH, including among others cord blood as the source of the graft, human leukocyte antigen (HLA)-mismatched unrelated donor or recipient, age below 4 years [9], cyclophosphamide [54] or busulphan as components of the conditioning regimen [55], and GvHD prophylaxis with methylprednisolone [9] or tacrolimus [56]. Furthermore, cord blood as the source of the graft, compared to peripheral blood or bone marrow, has been correlated with more severe symptoms, e.g., seizures, somnolence, and earlier onset of hyponatremia [57].
IL-6 and TNF-a have been implicated in the pathophysiology of SCT-related SIADH. These cytokines have been reported to be elevated post SCT from an HLA-mismatched donor or unrelated donor [58]. However, no correlation has been found between acute GvHD and SCT-related SIADH [9,57] as one would expect. Another interesting mechanism of SCT-related SIADH is the reactivation of varicella zoster virus (VZV), one of the most common post-transplant complications with atypical manifestations [59,60,61]. Rau et al. suggested that the triad of severe abdominal pain, inappropriate ADH secretion, and disseminated VZV infection preceding skin lesions should prompt clinicians for VZV DNA blood detection for early recognition and treatment [62].
Other infections affecting the respiratory or CNS as well as several drugs (discussed below) are also frequent underlying causes of SIADH in hematologic diseases. Moreover, pain, nausea, and stress, which are frequently encountered in hematologic patients, are non-osmotic stimuli for ADH release [42].
3.3. Hypovolemia
Extracellular volume depletion is among the most common causes of hyponatremia in clinical practice. Hematologic patients may develop hypovolemic hyponatremia due to renal or extrarenal fluid losses induced by infections (see below), drugs (e.g., vomiting or diarrhea associated with chemotherapy), or the underlying hematologic disease per se. A rather uncommon cause of volume depletion is cerebral salt wasting syndrome (CSWS), first described by Peters JP et al. in 1950 [63]. The release of brain natriuretic peptide leading to natriuresis and hypovolemia has been suggested as the major pathophysiologic mechanism of CSWS [64,65]. Myeloproliferative diseases have been associated with CSWS; it is likely that these disorders cause ischemic lesions in the brain via hyperviscosity and microcirculating abnormalities [66]. CSWS-induced hyponatremia has been observed after AlloSCT and was accompanied by CNS complications (e.g., cerebral hemorrhage, encephalitis) [67], as well as in sickle cell disease [68]. Another term for CSWS is renal salt wasting syndrome (RSWS), given that the presence of cerebral disease is not necessary [69]. Hyponatremia due to renal salt loss ascribed to oncolysis-induced cytokine release has been reported in a patient suffering from natural killer-cell neoplasm accompanied by hemophagocytic syndrome [70]. Salt-losing nephropathy has also been attributed to leukemia-induced tubular defect [47]. In addition, polyuria may occur in central diabetes insipidus (due to leukemia or lymphoma) [71,72] or in nephrogenic diabetes insipidus (due to sickle cell disease or trait and renal amyloidosis) [73,74].
3.4. Hyponatremia Related to Infections in Hematology
Infections, which frequently complicate the clinical course of hematological patients, may cause hyponatremia with several different mechanisms [75]. During the course of an infection, diarrhea, vomiting, or excessive sweating may occur, leading to hypovolemic hyponatremia. Of note, certain infections may be triggered by several treatments used in hematologic patients (e.g., chemotherapy) in combination with the reduced underlying humoral or cell-mediated immunity. For example, in a patient treated with chemotherapy for follicular lymphoma (FL), diarrhea due to severe cytomegalovirus colitis contributed to hyponatremia [76]. Symptomatic hypovolemic hyponatremia ascribed to dengue hemorrhagic fever has also been reported in patients with thalassemias who are susceptible to this infection (endemic in Southeast Asia) [77].
SIADH due to increased hypothalamic production of ADH frequently complicates the course of viral, bacterial, fungal, and tuberculous infections affecting mainly the lungs and the CNS [75]. As aforementioned, acquired hemophagocytic syndrome, which can be triggered by infections (mostly viral), may cause IL-6-mediated SIADH [50]. Of note, coronavirus disease 2019 (COVID-19), which seems to affect the hematopoietic system (e.g., lymphopenia, coagulopathy) has also been associated with IL-6-related hyponatremia [78,79]. Other causes of hyponatremia in the context of an infection are primary (e.g., systemic fungal infections, acquired immunodeficiency syndrome) or secondary adrenal insufficiency (e.g., tuberculosis), severe renal injury (e.g., leptospirosis), nephrotic syndrome (e.g., HBV and HCV), CSWS (e.g., cerebral toxoplasmosis or human herpesvirus 6 encephalitis), and congestive heart failure (infection-induced myocarditis) [75]. Furthermore, by increasing the secretion of catecholamines, glucagon, and cortisol, infections may promote hyperglycemia and, subsequently, hyponatremia (see next section).
Importantly, some antibiotics may induce hyponatremia. Trimethoprim, which structurally resembles the potassium-sparing diuretic amiloride, may cause hypovolemic hyponatremia, especially if administered in high doses [75]. Other antibiotics or antifungals (e.g., ciprofloxacin, pentamidine, voriconazole) are rarely implicated in the development of hyponatremia [75].
Several infections (e.g., infective endocarditis, leishmaniasis, human immunodeficiency virus (HIV) infection, HCV) through polyclonal activation of B-lymphocytes may induce hypergammaglobulinemia and, accordingly, pseudohyponatremia [75]. Noteworthy, most of the aforementioned pathophysiological pathways causing hyponatremia may be observed in HIV infection [75]. Low serum sodium concentration in the context of an infection may be a negative prognostic indicator of mortality; in fact, in an observational, retrospective, cross-sectional study in patients < 18 years old with Shiga toxin-producing Escherichia coli hemolytic uremic syndrome, hyponatremia was a mortality predictor [7].
3.5. Hyponatremia Due to Disorders of Endocrine System and Metabolism in Hematology
Diabetes mellitus (DM) is frequently observed in the adult general population, and its incidence is constantly rising having reached epidemic proportions. Noteworthy, a meta-analysis of observational studies demonstrated that DM may increase the risk of developing non-Hodgkin lymphoma, leukemia, and myeloma [80]. Certain hematologic disorders (e.g., hemochromatosis, major thalassemia) are pathophysiologically linked to DM. Specifically, it has been postulated that DM is the result of iron overload, the latter being deposited to the pancreas and causing oxidative stress to β-cells, subsequently leading to pancreatic dysfunction [81,82]. DM as a complication of major thalassemia is usually manifested after the first decade of life [82,83]. Hyperglycemia in hematological patients may also be the result of infections or certain medications [84,85,86]. For instance, corticosteroids are frequently used for the treatment of both malignant and benign (e.g., immune thrombocytopenia and autoimmune hemolytic anemia) disorders. Furthermore, immunosuppressive drugs, such as tacrolimus, have been associated with post-transplant DM [86]. Long-term survivors of HSCT are at increased risk of developing metabolic syndrome and DM; these probably ensue in the context of the long-term effects of intensive chemotherapy, as well as the immunological and inflammatory consequences of GvHD and its treatment [87]. Immune checkpoint inhibitors, such as pembrolizumab and nivolumab used in Hodgkin’s lymphoma (HL), have been associated with autoimmune diabetes and even diabetic ketoacidosis [88]. Finally, interferon therapy has been associated with hyperglycemia and DM [89].
Glucose is an osmotically active substance; thus, in the context of hyperglycemia, osmotic shifts of water from the intracellular to the extracellular space lead to dilutional hyponatremia. In hyperglycemic states, serum sodium concentration should be corrected; the most commonly used formula is corrected sodium = measured sodium + (1.6 (glucose − 100)/100). When glucose concentration is above 400 mg/dL, a correction factor of 2.4 should be used. Poorly controlled DM may cause hypovolemic hyponatremia via osmotic diuresis, whereas in patients with diabetic ketoacidosis, the excretion of beta-hydroxybutyrate and acetoacetate aggravates urine sodium losses [90]. Of note, DM per se (in the absence of hyperglycemia) may lead to hyponatremia, possibly through induction of aquaporin-2 (AQP2) by insulin [91]. AQP2 is found in the apical cell membranes of the principal cells in the collecting duct of the kidney, as well as in intracellular vesicles located throughout these cells. It is regulated by vasopressin and is involved in water reabsorption. Thus, in the case of increased expression of AQP2, excessive water reabsorption and subsequently hyponatremia occur [92].
Other endocrine disorders, including primary adrenal insufficiency (Addison’s disease), secondary adrenal insufficiency, and hypothyroidism, are less frequent causes of hyponatremia [16]. The association between infections and adrenal insufficiency in hematologic individuals has already been discussed.
Hyponatremia has been observed in patients with intravascular large B-cell lymphoma both via SIADH and hypopituitarism [93,94]. On the other hand, diffuse large B cell lymphoma (DLBCL) may lead to hyponatremia through bilateral adrenal or hypothalamus invasion [95,96]. In fact, a recent meta-analysis showed that malignancies, including lymphomas, may lead to adrenal insufficiency due to bilateral adrenal infiltration [97]. A case of bilateral adrenal hemorrhage in a patient with acute myeloid leukemia (AML) has also been reported [98]. Furthermore, adrenal insufficiency may be the result of isolated adrenocorticotropic hormone (ACTH) deficiency in ALL patients [99]. Patients with hemoglobinopathies, including thalassemias and sickle cell disease, may present with several endocrine disorders, including hypogonadotropic hypogonadism, DM, hypothyroidism, hypoparathyroidism, and adrenal insufficiency, mainly due to iron overload [100,101]. Adrenal insufficiency due to plasma cell infiltration with light-chain (AL) amyloid deposition in the pituitary and adrenal gland has been reported in a patient with WM [46].
Adrenal insufficiency may occur due to inappropriate interruption of glucocorticoid therapy, as the hypothalamus adrenal axis is suppressed. This, however, may be easily prevented by meticulous explanation regarding corticosteroid therapy from the physicians in charge and close follow-up of patients. Importantly, the synchronous administration of antifungal agents (e.g., fluconazole, posaconazole), which are frequently used in hematologic patients, may keep the axis suppressed for longer periods of time due to inhibition of the steroidogenesis pathway [102,103]. Nivolumab has been associated with adrenalitis and Addison’s disease [104], as well as hypothyroidism and secondary adrenal insufficiency due to selective pituitary dysfunction [105]. In addition, long-term survivors of childhood ALL, who were treated with moderate dose of cranial radiotherapy, exhibited central adrenal insufficiency 20 years after treatment [106].
3.6. Hyponatremia Related to Kidney Injury in Patients with Hematologic Diseases
Renal impairment affecting the urinary dilution capacity leads to hyponatremia due to decreased excretion of water. However, in less severe renal disease, water retention is limited and excessive water intake plays a major role in the development of hyponatremia [107]. Kidney disorders are often encountered in clinical practice. For example, acute kidney injury (AKI) due to prerenal azotemia may be induced by hemorrhage, gastrointestinal losses, renal losses (e.g., osmotic diuresis), low cardiac output, or decreased vascular resistance (e.g., due to infections). Of note, several pharmaceutical agents used in hematological disorders, such as platinum-containing drugs, alkylating agents, and methotrexate, are nephrotoxic [108,109]. Furthermore, contrast-induced kidney injury is common, especially in patients with cancer [110]. In a recent study, the incidence of AKI in hospitalized patients with hematological malignancies was 15.4% and serum sodium levels were directly related to AKI [111]. Hemoglobinopathies, complement disorders, and infections such as malaria may cause AKI via intravascular hemolysis [112]. Renal thrombotic microangiopathy leading to impaired renal function is a common complication associated with hematopoietic stem cell transplantation (HSCT) [113]. Kidney injury post-HSCT may also be the result of several other factors, including chemotherapy, radiation, sepsis, drugs (e.g., antibiotics, calcineurin inhibitors), bone marrow toxicity, hepatic veno-occlusive disease, and GvHD [114]. Renal impairment is very common in MM and other lymphoid malignancies and paraproteinemias [115,116,117]. Hypercalcemia, hyperuricemia, dehydration, renal parenchymal involvement, ureteral obstruction, glomerulonephropathy, renal vascular compromise, and tumor lysis syndrome may all be culprits of kidney injury in these patients [117]. In addition, patients suffering MM are prone to infections and often use non-steroid anti-inflammatory drugs (NSAIDs) as painkillers; these are also risk factors for AKI [118]. A case of cryoglobulinemic glomerulonephritis associated with nodal and renal infiltration by T-cell lymphoma of T-follicular helper phenotype has also been reported [119]. AKI is mainly observed in hemolytic uremic syndrome but may also occur in thrombotic thrombocytopenic purpura [120,121,122]. Paroxysmal nocturnal hemoglobinuria (PNH) may cause both acute and chronic renal impairment via several pathophysiological mechanisms, mainly including the release of free heme and iron due to intravascular hemolysis and subsequent hemoglobinuria, Fanconi syndrome, and possibly subclinical microvascular thrombosis [123].
Furthermore, chronic kidney disease is a common complication in sickle cell disease and sickle trait. This mainly occurs due to repetitive episodes of sickling, which induce ischemic damage and microinfarctions, leading to loss of the vascular architecture of the renal medulla. Other contributory factors are glomerular hyperfiltration and renal hyperperfusion, endothelial dysfunction, and the release of free heme due to hemolysis [124,125,126].
3.7. Hyponatremia Related to Cardiac Disorders in Hematologic Patients
Hyponatremia in heart failure (HF) is mainly attributed either to neurohormonal activation due to effective circulating volume depletion or to diuretic administration [127].
HF is a common complication of various hematologic diseases and drugs used in clinical hematology. Hemoglobinopathies, mainly beta (β)-thalassemia and sickle cell disease, are associated with HF in the context of chronic hemolysis and sickling. Specifically, chronic hemolysis leads to anemia and, accordingly, high-output HF, as well as vasculopathy, while sickling induces both vasculopathy and myocardial ischemia. Furthermore, repetitive blood transfusions and increased iron absorption from ineffective erythropoiesis in patients with hemoglobinopathies may induce iron overload cardiomyopathy [128]. Deposition of amyloid and iron in the heart in amyloid disease and hemochromatosis, respectively, have also been associated with cardiomyopathy [129].
Of note, the treatment of several hematological diseases may impair cardiac function. In particular, thoracic radiation may provoke cardiomyopathy 5 to 30 years after initial exposure [130], whereas anthracyclines have been shown to cause irreversible dose-dependent cardiac damage and late-onset HF [131]. Several studies have demonstrated the involvement of anthracyclines in the development of HF in survivors of both childhood- and adult-onset cancers, as well as in patients with HL or aggressive NHL [132,133,134,135]. Alkylating agents, such as cyclophosphamide, fluoropyrimidines, and tyrosine kinase inhibitors, have been associated with cardiovascular complications including HF [136,137,138]. Chimeric antigen receptor (CAR) T-cell therapy may have deleterious effects on the myocardium and even lead to HF via excessive release of cytokines [139]. Furthermore, immune checkpoint inhibitors have been associated with myocarditis [140].
3.8. Hyponatremia Related to Liver Diseases in Hematologic Patients
Hyponatremia is frequently encountered in hepatopathies, mainly cirrhosis, in part due to reduced effective arterial blood volume as well as other involved mechanisms. It should be noted that marked hyperlipidemia (hypertriglyceridemia and/or hypercholesterolemia) and hypergammaglobulinemia, which are also common features of liver disorders, are among the major culprits of pseudohyponatremia [37]. Liver involvement may be observed in the course of several hematologic diseases, potentially leading to or aggravating hyponatremia. Cirrhosis may be the outcome of hemosiderosis due to transfusional iron overload in beta (β)-thalassemias. In sickle cell disease, repeated episodes of vascular occlusion affecting the liver may impair its function. Autoimmune hemolytic anemia and autoimmune hepatitis may co-exist. Hepatic vein obstruction (Budd–Chiari syndrome) may occur in polycythemia vera or other myeloproliferative diseases, PNH, as well as in patients who have undergone bone marrow transplantation [141,142,143]. Liver infiltration (e.g., lymphoma, leukemia, multiple myeloma) may end up in a broad spectrum of disorders ranging from asymptomatic elevation of liver function tests to acute hepatic failure [144]. Importantly, certain diseases (e.g., hemochromatosis, Wilson disease) may have both hepatic and hematologic manifestations, whereas several comorbidities or sequelae of hematologic diseases (e.g., DM, HF, HBV, HCV) are implicated in the development of hepatic cirrhosis. Specifically, cirrhosis may be the result of DM-related non-alcoholic fatty liver disease, while HF may lead to hepatic fibrosis (“cardiac cirrhosis”) [37]. Furthermore, HBV and HCV infections after multiple blood transfusions in hematologic patients may also develop cirrhosis.
3.9. Hyponatremia Related to Pharmacological Agents Used in the Treatment of Blood Diseases
Many drugs commonly used for the treatment of certain hematological diseases have been associated with low serum sodium concentration (Table 1). The most common mechanism of drug-induced hyponatremia is SIADH. Nausea, a common side effect of chemotherapeutic agents, is a very potent trigger for ADH secretion. Vinca alkaloids, such as vincristine, induce hyponatremia through SIADH [145,146,147]. We should note that the simultaneous administration of vincristine with azoles is contraindicated, as the latter inhibit vincristine metabolism and, subsequently, may exacerbate the adverse effects of this drug, including neurotoxicity and hyponatremia [148,149]. CD19 + CAR T-cells used for the treatment of relapsed/refractory ALL may cause hyponatremia due to hypercytokinemia and elevated IL-6, which stimulates the hypothalamus for the inappropriate release of ADH [150]. Methotrexate in high doses may lead to hyponatremia, probably due to the toxic effects on the neurosecretory areas of the cerebrum, activation of natriuretic peptides, or changes in the distribution of body fluid volumes [109,151]. Cyclophosphamide causes hyponatremia, mainly when it is administered in high doses due to concurrent administration of large volume of hypotonic fluids in order to prevent hemorrhagic cystitis. However, hyponatremia may also be observed when cyclophosphamide is administered at lower doses [152]. It should be noted that several chemotherapy protocols mainly for patients with lymphoma, such as hyper-CVAD (cyclophosphamide, vincristine sulfate, doxorubicin hydrochloride, dexamethasone, methotrexate, cytarabine) and CODOX-M/IVAC (cyclophosphamide, vincristine, doxorubicin, high-dose methotrexate/ifosfamide, etoposide, high-dose cytarabine) include the co-administration of cyclophosphamide and vincristine. Both regimens carry a > 20% risk of febrile neutropenia, and antifungals such as azoles are routinely co-administered, increasing the risk of hyponatremia, as mentioned above. Selinexor, an oral selective inhibitor of nuclear export currently in clinical development for relapsed refractory multiple myeloma, has been shown to cause hyponatremia in almost 30% of patients [153]. Ibrutinib, which is widely used for the treatment of chronic lymphocytic leukemia, mantle cell lymphoma and WM, has been shown to cause hyponatremia in up to 6% of treated patients [154].
Platinum-based antineoplastic drugs may also lower sodium levels, mainly due to the concurrent administration of large volumes of hypotonic fluids in order to prevent nephrotoxicity [109]. Both SIADH and CSWS have been recognized as underlying mechanisms of hyponatremia in patients taking cisplatin [145,155,156]. In contrast, hyponatremia is less frequently encountered with oxaliplatin compared with cisplatin [157]. An increase in urinary N-acetyl β-glycosaminidase, a proximal tubule lysosomal enzyme, within 24–48 h after administration of cisplatin, is proposed as a predictor of developing hyponatremia associated with this drug [155,158].
Intravenous administration of sucrose-containing immunoglobulin may cause true hyponatremia attributed to the translocational effect of the osmotic load of sucrose [159]. Translocational (hyperosmolar) hyponatremia may also be observed with maltose-containing IVIG in the presence of renal impairment. In this setting, maltose, normally metabolized by maltase at the proximal renal tubules, is accumulated in the extracellular fluid, thus increasing serum osmolality and diminishing serum levels by means of dilution. Aseptic meningitis-associated SIADH is another potential underlying mechanism of hyponatremia following IVIG [39]. Most tyrosine kinase inhibitors (TKIs), specifically imatinib, nilotinib, dasatinib, and bosutinib have been dose-dependently associated with hyponatremia, mainly due to SIADH [160,161]. In contrast, ponatinib has not been associated with hyponatremia so far.
Drugs used in clinical hematology and their associated underlying mechanisms for hyponatremia are shown in Table 2.
Patients treated for hematological disorders are often administered several drugs for various other conditions, including tricyclic antidepressants, selective serotonin re-uptake inhibitors, proton pump inhibitors, antiepileptic drugs, trimethoprim-sulfamethoxazole, NSAIDs, tramadol, and other opioid analgesics, all of which have also been related to hyponatremia [39,162].
4. Evaluation of Hyponatremia
Patients with hyponatremia frequently manifest severe neurologic complications due to brain edema. On the other hand, the rapid correction of hyponatremia may lead to the development of central demyelinating lesions, particularly in the pons (a disorder called central pontine myelinolysis or osmotic demyelination syndrome (ODS)) with major neurologic disabilities or even death [181]. Consequently, the timely recognition of the underlying cause(s) of hyponatremia is crucial for the appropriate management and avoidance of therapeutic pitfalls, which can lead to under- or over-treatment of hyponatremia. A step-by-step diagnostic evaluation of hyponatremia in hematologic patients is shown in Figure 1. Some points, however, deserve emphasis.
Urine sodium concentration (UNa) in a random urine specimen has a pivotal role in the diagnostic approach. Values less or more than 30 mEq/L are suggestive of low effective arterial blood volume or SIADH, respectively. However, UNa levels > 30 mEq/L are also found in case of diuretic administration, osmotic diuresis, salt losing nephropathy, primary adrenal insufficiency, and metabolic alkalosis. On the other hand, UNa < 30 mEq/L can be observed in patients with chronic SIADH on a low salt diet or anorexia. In the presence of metabolic alkalosis, a low urine chloride concentration (<25 mEq/L) is a useful index of extracellular volume depletion [37].
Hyponatremia due to SIADH and CSWS may be observed in hematologic diseases with intracranial involvement [182]. The latter has a similar laboratory picture with SIADH (i.e., hypouricemia along with a fractional excretion of uric acid (FEUA) > 11%, Una > 30 mmol/L and Uosm > 100 mOsmol/kg). Importantly, though, the treatment is not the same due to the different volume status in these disorders (i.e., normovolemia in the case of SIADH versus hypovolemia in the case of CSWS). The differentiation between CSWS and SIADH is often challenging in clinical practice, since the assessment of extracellular volume, not infrequently, is unreliable on clinical grounds. In fact, clear evidence of volume depletion (e.g., hypotension, decreased skin turgor, elevated hematocrit, increased blood urea nitrogen to creatinine ratio) is frequently absent in CSWS. Thus, in a seemingly normovolemic patient with hyponatremia associated with “intracranial disease”, fluid restriction, loop diuretics, and vaptans (ADH antagonists) used for the treatment of SIADH should be avoided, as they may deteriorate both hypovolemia and hyponatremia, leading to cerebral edema and even seizures in case of CSWS [183]. On the contrary, hypertonic saline should be administered in such cases. The estimation of FEUA after correcting hyponatremia is considered a useful tool in establishing the correct diagnosis given that FEUA normalizes in SIADH but remains > 11% in CSWS. Noteworthy, isotonic saline may aggravate hyponatremia due to SIADH if the Uosm is higher than serum osmolarity (especially in cases of Uosm > 530 mOsm/kg), thus, it should be avoided [182,184].
Hypopituitarism with secondary adrenal insufficiency is another overlooked cause of hyponatremia often presenting with a SIADH-like picture (euvolemic hyponatremia, low serum uric acid, and urea levels, UNa > 30 mmol/L, Uosm > 100 mOsmol/kg). Moreover, the differentiation between primary and secondary adrenal insufficiency are not infrequently difficult given that typical characteristics ascribed to mineralocorticoid deficiency, may not be present in the latter. Indeed, hyperkalemia may be absent in approximately 30–50% of patients with Addison’s disease, while hypovolemia as clinically assessed may not be evident. In such cases, certain diagnostic tests (cortisol determination and adrenocorticotropic hormone (ACTH) stimulation test) may be required for the diagnosis of hypothalamic–pituitary–adrenal axis disorders [16].
Finally, it should be pointed out that hypothyroidism-induced hyponatremia is rather rare and probably occurs only in severe hypothyroidism (TSH > 50 mIU/L). Even in myxedema coma, however, other possible causes and superimposed factors of hyponatremia (e.g., drugs, infections, adrenal insufficiency) should be considered before attributing the low serum sodium levels to hypothyroidism per se [185]. An algorithm for the proper approach to a patient with hypotonic hyponatremia, Uosm > 100 mOsm/kg, and hematologic disease is shown in Figure 2.
5. Treatment of Hyponatremia
Treatment of hyponatremia is mainly focused on how to avoid the devastating neurologic complications, which may occur either during the course of or after overcorrection of this electrolyte disorder. The appropriate rate of correction of hyponatremia should be <8–10 mEq/L/24 h [181,186]. However, in the presence of conditions that predispose patients to develop ODS (i.e., hypokalemia, malnutrition, liver disease, alcoholism, and serum sodium levels ≤ 105 mEq/L), the appropriate rate of correction should be limited to 4–6 mEq/L/24 h [181,186,187]. As a general rule, the therapeutic interventions for hyponatremia are based on its duration, as well as on patient’s symptoms and extracellular volume status [18,188].
In cases of severe neurological symptoms due to hyponatremia a bolus infusion of 100–150 mL of hypertonic saline (3% NaCl) over 20 min, up to three times is recommended [186,187]. The goal is an increase in serum sodium concentration by 4–6 mEq/L within the first 4–6 h in order to reverse the symptoms of hyponatremic encephalopathy, without, however, exceeding the aforementioned targets. Continuous infusion of 3% NaCl (0.5–2 mL/kg/hour) can be used for moderate symptoms [186,187,189,190].
Treatment of the underlying conditions related to hyponatremia (e.g., infections, hyperglycemia, primary adrenal insufficiency) and discontinuation of diuretics are crucial in the management of hypovolemic hyponatremia. Normal saline or lactated Ringer’s solution should be used to restore the intravascular volume [187,191]. Close monitoring of serum sodium levels (every few hours) and urine output is strongly recommended in order to avoid an overly rapid increase in sodium concentration when volume status is restored. In this setting, an abrupt decrease in ADH secretion and, subsequently, a rapid increase in diuresis is observed. Noteworthy, in hypovolemic states, any potassium deficit should also be corrected. In such cases, potassium chloride should be added in hypotonic fluids. The administration of normal saline plus potassium chloride (i.e., a hypertonic solution) should be avoided, as it increases the risk of overcorrection of hyponatremia as well as that of volume overload and pulmonary edema, especially in the elderly or in patients with HF [191].
Fluid restriction is the first line therapy in hyponatremia due to SIADH. Discontinuation of the offending drugs and treatment of other superimposed factors (e.g., infection, pain, nausea) are also essential. Increased solute intake (such as salt tablets or urea) and loop diuretics can also be used to increase water clearance.
In contrast, restriction of fluid intake and administration of loop diuretics to correct increased total body water and sodium are required for the treatment of hypervolemic hyponatremia. Vaptans—drugs which promote water diuresis—are indicated as second-line therapy for hyponatremia related to hypervolemic or euvolemic hyponatremia due to SIADH [188]. Importantly, vaptans should not be used in hypovolemic hyponatremia or together with hypertonic saline solution owing to case reports of associated ODS [186,187,192]. Edematous hyponatremia, in the context of severe acute or chronic kidney injury generally, requires dialysis. Basic principles of hyponatremia management are shown in Table 3.
6. Conclusions
Hyponatremia, often multifactorial, is frequently observed in patients with hematologic disorders and may aggravate their already fragile clinical condition. The severity of this disorder is often underestimated because of its non-specific clinical features that may be mistakenly attributed to other clinical entities, such as neutropenic sepsis, chemotherapy side effects, CNS involvement, or disease-related fatigue. Special efforts should be made to define the underlying causal mechanisms and appropriately individualize therapy. Specific attention should be given to the co-administration of drugs that alter each other’s metabolism, as this may contribute to or aggravate an already existing hyponatremia. Beyond the specific treatment of hyponatremia based on its duration, symptoms, and extracellular volume status, the therapeutic approach should involve discontinuation of any offending medications and management of other conditions (e.g., infectious, cardiac, renal, or endocrine) that may also contribute to this disorder. Overall, it is important for hematologists to become familiar with the timely recognition and appropriate therapeutic approach of hyponatremia.
Author Contributions
Conceptualization and design: E.K., G.L., E.H., M.F.; writing—original draft preparation: E.K., G.L.; writing—review and editing of the manuscript M.F., E.H., G.L.; figures and tables created by E.K. and M.F. and critically revised by E.H. and G.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Upadhyay, A.; Jaber, B.L.; Madias, N.E. Incidence and prevalence of hyponatremia. Am. J. Med. 2006, 119, S30–S35. [Google Scholar] [CrossRef] [PubMed]
- Mohan, S.; Gu, S.; Parikh, A.; Radhakrishnan, J. Prevalence of hyponatremia and association with mortality: Results from NHANES. Am. J. Med. 2013, 126, 1127–1137.e1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterns, R.H. Disorders of plasma sodium—Causes, consequences, and correction. N. Engl. J. Med. 2015, 372, 55–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verbalis, J.G.; Barsony, J.; Sugimura, Y.; Tian, Y.; Adams, D.J.; Carter, E.A.; Resnick, H.E. Hyponatremia-induced osteoporosis. J. Bone Miner. Res. 2010, 25, 554–563. [Google Scholar] [CrossRef] [Green Version]
- Burst, V. Etiology and epidemiology of hyponatremia. Front. Horm. Res. 2019, 52, 24–35. [Google Scholar] [CrossRef]
- Li, Y.; Chen, X.; Shen, Z.; Wang, Y.; Hu, J.; Xu, J.; Shen, B.; Ding, X. Electrolyte and acid-base disorders in cancer patients and its impact on clinical outcomes: Evidence from a real-world study in China. Ren. Fail. 2020, 42, 234–243. [Google Scholar] [CrossRef] [Green Version]
- Alconcher, L.F.; Coccia, P.A.; Suarez, A.D.C.; Monteverde, M.L.; Perez, Y.G.M.G.; Carlopio, P.M.; Missoni, M.L.; Balestracci, A.; Principi, I.; Ramírez, F.B.; et al. Hyponatremia: A new predictor of mortality in patients with Shiga toxin-producing Escherichia coli hemolytic uremic syndrome. Pediatr. Nephrol. 2018, 33, 1791–1798. [Google Scholar] [CrossRef]
- Janczar, S.; Zalewska-Szewczyk, B.; Mlynarski, W. Severe hyponatremia in a single-center series of 84 homogenously treated children with acute lymphoblastic leukemia. J. Pediatr. Hematol. Oncol. 2017, 39, e54–e58. [Google Scholar] [CrossRef]
- Kobayashi, R.; Iguchi, A.; Nakajima, M.; Sato, T.; Yoshida, M.; Kaneda, M.; Suzuki, Y.; Mino, E.; Kuroki, F.; Kobayashi, K. Hyponatremia and syndrome of inappropriate antidiuretic hormone secretion complicating stem cell transplantation. Bone Marrow Transplant. 2004, 34, 975–979. [Google Scholar] [CrossRef]
- Castillo, J.J.; Glezerman, I.G.; Boklage, S.H.; Chiodo, J., 3rd; Tidwell, B.A.; Lamerato, L.E.; Schulman, K.L. The occurrence of hyponatremia and its importance as a prognostic factor in a cross-section of cancer patients. BMC Cancer 2016, 16, 564. [Google Scholar] [CrossRef] [Green Version]
- Marroncini, G.; Fibbi, B.; Errico, A.; Grappone, C.; Maggi, M.; Peri, A. Effects of low extracellular sodium on proliferation and invasive activity of cancer cells in vitro. Endocrine 2020, 67, 473–484. [Google Scholar] [CrossRef] [PubMed]
- Rech, J.S.; Yao, K.; Bachmeyer, C.; Bailleul, S.; Javier, O.; Grateau, G.; Lionnet, F.; Steichen, O. Prognostic value of hyponatremia during acute painful episodes in sickle cell disease. Am. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Xiao, Y.; Yu, X.; Zhou, J.; Zhang, Y. Early onset of syndrome of inappropriate antidiuretic hormone secretion (SIADH) after allogeneic haematopoietic stem cell transplantation: Case report and review of the literature. J. Int. Med. Res. 2010, 38, 705–710. [Google Scholar] [CrossRef] [PubMed]
- Gillum, D.M.; Linas, S.L. Water intoxication in a psychotic patient with normal renal water excretion. Am. J. Med. 1984, 77, 773–774. [Google Scholar] [CrossRef]
- Sahay, M.; Sahay, R. Hyponatremia: A practical approach. Indian J. Endocrinol. Metab. 2014, 18, 760–771. [Google Scholar] [CrossRef]
- Liamis, G.; Milionis, H.J.; Elisaf, M. Endocrine disorders: Causes of hyponatremia not to neglect. Ann. Med. 2011, 43, 179–187. [Google Scholar] [CrossRef]
- Berl, T. Impact of solute intake on urine flow and water excretion. J. Am. Soc. Nephrol. 2008, 19, 1076–1078. [Google Scholar] [CrossRef]
- Filippatos, T.D.; Liamis, G.; Elisaf, M.S. Ten pitfalls in the proper management of patients with hyponatremia. Postgrad. Med. 2016, 128, 516–522. [Google Scholar] [CrossRef]
- Liamis, G.; Liberopoulos, E.; Barkas, F.; Elisaf, M. Spurious electrolyte disorders: A diagnostic challenge for clinicians. Am. J. Nephrol. 2013, 38, 50–57. [Google Scholar] [CrossRef]
- Yavasoglu, I.; Tombuloglu, M.; Kadikoylu, G.; Donmez, A.; Cagirgan, S.; Bolaman, Z. Cholesterol levels in patients with multiple myeloma. Ann. Hematol. 2008, 87, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Burnside, N.J.; Alberta, L.; Robinson-Bostom, L.; Bostom, A. Type III hyperlipoproteinemia with xanthomas and multiple myeloma. J. Am. Acad. Dermatol. 2005, 53, S281–S284. [Google Scholar] [CrossRef] [PubMed]
- Chudy-Onwugaje, K.; Anyadike, N.; Tsirlin, Y. Severe Hypercholesterolemia: A unique presentation of non-hodgkin’s lymphoma in a patient with neurofibromatosis type 1. Case Rep. Gastrointest. Med. 2014, 2014, 579352. [Google Scholar] [CrossRef] [PubMed]
- Zawitkowska, J.; Lejman, M.; Zaucha-Prazmo, A.; Sekula, N.; Greczkowska-Chmiel, T.; Drabko, K. Severe drug-induced hypertriglyceridemia treated with plasmapheresis in children with acute lymphoblastic leukemia. Transfus. Apher. Sci. 2019, 58, 634–637. [Google Scholar] [CrossRef] [PubMed]
- Kothari, J.; Thomas, A.; Goldstone, A. Pseudohyponatraemia due to L-asparaginase-associated dyslipidaemia in T-cell lymphoblastic lymphoma. BMJ Case Rep. 2014, 2014. [Google Scholar] [CrossRef] [Green Version]
- Conley, B.A.; Egorin, M.J.; Sridhara, R.; Finley, R.; Hemady, R.; Wu, S.; Tait, N.S.; van Echo, D.A. Phase I clinical trial of all-trans-retinoic acid with correlation of its pharmacokinetics and pharmacodynamics. Cancer Chemother. Pharmacol. 1997, 39, 291–299. [Google Scholar] [CrossRef]
- Inamoto, Y.; Teramoto, T.; Shirai, K.; Tsukamoto, H.; Sanda, T.; Miyamura, K.; Yamamori, I.; Hirabayashi, N.; Kodera, Y. Severe hypercholesterolemia associated with decreased hepatic triglyceride lipase activity and pseudohyponatremia in patients after allogeneic stem cell transplantation. Int. J. Hematol. 2005, 82, 362–366. [Google Scholar] [CrossRef]
- Joukhadar, R.; Chiu, K. Severe hypercholesterolemia in patients with graft-vs-host disease affecting the liver after stem cell transplantation. Endocr. Pract. 2012, 18, 90–97. [Google Scholar] [CrossRef]
- Li, J.; Wang, Q.; Zheng, W.; Ma, J.; Zhang, W.; Wang, W.; Tian, X. Hemophagocytic lymphohistiocytosis: Clinical analysis of 103 adult patients. Medicine 2014, 93, 100–105. [Google Scholar] [CrossRef]
- Jordan, M.B.; Allen, C.E.; Weitzman, S.; Filipovich, A.H.; McClain, K.L. How I treat hemophagocytic lymphohistiocytosis. Blood 2011, 118, 4041–4052. [Google Scholar] [CrossRef] [Green Version]
- Gupta, N.; Kaur, H.; Wajid, S. Renal amyloidosis: An update on diagnosis and pathogenesis. Protoplasma 2020. [Google Scholar] [CrossRef]
- Joven, J.; Villabona, C.; Vilella, E.; Masana, L.; Albertí, R.; Vallés, M. Abnormalities of lipoprotein metabolism in patients with the nephrotic syndrome. N. Engl. J. Med. 1990, 323, 579–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wheeler, D.C.; Bernard, D.B. Lipid abnormalities in the nephrotic syndrome: Causes, consequences, and treatment. Am. J. Kidney Dis. 1994, 23, 331–346. [Google Scholar] [CrossRef]
- Vaziri, N.D. Disorders of lipid metabolism in nephrotic syndrome: Mechanisms and consequences. Kidney Int. 2016, 90, 41–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Moshary, M.; Al-Mussaed, E.; Khan, A. Prevalence of transfusion transmitted infections and the quality of life in β-thalassemia major patients. Cureus 2019, 11, e6129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akhtar, S.; Nasir, J.A.; Hinde, A. The prevalence of hepatitis C virus infection in β-thalassemia patients in Pakistan: A systematic review and meta-analysis. BMC Public Health 2020, 20, 587. [Google Scholar] [CrossRef]
- Vo, H.; Gosmanov, A.R.; Garcia-Rosell, M.; Wall, B.M. Pseudohyponatremia in acute liver disease. Am. J. Med. Sci. 2013, 345, 62–64. [Google Scholar] [CrossRef]
- Liamis, G.; Filippatos, T.D.; Liontos, A.; Elisaf, M.S. Hyponatremia in patients with liver diseases: Not just a cirrhosis-induced hemodynamic compromise. Hepatol. Int. 2016, 10, 762–772. [Google Scholar] [CrossRef]
- Decaux, O.; Laurat, E.; Perlat, A.; Cazalets, C.; Jego, P.; Grosbois, B. Systemic manifestations of monoclonal gammopathy. Eur. J. Intern. Med. 2009, 20, 457–461. [Google Scholar] [CrossRef]
- Liamis, G.; Megapanou, E.; Elisaf, M.; Milionis, H. Hyponatremia-inducing drugs. Front. Horm. Res. 2019, 52, 167–177. [Google Scholar] [CrossRef]
- Goldwasser, P.; Ayoub, I.; Barth, R.H. Pseudohypernatremia and pseudohyponatremia: A linear correction. Nephrol. Dial. Transpl. 2015, 30, 252–257. [Google Scholar] [CrossRef] [Green Version]
- Dimeski, G.; Morgan, T.J.; Presneill, J.J.; Venkatesh, B. Disagreement between ion selective electrode direct and indirect sodium measurements: Estimation of the problem in a tertiary referral hospital. J. Crit. Care 2012, 27, 316–326.e329. [Google Scholar] [CrossRef]
- Ellison, D.H.; Berl, T. Clinical practice. The syndrome of inappropriate antidiuresis. N. Engl. J. Med. 2007, 356, 2064–2072. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, N.; Tanaka, S.; Watanabe, Y.; Tokuyama, W.; Hiruta, N.; Ohwada, C.; Sakaida, E.; Nakaseko, C.; Tatsuno, I. Syndrome of inappropriate antidiuretic hormone secretion in a patient with mucosa-associated lymphoid tissue lymphoma. Intern. Med. 2017, 56, 3225–3229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, A.; Shafi, F.; Iqbal, M.; Kollipara, R.; Rouf, E. Syndrome of inappropriate antidiuretic hormone due to multiple myeloma. Mo. Med. 2011, 108, 377–379. [Google Scholar]
- Braden, G.L.; Mikolich, D.J.; White, C.F.; Germain, M.J.; Fitzgibbons, J.P. Syndrome of inappropriate antidiuresis in Waldenstrom’s macroglobulinemia. Am. J. Med. 1986, 80, 1242–1244. [Google Scholar] [CrossRef]
- Yamada, C.; Yoneda, C.; Ogino, J.; Fukushima, S.; Kodama, S.; Asano, C.; Masuda, M.; Horie-Tajima, K.; Toyonaga, A.; Hiroshima, K.; et al. An autopsy case of macroglobulinemia complicated with syndrome of inappropriate secretion of ADH (SIADH) like hyponatremia, hypopituitarism and AL amyloidosis. Endocr. J. 2014, 61, 417–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippatos, T.D.; Milionis, H.J.; Elisaf, M.S. Alterations in electrolyte equilibrium in patients with acute leukemia. Eur. J. Haematol. 2005, 75, 449–460. [Google Scholar] [CrossRef] [PubMed]
- Joshi, H.; Nagumantry, S.; Pierres, F.; Oyibo, S.O.; Sagi, S.V. Difficult-to-treat syndrome of inappropriate antidiuretic hormone secretion in a patient with secondary central nervous system lymphoma. Cureus 2019, 11, e3905. [Google Scholar] [CrossRef] [Green Version]
- Swart, R.M.; Hoorn, E.J.; Betjes, M.G.; Zietse, R. Hyponatremia and inflammation: The emerging role of interleukin-6 in osmoregulation. Nephron. Physiol. 2011, 118, 45–51. [Google Scholar] [CrossRef]
- Malinowska, I.; Machaczka, M.; Popko, K.; Siwicka, A.; Salamonowicz, M.; Nasilowska-Adamska, B. Hemophagocytic syndrome in children and adults. Arch. Immunol. Ther. Exp. 2014, 62, 385–394. [Google Scholar] [CrossRef] [Green Version]
- Suarez, C.R.; Black, L.E., 3rd; Hurley, R.M. Elevated lead levels in a patient with sickle cell disease and inappropriate secretion of antidiuretic hormone. Pediatr. Emerg. Care 1992, 8, 88–90. [Google Scholar] [CrossRef] [PubMed]
- Domingos, I.F.; Pereira-Martins, D.A.; Sobreira, M.; Oliveira, R.T.D.; Alagbe, A.E.; Lanaro, C.; Albuquerque, D.M.; Blotta, M.; Araujo, A.S.; Costa, F.F.; et al. High levels of proinflammatory cytokines IL-6 and IL-8 are associated with a poor clinical outcome in sickle cell anemia. Ann. Hematol. 2020, 99, 947–953. [Google Scholar] [CrossRef]
- Valle Feijóo, M.L.; Bermúdez Sanjurjo, J.R.; González Vázquez, L.; Rey Martínez, M.; de la Fuente Aguado, J. Abdominal pain and syndrome of inappropriate antidiuretic hormone secretion as clinical presentation of acute intermittent porphyria. Rev. Clin. Esp. 2015, 215, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Festuccia, F.; Polci, R.; Pugliese, F.; Gargiulo, A.; Cinotti, G.A.; Menè, P. Syndrome of inappropriate ADH secretion: A late complication of hemopoietic stem cell allograft. G Ital. Nefrol. 2002, 19, 353–360. [Google Scholar] [PubMed]
- Tsutsumi, Y.; Shiratori, S.; Nakata, A.; Kawamura, T.; Mashiko, S.; Ibata, M.; Mori, A.; Tanaka, J.; Asaka, M.; Imamura, M.; et al. Hyponatremia after administration of conditioning regimen in myelodysplastic syndrome with empty sella after glandula pituitaria surgery. Ann. Hematol. 2007, 86, 843–844. [Google Scholar] [CrossRef] [PubMed]
- Azuma, T.; Narumi, H.; Kojima, K.; Nawa, Y.; Hara, M. Hyponatremia during administration of tacrolimus in an allogeneic bone marrow transplant recipient. Int. J. Hematol. 2003, 78, 268–269. [Google Scholar] [CrossRef]
- Suzuki, Y.; Kobayashi, R.; Iguchi, A.; Sato, T.; Kaneda, M.; Kobayashi, K.; Ariga, T. The syndrome of inappropriate secretion of antidiuretic hormone associated with SCT: Clinical differences following SCT using cord blood and BM/peripheral blood. Bone Marrow Transplant. 2008, 42, 743–748. [Google Scholar] [CrossRef] [Green Version]
- Nagler, A.; Bishara, A.; Brautbar, C.; Barak, V. Dysregulation of inflammatory cytokines in unrelated bone marrow transplantation. Cytokines Cell Mol. Ther. 1998, 4, 161–167. [Google Scholar]
- Au, W.Y.; Ma, S.Y.; Cheng, V.C.; Ooi, C.G.; Lie, A.K. Disseminated zoster, hyponatraemia, severe abdominal pain and leukaemia relapse: Recognition of a new clinical quartet after bone marrow transplantation. Br. J. Dermatol. 2003, 149, 862–865. [Google Scholar] [CrossRef]
- McIlwaine, L.M.; Fitzsimons, E.J.; Soutar, R.L. Inappropriate antidiuretic hormone secretion, abdominal pain and disseminated varicella-zoster virus infection: An unusual and fatal triad in a patient 13 months post Rituximab and autologous stem cell transplantation. Clin. Lab. Haematol. 2001, 23, 253–254. [Google Scholar] [CrossRef]
- Szabó, F.; Horvath, N.; Seimon, S.; Hughes, T. Inappropriate antidiuretic hormone secretion, abdominal pain and disseminated varicella-zoster virus infection: An unusual triad in a patient 6 months post mini-allogeneic peripheral stem cell transplant for chronic myeloid leukemia. Bone Marrow Transplant. 2000, 26, 231–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rau, R.; Fitzhugh, C.D.; Baird, K.; Cortez, K.J.; Li, L.; Fischer, S.H.; Cowen, E.W.; Balow, J.E.; Walsh, T.J.; Cohen, J.I.; et al. Triad of severe abdominal pain, inappropriate antidiuretic hormone secretion, and disseminated varicella-zoster virus infection preceding cutaneous manifestations after hematopoietic stem cell transplantation: Utility of PCR for early recognition and therapy. Pediatr. Infect. Dis. J. 2008, 27, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.P.; Welt, L.G.; Sims, E.A.; Orloff, J.; Needham, J. A salt-wasting syndrome associated with cerebral disease. Trans. Assoc. Am. Physicians 1950, 63, 57–64. [Google Scholar] [PubMed]
- Cerda-Esteve, M.; Cuadrado-Godia, E.; Chillaron, J.J.; Pont-Sunyer, C.; Cucurella, G.; Fernandez, M.; Goday, A.; Cano-Perez, J.F.; Rodriguez-Campello, A.; Roquer, J. Cerebral salt wasting syndrome: Review. Eur. J. Intern. Med. 2008, 19, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.C.; Binder, D.K.; Chien, B.; Maisel, A.; Manley, G.T. Cerebral salt wasting and elevated brain natriuretic peptide levels after traumatic brain injury: 2 case reports. Surg. Neurol. 2008, 69, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Orlik, L.; Venzin, R.; Fehr, T.; Hohloch, K. Cerebral salt wasting in a patient with myeloproliferative neoplasm. BMC Neurol. 2019, 19, 169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, Y.J.; Lee, H.Y.; Jung, I.A.; Cho, W.K.; Cho, B.; Suh, B.K. Cerebral salt-wasting syndrome after hematopoietic stem cell transplantation in adolescents: 3 case reports. Ann. Pediatr. Endocrinol. Metab. 2015, 20, 220–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radel, E.G.; Kochen, J.A.; Finberg, L. Hyponatremia in sickle cell disease. A renal salt-losing state. J. Pediatr. 1976, 88, 800–805. [Google Scholar] [CrossRef]
- Della Corte, V.; Tuttolomondo, A.; Pecoraro, R.; Pinto, A. Chronic hyponatremia in a patient with renal salt wasting and without cerebral disease: Relationship between RSW, risk of fractures and cognitive impairment. Intern. Emerg. Med. 2018, 13, 1167–1171. [Google Scholar] [CrossRef]
- Ariizumi, H.; Sasaki, Y.; Harada, H.; Uto, Y.; Azuma, R.; Isobe, T.; Kishimoto, K.; Shiozawa, E.; Takimoto, M.; Ohike, N.; et al. Post-cytokine-release Salt Wasting as Inverse Tumor Lysis Syndrome in a Non-cerebral Natural Killer-cell Neoplasm. Intern. Med. 2017, 56, 1855–1861. [Google Scholar] [CrossRef] [Green Version]
- Cull, E.H.; Watts, J.M.; Tallman, M.S.; Kopp, P.; Frattini, M.; Rapaport, F.; Rampal, R.; Levine, R.; Altman, J.K. Acute myeloid leukemia presenting with panhypopituitarism or diabetes insipidus: A case series with molecular genetic analysis and review of the literature. Leuk. Lymphoma 2014, 55, 2125–2129. [Google Scholar] [CrossRef] [PubMed]
- Zenimaru, Y.; Yamada, M.; Suzuki, J.; Konoshita, T. Hypopituitarism and central diabetes insipidus caused by central nervous system lymphoma. Intern. Med. 2018, 57, 3335–3336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tharaux, P.L.; Hagège, I.; Placier, S.; Vayssairat, M.; Kanfer, A.; Girot, R.; Dussaule, J.C. Urinary endothelin-1 as a marker of renal damage in sickle cell disease. Nephrol. Dial. Transpl. 2005, 20, 2408–2413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carone, F.A.; Epstein, F.H. Nephrogenic diabetes insipidus caused by amyloid disease. Evidence in man of the role of the collecting ducts in concentrating urine. Am. J. Med. 1960, 29, 539–544. [Google Scholar] [CrossRef]
- Liamis, G.; Milionis, H.J.; Elisaf, M. Hyponatremia in patients with infectious diseases. J. Infect. 2011, 63, 327–335. [Google Scholar] [CrossRef]
- Polprasert, C.; Wongjitrat, C.; Wisedopas, N. Case report: Severe CMV colitis in a patient with follicular lymphoma after chemotherapy. J. Med. Assoc. Thail. 2011, 94, 498–500. [Google Scholar]
- Pongtanakul, B.; Narkbunnam, N.; Veerakul, G.; Sanpakit, K.; Viprakasit, V.; Tanphaichitr, V.T.; Suvatte, V. Dengue hemorrhagic fever in patients with thalassemia. J. Med. Assoc. Thai. 2005, 88 (Suppl. 8), S80–S85. [Google Scholar]
- Debuc, B.; Smadja, D.M. Is COVID-19 a new hematologic disease? Stem. Cell Rev. Rep. 2020. [Google Scholar] [CrossRef]
- Berni, A.; Malandrino, D.; Parenti, G.; Maggi, M.; Poggesi, L.; Peri, A. Hyponatremia, IL-6, and SARS-CoV-2 (COVID-19) infection: May all fit together? J. Endocrinol. Invest. 2020. [Google Scholar] [CrossRef]
- Castillo, J.J.; Mull, N.; Reagan, J.L.; Nemr, S.; Mitri, J. Increased incidence of non-Hodgkin lymphoma, leukemia, and myeloma in patients with diabetes mellitus type 2: A meta-analysis of observational studies. Blood 2012, 119, 4845–4850. [Google Scholar] [CrossRef] [Green Version]
- Noetzli, L.J.; Mittelman, S.D.; Watanabe, R.M.; Coates, T.D.; Wood, J.C. Pancreatic iron and glucose dysregulation in thalassemia major. Am. J. Hematol. 2012, 87, 155–160. [Google Scholar] [CrossRef]
- De Sanctis, V.; Soliman, A.T.; Elsedfy, H.; Pepe, A.; Kattamis, C.; El Kholy, M.; Yassin, M. Diabetes and glucose metabolism in thalassemia major: An update. Expert. Rev. Hematol. 2016, 9, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.; DeSanctis, V.; Yassin, M.; Elalaily, R.; Eldarsy, N.E. Continuous glucose monitoring system and new era of early diagnosis of diabetes in high risk groups. Indian J. Endocrinol. Metab. 2014, 18, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Gearhart, M.M.; Parbhoo, S.K. Hyperglycemia in the critically ill patient. AACN Clin. Issues 2006, 17, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Fuji, S.; Loffler, J.; Savani, B.N.; Einsele, H.; Kapp, M. Hyperglycemia as a possible risk factor for mold infections-the potential preventative role of intensified glucose control in allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2017, 52, 657–662. [Google Scholar] [CrossRef] [Green Version]
- Fuji, S.; Rovo, A.; Ohashi, K.; Griffith, M.; Einsele, H.; Kapp, M.; Mohty, M.; Majhail, N.S.; Engelhardt, B.G.; Tichelli, A.; et al. How do I manage hyperglycemia/post-transplant diabetes mellitus after allogeneic HSCT. Bone Marrow Transplant. 2016, 51, 1041–1049. [Google Scholar] [CrossRef] [Green Version]
- DeFilipp, Z.; Duarte, R.F.; Snowden, J.A.; Majhail, N.S.; Greenfield, D.M.; Miranda, J.L.; Arat, M.; Baker, K.S.; Burns, L.J.; Duncan, C.N.; et al. Metabolic syndrome and cardiovascular disease following hematopoietic cell transplantation: Screening and preventive practice recommendations from CIBMTR and EBMT. Bone Marrow Transplant. 2017, 52, 173–182. [Google Scholar] [CrossRef] [Green Version]
- Parthymos, I.; Liamis, G.; Dounousi, E.; Pentheroudakis, G.; Mauri, D.; Zarkavelis, G.; Florentin, M. Metabolic consequences of immune checkpoint inhibitors: A new challenge in clinical practice. Crit. Rev. Oncol. Hematol. 2020, 151, 102979. [Google Scholar] [CrossRef]
- Abdel-Hamid, N.; Jubori, T.A.; Farhan, A.; Mahrous, M.; Gouri, A.; Awad, E.; Breuss, J. Underlying pathways for interferon risk to type II diabetes mellitus. Curr. Diabetes Rev. 2013, 9, 472–477. [Google Scholar] [CrossRef]
- Chiasson, J.L.; Aris-Jilwan, N.; Belanger, R.; Bertrand, S.; Beauregard, H.; Ekoe, J.M.; Fournier, H.; Havrankova, J. Diagnosis and treatment of diabetic ketoacidosis and the hyperglycemic hyperosmolar state. Cmaj 2003, 168, 859–866. [Google Scholar]
- Bustamante, M.; Hasler, U.; Kotova, O.; Chibalin, A.V.; Mordasini, D.; Rousselot, M.; Vandewalle, A.; Martin, P.Y.; Féraille, E. Insulin potentiates AVP-induced AQP2 expression in cultured renal collecting duct principal cells. Am. J. Physiol. Ren. Physiol. 2005, 288, F334–F344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishikawa, S.; Saito, T.; Kasono, K. Pathological role of aquaporin-2 in impaired water excretion and hyponatremia. J. Neuroendocr. 2004, 16, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, S.; Cheesman, E.; Jude, E.B. SIADH and partial hypopituitarism in a patient with intravascular large B-cell lymphoma: A rare cause of a common presentation. BMJ Case Rep. 2013, 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pekic, S.; Milicevic, S.; Colovic, N.; Colovic, M.; Popovic, V. Intravascular large B-cell lymphoma as a cause of hypopituitarism: Gradual and late reversal of hypopituitarism after long-term remission of lymphoma with immunochemotherapy. Endocrine 2008, 34, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.L.; Lu, Z.H.; Mu, Y.M.; Dou, J.T.; Lu, J.M.; Zhong, W.W.; Pan, C.Y. Diffuse large cell non-Hodgkin lymphoma with pituitary and bilateral adrenal involvement. Intern. Med. J. 2012, 42, 329–332. [Google Scholar] [CrossRef] [PubMed]
- An, P.; Chen, K.; Yang, G.Q.; Dou, J.T.; Chen, Y.L.; Jin, X.Y.; Wang, X.L.; Mu, Y.M.; Wang, Q.S. Diffuse large B cell lymphoma with bilateral adrenal and hypothalamic involvement: A case report and literature review. World J. Clin. Cases 2019, 7, 4075–4083. [Google Scholar] [CrossRef] [PubMed]
- Tallis, P.H.; Rushworth, R.L.; Torpy, D.J.; Falhammar, H. Adrenal insufficiency due to bilateral adrenal metastases—A systematic review and meta-analysis. Heliyon 2019, 5, e01783. [Google Scholar] [CrossRef] [Green Version]
- Mendoza, H.; Podoltsev, N.A.; Siddon, A.J.; Gnanapandithan, K. Acute myeloid leukemia presenting as bilateral adrenal hemorrhage. Ann. Hematol. 2019, 98, 2421–2423. [Google Scholar] [CrossRef]
- Yamaguchi, H.; Nakamura, H.; Mamiya, Y.; Yamamoto, Y.; Tajika, K.; Sugihara, H.; Gomi, S.; Inokuchi, K.; Hasegawa, S.; Shibazaki, T.; et al. Acute lymphoblastic leukemia with isolated adrenocorticotropic hormone deficiency. Intern. Med. 1997, 36, 819–821. [Google Scholar] [CrossRef] [Green Version]
- Baldini, M.; Mancarella, M.; Cassinerio, E.; Marcon, A.; Ambrogio, A.G.; Motta, I. Adrenal insufficiency: An emerging challenge in thalassemia? Am. J. Hematol. 2017, 92, E119–E121. [Google Scholar] [CrossRef] [Green Version]
- Sobngwi, E.; Mbango, N.D.; Balti, E.V.; Sack, F.N.; Ama Moor, V.; Mbanya, J.C. Relative adrenal insufficiency in adults with sickle cell disease. Pan. Afr. Med. J. 2018, 29, 30. [Google Scholar] [CrossRef] [PubMed]
- Rensen, N.; Gemke, R.J.; van Dalen, E.C.; Rotteveel, J.; Kaspers, G.J. Hypothalamic-pituitary-adrenal (HPA) axis suppression after treatment with glucocorticoid therapy for childhood acute lymphoblastic leukaemia. Cochrane Database Syst. Rev. 2017, 11, Cd008727. [Google Scholar] [CrossRef] [Green Version]
- Miller, A.; Brooks, L.K.; Poola-Kella, S.; Malek, R. Posaconazole-induced adrenal insufficiency in a case of chronic myelomonocytic leukemia. Case Rep. Endocrinol. 2018, 2018, 2170484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trainer, H.; Hulse, P.; Higham, C.E.; Trainer, P.; Lorigan, P. Hyponatraemia secondary to nivolumab-induced primary adrenal failure. Endocrinol. Diabetes Metab. Case Rep. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Kastrisiou, M.; Kostadima, F.L.; Kefas, A.; Zarkavelis, G.; Kapodistrias, N.; Ntouvelis, E.; Petrakis, D.; Papadaki, A.; Vassou, A.; Pentheroudakis, G. Nivolumab-induced hypothyroidism and selective pituitary insufficiency in a patient with lung adenocarcinoma: A case report and review of the literature. ESMO Open 2017, 2, e000217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Follin, C.; Wiebe, T.; Moëll, C.; Erfurth, E.M. Moderate dose cranial radiotherapy causes central adrenal insufficiency in long-term survivors of childhood leukaemia. Pituitary 2014, 17, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Combs, S.; Berl, T. Dysnatremias in patients with kidney disease. Am. J. Kidney Dis. 2014, 63, 294–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howard, S.C.; McCormick, J.; Pui, C.H.; Buddington, R.K.; Harvey, R.D. Preventing and managing toxicities of high-dose methotrexate. Oncologist 2016, 21, 1471–1482. [Google Scholar] [CrossRef] [Green Version]
- Liamis, G.; Filippatos, T.D.; Elisaf, M.S. Electrolyte disorders associated with the use of anticancer drugs. Eur. J. Pharmacol. 2016, 777, 78–87. [Google Scholar] [CrossRef]
- Malyszko, J.; Kozlowska, K.; Kozlowski, L.; Malyszko, J. Nephrotoxicity of anticancer treatment. Nephrol. Dial. Transpl. 2017, 32, 924–936. [Google Scholar] [CrossRef]
- Li, Y.; Chen, X.; Wang, Y.; Hu, J.; Shen, Z.; Ding, X. Application of group LASSO regression based Bayesian networks in risk factors exploration and disease prediction for acute kidney injury in hospitalized patients with hematologic malignancies. BMC Nephrol. 2020, 21, 162. [Google Scholar] [CrossRef] [PubMed]
- Van Avondt, K.; Nur, E.; Zeerleder, S. Mechanisms of haemolysis-induced kidney injury. Nat. Rev. Nephrol. 2019, 15, 671–692. [Google Scholar] [CrossRef] [PubMed]
- Wanchoo, R.; Bayer, R.L.; Bassil, C.; Jhaveri, K.D. Emerging concepts in hematopoietic stem cell transplantation-associated renal thrombotic microangiopathy and prospects for new treatments. Am. J. Kidney Dis. 2018, 72, 857–865. [Google Scholar] [CrossRef]
- Kemmner, S.; Verbeek, M.; Heemann, U. Renal dysfunction following bone marrow transplantation. J. Nephrol. 2017, 30, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Yadav, P.; Cook, M.; Cockwell, P. Current trends of renal impairment in multiple myeloma. Kidney Dis. 2016, 1, 241–257. [Google Scholar] [CrossRef]
- Hogan, J.J.; Alexander, M.P.; Leung, N. Dysproteinemia and the kidney: Core curriculum 2019. Am. J. Kidney Dis. 2019, 74, 822–836. [Google Scholar] [CrossRef] [Green Version]
- Lommatzsch, S.E.; Bellizzi, A.M.; Cathro, H.P.; Rosner, M.H. Acute renal failure caused by renal infiltration by hematolymphoid malignancy. Ann. Diagn. Pathol. 2006, 10, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Basnayake, K.; Stringer, S.J.; Hutchison, C.A.; Cockwell, P. The biology of immunoglobulin free light chains and kidney injury. Kidney Int. 2011, 79, 1289–1301. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Umakanathan, M.; P’Ng, C.H.; Varikatt, W.; Kwok, F.; Lin, M.W.; Vucak-Dzumhur, M. Cryoglobulinemic glomerulonephritis associated with nodal and renal infiltration by T-Cell lymphoma of T-Follicular helper phenotype: A case report. Am. J. Kidney Dis. 2018, 72, 606–611. [Google Scholar] [CrossRef]
- Walsh, P.R.; Johnson, S. Treatment and management of children with haemolytic uraemic syndrome. Arch. Dis. Child. 2018, 103, 285–291. [Google Scholar] [CrossRef]
- Tsai, H.M. The kidney in thrombotic thrombocytopenic purpura. Minerva Med. 2007, 98, 731–747. [Google Scholar] [PubMed]
- Zafrani, L.; Azoulay, E. Acute renal failure is prevalent in patients with thrombotic thrombocytopenic purpura associated with low plasma ADAMTS13 activity: Reply. J. Thromb. Haemost. 2015, 13, 1526–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kokoris, S.I.; Gavriilaki, E.; Miari, A.; Travlou, A.; Kyriakou, E.; Anagnostopoulos, A.; Grouzi, E. Renal involvement in paroxysmal nocturnal hemoglobinuria: An update on clinical features, pathophysiology and treatment. Hematology 2018, 23, 558–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naik, R.P.; Derebail, V.K. The spectrum of sickle hemoglobin-related nephropathy: From sickle cell disease to sickle trait. Expert Rev. Hematol. 2017, 10, 1087–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kato, G.J.; Piel, F.B.; Reid, C.D.; Gaston, M.H.; Ohene-Frempong, K.; Krishnamurti, L.; Smith, W.R.; Panepinto, J.A.; Weatherall, D.J.; Costa, F.F.; et al. Sickle cell disease. Nat. Rev. Dis. Primers. 2018, 4, 18010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vichinsky, E. Chronic organ failure in adult sickle cell disease. Hematol. Am. Soc. Hematol. Educ. Program. 2017, 2017, 435–439. [Google Scholar] [CrossRef] [Green Version]
- Filippatos, T.D.; Elisaf, M.S. Hyponatremia in patients with heart failure. World J. Cardiol. 2013, 5, 317–328. [Google Scholar] [CrossRef]
- Farmakis, D.; Triposkiadis, F.; Lekakis, J.; Parissis, J. Heart failure in haemoglobinopathies: Pathophysiology, clinical phenotypes, and management. Eur. J. Heart Fail. 2017, 19, 479–489. [Google Scholar] [CrossRef] [Green Version]
- Ocel, J.J.; Edwards, W.D.; Tazelaar, H.D.; Petrovic, L.M.; Edwards, B.S.; Kamath, P.S. Heart and liver disease in 32 patients undergoing biopsy of both organs, with implications for heart or liver transplantation. Mayo Clin. Proc. 2004, 79, 492–501. [Google Scholar] [CrossRef]
- Tukenova, M.; Guibout, C.; Oberlin, O.; Doyon, F.; Mousannif, A.; Haddy, N.; Guerin, S.; Pacquement, H.; Aouba, A.; Hawkins, M.; et al. Role of cancer treatment in long-term overall and cardiovascular mortality after childhood cancer. J. Clin. Oncol. 2010, 28, 1308–1315. [Google Scholar] [CrossRef]
- Zhang, S.; Liu, X.; Bawa-Khalfe, T.; Lu, L.S.; Lyu, Y.L.; Liu, L.F.; Yeh, E.T. Identification of the molecular basis of doxorubicin-induced cardiotoxicity. Nat. Med. 2012, 18, 1639–1642. [Google Scholar] [CrossRef] [PubMed]
- Armenian, S.H.; Gelehrter, S.K.; Vase, T.; Venkatramani, R.; Landier, W.; Wilson, K.D.; Herrera, C.; Reichman, L.; Menteer, J.D.; Mascarenhas, L.; et al. Screening for cardiac dysfunction in anthracycline-exposed childhood cancer survivors. Clin. Cancer Res. 2014, 20, 6314–6323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardinale, D.; Colombo, A.; Bacchiani, G.; Tedeschi, I.; Meroni, C.A.; Veglia, F.; Civelli, M.; Lamantia, G.; Colombo, N.; Curigliano, G.; et al. Early detection of anthracycline cardiotoxicity and improvement with heart failure therapy. Circulation 2015, 131, 1981–1988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhakta, N.; Liu, Q.; Yeo, F.; Baassiri, M.; Ehrhardt, M.J.; Srivastava, D.K.; Metzger, M.L.; Krasin, M.J.; Ness, K.K.; Hudson, M.M.; et al. Cumulative burden of cardiovascular morbidity in paediatric, adolescent, and young adult survivors of Hodgkin’s lymphoma: An analysis from the St Jude Lifetime Cohort Study. Lancet Oncol. 2016, 17, 1325–1334. [Google Scholar] [CrossRef] [Green Version]
- Salz, T.; Zabor, E.C.; de Nully Brown, P.; Dalton, S.O.; Raghunathan, N.J.; Matasar, M.J.; Steingart, R.; Vickers, A.J.; Svenssen Munksgaard, P.; Oeffinger, K.C.; et al. Preexisting cardiovascular risk and subsequent heart failure among non-hodgkin lymphoma survivors. J. Clin. Oncol. 2017, 35, 3837–3843. [Google Scholar] [CrossRef] [PubMed]
- Pai, V.B.; Nahata, M.C. Cardiotoxicity of chemotherapeutic agents: Incidence, treatment and prevention. Drug Saf. 2000, 22, 263–302. [Google Scholar] [CrossRef] [PubMed]
- Labianca, R.; Beretta, G.; Clerici, M.; Fraschini, P.; Luporini, G. Cardiac toxicity of 5-fluorouracil: A study on 1083 patients. Tumori 1982, 68, 505–510. [Google Scholar] [CrossRef]
- Orphanos, G.S.; Ioannidis, G.N.; Ardavanis, A.G. Cardiotoxicity induced by tyrosine kinase inhibitors. Acta Oncol. 2009, 48, 964–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamal, F.A.; Khaled, S.K. The cardiovascular complications of chimeric antigen receptor T cell therapy. Curr. Hematol. Malig. Rep. 2020, 15, 130–132. [Google Scholar] [CrossRef]
- Ganatra, S.; Neilan, T.G. Immune checkpoint inhibitor-associated myocarditis. Oncologist 2018, 23, 879–886. [Google Scholar] [CrossRef] [Green Version]
- Murakami, J.; Shimizu, Y. Hepatic manifestations in hematological disorders. Int. J. Hepatol. 2013, 2013, 484903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wanless, I.R.; Peterson, P.; Das, A.; Boitnott, J.K.; Moore, G.W.; Bernier, V. Hepatic vascular disease and portal hypertension in polycythemia vera and agnogenic myeloid metaplasia: A clinicopathological study of 145 patients examined at autopsy. Hepatology 1990, 12, 1166–1174. [Google Scholar] [CrossRef] [PubMed]
- Jarasvaraparn, C.; Imran, H.; Siddiqui, A.; Wilson, F.; Gremse, D.A. Association of autoimmune hepatitis type 1 in a child with Evans syndrome. World J. Hepatol. 2017, 9, 1008–1012. [Google Scholar] [CrossRef] [PubMed]
- Tomasian, A.; Sandrasegaran, K.; Elsayes, K.M.; Shanbhogue, A.; Shaaban, A.; Menias, C.O. Hematologic malignancies of the liver: Spectrum of disease. Radiographics 2015, 35, 71–86. [Google Scholar] [CrossRef] [PubMed]
- Berghmans, T. Hyponatremia related to medical anticancer treatment. Support Care Cancer 1996, 4, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Hammond, I.W.; Ferguson, J.A.; Kwong, K.; Muniz, E.; Delisle, F. Hyponatremia and syndrome of inappropriate anti-diuretic hormone reported with the use of Vincristine: An over-representation of Asians? Pharmacoepidemiol Drug Saf. 2002, 11, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Ravikumar, T.S.; Grage, T.B. The syndrome of inappropriate ADH secretion secondary to vinblastine-bleomycin therapy. J. Surg. Oncol. 1983, 24, 242–245. [Google Scholar] [CrossRef]
- Moriyama, B.; Henning, S.A.; Leung, J.; Falade-Nwulia, O.; Jarosinski, P.; Penzak, S.R.; Walsh, T.J. Adverse interactions between antifungal azoles and vincristine: Review and analysis of cases. Mycoses 2012, 55, 290–297. [Google Scholar] [CrossRef]
- Kamaluddin, M.; McNally, P.; Breatnach, F.; O’Marcaigh, A.; Webb, D.; O’Dell, E.; Scanlon, P.; Butler, K.; O’Meara, A. Potentiation of vincristine toxicity by itraconazole in children with lymphoid malignancies. Acta Paediatr. 2001, 90, 1204–1207. [Google Scholar] [CrossRef]
- Dixon, B.N.; Daley, R.J.; Buie, L.W.; Hsu, M.; Park, J.H.; Brentjens, R.J.; Purdon, T.J.; Latcha, S. Correlation of IL-6 secretion and hyponatremia with the use of CD19+ chimeric antigen receptor T-cells. Clin. Nephrol. 2020, 93, 42–46. [Google Scholar] [CrossRef]
- Frahm, H.; von Hulst, M. Increased secretion of vasopressin and edema formation in high dosage methotrexate therapy. Z Gesamte Inn. Med. 1988, 43, 411–414. [Google Scholar] [PubMed]
- Lee, Y.C.; Park, J.S.; Lee, C.H.; Bae, S.C.; Kim, I.S.; Kang, C.M.; Kim, G.H. Hyponatraemia induced by low-dose intravenous pulse cyclophosphamide. Nephrol. Dial. Transpl. 2010, 25, 1520–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sweet, K.; Komrokji, R.; Padron, E.; Cubitt, C.L.; Turner, J.G.; Zhou, J.; List, A.F. Phase I clinical trial of selinexor in combination with daunorubicin and cytarabine in previously untreated poor-risk acute myeloid leukemia. Clin. Cancer Res. 2020, 26, 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burger, J.A.; Barr, P.M.; Robak, T.; Owen, C.; Ghia, P. Long-term efficacy and safety of first-line ibrutinib treatment for patients with CLL/SLL: 5 years of follow-up from the phase 3 RESONATE-2 study. Leukemia 2020, 34, 787–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tscherning, C.; Rubie, H.; Chancholle, A.; Claeyssens, S.; Robert, A.; Fabre, J.; Bouissou, F. Recurrent renal salt wasting in a child treated with carboplatin and etoposide. Cancer 1994, 73, 1761–1763. [Google Scholar] [CrossRef]
- Lee, Y.K.; Shin, D.M. Renal salt wasting in patients treated with high-dose cisplatin, etoposide, and mitomycin in patients with advanced non-small cell lung cancer. Korean J. Intern. Med. 1992, 7, 118–121. [Google Scholar] [CrossRef]
- Yamada, Y.; Higuchi, K.; Nishikawa, K.; Gotoh, M.; Fuse, N.; Sugimoto, N.; Nishina, T.; Amagai, K.; Chin, K.; Niwa, Y.; et al. Phase III study comparing oxaliplatin plus S-1 with cisplatin plus S-1 in chemotherapy-naive patients with advanced gastric cancer. Ann. Oncol. 2015, 26, 141–148. [Google Scholar] [CrossRef]
- Arakawa, Y.; Tamura, M.; Sakuyama, T.; Aiba, K.; Eto, S.; Yuda, M.; Tanaka, Y.; Matsumoto, A.; Nishikawa, K. Early measurement of urinary N-acetyl-beta-glucosaminidase helps predict severe hyponatremia associated with cisplatin-containing chemotherapy. J. Infect. Chemother. 2015, 21, 502–506. [Google Scholar] [CrossRef]
- Daphnis, E.; Stylianou, K.; Alexandrakis, M.; Xylouri, I.; Vardaki, E.; Stratigis, S.; Kyriazis, J. Acute renal failure, translocational hyponatremia and hyperkalemia following intravenous immunoglobulin therapy. Nephron. Clin. Pract. 2007, 106, c143–c148. [Google Scholar] [CrossRef]
- Liapis, K.; Apostolidis, J.; Charitaki, E.; Panitsas, F.; Harhalakis, N.; Nikiforakis, E. Syndrome of inappropriate secretion of antidiuretic hormone associated with imatinib. Ann. Pharmacother. 2008, 42, 1882–1886. [Google Scholar] [CrossRef]
- Hill, J.; Shields, J.; Passero, V. Tyrosine kinase inhibitor-associated syndrome of inappropriate secretion of anti-diuretic hormone. J. Oncol. Pharm. Pract. 2016, 22, 729–732. [Google Scholar] [CrossRef] [PubMed]
- Sarret, D.; Le Berre, J.P.; Zemraoui, N. Tramadol-induced hyponatremia. Am. J. Kidney Dis. 2008, 52, 1026. [Google Scholar] [CrossRef] [PubMed]
- Gilbar, P.J.; Richmond, J.; Wood, J.; Sullivan, A. Syndrome of inappropriate antidiuretic hormone secretion induced by a single dose of oral cyclophosphamide. Ann. Pharmacother. 2012, 46, e23. [Google Scholar] [CrossRef]
- Glezerman, I.G. Successful treatment of ifosfamide-induced hyponatremia with AVP receptor antagonist without interruption of hydration for prevention of hemorrhagic cystitis. Ann. Oncol. 2009, 20, 1283–1285. [Google Scholar] [CrossRef] [PubMed]
- Kirch, C.; Gachot, B.; Germann, N.; Blot, F.; Nitenberg, G. Recurrent ifosfamide-induced hyponatraemia. Eur. J. Cancer 1997, 33, 2438–2439. [Google Scholar] [CrossRef]
- Burke, J.M.; Shustov, A.; Essell, J.; Patel-Donnelly, D.; Yang, J.; Chen, R.; Ye, W.; Shi, W.; Assouline, S.; Sharman, J. An open-label, phase ii trial of entospletinib (GS-9973), a selective spleen tyrosine kinase inhibitor, in diffuse large B-cell lymphoma. Clin. Lymphoma Myeloma Leuk. 2018, 18, e327–e331. [Google Scholar] [CrossRef] [Green Version]
- Diskin, C.; Dansby, L.M.; Radcliff, L.; Carter, T.B.; Graves, E.; Graves, A. Recurrent hyponatremia after intrathecal methotrexate not related to antidiuretic hormone: Is a natriuretic peptide activated? Am. J. Med. Sci. 2006, 331, 37–39. [Google Scholar] [CrossRef]
- Sanchez-Fructuoso, A.I.; Santin Cantero, J.M.; Perez Flores, I.; Valero San Cecilio, R.; Calvo Romero, N.; Vilalta Casas, R. Changes in magnesium and potassium homeostasis after conversion from a calcineurin inhibitor regimen to an mTOR inhibitor-based regimen. Transpl. Proc. 2010, 42, 3047–3049. [Google Scholar] [CrossRef]
- O’Brien, S.; Rizzieri, D.A.; Vey, N.; Ravandi, F.; Krug, U.O.; Sekeres, M.A.; Dennis, M.; Venditti, A.; Berry, D.A.; Jacobsen, T.F.; et al. Elacytarabine has single-agent activity in patients with advanced acute myeloid leukaemia. Br. J. Haematol. 2012, 158, 581–588. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, N.; Tani, M.; Tanaka, Y.; Kurata, M.; Matsushita, A.; Maeda, A.; Nagai, K.; Takahashi, T. Severe hyponatremia with consciousness disturbance caused by hydroxyurea in a patient with chronic myeloid leukemia. Rinsho. Ketsueki. 2004, 45, 243–246. [Google Scholar]
- Middleton, G.; Brock, K.; Savage, J.; Mant, R.; Summers, Y.; Connibear, J.; Shah, R.; Ottensmeier, C.; Shaw, P.; Lee, S.M.; et al. Pembrolizumab in patients with non-small-cell lung cancer of performance status 2 (PePS2): A single arm, phase 2 trial. Lancet Respir. Med. 2020. [Google Scholar] [CrossRef]
- Tan, M.H.; Iyengar, R.; Mizokami-Stout, K.; Yentz, S.; MacEachern, M.P.; Shen, L.Y.; Redman, B.; Gianchandani, R. Spectrum of immune checkpoint inhibitors-induced endocrinopathies in cancer patients: A scoping review of case reports. Clin. Diabetes Endocrinol. 2019, 5, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuscano, J.M.; Dutia, M.; Chee, K.; Brunson, A.; Reed-Pease, C.; Abedi, M.; Welborn, J.; O’Donnell, R.T. Lenalidomide plus rituximab can produce durable clinical responses in patients with relapsed or refractory, indolent non-Hodgkin lymphoma. Br. J. Haematol. 2014, 165, 375–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruno, J.J.; Canada, T.W. Possible pentostatin-induced symptomatic hyponatremia. Pharmacotherapy 2007, 27, 164–169. [Google Scholar] [CrossRef]
- de Kort, E.A.; de Lil, H.S.; Bremmers, M.E.J.; van Groningen, L.F.J.; Blijlevens, N.M.A.; Huls, G.; Bruggemann, R.J.M. Cyclosporine a trough concentrations are associated with acute GvHD after non-myeloablative allogeneic hematopoietic cell transplantation. PLoS ONE 2019, 14, e0213913. [Google Scholar] [CrossRef]
- Stoof, S.C.; Cnossen, M.H.; de Maat, M.P.; Leebeek, F.W.; Kruip, M.J. Side effects of desmopressin in patients with bleeding disorders. Haemophilia 2016, 22, 39–45. [Google Scholar] [CrossRef]
- Sharma, R.; Stein, D. Hyponatremia after desmopressin (DDAVP) use in pediatric patients with bleeding disorders undergoing surgeries. J. Pediatr. Hematol. Oncol. 2014, 36, e371–e375. [Google Scholar] [CrossRef] [Green Version]
- O’Connor-Byrne, N.; Glavey, S.; Tudor, R.; Murphy, P.; Thompson, C.J.; Quinn, J. Bortezomib-induced hyponatremia: Tolvaptan therapy permits continuation of lenalidomide, bortezomib and dexamethasone therapy in relapsed myeloma. Exp. Hematol. Oncol. 2019, 8, 4. [Google Scholar] [CrossRef] [Green Version]
- Quesada, J.R.; Talpaz, M.; Rios, A.; Kurzrock, R.; Gutterman, J.U. Clinical toxicity of interferons in cancer patients: A review. J. Clin. Oncol. 1986, 4, 234–243. [Google Scholar] [CrossRef]
- Greenbaum-Lefkoe, B.; Rosenstock, J.G.; Belasco, J.B.; Rohrbaugh, T.M.; Meadows, A.T. Syndrome of inappropriate antidiuretic hormone secretion. A complication of high-dose intravenous melphalan. Cancer 1985, 55, 44–46. [Google Scholar] [CrossRef]
- Singh, T.D.; Fugate, J.E.; Rabinstein, A.A. Central pontine and extrapontine myelinolysis: A systematic review. Eur. J. Neurol. 2014, 21, 1443–1450. [Google Scholar] [CrossRef] [PubMed]
- Maesaka, J.K.; Imbriano, L.; Mattana, J.; Gallagher, D.; Bade, N.; Sharif, S. Differentiating SIADH from cerebral/renal salt wasting: Failure of the volume approach and need for a new approach to hyponatremia. J. Clin. Med. 2014, 3, 1373–1385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonard, J.; Garrett, R.E.; Salottolo, K.; Slone, D.S.; Mains, C.W.; Carrick, M.M.; Bar-Or, D. Cerebral salt wasting after traumatic brain injury: A review of the literature. Scand J. Trauma Resusc. Emerg. Med. 2015, 23, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maesaka, J.K.; Imbriano, L.J.; Miyawaki, N. Determining fractional urate excretion rates in hyponatremic conditions and improved methods to distinguish cerebral/renal salt wasting from the syndrome of inappropriate secretion of antidiuretic hormone. Front. Med. 2018, 5, 319. [Google Scholar] [CrossRef] [PubMed]
- Liamis, G.; Filippatos, T.D.; Liontos, A.; Elisaf, M.S. Management of endocrine disease: Hypothyroidism-associated hyponatremia: Mechanisms, implications and treatment. Eur. J. Endocrinol. 2017, 176, R15–R20. [Google Scholar] [CrossRef] [Green Version]
- Verbalis, J.G.; Goldsmith, S.R.; Greenberg, A.; Korzelius, C.; Schrier, R.W.; Sterns, R.H.; Thompson, C.J. Diagnosis, evaluation, and treatment of hyponatremia: Expert panel recommendations. Am. J. Med. 2013, 126, S1–S42. [Google Scholar] [CrossRef] [PubMed]
- Spasovski, G.; Vanholder, R.; Allolio, B.; Annane, D.; Ball, S.; Bichet, D.; Decaux, G.; Fenske, W.; Hoorn, E.J.; Ichai, C.; et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Nephrol. Dial. Transpl. 2014, 29 (Suppl. 2), i1–i39. [Google Scholar] [CrossRef] [Green Version]
- Filippatos, T.; Elisaf, M. Pharmacological management of hyponatremia. Expert Opin. Pharmacother. 2018, 19, 1337–1344. [Google Scholar] [CrossRef]
- Ayus, J.C.; Caputo, D.; Bazerque, F.; Heguilen, R.; Gonzalez, C.D.; Moritz, M.L. Treatment of hyponatremic encephalopathy with a 3% sodium chloride protocol: A case series. Am. J. Kidney Dis. 2015, 65, 435–442. [Google Scholar] [CrossRef] [Green Version]
- Moritz, M.L.; Ayus, J.C. 100 cc 3% sodium chloride bolus: A novel treatment for hyponatremic encephalopathy. Metab. Brain Dis. 2010, 25, 91–96. [Google Scholar] [CrossRef]
- Liamis, G.; Filippatos, T.D.; Elisaf, M.S. Correction of hypovolemia with crystalloid fluids: Individualizing infusion therapy. Postgrad. Med. 2015, 127, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Seay, N.W.; Lehrich, R.W.; Greenberg, A. Diagnosis and management of disorders of body tonicity-hyponatremia and hypernatremia: Core curriculum 2020. Am. J. Kidney Dis. 2020, 75, 272–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Approach to a patient with hyponatremia (and hematologic disease). * Serum sodium should be corrected for the degree of hyperglycemia. IVIG: Intravenous Immunoglobulin, mOsm: milliosmole, Uosm: urine osmolality.
Figure 1.
Approach to a patient with hyponatremia (and hematologic disease). * Serum sodium should be corrected for the degree of hyperglycemia. IVIG: Intravenous Immunoglobulin, mOsm: milliosmole, Uosm: urine osmolality.

Figure 2.
Approach to a patient with hypotonic hyponatremia, Uosm > 100 mOsm/kg, and hematologic disease. Uosm: urine osmolality, TSH: thyroid-stimulating hormone, CRE: creatinine, COR: cortisol, CSWS: cerebral salt wasting syndrome, SIADH: syndrome of inappropriate antidiuretic hormone secretion, CNS: central nervous system.
Figure 2.
Approach to a patient with hypotonic hyponatremia, Uosm > 100 mOsm/kg, and hematologic disease. Uosm: urine osmolality, TSH: thyroid-stimulating hormone, CRE: creatinine, COR: cortisol, CSWS: cerebral salt wasting syndrome, SIADH: syndrome of inappropriate antidiuretic hormone secretion, CNS: central nervous system.


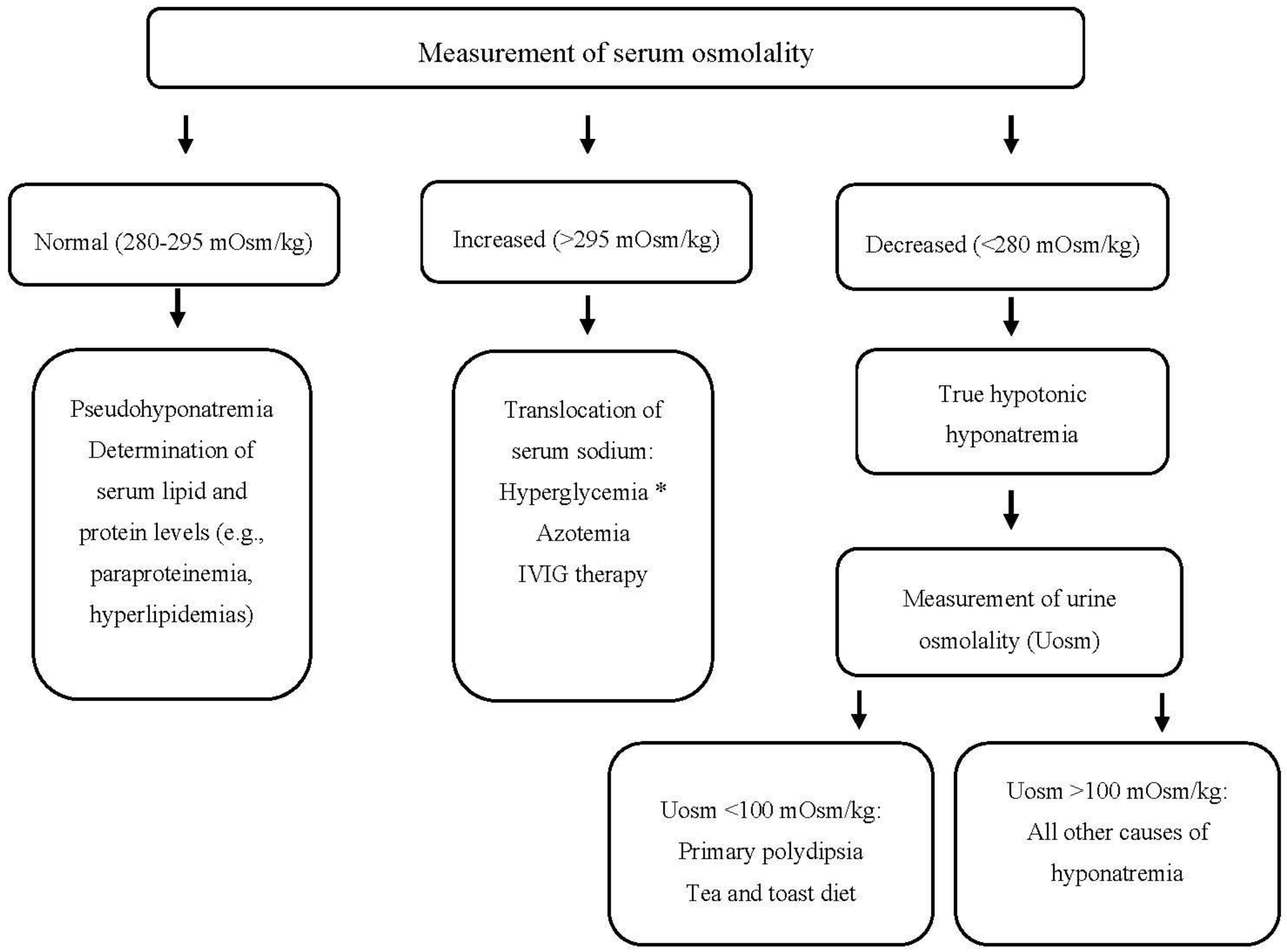{kind=link}
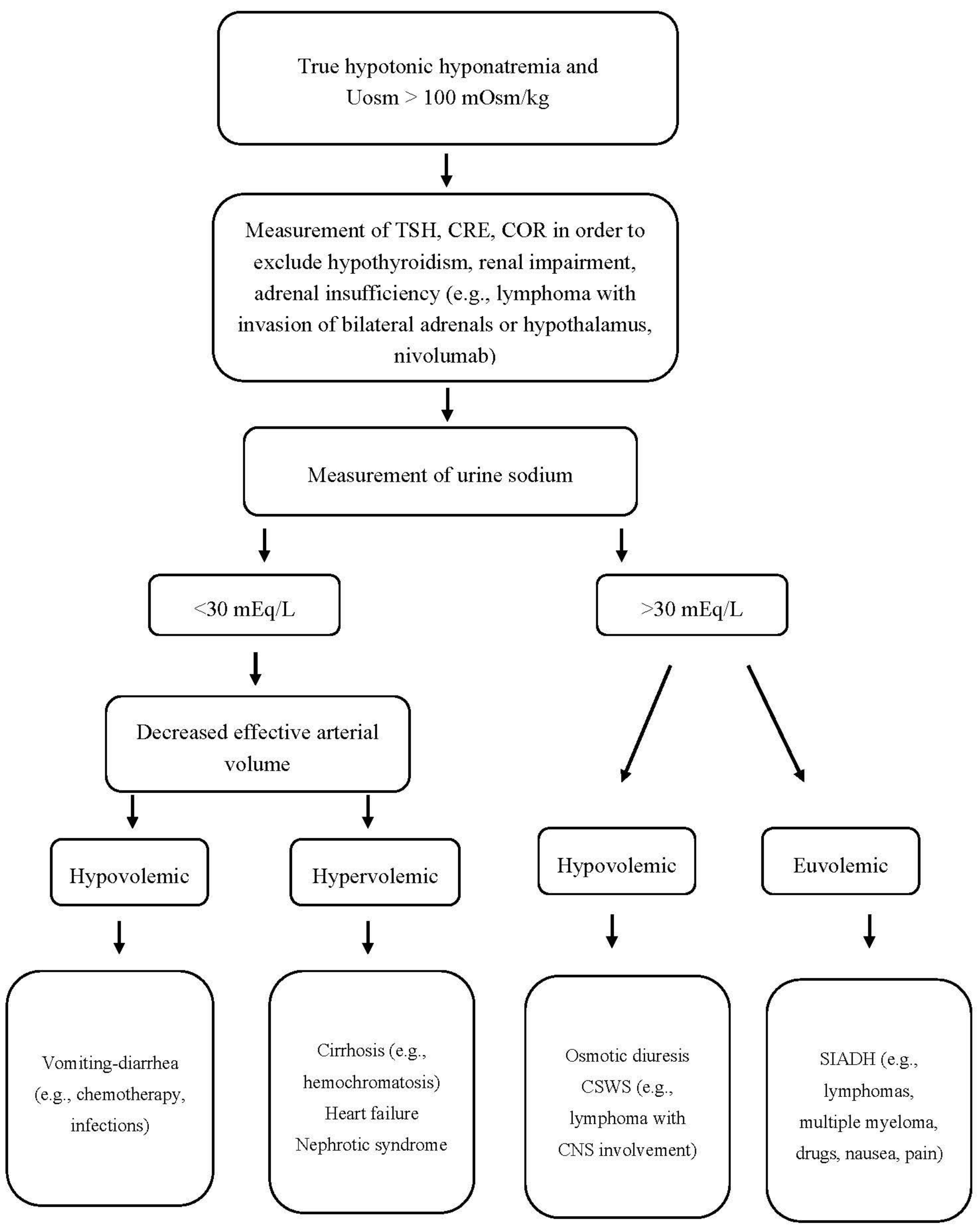{kind=link}
Table 1.
Causes and/or superimposed factors of hyponatremia in hematological patients.
| Type of Hyponatremia | Causes | Associated Conditions |
|---|---|---|
| Pseudohyponatremia (isotonic hyponatremia: serum osmolality 280–295 mOsm/kg) | Hyperglobulinemia | MM, other paraproteinemias, POEMS syndrome, Castleman’s disease, post-transplant monoclonal gammopathies, NHL, CLL, cryoglobulinemia, cold agglutinin disease, Gaucher disease, HCV or HIV infection, cirrhosis drugs: IVIG, interferon. |
| Hypertriglyceridemia | HLH, uncontrolled diabetes mellitus drugs: L-asparaginase, ATRA. Interferon. | |
| Hypercholesterolemia | Allogeneic stem cell transplantation, MM, NHL. | |
| Mixed dyslipidemia | Nephrotic syndrome (secondary causes include: HL, monoclonal gammopathy, cryoglobulinemia, POEMS syndrome, leukemia, glycogen storage diseases, sickle cell disease, MDS, GVHD, infections). | |
| Hypertonic hyponatremia: (serum osmolality >295 mOsm/kg) | Hyperglycemia | Diabetes mellitus: preexisting or related to hemochromatosis, thalassemia, and HSCT. Infections. Drugs: glucocorticoids, interferon, tacrolimus, immune checkpoint inhibitors. |
| Hypotonic hyponatremia (serum osmolality <280 mOsm/kg) | Hypervolemic (edematous hyponatremia) | Cirrhosis. Nephrotic syndrome. Renal insufficiency: chemotherapy, contrast media, NSAIDs, infections, post-HSCT, PNH, sickle cell disease and other hemoglobinopathies, MM, lymphomas, paraproteinemia, TTP, HUS, TLS Heart failure: cardiomyopathy due to hemochromatosis, hemoglobinopathies, amyloidosis, or paraproteinemias. Drug-induced heart failure (e.g., anthracyclines, alkylating agents, fluopyrimidines, TKIs), CAR T- cell therapy, thoracic radiation therapy, immune checkpoint inhibitors-induced myocarditis. POEMS syndrome. (Extravascular volume overload is among the minor criteria of the syndrome). |
| Euvolemic hyponatremia | SIADH: lymphomas, paraproteinemias, HLH, post-HSCT, sickle cell disease, porphyria. Pain and nausea. Pulmonary and CNS infections. Drugs: vinca alkaloids, cyclophosphamide, platinum compound drugs, melphalan, busulfan, interferon, bortezomib, TKIs, methotrexate, tacrolimus, cyclosporine A, CAR T-cells therapy, carbamazepine, SSRIs. | |
| Hypovolemic hyponatremia | Adrenal insufficiency: adrenal metastases or CNS invasion by lymphomas, AML, ALL, hemoglobinopathies. Infections: CNS infections (e.g., tuberculosis), systemic fungal infections. Bilateral cranial radiation therapy. Drugs: steroids, immune checkpoint inhibitors. Extra-renal salt loss: infection mediated. Renal salt loss: myeloproliferative diseases, LAHS, sickle cell disease. Post-HSCT with CNS complications. Drugs: methotrexate, hydroxyurea, platinum compounds, etc. Adrenal hemorrhage: e.g., coagulopathy. |
ALL: acute lymphoblastic leukemia, ATRA: all trans retinoic acid, AML: acute myeloid leukemia, CAR: chimeric antigen receptor, CML: chronic myeloid leukemia, CLL: chronic lymphocytic leukemia, CNS: central nervous system, GVHD: graft versus host disease, HCV: hepatitis C virus, HIV: human immunodeficiency virus, HL: Hodgkin’s lymphoma, HLH: hemophagocytic lymphohistiocytosis, HSCT: hematopoietic stem cell transplantation, HUS: hemolytic uremic syndrome, IVIG: intravenous immunoglobulin, LAHS: lymphoma-associated hemophagocytic syndrome, MDS: myelodysplastic syndrome, MM: multiple myeloma, NHL: non Hodgkin, POEMS: polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes, SSRIs: selective serotonin reuptake inhibitors.
Table 2.
Drugs used in clinical hematology and associated underlying mechanisms for hyponatremia.
| Drug | Disease | Mechanism |
|---|---|---|
| Cyclophosphamide, ifosfamide [152,163,164,165] | Multiple myeloma, lymphomas | SIADH, hypotonic fluids to prevent hemorrhagic cystitis |
| Imatinib and other TKIs [160,161] | CML, ALL | SIADH |
| Entospletinib [166] | In development | SIADH |
| Vincristine [145,146,147] | Lymphomas, ALL | SIADH |
| Methotrexate [167] | Lymphomas, ALL | SIADH and CSWS |
| mTOR inhibitors (everolimus) [168] | In development | Aldosterone resistance |
| Tacrolimus [56] | Post AlloSCT | SIADH |
| Selinexor [153] | In development | Unknown |
| Cytarabine, Elacytarabine [169] | Lymphomatous meningitis, AML | Unknown |
| Hydroxyurea [170] | Myeloproliferative neoplasms, sickle cell disease | CSWS |
| Ibrutinib [154] | CLL, mantle cell lymphoma, Waldenstöm’s macroglobulinemia | Unknown |
| Nivolumab, Pembrolizumab [104,171,172] | Hodgkin lymphoma | Primary adrenal insufficiency, Diabetes mellitus |
| Rituximab plus lenalidomide [173] | Follicular lymphoma | Unknown |
| Pentostatin [174] | HCL | Unknown |
| Cyclosporine A [175] | Immunosuppression post AlloSCT | SIADH |
| Desmopressin [176,177] | Bleeding disorders | Unknown |
| Intravenous immunoglobulin (IVIG) [159] | ITP | Translocational effect of the osmotic load of sucrose and IVIG nephropathy |
| Bortezomib [178] | Multiple myeloma | SIADH |
| CD19+ chimeric antigen receptor (CAR) T-cells [150] | ALL, DLBCL, PMBCL | Elevated IL-6→ SIADH |
| Platinum compounds (cisplatin, carboplatin, oxaliplatin) [145,155,156] | Relapsed or refractory lymphomas | SIADH, CSWS, hypotonic fluids |
| Interferon [179] | HCL, CML, multiple myeloma, follicular lymphoma | SIADH |
| Melphalan [180] | Multiple myeloma | SIADH |
| Busulfan [109] | Prior to SCT | SIADH |
ALL: acute lymphocytic leukemia, AlloSCT: allogeneic stem cell transplantation, AML: acute myeloid leukemia, CML: chronic myeloid leukemia, CLL: chronic lymphocytic leukemia, CSWS: cerebral salt wasting syndrome, DLBCL: diffuse large B-cell lymphoma, HCL: hairy cell leukemia, ITP: immune thrombocytopenia mTOR: mammalian target of rapamycin, PMBCL: primary mediastinal B-cell lymphoma SIADH: syndrome of inappropriate secretion of antidiuretic hormone, TKIs: tyrosine kinase inhibitors.
Table 3.
Basic principles of hyponatremia management.
|
|
|
|
|
|
CSWS: cerebral salt wasting syndrome, h: hours, ODS: osmotic demyelination syndrome, SIADH: syndrome of inappropriate secretion of antidiuretic hormone.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Koumpis, E.; Florentin, M.; Hatzimichael, E.; Liamis, G. Hyponatremia in Patients with Hematologic Diseases. J. Clin. Med. 2020, 9, 3721. https://doi.org/10.3390/jcm9113721
AMA Style
Koumpis E, Florentin M, Hatzimichael E, Liamis G. Hyponatremia in Patients with Hematologic Diseases. Journal of Clinical Medicine. 2020; 9(11):3721. https://doi.org/10.3390/jcm9113721
Chicago/Turabian StyleKoumpis, Epameinondas, Matilda Florentin, Eleftheria Hatzimichael, and George Liamis. 2020. "Hyponatremia in Patients with Hematologic Diseases" Journal of Clinical Medicine 9, no. 11: 3721. https://doi.org/10.3390/jcm9113721
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.