Risks According to the Timing and Frequency of Hypotension Episodes in Postanoxic Comatose Patients

 , , and
on behalf of the Korean Hypothermia Network Investigators
, , and
on behalf of the Korean Hypothermia Network Investigators
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
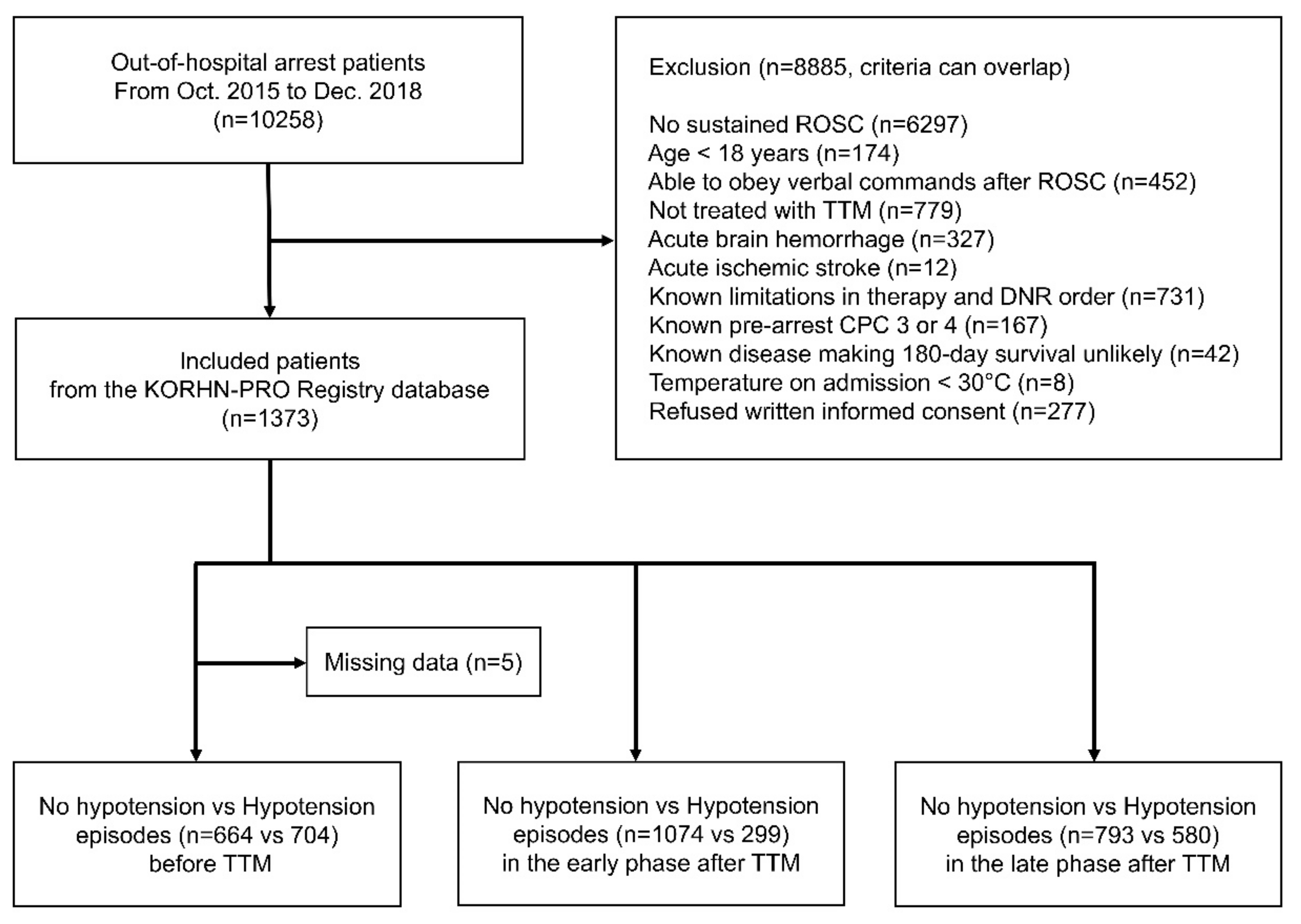
2.2. Study Population
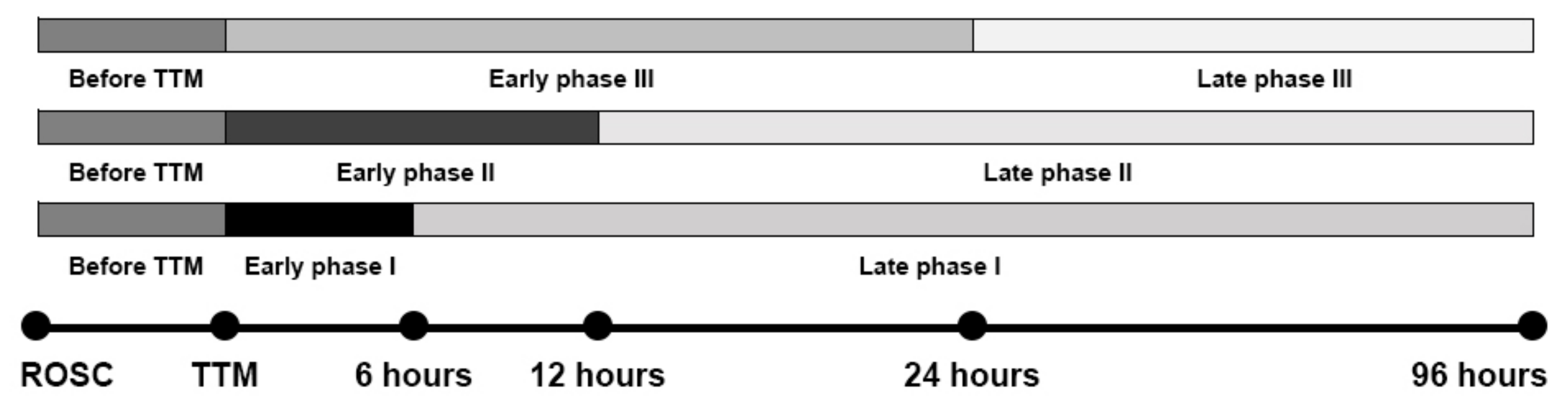
2.3. Variables and Endpoints
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. The Overall Results
4.2. Hypotension Episodes and Unfavorable Neurological Outcome in Cardiac Arrest Patients
4.3. Hypotension Episodes in the Early Phase after Targeted Temperature Management (TTM) Initiation
4.4. Vasoactive Agents and Fluids
4.5. Complications Due to Hypotension Episodes and TTM
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jentzer, J.C.; Chonde, M.D.; Dezfulian, C. Myocardial dysfunction and shock after cardiac arrest. BioMed Res. Int. 2015, 2015, 314796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurent, I.; Monchi, M.; Chiche, J.D.; Joly, L.M.; Spaulding, C.; Bourgeois, B.é.; Cariou, A.; Rozenberg, A.; Carli, P.; Weber, S.; et al. Reversible myocardial dysfunction in survivors of out-of-hospital cardiac arrest. J. Am. Coll. Cardiol. 2002, 40, 2110–2116. [Google Scholar] [CrossRef] [Green Version]
- Geurts, M.; Macleod, M.R.; Kollmar, R.; Kremer, P.H.C.; van der Worp, H.B. Therapeutic hypothermia and the risk of infection. Crit. Care Med. 2014, 42, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Daviaud, F.; Dumas, F.; Demars, N.; Geri, G.; Bouglé, A.; Morichau-Beauchant, T.; Nguyen, Y.L.; Bougouin, W.; Pène, F.; Charpentier, J.; et al. Blood glucose level and outcome after cardiac arrest: Insights from a large registry in the hypothermia era. Intensive Care Med. 2014, 40, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.; Sunde, K.; Hovdenes, J.; Riker, R.R.; Rubertsson, S.; Stammet, P.; Nilsson, F.; Friberg, H. Adverse events and their relation to mortality in out-of-hospital cardiac arrest patients treated with therapeutic hypothermia. Crit. Care Med. 2011, 39, 57–64. [Google Scholar] [CrossRef]
- Huang, C.H.; Tsai, M.S.; Ong, H.N.; Chen, W.; Wang, C.H.; Chang, W.T.; Wang, T.D.; Chen, S.C.; Ma, M.H.M.; Chen, W.J. Association of hemodynamic variables with in-hospital mortality and favorable neurological outcomes in post-cardiac arrest care with targeted temperature management. Resuscitation 2017, 120, 146–152. [Google Scholar] [CrossRef]
- Oh, J.H.; Lee, D.H.; Cho, I.S.; Youn, C.S.; Lee, B.K.; Wee, J.H.; Cha, K.C.; Chae, M.K.; Shin, J. Korean Hypothermia Network Investigators. Association between acute kidney injury and neurological outcome or death at 6 months in out-of-hospital cardiac arrest: A prospective, multicenter, observational cohort study. J. Crit. Care 2019, 54, 197–204. [Google Scholar] [CrossRef]
- Nolan, J.P.; Soar, J.; Cariou, A.; Cronberg, T.; Moulaert, V.R.M.; Deakin, C.D.; Bottiger, B.W.; Friberg, H.; Sunde, K.; Sandroni, C.; et al. European Resuscitation Council and European Society of Intensive Care Medicine 2015 guidelines for post-resuscitation care. Intensive Care Med. 2015, 41, 2039–2056. [Google Scholar] [CrossRef]
- Callaway, C.W.; Donnino, M.W.; Fink, E.L.; Geocadin, R.G.; Golan, E.; Kern, K.B.; Leary, M.; Meurer, W.J.; Peberdy, M.A.; Thompson, T.M.; et al. Part 8: Post-Cardiac Arrest Care: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S465–S482. [Google Scholar] [CrossRef] [Green Version]
- Annborn, M.; Bro-Jeppesen, J.; Nielsen, N.; Ullén, S.; Kjaergaard, J.; Hassager, C.; Wanscher, M.; Hovdenes, J.; Pellis, T.; Pelosi, P.; et al. The association of targeted temperature management at 33 and 36 °C with outcome in patients with moderate shock on admission after out-of-hospital cardiac arrest: A post hoc analysis of the target temperature management trial. Intensive Care Med. 2014, 40, 1210–1219. [Google Scholar] [CrossRef]
- Kim, Y.M.; Youn, C.S.; Kim, S.H.; Lee, B.K.; Cho, I.S.; Cho, G.C.; Jeung, K.W.; Oh, S.H.; Choi, S.P.; Shin, J.H.; et al. Adverse events associated with poor neurological outcome during targeted temperature management and advanced critical care after out-of-hospital cardiac arrest. Crit. Care 2015, 19, 283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bro-Jeppesen, J.; Annborn, M.; Hassager, C.; Wise, M.P.; Pelosi, P.; Nielsen, N.; Erlinge, D.; Wanscher, M.; Friberg, H.; Kjaergaard, J. The association between systolic blood pressure on arrival at hospital and outcome in adults surviving from out-of-hospital cardiac arrests of presumed cardiac aetiologyHemodynamics and vasopressor support during targeted temperature management at 33 °C versus 36 °C after out-of-hospital cardiac arrest: A post hoc study of the target temperature management trial. Crit. Care Med. 2015, 43, 318–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trzeciak, S.; Jones, A.E.; Kilgannon, J.H.; Milcarek, B.; Hunter, K.; Shapiro, N.I.; Hollenberg, S.M.; Dellinger, R.P.; Parrillo, J.E. Significance of arterial hypotension after resuscitation from cardiac arrest. Crit. Care Med. 2009, 37, 2895–2903. [Google Scholar] [CrossRef] [PubMed]
- Bray, J.E.; Bernard, S.; Cantwell, K.; Stephenson, M.; Smith, K.; VACAR Steering Committee. The association between systolic blood pressure on arrival at hospital and outcome in adults surviving from out-of-hospital cardiac arrests of presumed cardiac aetiology. Resuscitation 2014, 85, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Chiu, Y.K.; Lui, C.T.; Tsui, K.L. Impact of hypotension after return of spontaneous circulation on survival in patients of out-of-hospital cardiac arrest. Am. J. Emerg. Med. 2018, 36, 79–83. [Google Scholar] [CrossRef]
- Pitcher, J.H.; Dziodzio, J.; Keller, J.; May, T.; Riker, R.R.; Seder, D.B. Hemodynamic, biochemical, and ventilatory parameters are independently associated with outcome after cardiac arrest. Neurocrit. Care 2018, 29, 69–76. [Google Scholar] [CrossRef]
- Perkins, G.D.; Jacobs, I.G.; Nadkarni, V.M.; Berg, R.A.; Bhanji, F.; Biarent, D.; Bossaert, L.L.; Brett, S.J.; Chamberlain, D.; de Caen, A.R.; et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: Update of the utstein resuscitation registry templates for out-of-hospital cardiac arrest: A statement for healthcare professionals from a task force of the international liaison committee on resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Resuscitation 2015, 96, 328–340. [Google Scholar] [CrossRef]
- Topjian, A.A.; Telford, R.; Holubkov, R.; Nadkarni, V.M.; Berg, R.A.; Dean, J.M.; Moler, F.W.; Therapeutic Hypothermia After Pediatric Cardiac Arrest (THAPCA) Trial Investigators. Association of early postresuscitation hypotension with survival to discharge after targeted temperature management for pediatric out-of-hospital cardiac arrest: Secondary analysis of a randomized clinical trial. JAMA Pediatr. 2018, 172, 143–153. [Google Scholar] [CrossRef]
- Lemiale, V.; Dumas, F.; Mongardon, N.; Giovanetti, O.; Charpentier, J.; Chiche, J.D.; Carli, P.; Mira, J.P.; Nolan, J.; Cariou, A. Intensive care unit mortality after cardiac arrest: The relative contribution of shock and brain injury in a large cohort. Intensive Care Med. 2013, 39, 1972–1980. [Google Scholar] [CrossRef]
- Kaji, A.H.; Hanif, A.M.; Thomas, J.L.; Niemann, J.T. Out-of-hospital cardiac arrest: Early in-hospital hypotension versus out-of-hospital factors in predicting in-hospital mortality among those surviving to hospital admission. Resuscitation 2011, 82, 1314–1317. [Google Scholar] [CrossRef]
- Kilgannon, J.H.; Roberts, B.W.; Reihl, L.R.; Chansky, M.E.; Jones, A.E.; Dellinger, R.P.; Parrillo, J.E.; Trzeciak, S. Early arterial hypotension is common in the post-cardiac arrest syndrome and associated with increased in-hospital mortality. Resuscitation 2008, 79, 410–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, G.; Kim, Y.J.; Lee, S.H.; Ryoo, S.M.; Kim, W.Y. Optimal hemodynamic parameter to predict the neurological outcome in out-of-hospital cardiac arrest survivors treated with target temperature management. Ther. Hypothermia Temp. Manag. 2019. [Google Scholar] [CrossRef] [PubMed]
- Bisschops, L.L.A.; Hoedemaekers, C.W.E.; Simons, K.S.; van der Hoeven, J.G. Preserved metabolic coupling and cerebrovascular reactivity during mild hypothermia after cardiac arrest. Crit. Care Med. 2010, 38, 1542–1547. [Google Scholar] [CrossRef] [PubMed]
- Stretti, F.; Gotti, M.; Pifferi, S.; Brandi, G.; Annoni, F.; Stocchetti, N. Body temperature affects cerebral hemodynamics in acutely brain injured patients: An observational transcranial color-coded duplex sonography study. Crit. Care 2014, 18, 552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundgreen, C.; Larsen, F.S.; Herzog, T.M.; Knudsen, G.M.; Boesgaard, S.; Aldershvile, J. Autoregulation of cerebral blood flow in patients resuscitated from cardiac arrest. Stroke 2001, 32, 128–132. [Google Scholar] [CrossRef] [Green Version]
- Torgersen, C.; Meichtry, J.; Schmittinger, C.A.; Bloechlinger, S.; Jakob, S.M.; Takala, J.; Dünser, M.W. Haemodynamic variables and functional outcome in hypothermic patients following out-of-hospital cardiac arrest. Resuscitation 2013, 84, 798–804. [Google Scholar] [CrossRef]
- Bro-Jeppesen, J.; Kjaergaard, J.; Søholm, H.; Wanscher, M.; Lippert, F.K.; Møller, J.E.; Køber, L.; Hassager, C. Hemodynamics and vasopressor support in therapeutic hypothermia after cardiac arrest: Prognostic implica-tions. Resuscitation 2014, 85, 664–670. [Google Scholar] [CrossRef]
- Beylin, M.E.; Perman, S.M.; Abella, B.M.; Leary, M.; Shofer, F.S.; Grossestreuer, A.V.; Gaieski, D.F. Higher mean arterial pressure with or without vasoactive agents is associated with increased survival and better neurological outcomes in comatose survivors of cardiac arrest. Intensive Care Med. 2013, 39, 1981–1988. [Google Scholar] [CrossRef]
- Bergman, R.; Braber, A.; Adriaanse, M.A.; van Vugt, R.; Tjan, D.H.; van Zanten, A.R. Haemodynamic consequences of mild therapeutic hypothermia after cardiac arrest. Eur. J. Anaesthesiol. 2010, 27, 383–387. [Google Scholar] [CrossRef]
- Stær-Jensen, H.; Sunde, K.; Olasveengen, T.M.; Jacobsen, D.; Drægni, T.; Nakstad, E.R.; Eritsland, J.; Andersen, G.Ø. Bradycardia during therapeutic hypothermia is associated with good neurologic outcome in comatose survivors of out-of-hospital cardiac arrest. Crit. Care Med. 2014, 42, 2401–2408. [Google Scholar] [CrossRef]
- Thomsen, J.H.; Hassager, C.; Bro-Jeppesen, J.; Søholm, H.; Nielsen, N.; Wanscher, M.; Køber, L.; Pehrson, S.; Kjaergaard, J. Sinus bradycardia during hypothermia in comatose survivors of out-of-hospital cardiac arrest—A new early marker of favorable outcome? Resuscitation 2015, 89, 36–42. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 1368) | No Hypotension Before TTM (n = 664) | Hypotension Before TTM (n = 704) | p-Value 5 |
|---|---|---|---|---|
| Age, years | 62 (51, 74) | 61 (49, 72) | 64 (53, 76) | <0.001 |
| Male, n (%) | 974 (71.2) | 484 (72.9) | 490 (69.6) | 0.189 |
| BMI, kg/m2 | 23.4 (20.9, 25.7) | 23.4 (21.1, 25.7) | 23.3 (20.8, 25.4) | 0.163 |
| Systolic blood pressure, mmHg | 120 (90, 154) | 130 (104,161) | 110 (80, 147) | <0.001 |
| Witness arrest, n (%) | 946 (69.2) | 489 (74.5) | 457 (65.6) | <0.001 |
| Bystander CPR, n (%) | 840 (61.4) | 406 (62.2) | 434 (62.4) | 0.955 |
| Time from arrest to CPR initiation, minutes | 1 (0, 7) | 1 (0, 7) | 1 (0, 7) | 0.685 |
| Time from CPR initiation to ROSC, minutes | 25 (15, 38) | 22 (12, 34) | 30 (18, 43) | <0.001 |
| Time from ROSC to TTM initiation, hours | 3.4 (2.2, 4.9) | 3.4 (2.1, 4.9) | 3.4 (2.2, 4.8) | 0.53 |
| Initial prehospital ECG rhythm | <0.001 | |||
| Asystole, n (%) | 444 (32.5) | 185 (30.8) | 259 (43.1) | |
| PEA, n (%) | 268 (19.6) | 127 (21.1) | 141 (23.5) | |
| Pulseless VT, n (%) | 15 (1.1) | 10 (1.7) | 5 (0.8) | |
| VF, n (%) | 448 (32.7) | 270 (44.9) | 178 (29.6) | |
| Already achieved ROSC at EMS arrival, n (%) | 27 (2) | 9 (1.5) | 18 (3) | |
| Previous history | ||||
| Cardiovascular disease 1, n (%) | 285 (20.8) | 145 (21.8) | 140 (19.9) | 0.375 |
| Neurologic disease 2, n (%) | 137 (10) | 60 (9) | 77 (10.9) | 0.242 |
| Pulmonary disease, n (%) | 106 (7.7) | 37 (5.6) | 69 (9.8) | 0.003 |
| Malignancy, n (%) | 80 (5.8) | 42 (6.3) | 38 (5.4) | 0.465 |
| Psychologic disease, n (%) | 50 (3.7) | 23 (3.5) | 27 (3.8) | 0.714 |
| Cardiac cause | 850 (62.1) | 431 (81.6) | 419 (78.5) | 0.219 |
| Causes of cardiac arrest | 0.13 | |||
| Medical, n (%) | 851 (62.2) | 432 (65.1) | 419 (59.5) | |
| Trauma, n (%) | 28 (2) | 14 (2.1) | 14 (2) | |
| Submersion, n (%) | 19 (1.4) | 5 (0.8) | 14 (2) | |
| Electrocution, n (%) | 6 (0.4) | 3 (0.5) | 3 (0.4) | |
| Drug overdose, n (%) | 15 (1.1) | 5 (0.8) | 10 (1.4) | |
| Asphyxia, n (%) | 77 (0.56) | 29 (4.4) | 48 (6.8) | |
| Hanging, n (%) | 160 (11.7) | 79 (11.9) | 81 (11.5) | |
| Others, n (%) | 112 (8.2) | 97 (14.6) | 115 (16.3) | |
| PCI, n (%) | 207 (15.1) | 112 (41) | 95 (41.7) | 0.478 |
| Four score 3 | 0 (0, 3) | 1 (0, 4) | 0 (0, 2) | <0.001 |
| Cardiovascular SOFA 4 at day 1 | 4 (2, 4) | 3 (0, 4) | 4 (4, 4) | <0.001 |
| Total dose of dopamine, µg/kg | 5605 (1651, 21,600) | 3553 (1104, 19,200) | 6489 (1834, 22,941) | 0.012 |
| Total dose of norepinephrine, µg/kg | 108 (30, 360) | 50 (18, 182.4) | 162 (48, 576) | <0.001 |
| Total dose of vasopressin, IU/min | 31 (7, 113) | 31 (7, 118) | 32 (7.2, 108) | 0.919 |
| Total dose of epinephrine, µg/kg | 68 (18, 271) | 57 (16, 145) | 70 (18.3, 308) | 0.566 |
| Total dose of dobutamine, µg/kg | 3600 (800, 15,969) | 3480 (959, 12,789) | 3996 (719, 16,709) | 0.966 |
| Input/output at day 1, mL | 453 (−354, 1725) | 46 (−647, 1078) | 935 (−37, 2341) | <0.001 |
| Initial lactate, mg/dL | 9.7 (6.1, 12.9) | 8.5 (4.8, 11.5) | 10.9 (7.5, 14.1) | <0.001 |
| Initial creatinine, mg/dL | 1.3 (1.1, 1.8) | 1.2 (1, 1.6) | 1.4 (1.1, 2.1) | <0.001 |
| Target temperature, °C | 33 (33, 34) | 33 (33, 33) | 33 (33, 35) | <0.001 |
| Duration of TTM, hours | 24 (24, 24) | 24 (24, 24) | 24 (24, 24) | 0.018 |
| CPC 3–5, n (%) | 940 (68.8) | 380 (57.3) | 560 (79.5) | <0.001 |
| Variable | All Patients (n = 1368) | No Hypotension Before TTM (n = 664) | Hypotension Before TTM (n = 704) | p-Value 5 |
|---|---|---|---|---|
| Seizure, n (%) | 325 (23.8) | 144 (21.7) | 181 (25.7) | 0.077 |
| Significant bleeding, n (%) | 65 (4.8) | 25 (3.8) | 40 (5.7) | 0.115 |
| Significant infection 1, n (%) | 117 (8.6) | 23 (3.5) | 94 (13.4) | <0.001 |
| RRT 2, n (%) | 248 (18.1) | 89 (13.4) | 159 (22.8) | <0.001 |
| Hypokalemia, n (%) | 448 (32.7) | 206 (31.1) | 242 (34.5) | 0.173 |
| Hypophosphatemia, n (%) | 433 (31.7) | 205 (31.2) | 228 (33.1) | 0.467 |
| Hypomagnesemia, n (%) | 368 (26.9) | 177 (27.2) | 191 (27.9) | 0.816 |
| Hypoglycemia, n (%) | 153 (11.2) | 45 (6.8) | 108 (15.5) | <0.001 |
| Hyperglycemia, n (%) | 706 (51.6) | 283 (42.8) | 423 (60.6) | <0.001 |
| Tachycardia 3, n (%) | 79 (5.8) | 27 (4.1) | 56 (8) | 0.003 |
| Bradycardia 4, n (%) | 96 (7) | 44 (6.7) | 52 (7.4) | 0.614 |
| Rearrest, n (%) | 259 (18.9) | 82 (12.3) | 177 (25.2) | <0.001 |
| ICU length of stay in survivors, days | 34.1 (16.9, 50.5) | 34.9 (17.9, 50.9) | 32.5 (15.3, 50.2) | 0.133 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.H.; Lee, J.H.; Seo, J.I.; Lee, D.H.; Kim, W.Y.; Lee, B.K., on behalf of the Korean Hypothermia Network Investigators. Risks According to the Timing and Frequency of Hypotension Episodes in Postanoxic Comatose Patients. J. Clin. Med. 2020, 9, 2750. https://doi.org/10.3390/jcm9092750
Kim YH, Lee JH, Seo JI, Lee DH, Kim WY, Lee BK on behalf of the Korean Hypothermia Network Investigators. Risks According to the Timing and Frequency of Hypotension Episodes in Postanoxic Comatose Patients. Journal of Clinical Medicine. 2020; 9(9):2750. https://doi.org/10.3390/jcm9092750
Chicago/Turabian StyleKim, Yong Hwan, Jae Hoon Lee, Jung In Seo, Dong Hoon Lee, Won Young Kim, and Byung Kook Lee on behalf of the Korean Hypothermia Network Investigators. 2020. "Risks According to the Timing and Frequency of Hypotension Episodes in Postanoxic Comatose Patients" Journal of Clinical Medicine 9, no. 9: 2750. https://doi.org/10.3390/jcm9092750