Identification of Acupoint Indication from Reverse Inference: Data Mining of Randomized Controlled Clinical Trials


Abstract
:1. Introduction
2. Methods
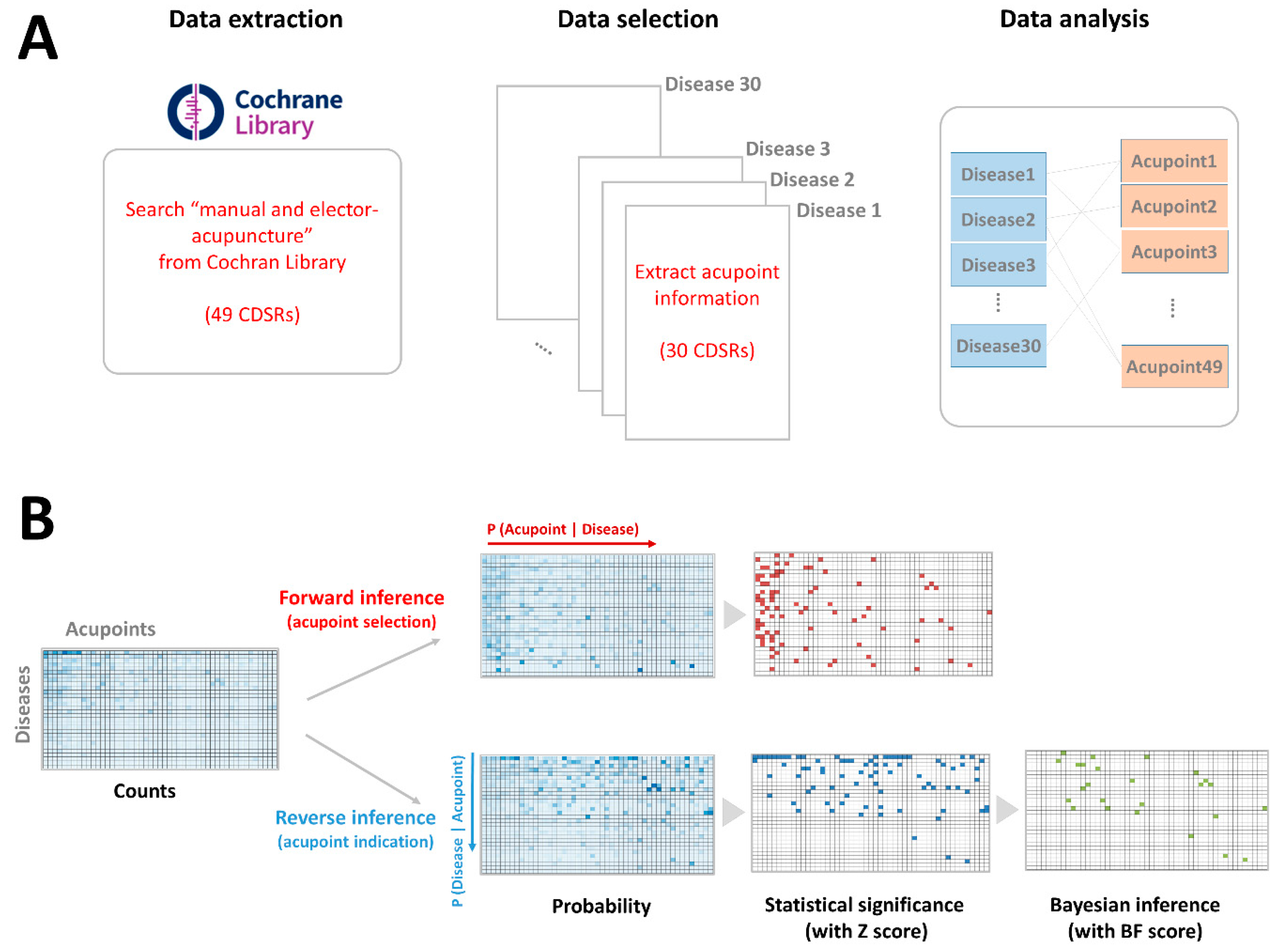
2.1. Data Extraction Process
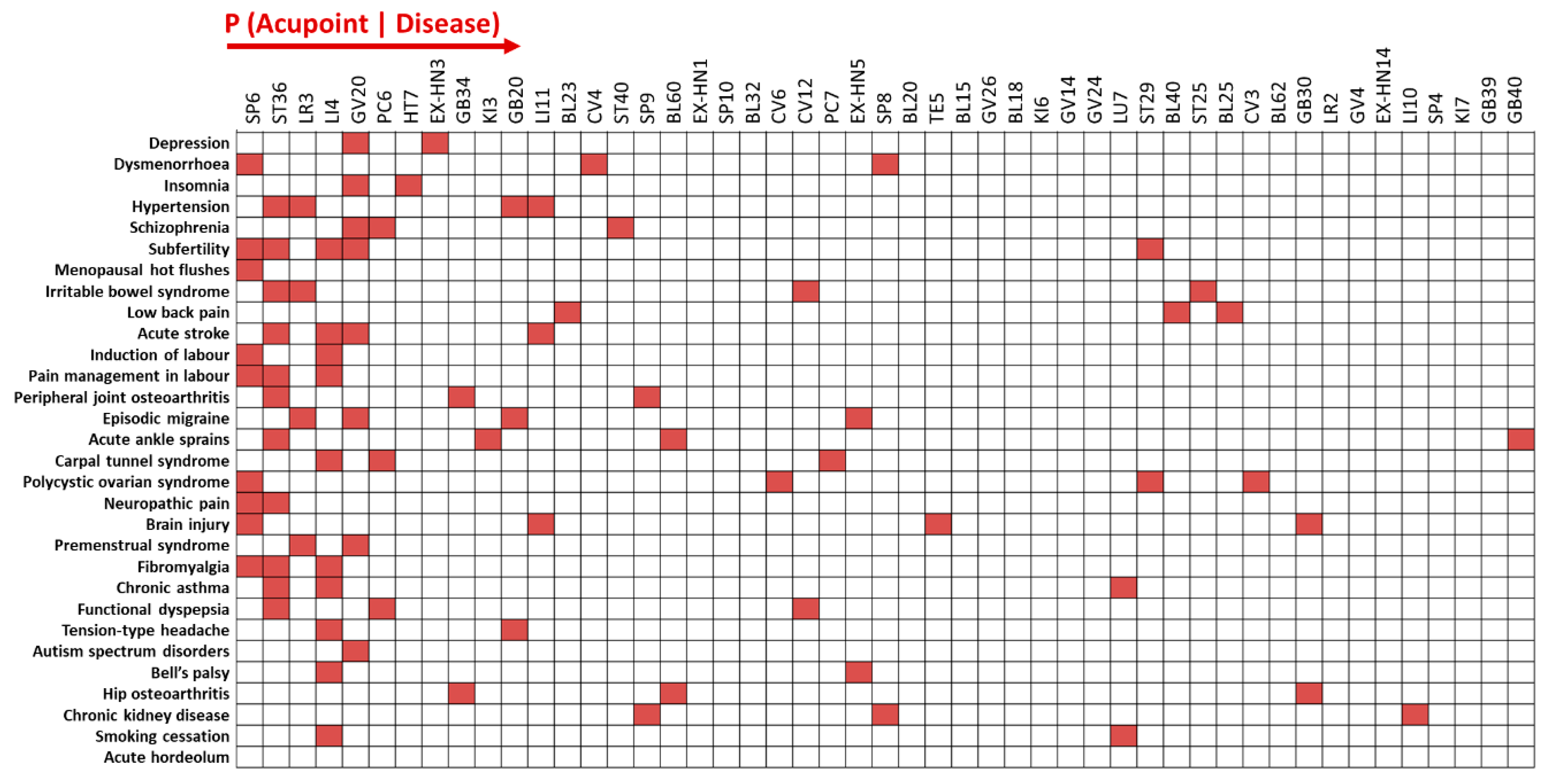
2.2. Data Analysis of Acupoint Selection Using Forward Inference
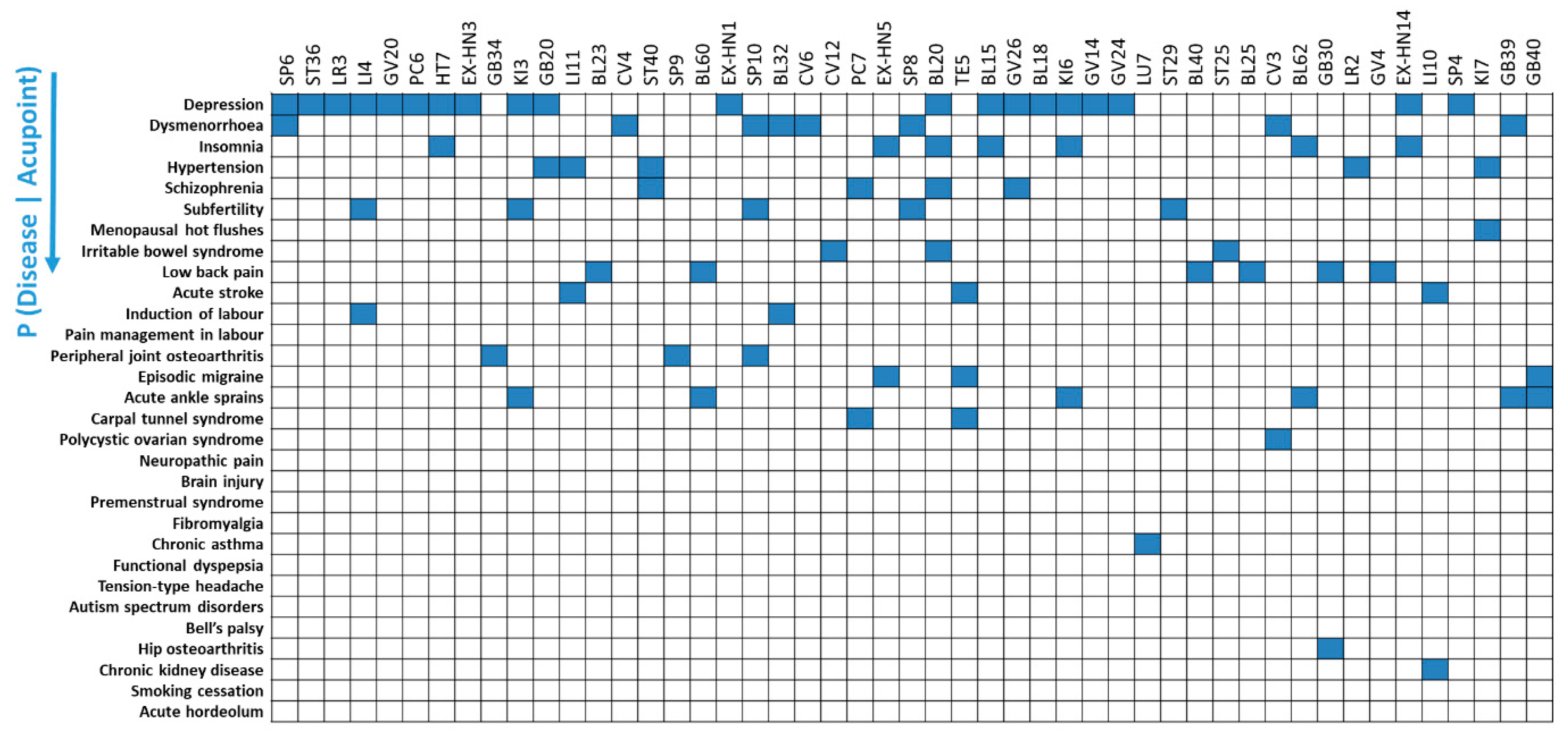
2.3. Data Analysis of Acupoint Indication Using Reverse Inference
2.4. Bayes Factor Correction of Acupoint Indication
3. Results
3.1. Patterns of Acupoint Selection for 30 Diseases Using Forward Inference
3.2. Patterns of Acupoint Indications for 49 Acupoints Using Reverse Inference
3.3. Specificity of Acupoint Indications Using Bayes Factor Correction
3.4. Two Different Patterns of Acupoint Indications
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Hwang, Y.C.; Lee, I.S.; Ryu, Y.; Lee, M.S.; Chae, Y. Exploring traditional acupuncture point selection patterns for pain control: Data mining of randomised controlled clinical trials. Acupunct. Med. 2020, 964528420926173. [Google Scholar] [CrossRef] [PubMed]
- White, A. Editorial Board of Acupuncture in M. Western medical acupuncture: A definition. Acupunct. Med. 2009, 27, 33–35. [Google Scholar] [CrossRef] [PubMed]
- Chae, Y.; Chang, D.S.; Lee, S.H.; Jung, W.M.; Lee, I.S.; Jackson, S.; Kong, J.; Lee, H.; Park, H.J.; Lee, H.; et al. Inserting needles into the body: A meta-analysis of brain activity associated with acupuncture needle stimulation. J. Pain 2013, 14, 215–222. [Google Scholar] [CrossRef]
- Jung, W.M.; Lee, I.S.; Lee, Y.S.; Kim, J.; Park, H.J.; Wallraven, C.; Chae, Y. Decoding spatial location of perceived pain to acupuncture needle using multivoxel pattern analysis. Mol. Pain 2019, 15, 1744806919877060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, I.S.; Jung, W.M.; Park, H.J.; Chae, Y. Spatial Information of Somatosensory Stimuli in the Brain: Multivariate Pattern Analysis of Functional Magnetic Resonance Imaging Data. Neural Plast. 2020, 8307580. [Google Scholar] [CrossRef]
- Chen, Y.R.; Zhu, J.; Song, J.S.; She, Y.F. Discussion on point selection and compatibility of acupuncture formula. Zhongguo Zhen Jiu 2012, 32, 65–68. [Google Scholar] [PubMed]
- Jung, W.M.; Lee, T.; Lee, I.S.; Kim, S.; Jang, H.; Kim, S.Y.; Park, H.J.; Chae, Y. Spatial Patterns of the Indications of Acupoints Using Data Mining in Classic Medical Text: A Possible Visualization of the Meridian System. Evid. Based Complement. Altern. Med. 2015, 2015, 457071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Kim, C.E.; Lee, I.S.; Jung, W.M.; Kim, H.G.; Jang, H.; Kim, S.J.; Lee, H.; Park, H.J.; Chae, Y. Network analysis of acupuncture points used in the treatment of low back pain. Evid. Based Complement. Altern. Med. 2013, 2013, 402180. [Google Scholar] [CrossRef]
- Alvim, D.T.; Ferreira, A.S. Inter-expert agreement and similarity analysis of traditional diagnoses and acupuncture prescriptions in textbook- and pragmatic-based practices. Complement. Ther. Clin. Pract. 2018, 30, 38–43. [Google Scholar] [CrossRef]
- Lee, T.; Jung, W.M.; Lee, I.S.; Lee, Y.S.; Lee, H.; Park, H.J.; Kim, N.; Chae, Y. Data Mining of Acupoint Characteristics from the Classical Medical Text: DongUiBoGam of Korean Medicine. Evid. Based Complement. Altern. Med. 2014, 2014, 329563. [Google Scholar] [CrossRef] [Green Version]
- Lee, I.S.; Cheon, S.; Park, J.Y. Central and Peripheral Mechanism of Acupuncture Analgesia on Visceral Pain: A Systematic Review. Evid. Based Complement. Altern. Med. 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Li, J.B.; Xiong, Q.L.; Qu, S.K.; Qi, F.; Zhang, L.; Wang, Q.; Bao, K.; Li, F.B. Discussion on the regular of acupoint selection of acupuncture and moxibustion for lumbar disc herniation during recent 10 years. Zhongguo Zhen Jiu 2013, 33, 668–672. [Google Scholar] [PubMed]
- Yu, S.; Yang, J.; Ren, Y.; Chen, L.; Liang, F.; Hu, Y. Characteristics of acupoints selection of moxibustion for primary dysmenorrhea based on data mining technology. Zhongguo Zhen Jiu 2015, 35, 845–849. [Google Scholar] [PubMed]
- Zhang, K.; Xu, Y.; Ding, S.; Hong, S.; Zhao, X.; Guo, Y. Literature study for acupoint selection rule of rheumatoid arthritis treated with acupuncture. Zhongguo Zhen Jiu 2017, 37, 221–224. [Google Scholar] [CrossRef] [PubMed]
- Hwang, Y.C.; Lee, Y.S.; Ryu, Y.; Lee, I.S.; Chae, Y. Statistical inference of acupoint specificity: Forward and reverse inference. Integr. Med. Res. 2020, 9, 17–20. [Google Scholar] [CrossRef]
- Smith, C.A.; Armour, M.; Lee, M.S.; Wang, L.Q.; Hay, P.J. Acupuncture for depression. Cochrane Database Syst Rev. 2018, 3. [Google Scholar] [CrossRef]
- Heit, E. Brain imaging, forward inference, and theories of reasoning. Front. Hum. Neurosci. 2014, 8, 1056. [Google Scholar] [CrossRef]
- Henson, R. Forward inference using functional neuroimaging: Dissociations versus associations. Trends Cogn Sci. 2006, 10, 64–69. [Google Scholar] [CrossRef]
- Hutzler, F. Reverse inference is not a fallacy per se: Cognitive processes Can be inferred from functional imaging data. Neuroimage 2014, 84, 1061–1069. [Google Scholar] [CrossRef] [Green Version]
- Poldrack, R.A. Can cognitive processes be inferred from neuroimaging data? Trends Cogn Sci. 2006, 10, 59–63. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.S.; Ryu, Y.; Yoon, D.-E.; Kim, C.H.; Hong, G.; Hwang, Y.C.; Chae, Y. Commonality and specificity of acupuncture points selections. Evid. Based Complement. Altern. Med. 2020, 2020, 2948292. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Ryu, Y.; Chae, Y. Acupoint selection based on pattern identification results or disease state. Integr. Med. Res. 2020, 9, 100405. [Google Scholar] [CrossRef]
- Birch, S.; Alraek, T. Traditional East Asian medicine: How to understand and approach diagnostic findings and patterns in a modern scientific framework? Chin. J. Integr. Med. 2014, 20, 336–340. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Yoon, D.E.; Lee, Y.S.; Jung, W.; Kim, J.H.; Chae, Y. Revealing Associations between Diagnosis Patterns and Acupoint Prescriptions Using Medical Data Extracted from Case Reports. J. Clin. Med. 2019, 8, 1663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kam, W.; Zhang, Z.J.; Baarnhielm, S. Traditional Chinese Medicine Explanatory Models of Depressive Disorders: A Qualitative Study. Cult. Med. Psychiatry 2019, 43, 387–403. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
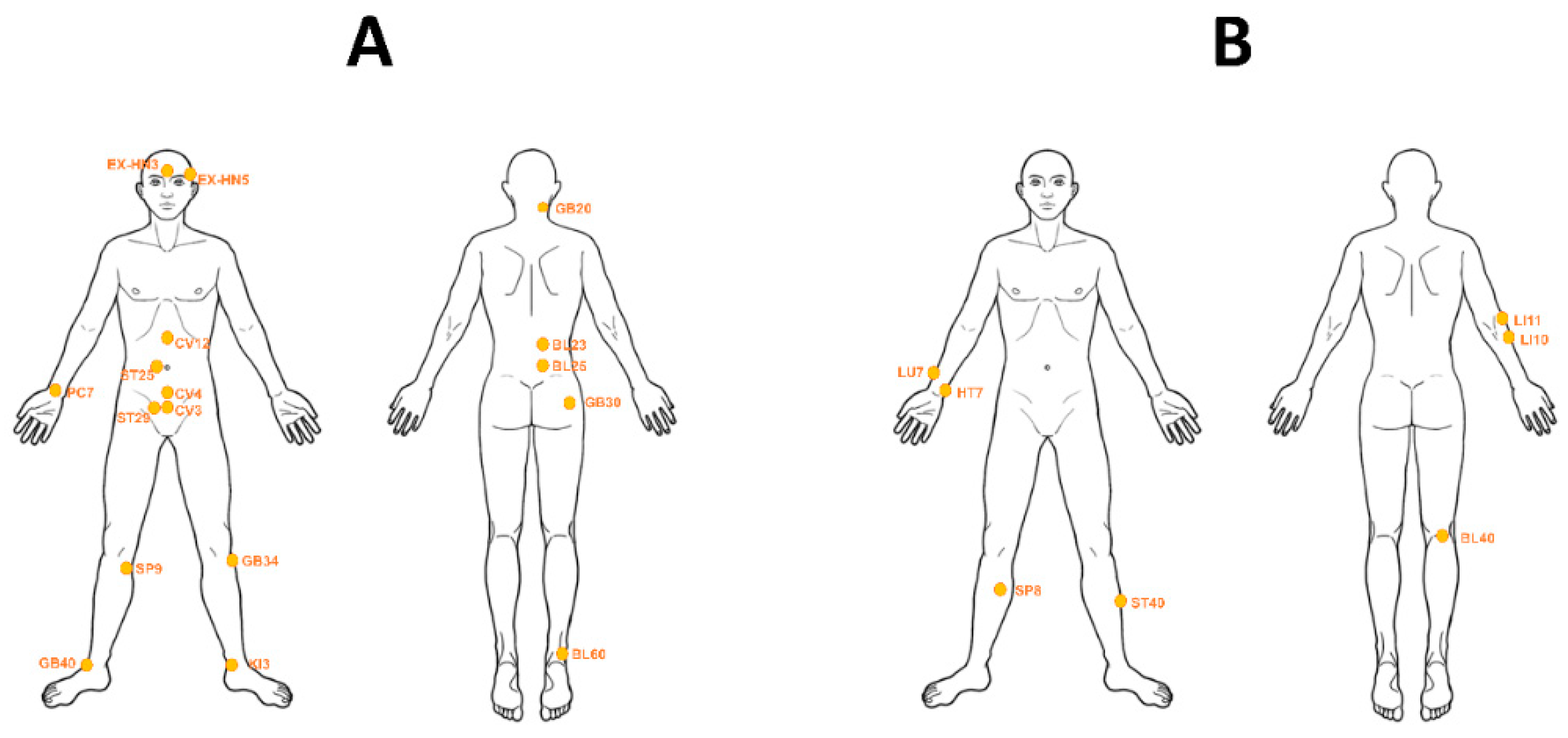
| Type I (Regional Acupoints, n = 17) | |
| BL23 (back) | Low back pain (BF = 10.12) |
| BL25 (back) | Low back pain (BF = 36.87) |
| BL60 (feet) | Acute ankle sprain (BF = 13.47) |
| CV3 (abdomen) | Polycystic ovarian syndrome (BF = 18.53) |
| CV4 (abdomen) | Dysmenorrhea (BF = 5.51) |
| CV12 (abdomen) | Irritable bowel syndrome (BF = 8.29) |
| EX-HN3 (head) | Depression (BF = 6.36) |
| EX-HN5 (head) | Episodic migraine (BF = 9.03) |
| GB20 (head) | Hypertension (BF = 3.94) |
| GB30 (lower limb) | Hip osteoarthritis (BF = 53.94) |
| GB34 (lower limb) | Peripheral joint osteoarthritis (BF = 7.60) |
| GB40 (feet) | Acute ankle sprain (BF = 38.50) |
| KI3 (feet) | Acute ankle sprain (BF = 5.39) |
| PC7 (upper limb) | Carpal tunnel syndrome (BF = 35.31) |
| SP9 (lower limb) | Peripheral joint osteoarthritis (BF = 9.39) |
| ST25 (abdomen) | Irritable bowel syndrome (BF = 33.16) |
| ST29 (abdomen) | Subfertility (BF = 27.09) |
| Type II (Distal Acupoints, n = 7) | |
| BL40 (lower limb) | Low back pain (BF = 32.26) |
| HT7 (upper limb) | Insomnia (BF = 3.68) |
| LI10 (upper limb) | Chronic kidney disease (BF = 105.3) |
| LI11 (upper limb) | Hypertension (BF = 6.60), Acute stroke (BF = 6.57) |
| LU7 (upper limb) | Chronic asthma (BF = 22.48) |
| SP8 (lower limb) | Dysmenorrhea (BF = 17.56) |
| ST40 (lower limb) | Schizophrenia (BF = 5.29) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, Y.-C.; Lee, I.-S.; Ryu, Y.; Lee, Y.-S.; Chae, Y. Identification of Acupoint Indication from Reverse Inference: Data Mining of Randomized Controlled Clinical Trials. J. Clin. Med. 2020, 9, 3027. https://doi.org/10.3390/jcm9093027
Hwang Y-C, Lee I-S, Ryu Y, Lee Y-S, Chae Y. Identification of Acupoint Indication from Reverse Inference: Data Mining of Randomized Controlled Clinical Trials. Journal of Clinical Medicine. 2020; 9(9):3027. https://doi.org/10.3390/jcm9093027
Chicago/Turabian StyleHwang, Ye-Chae, In-Seon Lee, Yeonhee Ryu, Ye-Seul Lee, and Younbyoung Chae. 2020. "Identification of Acupoint Indication from Reverse Inference: Data Mining of Randomized Controlled Clinical Trials" Journal of Clinical Medicine 9, no. 9: 3027. https://doi.org/10.3390/jcm9093027