Ductal Carcinoma In Situ Underestimation of Microcalcifications Only by Stereotactic Vacuum-Assisted Breast Biopsy: A New Predictor of Specimens without Microcalcifications


Abstract
:1. Introduction
2. Materials and Methods
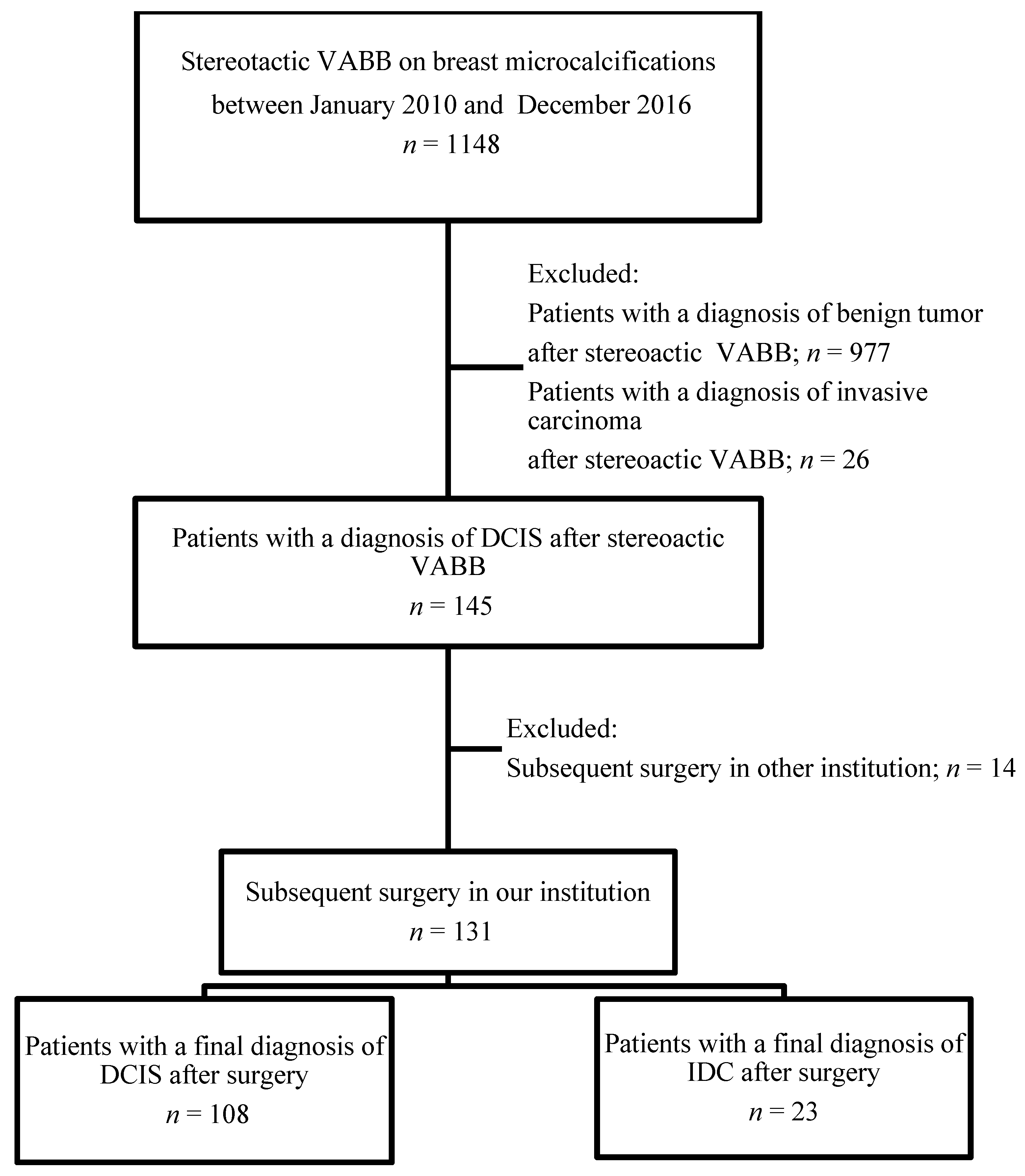
2.1. Patients
2.2. Stereotactic Breast Biopsy on Microcalcifications
2.3. Subsequent Surgical Excision
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Mammographic Features
3.3. Procedural Relationships
3.4. Pathological Findings
3.5. Univariates among DCIS and Upgraded Invasive Carcinoma
4. Discussion
5. Conclusions
Author Contributions
Funding
Ethics Approval
Conflicts of Interest
References
- Sankatsing, V.D.V.; van Ravesteyn, N.T.; Heijnsdijk, E.A.M.; Looman, C.W.N.; van Luijt, P.A.; Fracheboud, J.; de Heeten, G.J.; Broeders, M.J.M.; de Koning, H.J. The effect of population-based mammography screening in Dutch municipalities on breast cancer mortality 20 years of follow-up. Int. J. Cancer 2017, 141, 671–677. [Google Scholar] [CrossRef] [Green Version]
- Bruening, W.; Fontanarosa, J.; Tipton, K.; Treadwell, J.R.; Launders, J.; Schoelles, K. Systematic Review: Comparative Effectiveness of Core-Needle and Open Surgical Biopsy to Diagnose Breast Lesions. Ann. Intern. Med. 2010, 152, 238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kettritz, U.; Rotter, K.; Schreer, I.; Murauer, M.; Schulz-Wendtland, R.; Peter, D.; Heywang-Köbrunner, S. Stereotactic vacuum-assisted breast biopsy (VB) in 2874 patients: A multicenter study. Cancer 2004, 100, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.L.; Adrada, B.E.; Candelaria, R.; Thames, D.; Dawson, D.; Yang, W.T. Stereotactic Breast Biopsy: Pitfalls and Pearls. Tech. Vasc. Interv. Radiol. 2014, 17, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Kunju, L.P.; Kleer, C.G. Significance of flat epithelial atypia on mammotome core needle biopsy: Should it be excised? Hum. Pathol. 2007, 38, 35–41. [Google Scholar] [CrossRef]
- Chivukula, M.; Bhargava, R.; Tseng, G.C.; Dabbs, D.J. Clinicopathologic Implications of “Flat Epithelial Atypia” in Core Needle Biopsy Specimens of the Breast. Am. J. Clin. Pathol. 2009, 131, 802–808. [Google Scholar] [CrossRef] [Green Version]
- Senetta, R.; Campanino, P.P.; Mariscotti, G.; Garberoglio, S.; Daniele, L.; Pennecchi, F.; Macri, L.; Bosco, M.; Gandini, G.; Sapino, A. Columnar cell lesions associated with breast calcifications on vacuum-assisted core biopsies: Clinical, radiographic, and histological correlations. Mod. Pathol. 2009, 22, 762–769. [Google Scholar] [CrossRef]
- Eby, P.R.; Ochsner, J.E.; DeMartini, W.B.; Allison, K.H.; Peacock, S.; Lehman, C.D. Frequency and Upgrade Rates of Atypical Ductal Hyperplasia Diagnosed at Stereotactic Vacuum-Assisted Breast Biopsy: 9-Versus 11-Gauge. Am. J. Roentgenol. 2009, 192, 229–234. [Google Scholar] [CrossRef]
- Sneige, N.; Lim, S.C.; Whitman, G.J.; Krishnamurthy, S.; Sahin, A.A.; Smith, T.L.; Selling, C.B. Atypical ductal hyperplasia diagnosis by directional vacuum-assisted stereotactic biopsy of breast microcalcifications. Considerations for surgical excision. Am. J. Clin. Pathol. 2003, 119, 248–253. [Google Scholar] [CrossRef]
- Ingegnoli, A.; D’Aloia, C.; Frattaruolo, A.; Pallavera, L.; Martella, E.; Crisi, G.; Zompatori, M. Flat Epithelial Atypia and Atypical Ductal Hyperplasia: Carcinoma Underestimation Rate. Breast J. 2010, 16, 55–59. [Google Scholar] [CrossRef]
- Degnim, A.C.; Visscher, D.W.; Berman, H.K.; Frost, M.H.; Sellers, T.A.; Vierkant, R.A.; Maloney, S.D.; Pankratz, V.S.; De Groen, P.C.; Lingle, W.L.; et al. Stratification of Breast Cancer Risk in Women With Atypia: A Mayo Cohort Study. J. Clin. Oncol. 2007, 25, 2671–2677. [Google Scholar] [CrossRef] [PubMed]
- Becker, A.K.; Gordon, P.B.; Harrison, D.A.; Hassell, P.R.; Hayes, M.M.; Van Niekerk, D.; Wilson, C.M. Flat Ductal Intraepithelial Neoplasia 1A Diagnosed at Stereotactic Core Needle Biopsy: Is Excisional Biopsy Indicated? Am. J. Roentgenol. 2013, 200, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Dialani, V.; Venkataraman, S.; Frieling, G.; Schnitt, S.J.; Mehta, T.S. Does Isolated Flat Epithelial Atypia on Vacuum-assisted Breast Core Biopsy Require Surgical Excision? Breast J. 2014, 20, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Brennan, M.; Turner, R.M.; Ciatto, S.; Marinovich, M.L.; French, J.R.; Macaskill, P.; Houssami, N. Ductal Carcinoma in Situ at Core-Needle Biopsy: Meta-Analysis of Underestimation and Predictors of Invasive Breast Cancer. Radiology 2011, 260, 119–128. [Google Scholar] [CrossRef]
- Lyman, G.H.; Somerfield, M.R.; Bosserman, L.D.; Perkins, C.L.; Weaver, D.L.; Giuliano, A.E. Sentinel lymph node biopsy for patients with early stage breast cancer: American Society of Clinical Oncology Clinical Practice guideline update. J. Clin. Oncol. 2017, 35, 561–564. [Google Scholar] [CrossRef] [Green Version]
- Burnside, E.S.; Ochsner, J.E.; Fowler, K.J.; Fine, J.P.; Salkowski, L.R.; Rubin, D.L.; Sisney, G.A. Use of microcalcification descriptors in BI-RADS 4th edition to stratify risk of malignancy. Radiology 2007, 242, 388–395. [Google Scholar] [CrossRef]
- Correa, C.; McGale, P.; Taylor, C.; Wang, Y.; Clarke, M.; Davies, C.; Peto, R.; Bijker, N.; Solin, L.; Darby, S. Overview of the randomized trials of radiotherapy in ductal carcinoma in situ of the breast. J. Natl. Cancer Inst. Monogr. 2010, 41, 162–177. [Google Scholar]
- Brem, R.F.; Schoonjans, J.M.; Goodman, S.N.; Nolten, A.; Askin, F.B.; Gatewood, O.M.B. Nonpalpable Breast Cancer: Percutaneous Diagnosis with 11- and 8-gauge Stereotactic Vacuum-assisted Biopsy Devices1. Radiology 2001, 219, 793–796. [Google Scholar] [CrossRef]
- Orsaria, P.; Granai, A.V.; Venditti, D.; Petrella, G.; Buonomo, O.C. Investigational Paradigms in Downscoring and Upscoring DCIS: Surgical Management Review. Int. J. Surg. Oncol. 2012, 2012, 1–10. [Google Scholar] [CrossRef]
- Philpotts, L.E.; Lee, C.H.; Horvath, L.J.; Lange, R.C.; Carter, D.; Tocino, I. Underestimation of Breast Cancer with II-Gauge Vacuum Suction Biopsy. Am. J. Roentgenol. 2000, 175, 1047–1050. [Google Scholar] [CrossRef]
- Lourenco, A.P.; Mainiero, M.B.; Lazarus, E.; Giri, D.; Schepps, B. Stereotactic Breast Biopsy: Comparison of Histologic Underestimation Rates with 11- and 9-Gauge Vacuum-Assisted Breast Biopsy. Am. J. Roentgenol. 2007, 189, W275–W279. [Google Scholar] [CrossRef] [PubMed]
- Jackman, R.J.; Burbank, F.; Parker, S.H.; Evans, W.P.; Lechner, M.C.; Richardson, T.R.; Smid, A.A.; Borofsky, H.B.; Lee, C.H.; Goldstein, H.M.; et al. Stereotactic Breast Biopsy of Nonpalpable Lesions: Determinants of Ductal Carcinoma in Situ Underestimation Rates. Radiology 2001, 218, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Liberman, L.; Dershaw, D.D.; Rosen, P.P.; Morris, E.A.; Abramson, A.F.; Borgen, P.I. Percutaneous removal of malignant mammographic lesions at stereo- tactic vacuum-assisted biopsy. Radiology 1998, 206, 711–715. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.C.; Lin, Y.C.; Cheng, H.Y.; Juan, Y.H.; Lin, G.G.; Cheung, Y.C. Performance of Stereotactic Vacuum-Assisted Biopsy on Breast Microcalci cations: Comparison of 7-gauge and 10-gauge Biopsy Needles. J. Radiol. Sci. 2020, 45, 25–31. [Google Scholar]
- Cheung, Y.-C.; Juan, Y.-H.; Ueng, S.-H.; Lo, Y.-F.; Huang, P.-C.; Lin, Y.-C.; Chen, S.-C. Assessment of Breast Specimens With or Without Calcifications in Diagnosing Malignant and Atypia for Mammographic Breast Microcalcifications without Mass: A STARD-compliant diagnostic accuracy article. Medicine 2015, 94, e1832. [Google Scholar] [CrossRef]
- Margolin, F.R.; Kaufman, L.; Jacobs, R.P.; Denny, S.R.; Schrumpf, J.D. Stereotactic Core Breast Biopsy of Malignant Calcifications: Diagnostic Yield of Cores with and Cores without Calcifications on Specimen Radiographs1. Radiology 2004, 233, 251–254. [Google Scholar] [CrossRef]


{kind=link}
| Variables | No. (%) | |
|---|---|---|
| Study Period | 2010–2016 | 131 (100) |
| Age of initial diagnosis (years) | Median (IQR) | 52.0 (10.0) |
| Lesion location | Right | 70 (53.4) |
| Left | 61 (46.6) | |
| Family history of breast cancer | Yes | 10 (7.6) |
| No | 121 (92.4) | |
| Parenchymal density | Almost entirely fat | 2 (1.5) |
| Scattered fibroglandular | 24 (18.3) | |
| Heterogeneously dense | 84 (64.1) | |
| Extremely dense | 21 (16.0) | |
| Microlcalcifications extent (mm) | Median (IQR) | 12.0 (13.0) |
| Distribution of microcalcifications | Regional | 18 (13.7) |
| Grouped | 96 (73.3) | |
| Linear or segmental | 17 (13.0) | |
| Morphology of microcalcifications | Amorphous | 50 (38.2) |
| Pleomorphic | 69 (52.7) | |
| Fine linear or branched | 12 (9.2) | |
| Biopsy needle gauge | 7 G | 27 (20.6) |
| 10 G | 104 (79.4) | |
| Microcalcification retrieval (%) | <90 | 81 (61.8) |
| ≥90 | 50 (38.2) | |
| BI-RADS category | 4a | 73 (55.7) |
| 4b | 31 (23.7) | |
| 4c | 27 (20.6) | |
| DCIS grade | Low | 18 (13.7) |
| Intermediate | 81 (61.8) | |
| High | 32 (24.4) | |
| Histology of non-calcified specimens | Benign | 65 (49.6) |
| DCIS | 66 (50.4) | |
| Estrogen receptor | Negative | 28 (21.4) |
| Positive | 103 (78.6) | |
| Progesterone receptor | Negative | 35 (26.7) |
| Positive | 96 (73.3) | |
| HER-2 status | Negative | 93 (71.0) |
| Positive | 38 (29.0) | |
| Variables | DCIS (n = 108) | IDC (n = 23) | p Value |
|---|---|---|---|
| Age | 0.142 | ||
| ≤50 | 46 (88.5) | 6 (11.5) | |
| >50 | 62 (78.5) | 17 (21.5) | |
| Lesion location | 0.744 | ||
| Right | 57 (81.4) | 13 (18.6) | |
| Left | 51 (83.6) | 10 (16.4) | |
| Family history of breast cancer | 0.208 | ||
| Yes | 10 (100.0) | 0 | |
| No | 98 (81.0) | 23 (19.0) | |
| Parenchymal density | 0.420 | ||
| Almost entirely fat | 1 (50.0) | 1 (50.0) | |
| Scattered fibroglandular | 19 (79.2) | 5 (20.8) | |
| Heterogeneously dense | 72 (85.7) | 12 (14.3) | |
| Extremely dense | 16 (76.2) | 5 (23.8) | |
| Microcalcifications extent (mm) | 0.002 | ||
| <11.5 | 58 (93.5) | 4 (6.5) | |
| ≥11.5 | 50 (72.5) | 19 (27.5) | |
| Distribution of microcalcifications | 0.021 | ||
| Regional | 11 (61.1) | 7 (38.9) | |
| Grouped | 84 (87.5) | 12 (12.5) | |
| Linear or segmental | 13 (76.5) | 4 (23.5) | |
| Morphology of microcalcifications | 0.195 | ||
| Amorphous | 45 (90.0) | 5 (10.0) | |
| Pleomorphic | 54 (78.3) | 15 (21.7) | |
| Fine linear or branched | 9 (75.0) | 3 (25.0) | |
| Biopsy needle gauge | 0.783 | ||
| 7 G | 23 (85.2) | 4 (14.8) | |
| 10 G | 85 (81.7) | 19 (18.3) | |
| Microcalcification retrieval (%) | 0.006 | ||
| <90 | 61 (75.3) | 20 (24.7) | |
| ≥90 | 47 (94.0) | 3 (6.0) | |
| BI-RADS category | 0.345 | ||
| 4a | 63 (86.3) | 10 (13.7) | |
| 4b | 25 (80.6) | 6 (19.4) | |
| 4c | 20 (74.1) | 7 (25.9) | |
| DCIS grade | 0.221 | ||
| Low | 17 (94.4) | 1 (5.6) | |
| Intermediate | 67 (82.7) | 14 (17.3) | |
| High | 24 (75.0) | 8 (25.0) | |
| Histology of non-calcified specimens | <0.0001 | ||
| Benign | 63 (96.9) | 2 (3.1) | |
| DCIS | 45 (68.2) | 21 (31.8) | |
| Estrogen receptor | 0.009 | ||
| Negative | 18 (64.3) | 10 (35.7) | |
| Positive | 90 (87.4) | 13 (12.6) | |
| Progesterone receptor | 0.045 | ||
| Negative | 25 (71.4) | 10 (28.6) | |
| Positive | 83 (86.5) | 13 (13.5) | |
| HER-2 status | 0.001 | ||
| Negative | 83 (89.2) | 10 (10.8) | |
| Positive | 25 (65.8) | 13 (34.2) |
| Variables | Multivariate | ||
|---|---|---|---|
| Odds Ratio | 95% CI | p Value | |
| Microcalcifications extent (mm) | |||
| <11.5 | 1 | ||
| ≥11.5 | 1.734 | 0.290–10.373 | 0.546 |
| Distribution of microcalcification | |||
| Grouped | 1 | ||
| Regional | 1.788 | 0.365–8.775 | 0.474 |
| Linear or segmental | 0.560 | 0.098–3.215 | 0.515 |
| Microcalcification retrieval (%) | |||
| <90 | 3.452 | 0.577–20.637 | 0.175 |
| ≥90 | 1 | ||
| Histology of non-calcified specimens | |||
| Benign | 1 | ||
| DCIS | 21.492 | 3.960–116.649 | <0.001 |
| Estrogen receptor | |||
| Negative | 10.267 | 0.520–202.855 | 0.126 |
| Positive | 1 | ||
| Progesterone receptor | |||
| Negative | 0.117 | 0.006–2.408 | 0.165 |
| Positive | 1 | ||
| HER-2 status | |||
| Negative | 1 | ||
| Positive | 2.606 | 0.649–10.466 | 0.177 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheung, Y.-C.; Chen, S.-C.; Ueng, S.-H.; Yu, C.-C. Ductal Carcinoma In Situ Underestimation of Microcalcifications Only by Stereotactic Vacuum-Assisted Breast Biopsy: A New Predictor of Specimens without Microcalcifications. J. Clin. Med. 2020, 9, 2999. https://doi.org/10.3390/jcm9092999
Cheung Y-C, Chen S-C, Ueng S-H, Yu C-C. Ductal Carcinoma In Situ Underestimation of Microcalcifications Only by Stereotactic Vacuum-Assisted Breast Biopsy: A New Predictor of Specimens without Microcalcifications. Journal of Clinical Medicine. 2020; 9(9):2999. https://doi.org/10.3390/jcm9092999
Chicago/Turabian StyleCheung, Yun-Chung, Shin-Cheh Chen, Shir-Hwa Ueng, and Chi-Chang Yu. 2020. "Ductal Carcinoma In Situ Underestimation of Microcalcifications Only by Stereotactic Vacuum-Assisted Breast Biopsy: A New Predictor of Specimens without Microcalcifications" Journal of Clinical Medicine 9, no. 9: 2999. https://doi.org/10.3390/jcm9092999