The Burden of Associated Comorbidities in Patients with Obstructive Sleep Apnea—Regional Differences in Two Central–Eastern European Sleep Centers

 ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Subjects and Design
2.2. Sleep Studies
2.3. Statistical Analyses
3. Results
3.1. Bivariate Analysis of Factors Associated with the Prevalence of Each Comorbidity
3.2. Comparative Analysis of Demographic and Clinical Characteristics of Patients from Hungary and Romania
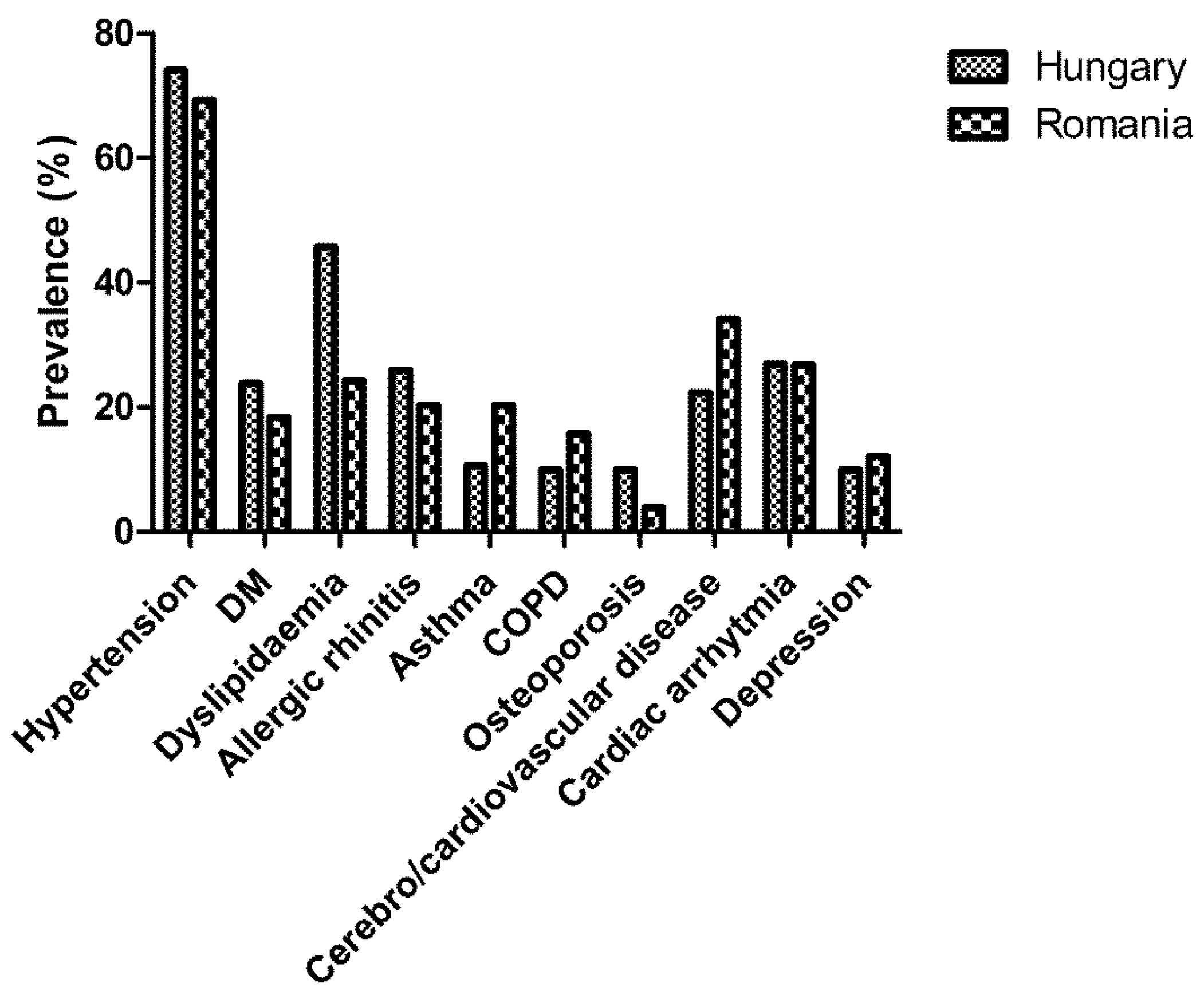
3.3. Comparison of the Prevalence of Comorbidities between Hungarian and Romanian Cohort
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.-L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [Green Version]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drager, L.F.; Togeiro, S.M.; Polotsky, V.Y.; Lorenzi-Filho, G. Obstructive sleep apnea: A cardiometabolic risk in obesity and the metabolic syndrome. J. Am. Coll. Cardiol. 2013, 62, 569–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayley, A.C.; Williams, L.J.; Venugopal, K.; Kennedy, G.A.; Berk, M.; Pasco, J.A. The relationships between insomnia, sleep apnoea and depression: Findings from the American National Health and Nutrition Examination Survey, 2005–2008. Aust. N. Z. J. Psychiatry 2015, 49, 156–170. [Google Scholar] [CrossRef] [PubMed]
- Bikov, A.; Losonczy, G.; Kunos, L. Role of lung volume and airway inflammation in obstructive sleep apnea. Respir. Investig. 2017, 55, 326–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collen, J.; Lettieri, C.; Wickwire, E.; Holley, A. Obstructive sleep apnea and cardiovascular disease, a story of confounders! Sleep Breath. 2020. [Google Scholar] [CrossRef] [PubMed]
- Mokhlesi, B.; Ham, S.A.; Gozal, D. The effect of sex and age on the comorbidity burden of OSA: An observational analysis from a large nationwide US health claims database. Eur. Respir. J. 2016, 47, 1162–1169. [Google Scholar] [CrossRef]
- Greenberg, H.; Fleischman, J.; Gouda, H.E.; De La Cruz, A.E.; Lopez, R.; Mrejen, K.; Web, A.; Feinsilver, S. Disparities in obstructive sleep apnea and its management between a minority-serving institution and a voluntary hospital. Sleep Breath. 2004, 8, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Meszaros, M.; Tarnoki, A.D.; Tarnoki, D.L.; Kovacs, D.T.; Forgo, B.; Lee, J.; Sung, J.; Vestbo, J.; Müller, V.; Kunos, L.; et al. Obstructive sleep apnea and hypertriglyceridaemia share common genetic background: Results of a twin study. J. Sleep Res. 2020, e12979. [Google Scholar] [CrossRef] [Green Version]
- Fietze, I.; Laharnar, N.; Obst, A.; Ewert, R.; Felix, S.B.; Garcia, C.; Gläser, S.; Glos, M.; Schmidt, C.O.; Stubbe, B.; et al. Prevalence and association analysis of obstructive sleep apnea with gender and age differences—Results of SHIP-Trend. J. Sleep Res. 2019, 28, e12770. [Google Scholar] [CrossRef]
- Petrov, I.; Dumitrescu, A.; Snejdrlova, M.; Zafrir, B.; Wożakowska-Kapłon, B.; Fabryova, L.; Pintarić, H.; Bridges, I.; Petkova, R. Clinical management of high and very high risk patients with hyperlipidaemia in Central and Eastern Europe: An observational study. Adv. Ther. 2019, 36, 608–620. [Google Scholar] [CrossRef] [Green Version]
- Müller-Nordhorn, J.; Holmberg, C.; Dokova, K.G.; Milevska-Kostova, N.; Chicin, G.; Ulrichs, T.; Rechel, B.; Willich, S.N.; Powles, J.; Tinnemann, P. Perceived challenges to public health in Central and Eastern Europe: A qualitative analysis. BMC Public Health 2012, 12, 311. [Google Scholar] [CrossRef] [Green Version]
- Kushida, C.A.; Littner, M.R.; Morgenthaler, T.; Alessi, C.A.; Bailey, D.; Coleman, J., Jr.; Friedman, L.; Hirshkowitz, M.; Kapen, S.; Kramer, M.; et al. Practice parameters for the indications for polysomnography and related procedures: An update for 2005. Sleep 2005, 28, 499–521. [Google Scholar] [CrossRef] [Green Version]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM manual for the scoring of sleep and associated events. deliberations of the sleep apnea definitions task force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [Green Version]
- Sforza, E.; Thomas, T.; Barthélémy, J.C.; Collet, P.; Roche, F. Obstructive sleep apnea is associated with preserved bone mineral density in healthy elderly subjects. Sleep 2013, 36, 1509–1515. [Google Scholar]
- Gileles-Hillel, A.; Kheirandish-Gozal, L.; Gozal, D. Biological plausibility linking sleep apnoea and metabolic dysfunction. Nat. Rev. Endocrinol. 2016, 12, 290–298. [Google Scholar] [CrossRef]
- McNicholas, W.T. Comorbid obstructive sleep apnoea and chronic obstructive pulmonary disease and the risk of cardiovascular disease. J. Thorac. Dis. 2018, 10 (Suppl. 34), S4253–S4261. [Google Scholar] [CrossRef]
- Kunos, L.; Lazar, Z.; Martinovszky, F.; Tarnoki, A.D.; Tarnoki, D.L.; Kovacs, D.; Forgo, B.; Horvath, P.; Losonczy, G.; Bikov, A. Overnight changes in lung function of obese patients with obstructive sleep apnoea. Lung 2017, 195, 127–133. [Google Scholar] [CrossRef] [Green Version]
- Zheng, M.; Wang, X.; Zhang, L. Association between allergic and nonallergic rhinitis and obstructive sleep apnea. Curr. Opin. Allergy Clin. Immunol. 2018, 18, 16–25. [Google Scholar] [CrossRef]
- Tiotiu, A.; Plavec, D.; Novakova, S.; Mihaicuta, S.; Novakova, P.; Labor, M.; Bikov, A. Current opinions for the management of asthma associated with ear, nose and throat comorbidities. Eur. Respir. Rev. 2018, 27, 180056. [Google Scholar] [CrossRef]
- Varga, A.W.; Mokhlesi, B. REM obstructive sleep apnea: Risk for adverse health outcomes and novel treatments. Sleep Breath. 2019, 23, 413–423. [Google Scholar] [CrossRef]
- Aurora, R.N.; Crainiceanu, C.; Gottlieb, D.J.; Kim, J.S.; Punjabi, N.M. Obstructive sleep apnea during REM sleep and cardiovascular disease. Am. J. Respir. Crit. Care Med. 2018, 197, 653–660. [Google Scholar] [CrossRef]
- Grimaldi, D.; Beccuti, G.; Touma, C.; Van Cauter, E.; Mokhlesi, B. Association of obstructive sleep apnea in rapid eye movement sleep with reduced glycemic control in type 2 diabetes: Therapeutic implications. Diabetes Care 2014, 37, 355–363. [Google Scholar] [CrossRef] [Green Version]
- Bikov, A.; Lazar, Z.; Horvath, P.; Tarnoki, D.L.; Tarnoki, A.D.; Fesus, L.; Horvath, M.; Meszaros, M.; Losonczy, G.; Kunos, L. Association between serum lipid profile and obstructive respiratory events during REM and non-REM sleep. Lung 2019, 197, 443–450. [Google Scholar] [CrossRef] [Green Version]
- Hedner, J.; Grote, L.; Bonsignore, M.; McNicholas, W.; Lavie, P.; Parati, G.; Sliwinski, P.; Barbé, F.; De Backer, W.; Escourrou, P.; et al. The European Sleep Apnoea Database (ESADA): Report from 22 European sleep laboratories. Eur. Respir. J. 2011, 38, 635–642. [Google Scholar] [CrossRef] [Green Version]
- Roche, F.; Sforza, E.; Pichot, V.; Maudoux, D.; Garcin, A.; Celle, S.; Picard-Kossovsky, M.; Gaspoz, J.M.; Barthélémy, J.C.; PROOF Study Group. Obstructive sleep apnoea/hypopnea influences high-density lipoprotein cholesterol in the elderly. Sleep Med. 2009, 10, 882–886. [Google Scholar] [CrossRef]
- Gunduz, C.; Basoglu, O.K.; Hedner, J.; Zou, D.; Bonsignore, M.R.; Hein, H.; Staats, R.; Pataka, A.; Barbe, F.; Sliwinski, P.; et al. Obstructive sleep apnoea independently predicts lipid levels: Data from the European Sleep Apnea Database. Respirology 2018, 23, 1180–1189. [Google Scholar] [CrossRef] [Green Version]
- Cocoş, R.; Schipor, S.; Hervella, M.; Cianga, P.; Popescu, R.; Bănescu, C.; Constantinescu, M.; Martinescu, A.; Raicu, F. Genetic affinities among the historical provinces of Romania and Central Europe as revealed by an mtDNA analysis. BMC Genet. 2017, 18, 20. [Google Scholar] [CrossRef] [Green Version]
- Lai, C.K.; Beasley, R.; Crane, J.; Foliaki, S.; Shah, J.; Weiland, S. Global variation in the prevalence and severity of asthma symptoms: Phase three of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax 2009, 64, 476–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Townsend, N.; Wilson, L.; Bhatnagar, P.; Wickramasinghe, K.; Rayner, M.; Nichols, M. Cardiovascular disease in Europe: Epidemiological update 2016. Eur. Heart J. 2016, 37, 3232–3245. [Google Scholar] [CrossRef]
- Movsisyan, N.K.; Vinciguerra, M.; Medina-Inojosa, J.R.; Lopez-Jimenez, F. Cardiovascular diseases in Central and Eastern Europe: A call for more surveillance and evidence-based health promotion. Ann. Glob. Health 2020, 86, 21. [Google Scholar] [CrossRef]
- Namen, A.M.; Dunagan, D.P.; Fleischer, A.; Tillett, J.; Barnett, M.; McCall, W.V.; Haponik, E.F. Increased physician-reported sleep apnea: The national ambulatory medical care survey. Chest 2002, 121, 1741–1747. [Google Scholar] [CrossRef] [Green Version]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; et al. Executive summary: Heart disease and stroke statistics—2016 update: A report from the American Heart Association. Circulation 2016, 133, 447–454. [Google Scholar] [CrossRef]
- Bikov, A.; Kolossvary, M.; Jermendy, A.L.; Drobni, Z.D.; Tarnoki, A.D.; Tarnoki, D.L.; Forgó, B.; Kovacs, D.T.; Losonczy, G.; Kunos, L.; et al. Comprehensive coronary plaque assessment in patients with obstructive sleep apnea. J. Sleep Res. 2019, 28, e12828. [Google Scholar] [CrossRef]
- Kapur, V.K.; Auckley, D.H.; Susmita Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical practice guideline for diagnostic Testing for adult obstructive sleep apnea: An American Academy of Sleep Medicine clinical practice guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- Alshaer, H.; Ryan, C.; Fernie, G.R.; Bradley, T.D. Reproducibility and predictors of the apnea hypopnea index across multiple nights. Sleep Sci. 2018, 11, 28–33. [Google Scholar] [CrossRef]


{kind=link}
| Hypertension | Diabetes | Dyslipidemia | COPD | Allergic Rhinitis | Asthma | Cerebro-/Cardiovascular Disease | Arrhythmia | Osteoporosis | Depression | |
|---|---|---|---|---|---|---|---|---|---|---|
| Age | 0.078 | 0.051 | 0.036 | 0.018 | −0.032 | −0.019 | 0.071 | 0.055 | 0.110 | 0.018 |
| Gender (male) | 0.480 | 0.591 | 0.318 | −0.870 | 0.010 | 0.542 | 0.020 | 0.474 | 2.203 | 0.738 |
| BMI | 0.118 | 0.076 | 0.039 | 0.059 | −0.015 | −0.001 | 0.034 | 0.042 | −0.097 | 0.010 |
| History of smoking | 0.129 | −0.096 | −0.170 | 2.536 | −0.113 | −0.752 | 0.304 | −0.091 | −1.171 | −0.231 |
| PY | 0.016 | 0.012 | 0.003 | 0.089 | −0.019 | −0.026 | 0.022 | 0.010 | −0.041 | 0.001 |
| Hypertension | - | 1.637 | 1.210 | 1.677 | −0.824 | −1.022 | 1.925 | 1.417 | 0.333 | 0.218 |
| Diabetes | 1.637 | - | 1.459 | 0.506 | −0.526 | 0.058 | 1.040 | 0.539 | 0.390 | −0.291 |
| Dyslipidemia | 1.210 | 1.459 | - | 0.558 | −0.380 | −0.343 | 0.952 | 0.611 | 0.582 | 0.192 |
| COPD | 1.677 | 0.506 | 0.558 | - | −2.134 | −1.067 | 1.212 | 0.993 | −0.308 | −0.634 |
| Allergic rhinitis | −0.824 | −0.526 | −0.380 | −2.134 | - | 1.005 | −0.529 | −0.487 | 0.393 | −0.196 |
| Asthma | −1.022 | 0.058 | −0.343 | −1.067 | 1.005 | - | −0.419 | −0.403 | 0.486 | −0.160 |
| Cerebro-/cardiovascular disease | 1.925 | 1.040 | 0.952 | 1.212 | −0.529 | −0.419 | - | 1.276 | 0.206 | 0.363 |
| Arrhythmia | 0.270 | 0.539 | 0.611 | 0.993 | −0.487 | −0.403 | 1.276 | - | 0.758 | 0.132 |
| Osteoporosis | 0.333 | 0.390 | 0.582 | −0.308 | 0.393 | 0.486 | 0.206 | 0.758 | - | 0.936 |
| Depression | 0.218 | −0.291 | 0.192 | −0.634 | −0.196 | −0.160 | 0.363 | 0.132 | 0.936 | - |
| Hypertension | Diabetes | Dyslipidemia | COPD | Allergic Rhinitis | Asthma | Cerebro-/Cardiovascular Disease | Arrhythmia | Osteoporosis | Depression | |
|---|---|---|---|---|---|---|---|---|---|---|
| AHI | 0.010 | 0.010 | −0.004 | 0.015 | −0.001 | 0.003 | 0.009 | 0.011 | −0.021 | −0.007 |
| AHIREM | 0.000 | 0.000 | 0.000 | 0.000 | −0.005 | 0.000 | 0.000 | 0.000 | −0.018 | 0.000 |
| AHINREM | 0.011 | 0.015 | −0.002 | 0.015 | −0.004 | 0.004 | 0.012 | 0.009 | −0.019 | −0.004 |
| ODI | 0.012 | 0.010 | −0.003 | 0.015 | −0.002 | 0.003 | 0.010 | 0.012 | −0.022 | −0.005 |
| TST90% | 0.004 | 0.005 | 0.000 | 0.007 | −0.001 | 0.001 | 0.005 | 0.005 | 0.000 | 0.000 |
| MinSatO2 | −0.047 | −0.040 | −0.011 | −0.044 | 0.029 | −0.003 | −0.026 | −0.033 | 0.004 | 0.016 |
| AI | 0.003 | 0.005 | 0.007 | 0.006 | 0.003 | −0.011 | 0.002 | 0.008 | 0.018 | −0.048 |
| ESS | 0.018 | 0.041 | 0.000 | 0.088 | −0.001 | 0.029 | 0.067 | 0.019 | −0.053 | 0.028 |
| Hungary (n = 282) | Romania (n = 306) | p | |
|---|---|---|---|
| Age | 59 /48–67/ | 52 /44–58/ | <0.01 |
| Gender (male%) | 66.3 | 71.6 | 0.17 |
| BMI | 32.1 /17.3–37.3/ | 32.2 /29.0–35.9/ | 0.72 |
| Smoking status (ever/never) | 120/162 | 154/152 | 0.06 |
| Smoking status (current/ex/never) | 79/41/162 | 91/63/152 | 0.09 |
| Cigarette pack years | 0 /0–12/ | 0 /0–19/ | 0.02 |
| ESS | 6 /3–9/ | 10 /6–13/ | <0.01 |
| TST | 415 /380–445/ * | 421 /360–466/ | 0.26 |
| SPT | 449 /413–483/ * | 479 /443–512/ | <0.01 |
| Sleep% | 95 /89–97/ * | 90 /79–96/ | <0.01 |
| REM% | 16.4 /12.0–21.2/ * | 14.9 /11.5–20.1/ | 0.32 |
| AHI | 22.7 /12.2–42.4/ | 39.3 /23.6–63.3/ | <0.01 |
| AHIREM | 24.6 /11.8–46.2/ * | 41.1 /23.9–62.3/ | <0.01 |
| AHINREM | 16.7 /9.6–30.9/ * | 38.6 /22.5–62.2/ | <0.01 |
| ODI | 19.35 /9.4–35.8/ | 38.0 /22.0–61.3/ | <0.01 |
| TST90% | 4.2 /0.7–13.8/ | 13.0 /3.0–52.5/ | <0.01 |
| MinSatO2 | 83 /76–86/ | 81 /72–87/ | 0.08 |
| AI | 43.4 /29.6–59.4/ * | 18.3 /11.2–26.5/ | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bikov, A.; Frent, S.; Pleava, R.; Kunos, L.; Bokhari, S.; Meszaros, M.; Mihaicuta, S. The Burden of Associated Comorbidities in Patients with Obstructive Sleep Apnea—Regional Differences in Two Central–Eastern European Sleep Centers. J. Clin. Med. 2020, 9, 3583. https://doi.org/10.3390/jcm9113583
Bikov A, Frent S, Pleava R, Kunos L, Bokhari S, Meszaros M, Mihaicuta S. The Burden of Associated Comorbidities in Patients with Obstructive Sleep Apnea—Regional Differences in Two Central–Eastern European Sleep Centers. Journal of Clinical Medicine. 2020; 9(11):3583. https://doi.org/10.3390/jcm9113583
Chicago/Turabian StyleBikov, Andras, Stefan Frent, Roxana Pleava, Laszlo Kunos, Saba Bokhari, Martina Meszaros, and Stefan Mihaicuta. 2020. "The Burden of Associated Comorbidities in Patients with Obstructive Sleep Apnea—Regional Differences in Two Central–Eastern European Sleep Centers" Journal of Clinical Medicine 9, no. 11: 3583. https://doi.org/10.3390/jcm9113583