The Prognostic Model of Pre-Treatment Complete Blood Count (CBC) for Recurrence in Early Cervical Cancer
 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical Management
2.3. Selection of Prognostic Variables for Survival and Recurrence
2.4. Model Development
2.5. Concordance Index (C-Index) Calculation
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics and Univariate Analysis of Pre-Treatment CBC
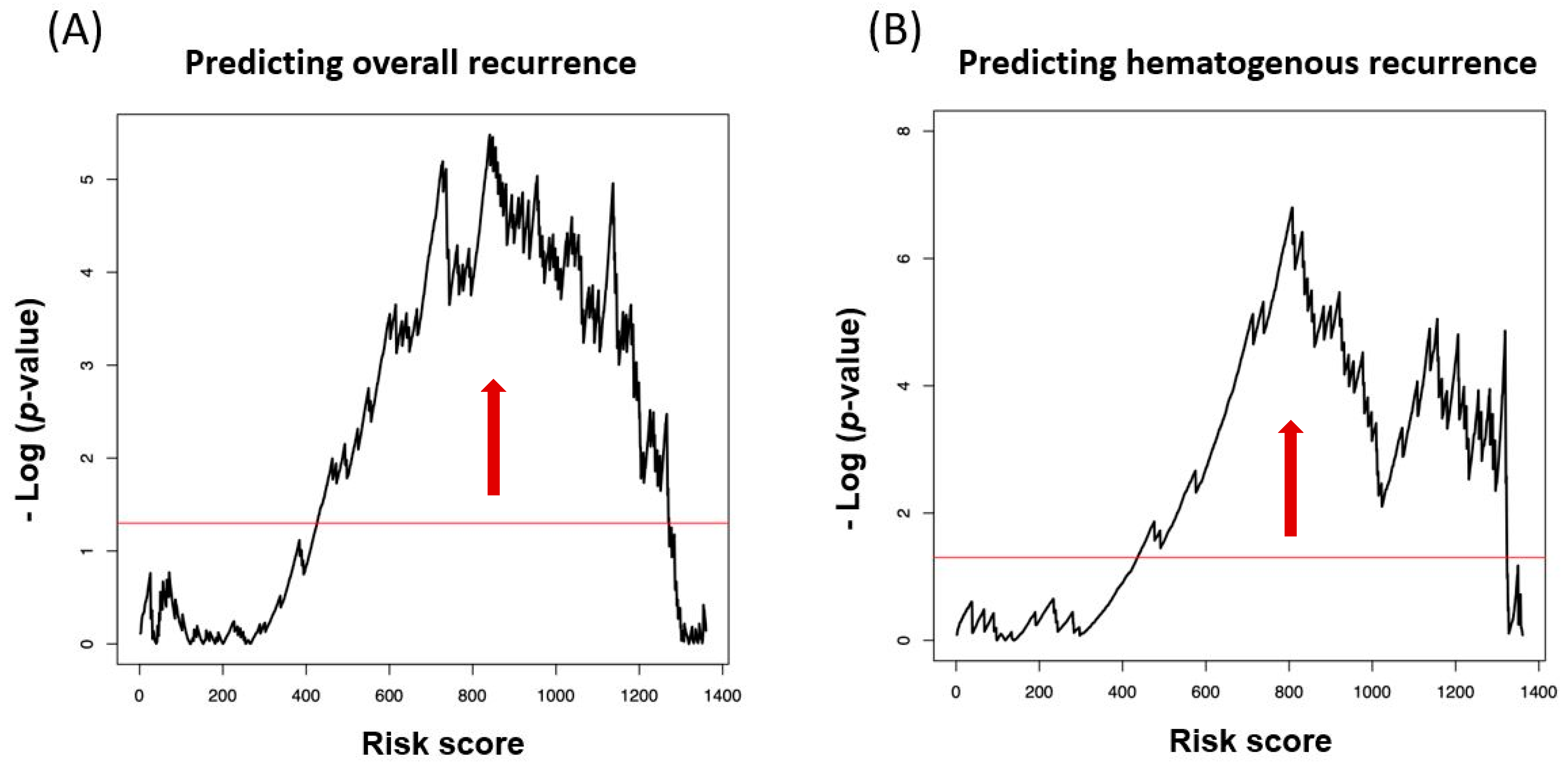
3.2. Model Development
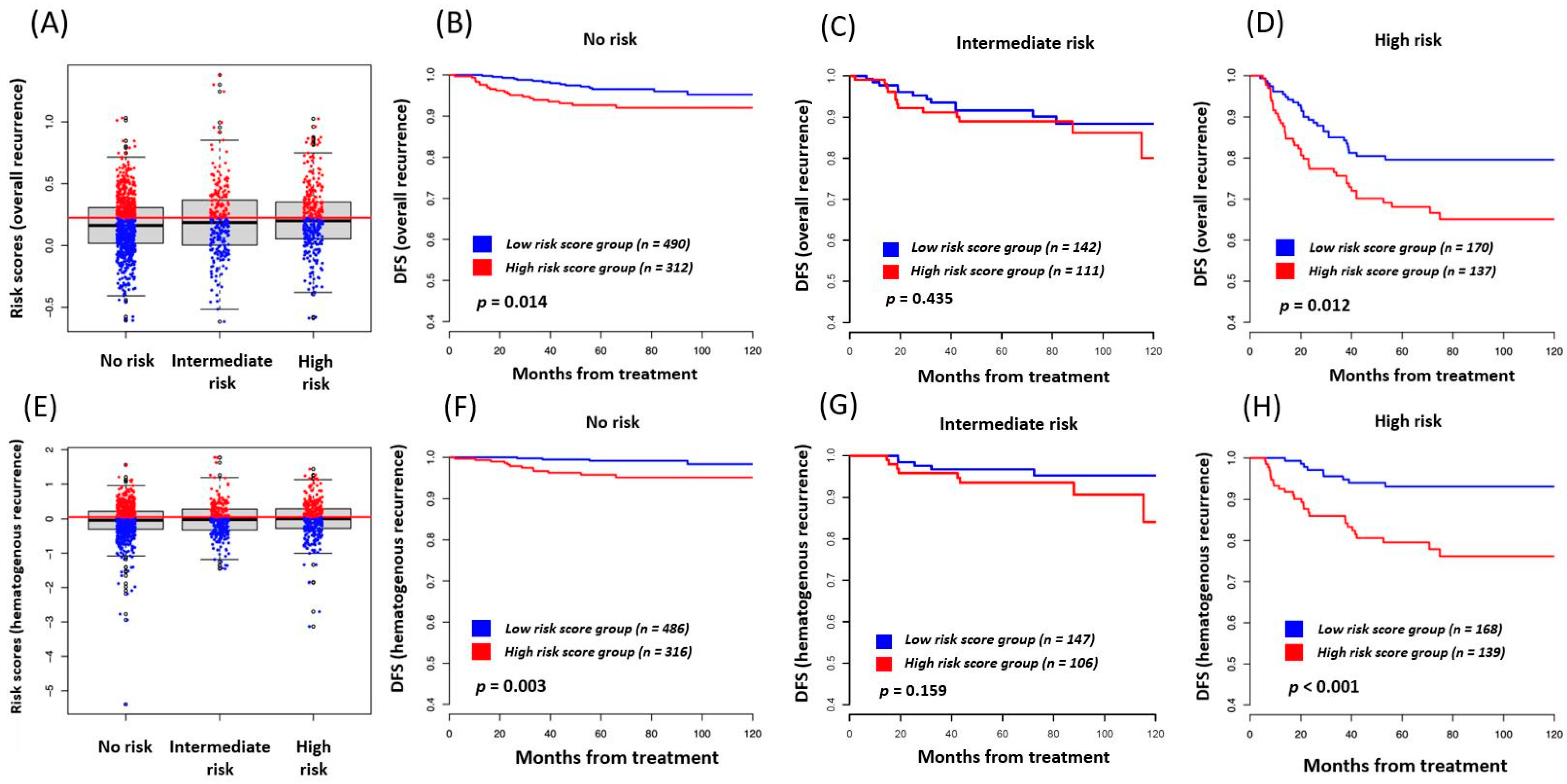
3.3. Risk Score as a Prognostic Marker in Each Traditional Risk Subgroup
3.4. Concordance Index (C-Index) Calculation
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gray, H.J. Primary Management of Early Stage Cervical Cancer (IA1-IB) and Appropriate Selection of Adjuvant Therapy. J. Natl. Compr. Cancer Netw. 2008, 6, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Delgado, G.; Bundy, B.; Zaino, R.; Sevin, B.-U.; Creasman, W.T.; Major, F. Prospective surgical-pathological study of disease-free interval in patients with stage IB squamous cell carcinoma of the cervix: A Gynecologic Oncology Group study. Gynecol. Oncol. 1990, 38, 352–357. [Google Scholar] [CrossRef]
- Zaino, R.J.; Ward, S.; Delgado, G.; Bundy, B.; Gore, H.; Fetter, G.; Ganjei, P.; Frauenhofer, E. Histopathologic predictors of the behavior of surgically treated stage IB squamous cell carcinoma of the cervix. A gynecologic oncology group study. Cancer 1992, 69, 1750–1758. [Google Scholar] [CrossRef]
- Burghardt, E.; Baltzer, J.; Tulusan, A.H.; Haas, J.; Baker, J. Results of surgical treatment of 1028 cervical cancers studied with volumetry. Cancer 1992, 70, 648–655. [Google Scholar] [CrossRef]
- Stehman, F.B.; Bundy, B.N.; DiSaia, P.J.; Keys, H.M.; Larson, J.E.; Fowler, W.C. Carcinoma of the cervix treated with radiation therapy I. A multi-variate analysis of prognostic variables in the gynecologic oncology group. Cancer 1991, 67, 2776–2785. [Google Scholar] [CrossRef]
- Pecorelli, S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int. J. Gynecol. Obstet. 2009, 105, 103–104. [Google Scholar] [CrossRef]
- Bipat, S.; Glas, A.S.; Van Der Velden, J.; Zwinderman, A.H.; Bossuyt, P.M.M.; Stoker, J. Computed tomography and magnetic resonance imaging in staging of uterine cervical carcinoma: A systematic review. Gynecol. Oncol. 2003, 91, 59–66. [Google Scholar] [CrossRef]
- McMillan, D.C. Systemic inflammation, nutritional status and survival in patients with cancer. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 223–226. [Google Scholar] [CrossRef] [Green Version]
- Akaike, H. A new look at the statistical model identification. IEEE Trans. Automat. Control 1974, 19, 716–722. [Google Scholar] [CrossRef]
- Harrell, F.E., Jr.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Moons, K.G.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.; Macaskill, P.; Steyerberg, E.W.; Vicker, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis. (TRIPOD): Explanation and elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.-H.; Wan, Q.-S.; Zhou, D.; Wang, T.; Hu, J.; He, Y.-T.; Yuan, H.-L.; Wang, Y.-Q.; Zhang, K.-H. A Simple-to-Use Nomogram for Predicting the Survival of Early Hepatocellular Carcinoma Patients. Front. Oncol. 2019, 9, 584. [Google Scholar] [CrossRef] [PubMed]
- Gönen, M.; Heller, G. Concordance probability and discriminatory power in proportional hazards regression. Biometrika 2005, 92, 965–970. [Google Scholar] [CrossRef]
- Shirai, Y.; Shiba, H.; Sakamoto, T.; Horiuchi, T.; Haruki, K.; Fujiwara, Y.; Futagawa, Y.; Ohashi, T.; Yanaga, K. Preoperative platelet to lymphocyte ratio predicts outcome of patients with pancreatic ductal adenocarcinoma after pancreatic resection. Surgery 2015, 158, 360–365. [Google Scholar] [CrossRef]
- Krenn-Pilko, S.; Langsenlehner, U.; Thurner, E.-M.; Stojakovic, T.; Pichler, M.; Gerger, A.; Kapp, K.S.; Langsenlehner, T. The elevated preoperative platelet-to-lymphocyte ratio predicts poor prognosis in breast cancer patients. Br. J. Cancer 2014, 110, 2524–2530. [Google Scholar] [CrossRef] [Green Version]
- Okamura, Y.; Ashida, R.; Ito, T.; Sugiura, T.; Mori, K.; Uesaka, K. Preoperative Neutrophil to Lymphocyte Ratio and Prognostic Nutritional Index Predict Overall Survival After Hepatectomy for Hepatocellular Carcinoma. World J. Surg. 2015, 39, 1501–1509. [Google Scholar] [CrossRef]
- Moghadamyeghaneh, Z.; Hanna, M.H.; Carmichael, J.C.; Mills, S.D.; Pigazzi, A.; Stamos, M.J. Preoperative Leukocytosis in Colorectal Cancer Patients. J. Am. Coll. Surg. 2015, 221, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Barber, E.L.; Rutstein, S.E.; Miller, W.C.; Gehrig, P.A. A preoperative personalized risk assessment calculator for elderly ovarian cancer patients undergoing primary cytoreductive surgery. Gynecol. Oncol. 2015, 139, 401–406. [Google Scholar] [CrossRef] [Green Version]
- Njølstad, T.S.; Engerud, H.; Werner, H.M.; Salvesen, H.B.; Trovik, J. Preoperative anemia, leukocytosis and thrombocytosis identify aggressive endometrial carcinomas. Gynecol. Oncol. 2013, 131, 410–415. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, L.; Liu, Y.; Wang, S.; Shang, P.; Gao, Y.; Chen, X. Preoperative Neutrophil-Lymphocyte Ratio Before Platelet-Lymphocyte Ratio Predicts Clinical Outcome in Patients With Cervical Cancer Treated with Initial Radical Surgery. Int. J. Gynecol. Cancer 2014, 24, 1319–1325. [Google Scholar] [CrossRef] [PubMed]
- Balkwill, F.; Mantovani, A.; Balkwill, F. Inflammation and cancer: Back to Virchow? Lancet 2001, 357, 539–545. [Google Scholar] [CrossRef]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef]
- Sato, K.; Fujii, Y.; Ono, M.; Nomura, H.; Shizume, K. Production of interleukin 1 alpha-like factor and colony-stimulating factor by a squamous cell carcinoma of the thyroid (T3M-5) derived from a patient with hypercalcemia and leukocytosis. Cancer Res. 1987, 47, 6474–6480. [Google Scholar]
- Nasser, S.M.; Choudry, U.H.; Nielsen, G.P.; Ott, M.J. A leukemoid reaction in a patient with a dedifferentiated liposarcoma. Surgery 2001, 129, 765–767. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Ono, K.; Ozeki, Y.; Tanaka, S.; Aida, S.; Okuno, Y. Production of Granulocyte--macrophage Colony-stimulating Factor in a Patient with Metastatic Chest Wall Large Cell Carcinoma. Jpn. J. Clin. Oncol. 1998, 28, 559–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wetzler, M.; Estrov, Z.; Talpaz, M.; Markowitz, A.; Gutterman, J.U.; Kurzrock, R. Granulocyte-macrophage colony-stimulating factor as a cause of paraneoplastic leukaemoid reaction in advanced transitional cell carcinoma. J. Intern. Med. 1993, 234, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, K.M.; Raman, A.K.; Tan, N.; Fakih, M.G. Leukemoid reaction in pancreatic cancer: A case report and review of the literature. JOP 2006, 7, 631–634. [Google Scholar]
- Mabuchi, S.; Matsumoto, Y.; Isohashi, F.; Yoshioka, Y.; Ohashi, H.; Morii, E.; Hamasaki, T.; Aozasa, K.; Mutch, D.G.; Kimura, T. Pretreatment leukocytosis is an indicator of poor prognosis in patients with cervical cancer. Gynecol. Oncol. 2011, 122, 25–32. [Google Scholar] [CrossRef]
- Hirasawa, K.; Kitamura, T.; Oka, T.; Matsushita, H. Bladder tumor producing granulocyte colony-stimulating factor and parathyroid hormone related protein. J. Urol. 2002, 167, 2130. [Google Scholar] [CrossRef]
- Takahashi, H.; Yasuda, A.; Ochi, N.; Sakamoto, M.; Takayama, S.; Wakasugi, T.; Funahashi, H.; Sawai, H.; Sato, M.; Akamo, Y.; et al. Granulocyte-colony stimulating factor producing rectal cancer. World J. Surg. Oncol. 2008, 6, 70. [Google Scholar] [CrossRef] [Green Version]
- Mabuchi, S.; Matsumoto, Y.; Morii, E.; Morishige, K.; Kimura, T. The First 2 Cases of Granulocyte Colony-stimulating Factor Producing Adenocarcinoma of the Uterine Cervix. Int. J. Gynecol. Pathol. 2010, 29, 483–487. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Mabuchi, S.; Muraji, M.; Morii, E.; Kimura, T. Squamous Cell Carcinoma of the Uterine Cervix Producing Granulocyte Colony-Stimulating Factor. Int. J. Gynecol. Cancer 2010, 20, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Mishalian, I.; Bayuh, R.; Levy, L.; Zolotarov, L.; Michaeli, J.; Fridlender, Z.G. Tumor-associated neutrophils (TAN) develop pro-tumorigenic properties during tumor progression. Cancer Immunol. Immunother. 2013, 62, 1745–1756. [Google Scholar] [CrossRef] [PubMed]
- Märkl, B.; Wieberneit, J.; Kretsinger, H.; Mayr, P.; Anthuber, M.; Arnholdt, H.M.; Schenkirsch, G. Number of Intratumoral T Lymphocytes Is Associated With Lymph Node Size, Lymph Node Harvest, and Outcome in Node-Negative Colon Cancer. Am. J. Clin. Pathol. 2016, 145, 826–883. [Google Scholar] [CrossRef] [PubMed]
- Noble, F.; Mellows, T.; Matthews, L.H.M.; Bateman, A.C.; Harris, S.; Underwood, T.J.; Byrne, J.P.; Bailey, I.S.; Sharland, D.M.; Kelly, J.J.; et al. Tumour infiltrating lymphocytes correlate with improved survival in patients with oesophageal adenocarcinoma. Cancer Immunol. Immunother. 2016, 65, 651–662. [Google Scholar] [CrossRef]
- Vaupel, P.; Höckel, M.; Mayer, A. Detection and Characterization of Tumor Hypoxia Using pO2 Histography. Antioxid. Redox Signal. 2007, 9, 1221–1236. [Google Scholar] [CrossRef]
- Harris, A.L. Hypoxia—A key regulatory factor in tumour growth. Nat. Rev. Cancer 2002, 2, 38–47. [Google Scholar] [CrossRef]
- Semenza, G.L. Targeting HIF-1 for cancer therapy. Nat. Rev. Cancer 2003, 3, 721–732. [Google Scholar] [CrossRef]
- Semenza, G.L. Hypoxia-inducible factors: Mediators of cancer progression and targets for cancer therapy. Trends Pharmacol. Sci. 2012, 33, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Menczer, J. Preoperative elevated platelet count and thrombocytosis in gynecologic malignancies. Arch. Gynecol. Obstet. 2017, 295, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.-F.; Huang, Y.; Lu, W.S.; Chen, Q.X. Preoperative platelet count in esophageal squamous cell carcinoma: Is it a prognostic factor? Langenbeck’s Arch. Surg. 2013, 398, 1115–1122. [Google Scholar] [CrossRef]
- Müller, B.G.; De Aretxabala, X.; Domingo, M.G. A Review of Recent Data in the Treatment of Gallbladder Cancer: What We Know, What We Do, and What Should Be Done. Am. Soc. Clin. Oncol. Educ. Book 2014, e165–e170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Placke, T.; Kopp, H.-G.; Salih, H.R. Modulation of Natural Killer Cell Anti-Tumor Reactivity by Platelets. J. Innate Immun. 2011, 3, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Bochner, B.H.; Kattan, M.W.; Vora, K.C. Postoperative Nomogram Predicting Risk of Recurrence after Radical Cystectomy for Bladder Cancer. J. Clin. Oncol. 2006, 24, 3967–3972. [Google Scholar]
- Steyerberg, E.W.; Roobol, M.; Kattan, M.W.; Van Der Kwast, T.; De Koning, H.; Schroder, F. Prediction of Indolent Prostate Cancer: Validation and Updating of a Prognostic Nomogram. J. Urol. 2007, 177, 107–112. [Google Scholar] [CrossRef]
- Wierda, W.G.; O’Brien, S.; Wang, X.; Faderl, S.; Ferrajoli, A.; Do, K.-A.; Cortes, J.; Thomas, D.; Garcia-Manero, G.; Koller, C.; et al. Prognostic nomogram and index for overall survival in previously untreated patients with chronic lymphocytic leukemia. Blood 2007, 109, 4679–4685. [Google Scholar] [CrossRef]
- Alran, S.; Institut Curie Breast Cancer Study Group; De Rycke, Y.; Fourchotte, V.; Charitansky, H.; Laki, F.; Falcou, M.C.; Benamor, M.; Fréneaux, P.; Salmon, R.J.; et al. Validation and Limitations of Use of a Breast Cancer Nomogram Predicting the Likelihood of Non–Sentinel Node Involvement After Positive Sentinel Node Biopsy. Ann. Surg. Oncol. 2007, 14, 2195–2201. [Google Scholar]
- Karakiewicz, P.I.; Briganti, A.; Chun, F.K.-H.; Trinh, Q.-D.; Perrotte, P.; Ficarra, V.; Cindolo, L.; De La Taille, A.; Tostain, J.; Mulders, P.F.; et al. Multi-Institutional Validation of a New Renal Cancer–Specific Survival Nomogram. J. Clin. Oncol. 2007, 25, 1316–1322. [Google Scholar] [CrossRef]
- Iasonos, A.; Schrag, D.; Raj, G.V.; Panageas, K.S. How To Build and Interpret a Nomogram for Cancer Prognosis. J. Clin. Oncol. 2008, 26, 1364–1370. [Google Scholar] [CrossRef]
- Gunter, M.J.; Stolzenberg-Solomon, R.Z.; Cross, A.J.; Leitzmann, M.F.; Weinstein, S.; Wood, R.J.; Virtamo, J.; Taylor, P.R.; Albanes, D.; Sinha, R. A Prospective Study of Serum C-Reactive Protein and Colorectal Cancer Risk in Men. Cancer Res. 2006, 66, 2483–2487. [Google Scholar] [CrossRef] [Green Version]
- Shiu, Y.-C.; Lin, J.-K.; Huang, C.-J.; Jiang, J.-K.; Wang, L.-W.; Huang, H.-C.; Yang, S.-H. Is C-Reactive Protein a Prognostic Factor of Colorectal Cancer? Dis. Colon Rectum 2008, 51, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Siemes, C.; Visser, L.E.; Coebergh, J.-W.W.; Splinter, T.A.; Witteman, J.C.; Uitterlinden, A.G.; Hofman, A.; Pols, H.A.; Stricker, B.H. C-Reactive Protein Levels, Variation in the C-Reactive Protein Gene, and Cancer Risk: The Rotterdam Study. J. Clin. Oncol. 2006, 24, 5216–5222. [Google Scholar] [CrossRef] [PubMed]
- Khandavilli, S.D.; Ceallaigh, P.Ó.; Lloyd, C.J.; Whitaker, R. Serum C-reactive protein as a prognostic indicator in patients with oral squamous cell carcinoma. Oral Oncol. 2009, 45, 912–914. [Google Scholar] [CrossRef] [PubMed]
- Jablonska, E.; Piotrowski, L.; Grabowska, Z. Serum Levels of IL-lβ, IL-6, TNF-α, sTNF-RI and CRP in Patients with oral cavity cancer. Pathol. Oncol. Res. 1997, 3, 126–129. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (N = 1443) | ||
|---|---|---|
| Age (years) | 48 | (41–57) |
| FIGO stage | ||
| IB1/IIA | 1274 | (88.3%) |
| IB2 | 167 | (11.6%) |
| Missing data | 2 | (0.1%) |
| Histology | ||
| Squamous cell carcinoma | 1089 | (75.5%) |
| Adenocarcinoma | 277 | (19.2%) |
| Adenosquamous carcinoma | 75 | (5.2%) |
| Missing data | 2 | (0.1%) |
| Lymphovascular space invasion | ||
| Negative | 791 | (54.8%) |
| Positive | 562 | (38.9%) |
| Missing data | 90 | (6.2%) |
| Depth of stromal invasion | ||
| Superficial 1/3 | 445 | (30.8%) |
| Middle 1/3 | 380 | (26.3%) |
| Deeper 1/3 | 577 | (40.0%) |
| Missing data | 41 | (2.8%) |
| Depth of stromal invasion | ||
| Superficial 1/2 | 642 | (44.5%) |
| Deeper 1/2 | 758 | (52.5%) |
| Missing data | 43 | (3.0%) |
| Lymph node metastasis | ||
| No lymph node metastasis | 1177 | (81.6%) |
| Pelvic lymph node metastasis | 239 | (16.6%) |
| Para-aortic lymph node metastasis | 22 | (1.5%) |
| Missing data | 5 | (0.3%) |
| Parametrial invasion | ||
| Negative | 1323 | (91.7%) |
| Positive | 116 | (8.0%) |
| Missing data | 4 | (0.3%) |
| Resection margin free | ||
| Resection margin negative | 1381 | (95.7%) |
| Resection margin (carcinoma in situ) | 16 | (1.1%) |
| Resection margin (cancer) | 44 | (3.0%) |
| Missing data | 2 | (0.1%) |
| Tumor size (cm) | 2.7 | (1.6–4.0) |
| White blood cell (×1000 cells/mm3) | 6.2 | (5.2–7.5) |
| Lymphocyte (×10%) | 1.9 | (1.5–2.3) |
| Monocyte (×10%) | 0.4 | (0.3–0.5) |
| Neutrophil (×1000 cells/mm2) | 3.6 | (2.7–4.6) |
| Glucose (milligrams/deciliter) | 100.0 | (91.0–111.0) |
| Hemoglobin (grams/deciliter) | 12.7 | (11.8–13.4) |
| Platelet (×10,000 cells/mm2) | 25.2 | (21.5–29.8) |
| Neutrophil-lymphocyte ratio (NLR) | 1.9 | (1.4–2.6) |
| Platelet-lymphocyte ratio (PLR) | 13.5 | (10.6–17.0) |
| Hazard Ratio | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|
| Lower Limit | Upper Limit | |||
| Lymphocyte | 0.74 | 0.55 | 0.99 | 0.046 |
| Platelet | 1.03 | 1.01 | 1.05 | 0.009 |
| Hazard Ratio | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|
| Lower Limit | Upper Limit | |||
| WBC § | 0.60 | 0.41 | 0.88 | 0.010 |
| Neutrophil | 1.66 | 1.11 | 2.49 | 0.014 |
| Platelet | 1.05 | 1.02 | 1.08 | 0.002 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noh, J.J.; Lim, M.C.; Kim, M.-H.; Kim, Y.H.; Song, E.S.; Seong, S.J.; Suh, D.H.; Lee, J.-M.; Lee, C.; Choi, C.H. The Prognostic Model of Pre-Treatment Complete Blood Count (CBC) for Recurrence in Early Cervical Cancer. J. Clin. Med. 2020, 9, 2960. https://doi.org/10.3390/jcm9092960
Noh JJ, Lim MC, Kim M-H, Kim YH, Song ES, Seong SJ, Suh DH, Lee J-M, Lee C, Choi CH. The Prognostic Model of Pre-Treatment Complete Blood Count (CBC) for Recurrence in Early Cervical Cancer. Journal of Clinical Medicine. 2020; 9(9):2960. https://doi.org/10.3390/jcm9092960
Chicago/Turabian StyleNoh, Joseph J., Myong Cheol Lim, Moon-Hong Kim, Yun Hwan Kim, Eun Seop Song, Seok Ju Seong, Dong Hoon Suh, Jong-Min Lee, Chulmin Lee, and Chel Hun Choi. 2020. "The Prognostic Model of Pre-Treatment Complete Blood Count (CBC) for Recurrence in Early Cervical Cancer" Journal of Clinical Medicine 9, no. 9: 2960. https://doi.org/10.3390/jcm9092960