Colchicine to Weather the Cytokine Storm in Hospitalized Patients with COVID-19

 , , and
, , and
Abstract
:1. Introduction
2. Experimental Section
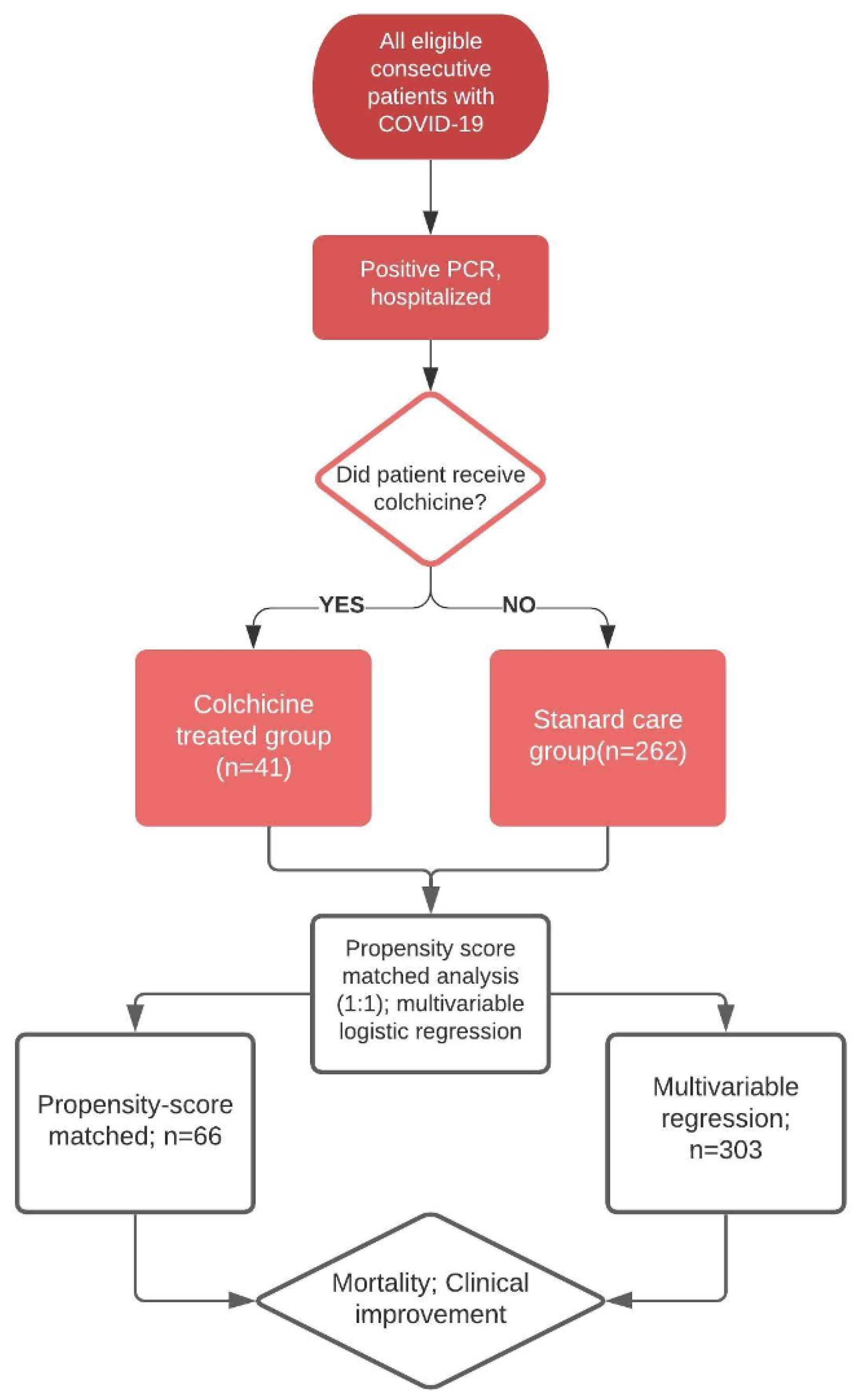
2.1. Patients and Study Design
2.2. Study Assessments
2.3. Institutional Review Board
2.4. Statistical Analysis
2.5. Role of the Funding Source
3. Results
3.1. Evaluation of Outcomes
3.1.1. Baseline Characteristics of the Patients
3.1.2. Treatment with Colchicine
3.1.3. Concomitant Drugs Given
3.1.4. Clinical Improvement during Colchicine Treatment
3.1.5. Mortality
3.1.6. Laboratory Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Group, R.C.; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- National Institutes of Health. COVID-19 Treatment. Available online: https://covid19treatmentguidelines.nih.gov/therapeutic-options-under-investigation (accessed on 24 May 2020).
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Cheng, V.C.; Edwards, K.M.; Gandhi, R.; Muller, W.J.; O’Horo, J.C.; et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Colchicine Information. Available online: https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/colchicine-marketed-colcrys-information (accessed on 1 August 2020).
- Fried, J.A.; Ramasubbu, K.; Bhatt, R.; Topkara, V.K.; Clerkin, K.J.; Horn, E.; Rabbani, L.; Brodie, D.; Jain, S.S.; Kirtane, A.J.; et al. The Variety of Cardiovascular Presentations of COVID-19. Circulation 2020, 141, 1930–1936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tardif, J.C.; Kouz, S.; Waters, D.D.; Bertrand, O.F.; Diaz, R.; Maggioni, A.P.; Pinto, F.J.; Ibrahim, R.; Gamra, H.; Kiwan, G.S.; et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N. Engl. J. Med. 2019, 381, 2497–2505. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, N.; Firestein, B.L.; Brunetti, L. Colchicine in COVID-19: An Old Drug, New Use. Curr. Pharmacol. Rep. 2020, 6, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Greber, U.F. Signalling in viral entry. Cell Mol. Life Sci. 2002, 59, 608–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackman, R.W.; Rhoads, M.G.; Cornwell, E.; Kandarian, S.C. Microtubule-mediated NF-kappaB activation in the TNF-alpha signaling pathway. Exp. Cell Res. 2009, 315, 3242–3249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, M.; Boldescu, V.; Graf, D.; Streicher, F.; Dimoglo, A.; Bartenschlager, R.; Klein, C.D. Synthesis, Biological Evaluation, and Molecular Docking of Combretastatin and Colchicine Derivatives and their hCE1-Activated Prodrugs as Antiviral Agents. ChemMedChem 2019, 14, 469–483. [Google Scholar] [CrossRef] [PubMed]
- Colchicine and COVID Search. Clinicaltrials.gov. Available online: https://clinicaltrials.gov/ct2/results?cond=COVID&term=colchicine&cntry=&state=&city=&dist= (accessed on 24 May 2020).
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- World Health Organization (WHO) R&D Blueprint Group. Available online: https://www.who.int/blueprint/priority-diseases/key-action/COVID-19_Treatment_Trial_Design_Master_Protocol_synopsis_Final_18022020.pdf (accessed on 24 May 2020).
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cumhur Cure, M.; Kucuk, A.; Cure, E. Colchicine may not be effective in COVID-19 infection; it may even be harmful? Clin. Rheumatol. 2020, 39, 2101–2102. [Google Scholar] [CrossRef] [PubMed]
- Deftereos, S.G.; Giannopoulos, G.; Vrachatis, D.A.; Siasos, G.D.; Giotaki, S.G.; Gargalianos, P.; Metallidis, S.; Sianos, G.; Baltagiannis, S.; Panagopoulos, P.; et al. Effect of Colchicine vs Standard Care on Cardiac and Inflammatory Biomarkers and Clinical Outcomes in Patients Hospitalized With Coronavirus Disease 2019: The GRECCO-19 Randomized Clinical Trial. JAMA Netw. Open. 2020, 3, e2013136. [Google Scholar] [CrossRef] [PubMed]
- Gendelman, O.; Amital, H.; Bragazzi, N.L.; Watad, A.; Chodick, G. Continuous hydroxychloroquine or colchicine therapy does not prevent infection with SARS-CoV-2: Insights from a large healthcare database analysis. Autoimmun. Rev. 2020, 19, 102566. [Google Scholar] [CrossRef] [PubMed]
- Parra-Medina, R.; Sarmiento-Monroy, J.C.; Rojas-Villarraga, A.; Garavito, E.; Montealegre-Gomez, G.; Gomez-Lopez, A. Colchicine as a possible therapeutic option in COVID-19 infection. Clin. Rheumatol. 2020, 39, 2485–2486. [Google Scholar] [CrossRef] [PubMed]
- Piantoni, S.; Patroni, A.; Toniati, P.; Furloni, R.; Franceschini, F.; Andreoli, L.; Scarsi, M. Why not to use colchicine in COVID-19? An oldanti-inflammatory drug for a novel auto-inflammatory disease. Rheumatology 2020, 59, 1769–1770. [Google Scholar] [CrossRef] [PubMed]
- Scarsi, M.; Piantoni, S.; Colombo, E.; Airo, P.; Richini, D.; Miclini, M.; Bertasi, V.; Bianchi, M.; Bottone, D.; Civelli, P.; et al. Association between treatment with colchicine and improved survival in a single-centre cohort of adult hospitalised patients with COVID-19 pneumonia and acute respiratory distress syndrome. Ann. Rheum. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Della-Torre, E.; Ramirez, G.A.; Dagna, L.; Tresoldi, M. Colchicine treatment in community healthcare setting to prevent severe COVID-19. Ann. Rheum. Dis. 2020. [Google Scholar] [CrossRef]
- Della-Torre, E.; Della-Torre, F.; Kusanovic, M.; Scotti, R.; Ramirez, G.A.; Dagna, L.; Tresoldi, M. Treating COVID-19 with colchicine in community healthcare setting. Clin. Immunol. 2020, 217, 108490. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Unmatched Patients | Propensity-Score Matched Patients | |||||
|---|---|---|---|---|---|---|
| Colchicine | Standard (n = 262) | p-Value | Colchicine (n = 33) | Standard | p-Value | |
| (n = 41) | (n = 33) | |||||
| Age (years, mean ± SD) | 61.2 ± 13.0 | 63.0 ± 16.4 | 0.496 | 61.7 ± 11.2 | 64.1 ± 15.4 | 0.473 |
| Female (n, %) | 13 (31.7) | 103 (29.3) | 0.352 | 12 (36.4) | 11 (33.3) | 0.796 |
| Race (n.%) | 0.712 | 0.694 | ||||
| White | 11 (26.8) | 68 (26.0) | 9 (27.3) | 8 (24.2) | ||
| Hispanic | 20 (48.8) | 140 (53.4) | 19 (57.6) | 18 (54.5) | ||
| African-American | 3 (7.3) | 26 (9.9) | 1 (3.0) | 3 (9.1) | ||
| Asian | 5 (12.2) | 17 (6.5) | 3 (9.1) | 4 (12.1) | ||
| Other | 2 (4.9) | 11 (4.2) | 1 (3.0) | 0 (0) | ||
| LDH (U/L, mean ± SD) | 410.9 ± 154.3 | 358.1 ± 144.4 | 0.032 | 402.6 ± 131.3 | 392.2 ± 156.8 | 0.773 |
| Lactic acid (mg/dL, mean ± SD) | 2.1 ± 2.0 | 1.8 ± 0.88 | 0.267 | 1.7 ± 0.6 | 1.9 ± 1.0 | 0.359 |
| CRP (mg/dL, mean ± SD) | 15.0 ± 9.0 | 10.9 ± 6.6 | 0.007 | 14.9 ± 8.9 | 14.4 ± 8.8 | 0.835 |
| Procalcitonin (ng/mL, mean ± SD) | 2.3 ± 8.9 | 0.66 ± 3.2 | 0.247 | 0.4 ± 0.5 | 0.6 ± 1.4 | 0.475 |
| Ferritin (ng/mL, mean ± SD) | 1315.7 ± 991.3 | 990.8 ± 918.0 | 0.038 | 1314.5 ± 1085.3 | 1281.5 ± 1052.8 | 0.901 |
| Serum creatinine (mg/dL, mean ± SD) | 0.87 ± 0.34 | 1.2 ± 1.4 | 0.132 | 0.9 ± 0.4 | 0.9 ± 0.5 | 0.801 |
| Oxygen saturation (%, ± SD) | 88.8 ± 6.4 | 90.7 ± 8.3 | 0.166 | 88.6 ± 6.3 | 86.24± 11.3 | 0.329 |
| Body mass index (kg/m2, mean ± SD) | 30.4 ± 7.4 | 30.0 ± 7.1 | 0.741 | 30.7 ± 7.0 | 30.6 ± 8.0 | 0.932 |
| Comorbidity index score (mean ± SD) | 1.4 ± 1.9 | 1.2 ± 1.8 | 0.561 | 1.3 ± 1.9 | 0.97 ± 1.5 | 0.392 |
| Hypertension (n, %) | 21 (51.2) | 139 (53.1) | 0.827 | 20 (60.6) | 12 (36.4) | 0.049 |
| Myocardial infarction (n, %) | 5 (12.2) | 23 (8.8) | 0.559 | 4 (12.1) | 2 (6.1) | 0.672 |
| Heart failure (n, %) | 3 (7.3) | 14 (5.3) | 0.712 | 3 (9.1) | 2 (6.1) | 1 |
| Cerebrovascular disease (n, %) | 5 (12.2) | 18 (6.9) | 0.215 | 5 (15.2) | 2 (6.1) | 0.427 |
| Dementia (n, %) | 5 (12.2) | 22 (8.4) | 0.386 | 4 (12.1) | 2 (6.1) | 0.672 |
| Chronic pulmonary disease (n, %) | 7 (17.1) | 30 (11.5) | 0.307 | 5 (15.2) | 4 (12.1) | 1 |
| Diabetes (n, %) | 8 (19.5) | 84 (32.1) | 0.047 | 7 (21.2) | 7 (21.2) | 1 |
| Obese (n, %) | 19 (46.3) | 124 (47.3) | 0.906 | 16 (48.5) | 14 (42.4) | 0.395 |
| Hydroxychloroquine (n, %) | 18 (43.9) | 228 (87.0) | <0.001 | 18 (54.5) | 30 (90.9) | 0.001 |
| Azithromycin (n, %) | 12 (31.7) | 167 (63.7) | <0.001 | 11 (33.3) | 26 (78.8) | >0.001 |
| Remdesivir (n, %) | 10 (24.4) | 9 (3.4) | <0.001 | 4 (12.1) | 4 (12.1) | 1 |
| Tocilizumab (n, %) | 13 (31.7) | 73 (27.9) | 0.612 | 12 (36.4) | 11 (33.3) | 0.796 |
| Colchicine early administration * (n, %) | - | - | 23 (69.7) | - | - | |
| Colchicine loading dose (n, %) | - | 24 (72.7) | - | - | ||
| WHO OSCI Score (n, %) ** | 0.216 | |||||
| ≤3 | 4 (12.1) | 5 (15.2) | ||||
| 4 | 17 (51.5) | 21 (63.6) | ||||
| 5 | 11 (33.3) | 5 (15.2) | ||||
| 6 | 1 (3.0) | 0 (0) | ||||
| 7 | 0 (0) | 2 (6.1) | ||||
| Colchicine (n = 33) (n, %) | Standard (n = 33) (n, %) | Odds Ratio (95% Confidence Interval) | p-Value | |
|---|---|---|---|---|
| Primary endpoint | ||||
| All-cause mortality by day 28 | 3 (9.1) | 11 (33.3) | 0.20 (0.05–0.80) | 0.023 |
| Secondary endpoints | ||||
| Favorable change in WHO OSCI on day 14 | 19 (57.6) | 17 (51.5) | 1.28 (0.48–3.37) | 0.621 |
| WHO OSCI * score of <4 (indicating no need for supplemental oxygen on day 14 | 18 (54.5) | 18 (54.5) | 1.0 (0.38–2.64) | 1.000 |
| Favorable change in WHO OSCI on day 28 | 26 (78.8) | 17 (51.5) | 3.50 (1.19–10.28) | 0.023 |
| WHO OSCI score of <4 (indicating no need for supplemental oxygen on day 28 | 26 (78.8) | 18 (54.5) | 3.10 (1.05–9.11) | 0.040 |
| Patients discharged on day 28 | 30 (90.9) | 22 (66.7) | 5.0 (1.25–20.08) | 0.023 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brunetti, L.; Diawara, O.; Tsai, A.; Firestein, B.L.; Nahass, R.G.; Poiani, G.; Schlesinger, N. Colchicine to Weather the Cytokine Storm in Hospitalized Patients with COVID-19. J. Clin. Med. 2020, 9, 2961. https://doi.org/10.3390/jcm9092961
Brunetti L, Diawara O, Tsai A, Firestein BL, Nahass RG, Poiani G, Schlesinger N. Colchicine to Weather the Cytokine Storm in Hospitalized Patients with COVID-19. Journal of Clinical Medicine. 2020; 9(9):2961. https://doi.org/10.3390/jcm9092961
Chicago/Turabian StyleBrunetti, Luigi, Oumou Diawara, Andrew Tsai, Bonnie L. Firestein, Ronald G. Nahass, George Poiani, and Naomi Schlesinger. 2020. "Colchicine to Weather the Cytokine Storm in Hospitalized Patients with COVID-19" Journal of Clinical Medicine 9, no. 9: 2961. https://doi.org/10.3390/jcm9092961