Impact of Intensive Glucose Control in Patients with Diabetes Mellitus Undergoing Percutaneous Coronary Intervention: 3-Year Clinical Outcomes

 , , ,
, , ,
Abstract
:
1. Introduction
2. Methods
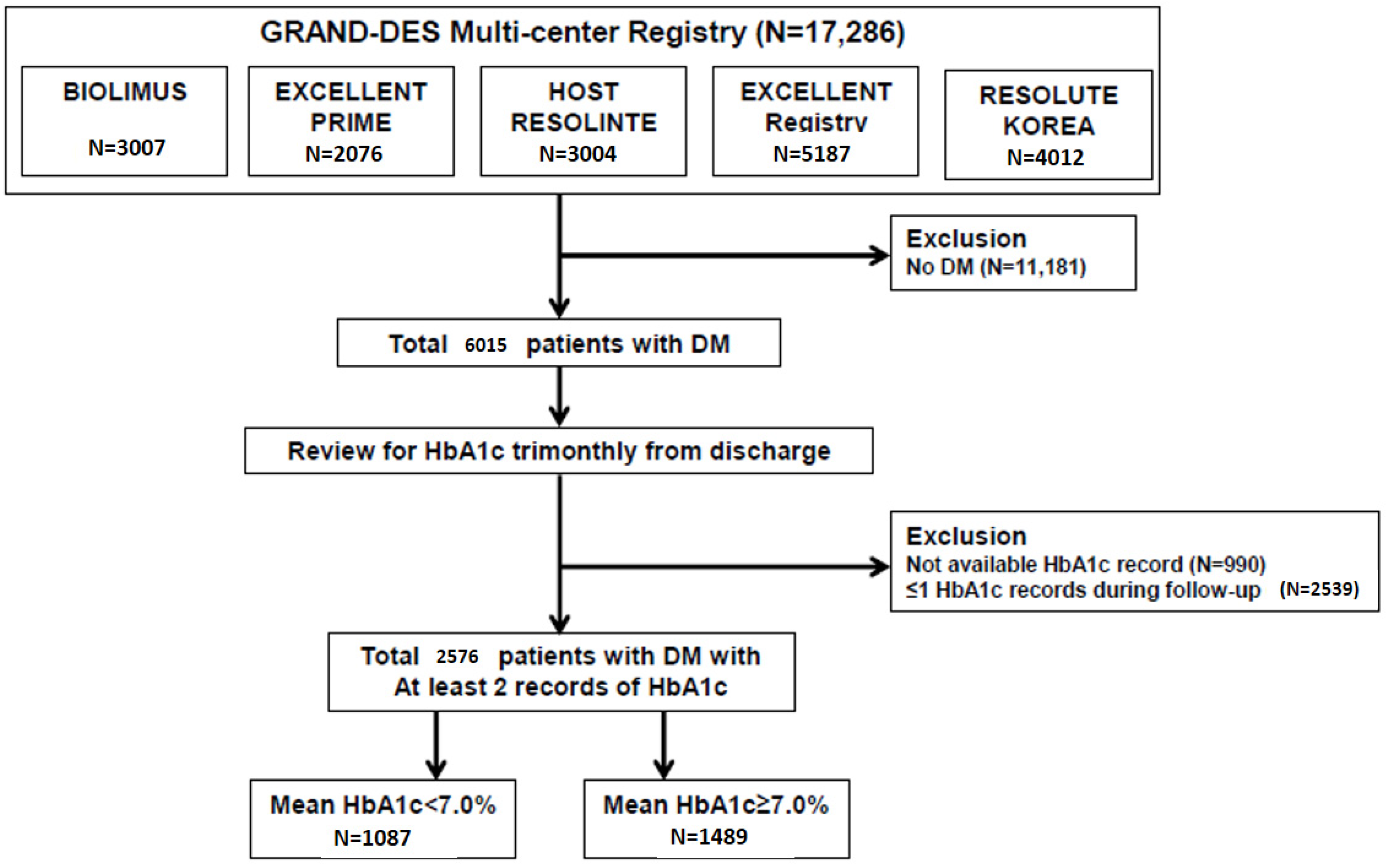
2.1. Data Source and Study Population
2.2. Statistical Analysis
3. Results
3.1. The Impact of Intensive Glucose Control with Mean HbA1c < 7.0% on Clinical Outcomes in Diabetic Patients after PCI: Whole Population
3.2. The Impact of Intensive Glucose Control with Mean HbA1c < 7.0% on Clinical Outcomes in Diabetic Patients after PCI: Propensity-Matched 516 Pairs
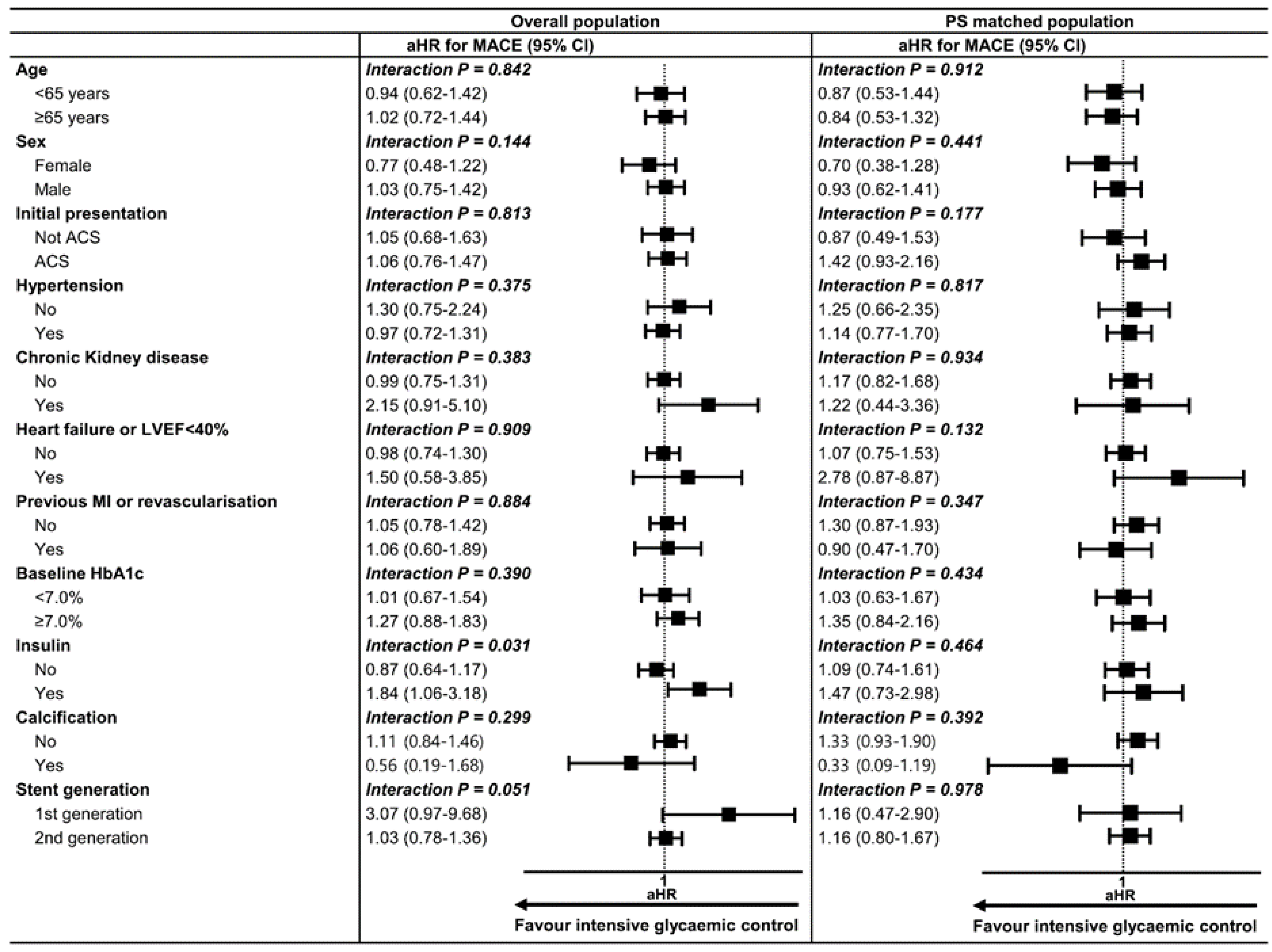
3.3. Subgroup Analysis of MACE
3.4. The impact of ‘Stable’ Glucose Control on Clinical Outcome after PCI
3.5. The Impact of ‘More Intensive’ Glucose Control on Clinical Outcome after PCI
4. Discussion
4.1. An HbA1c Goal to Reduce the Risk of Macrovascular Complications
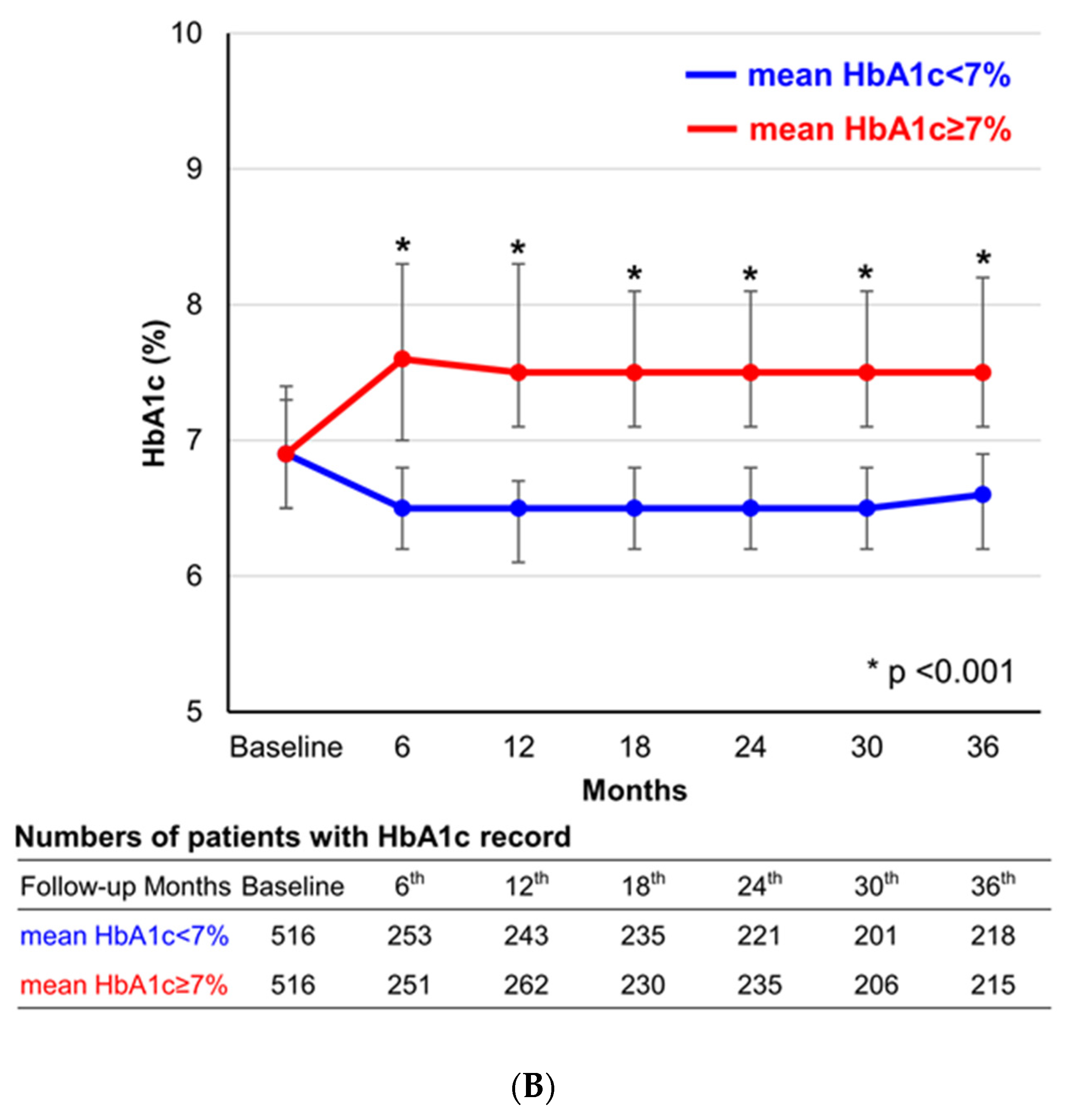
4.2. The Impact of Follow-up Glycemic Control after PCI on Clinical Outcomes in Diabetic Patients
4.3. Benefits of New Generation Glucose-Lowering Agents: SGLT2 Inhibitors and GLP-1 Receptor Agonists
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Authors/Task Force Members; Rydén, L.; Grant, P.J.; Anker, S.D.; Berne, C.; Cosentino, F.; Danchin, N.; Escaned, J.; Hammes, H.-P.; Huikuri, H.; et al. ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD.: The Task Force on diabetes, pre-diabetes, and cardiovascular diseases of the European Society of Cardiology (ESC) and developed in collaboration with the European Association for the Study of Diabetes (EASD). Eur. Hear. J. 2013, 34, 3035–3087. [Google Scholar] [CrossRef] [Green Version]
- Flaherty, J.D.; Davidson, C.J. Diabetes and coronary revascularization. JAMA 2005, 293, 1501–1508. [Google Scholar] [CrossRef]
- Lee, T.T.; Feinberg, L.; Baim, D.S.; Holmes, D.R.; Aroesty, J.M.; Carrozza, J.P.; Cohen, D.J.; Ho, K.K.; Cutlip, D.E. Effect of Diabetes Mellitus on Five-Year Clinical Outcomes After Single-Vessel Coronary Stenting (a Pooled Analysis of Coronary Stent Clinical Trials). Am. J. Cardiol. 2006, 98, 718–721. [Google Scholar] [CrossRef]
- Nakatani, D.; Sakata, Y.; Mizuno, H.; Shimizu, M.; Suna, S.; Usami, M.; Ito, H.; Yasumura, Y.; Hirayama, A.; Takeda, H.; et al. Impact of Diabetes Mellitus on Rehospitalization for Heart Failure Among Survivors of Acute Myocardial Infarction in the Percutaneous Coronary Intervention Era. Circ. J. 2009, 73, 662–666. [Google Scholar] [CrossRef] [Green Version]
- ADVANCE Collaborative Group; Patel, A.; MacMahon, S.; Chalmers, J.P.; Neal, B.; Billot, L.; Woodward, M.; Marre, M.; Cooper, M.; Glasziou, P.; et al. Intensive Blood Glucose Control and Vascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2008, 358, 2560–2572. [Google Scholar] [PubMed] [Green Version]
- Action to Control Cardiovascular Risk in Diabetes Study Group; Gerstein, H.C.; Miller, M.E.; Byington, R.P.; Goff, D.C., Jr.; Bigger, J.T.; Buse, J.B.; Cushman, W.C.; Genuth, S.; Ismail-Beigi, F.; et al. Effects of intensive glucose lowering in type 2 diabetes. N. Engl. J. Med. 2008, 358, 2545–2559. [Google Scholar] [PubMed] [Green Version]
- Duckworth, W.; Abraira, C.; Moritz, T.; Reda, D.; Emanuele, N.; Reaven, P.D.; Zieve, F.J.; Marks, J.; Davis, S.N.; Hayward, R.; et al. Glucose control and vascular complications in veterans with type 2 diabetes. N. Engl. J. Med. 2009, 360, 129–139. [Google Scholar] [CrossRef] [Green Version]
- Ike, A.; Nishikawa, H.; Shirai, K.; Mori, K.; Kuwano, T.; Fukuda, Y.; Takamiya, Y.; Yanagi, D.; Kubota, K.; Tsuchiya, Y.; et al. Impact of glycemic control on the clinical outcome in diabetic patients with percutaneous coronary intervention—From the FU-registry. Circ. J. 2011, 75, 791–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassaian, S.E.; Goodarzynejad, H.; Boroumand, M.; Salarifar, M.; Masoudkabir, F.; Tehrani, M.M.; Pourhoseini, H.; Sadeghian, S.; Ramezanpour, N.; Alidoosti, M.; et al. Glycosylated hemoglobin (HbA1c) levels and clinical outcomes in diabetic patients following coronary artery stenting. Cardiovasc. Diabetol. 2012, 11, 82. [Google Scholar] [CrossRef] [Green Version]
- Hwang, J.K.; Lee, S.-H.; Bin Song, Y.; Ahn, J.; Carriere, K.; Jang, M.J.; Park, T.K.; Choi, S.-H.; Yang, J.H.; Choi, J.-H.; et al. Glycemic Control Status After Percutaneous Coronary Intervention and Long-Term Clinical Outcomes in Patients With Type 2 Diabetes Mellitus. Circ. Cardiovasc. Interv. 2017, 10, e004157. [Google Scholar] [CrossRef]
- Parsons, L.S. Reducing Bias in a Propensity Score Matched-Pair Sample Using Greedy Matching Techniques. In Proceedings of the Twenty-Sixth Annual SAS Users Group International Conference, Cary, NC, USA, 22–25 April 2001; pp. 214–226. [Google Scholar]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [Green Version]
- Fihn, S.D.; Gardin, J.M.; Abrams, J.; Berra, K.; Blankenship, J.C.; Dallas, A.P.; Douglas, P.S.; Foody, J.M.; Gerber, T.C.; Hinderliter, A.L.; et al. ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: A report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation 2012, 126, e354–e471. [Google Scholar] [PubMed]
- Task Force Members; Montalescot, G.; Sechtem, U.; Achenbach, S.; Andreotti, F.; Arden, C.; Budaj, A.; Bugiardini, R.; Crea, F.; Cuisset, T.; et al. ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur. Hear. J. 2013, 34, 2949–3003. [Google Scholar] [CrossRef]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.E.; Grobbee, D.; Hansen, T.B.; et al. ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Hear. J. 2019, 41, 255–323. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Glycemic Targets: Standards of Medical Care in Diabetes—2019. Diabetes Care 2019, 42, S61–S70. [Google Scholar] [CrossRef] [Green Version]
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998, 352, 837–853. [Google Scholar] [CrossRef]
- Holman, R.R.; Paul, S.K.; Bethel, M.A.; Matthews, D.R.; Neil, H.A.W. 10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes. N. Engl. J. Med. 2008, 359, 1577–1589. [Google Scholar] [CrossRef] [Green Version]
- Reaven, P.D.; Emanuele, N.V.; Wiitala, W.L.; Bahn, G.D.; Reda, D.J.; McCarren, M.; Duckworth, W.C.; Hayward, R.A. VADT Investigators Intensive Glucose Control in Patients with Type 2 Diabetes-15-Year Follow-up. N. Engl. J. Med. 2019, 380, 2215–2224. [Google Scholar] [CrossRef]
- Corpus, R.A.; George, P.B.; House, J.A.; Dixon, S.R.; Ajluni, S.C.; Devlin, W.H.; Timmis, G.C.; Balasubramaniam, M.; O’Neill, W.W. Optimal glycemic control is associated with a lower rate of target vessel revascularization in treated type II diabetic patients undergoing elective percutaneous coronary intervention. J. Am. Coll. Cardiol. 2004, 43, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Ueda, H.; Mitsusada, N.; Harimoto, K.; Miyawaki, M.; Yasuga, Y.; Hiraoka, H. Glycosylated Hemoglobin Is a Predictor of Major Adverse Cardiac Events after Drug-Eluting Stent Implantation in Patients with Diabetes Mellitus. Cardiology 2010, 116, 51–57. [Google Scholar] [CrossRef]
- Kasai, T.; Miyauchi, K.; Kajimoto, K.; Kubota, N.; Kurata, T.; Daida, H. Influence of diabetes on >10-year outcomes after percutaneous coronary intervention. Hear. Vessel. 2008, 23, 149–154. [Google Scholar] [CrossRef]
- Cicek, G.; Uyarel, H.; Ergelen, M.; Ayhan, E.; Abanonu, G.B.; Eren, M.; Gibson, C.M. Hemoglobin A1c as a prognostic marker in patients undergoing primary angioplasty for acute myocardial infarction. Coron. Artery Dis. 2011, 22, 131–137. [Google Scholar] [CrossRef]
- Sharma, P.K.; Agarwal, S.; Ellis, S.G.; Goel, S.S.; Cho, L.; Tuzcu, E.M.; Lincoff, A.M.; Kapadia, S.R. Association of Glycemic Control With Mortality in Patients With Diabetes Mellitus Undergoing Percutaneous Coronary Intervention. Circ. Cardiovasc. Interv. 2014, 7, 503–509. [Google Scholar] [CrossRef] [Green Version]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; De Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R.; et al. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Santos-Gallego, C.G.; Requena-Ibanez, J.A.; Antonio, R.S.; Ishikawa, K.; Watanabe, S.; Picatoste, B.; Flores, E.; Garcia-Ropero, A.; Sanz, J.; Hajjar, R.J.; et al. Empagliflozin Ameliorates Adverse Left Ventricular Remodeling in Nondiabetic Heart Failure by Enhancing Myocardial Energetics. J. Am. Coll. Cardiol. 2019, 73, 1931–1944. [Google Scholar] [CrossRef]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husain, M.; Birkenfeld, A.L.; Donsmark, M.; Dungan, K.; Eliaschewitz, F.G.; Franco, D.R.; Jeppesen, O.K.; Lingvay, I.; Mosenzon, O.; Pedersen, S.D.; et al. Oral Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2019, 381, 841–851. [Google Scholar] [CrossRef] [Green Version]
- Das, S.R.; Everett, B.M.; Birtcher, K.K.; Brown, J.M.; Cefalu, W.T.; Januzzi, J.L.; Kalyani, R.R.; Kosiborod, M.; Magwire, M.L.; Morris, P.B.; et al. ACC Expert Consensus Decision Pathway on Novel Therapies for Cardiovascular Risk Reduction in Patients With Type 2 Diabetes and Atherosclerotic Cardiovascular Disease: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J. Am. Coll. Cardiol. 2018, 72, 3200–3223. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes—2019. Diabetes Care 2019, 43, S90–S102. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Population | PS Matched Population | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean HbA1c < 7.0% (N = 1087) | Mean HbA1c ≥ 7.0% (N = 1489) | p Value | ASD | Mean HbA1c < 7.0% (N = 516) | Mean HbA1c ≥ 7.0% (N = 516) | p Value | ASD | |
| Demographics | ||||||||
| Age | 67 (59–73) | 66 (58–72) | 0.190 | 0.050 | 67 (58–73) | 66 (59–72) | 0.733 | 0.059 |
| Male | 734 (67.5) | 957 (64.3) | 0.093 | 0.033 | 343 (66.5) | 350 (67.8) | 0.691 | 0.008 |
| BMI, kg/m2 | 24.7 ± 3.1 | 24.9 ± 3.2 | 0.296 | 0.042 | 24.9 ± 3.1 | 25.0 ± 3.0 | 0.696 | 0.022 |
| Follow-up duration, days | 990 (630–1113) | 990 (630–1114) | 0.317 | |||||
| Comorbidities | ||||||||
| Hypertension | 808 (74.3) | 1069 (71.8) | 0.164 | 0.025 | 376 (72.9) | 381 (73.8) | 0.778 | 0.025 |
| Dyslipidemia | 430 (39.6) | 604 (40.6) | 0.625 | 0.010 | 204 (39.5) | 217 (42.1) | 0.447 | 0.019 |
| Current smoking | 264 (24.3) | 383 (25.7) | 0.434 | 0.014 | 123 (23.8) | 123 (23.8) | 0.999 | 0.008 |
| Heart failure or LVEF < 40% | 90 (8.3) | 158 (10.6) | 0.050 | 0.023 | 54 (10.5) | 51 (9.9) | 0.837 | 0.004 |
| MI or revascularization | 236 (21.6) | 303 (20.3) | 0.405 | 0.014 | 107 (20.7) | 115 (22.3) | 0.596 | 0.008 |
| Chronic kidney disease | 82 (7.6) | 119 (8.0) | 0.710 | 0.004 | 38 (7.4) | 40 (7.8) | 0.906 | 0.004 |
| Peripheral vascular disease | 31 (2.9) | 43 (2.9) | 0.999 | <0.001 | 15 (2.9) | 14 (2.7) | 0.999 | 0.002 |
| Previous stroke | 108 (9.9) | 155 (10.4) | 0.742 | 0.005 | 57 (11.0) | 48 (9.3) | 0.410 | 0.006 |
| Initial presentation with acute MI | 294 (27.1) | 423 (28.5) | 0.449 | 0.014 | 138 (26.7) | 142 (27.5) | 0.834 | 0.029 |
| Lesion and Procedure Characteristics | ||||||||
| Multivessel disease | 396 (36.5) | 477 (32.0) | 0.021 | 0.044 | 176 (34.1) | 185 (35.9) | 0.602 | 0.008 |
| Left main disease | 88 (8.1) | 110 (7.4) | 0.502 | 0.007 | 35 (6.8) | 36 (7.0) | 0.999 | 0.002 |
| Type B2/C lesions | 913 (84.1) | 1217 (81.7) | 0.126 | 0.024 | 426 (82.6) | 429 (83.1) | 0.869 | 0.016 |
| Calcification | 87 (8.0) | 119 (8.0) | 0.999 | <0.001 | 38 (7.4) | 44 (8.5) | 0.565 | 0.017 |
| 2nd generation DES | 1010 (92.9) | 1359 (91.1) | 0.105 | 0.018 | 467 (90.5) | 475 (92.1) | 0.440 | 0.004 |
| Total stent number | 1.8 ± 1.1 | 1.7 ± 1.0 | 0.088 | 0.066 | 1.7 ± 1.0 | 1.8 ± 1.0 | 0.395 | 0.015 |
| Stent diameter, mm | 3.0 ± 0.4 | 3.0 ± 0.4 | 0.694 | 0.016 | 3.0 ± 0.4 | 3.0 ± 0.4 | 0.632 | 0.048 |
| Total stent length, mm | 44.8 ± 29.6 | 42.1 ± 27.8 | 0.022 | 0.089 | 42.8 ± 27.9 | 44.5 ± 30.2 | 0.326 | 0.017 |
| Medications | ||||||||
| Insulin | 198 (18.2) | 309 (20.8) | 0.120 | 0.025 | 104 (20.2) | 100 (19.4) | 0.815 | 0.006 |
| Sulfonylurea | 424 (39.0) | 706 (47.4) | <0.001 | 0.084 | 222 (43.0) | 236 (45.7) | 0.415 | 0.019 |
| Glinide | 13 (1.2) | 26 (2.4) | 0.036 | 0.012 | 10 (1.9) | 10 (1.9) | 0.999 | <0.001 |
| Metformin | 571 (52.6) | 797 (53.5) | 0.632 | <0.001 | 271 (52.5) | 272 (52.7) | 0.999 | <0.001 |
| DPP4i | 201 (18.5) | 259 (17.4) | 0.498 | 0.011 | 92 (17.8) | 107 (20.7) | 0.269 | 0.010 |
| Thiazolidinedione | 31 (2.9) | 42 (2.8) | 0.999 | <0.011 | 17 (3.3) | 18 (3.5) | 0.999 | 0.006 |
| a-glucosidase inhibitor | 73 (6.7) | 126 (8.5) | 0.118 | 0.017 | 41 (7.9) | 34 (6.6) | 0.472 | 0.017 |
| Aspirin | 1082 (99.5) | 1482 (99.5) | 0.999 | <0.001 | 512 (99.2) | 514 (99.6) | 0.682 | 0.006 |
| Clopidogrel | 1066 (98.1) | 1459 (98.0) | 0.955 | 0.001 | 503 (97.5) | 504 (97.7) | 0.999 | <0.001 |
| Beta-blockers | 660 (60.7) | 949 (63.7) | 0.128 | 0.030 | 324 (62.8) | 323 (62.6) | 0.999 | 0.004 |
| ACE inhibitors | 296 (27.2) | 464 (31.2) | 0.034 | 0.039 | 152 (29.5) | 147 (28.5) | 0.784 | 0.014 |
| ARBs | 415 (38.2) | 573 (38.5) | 0.908 | 0.003 | 183 (35.5) | 199 (38.6) | 0.334 | 0.006 |
| Statin | 948 (87.2) | 1289 (86.6) | 0.680 | 0.006 | 452 (87.6) | 447 (86.6) | 0.710 | 0.016 |
| Laboratory Results | ||||||||
| Baseline HbA1c, % | 6.5 ± 0.8 | 8.1 ± 1.5 | <0.001 | 2.074 | 7.0 ± 0.8 | 7.0 ± 1.0 | 0.397 | 0.061 |
| Numbers of HbA1c records | 5.7 ± 3.3 | 6.2 ± 3.5 | <0.001 | 0.161 | 6.2 ± 3.3 | 6.3 ± 3.4 | 0.624 | 0.024 |
| Total cholesterol, mg/dL | 158.5 ± 40.1 | 163.7 ± 43.4 | 0.002 | 0.128 | 163.1 ± 41.3 | 161.4 ± 40.5 | 0.505 | 0.028 |
| Triglyceride, mg/dL | 122.3 ± 95.5 | 127.1 ± 112.4 | 0.240 | 0.051 | 123.3 ± 98.2 | 122.9 ± 100.6 | 0.951 | 0.038 |
| HDL, mg/dL | 35.0 ± 18.2 | 34.8 ± 18.4 | 0.803 | 0.010 | 34.2 ± 19.0 | 35.2 ± 18.4 | 0.389 | 0.002 |
| LDL, mg/dL | 77.0 ± 47.8 | 78.8 ± 50.3 | 0.359 | 0.037 | 77.9 ± 51.3 | 77.5 ± 50.6 | 0.910 | 0.028 |
| Creatinine clearance, ml/min | 67.7 ± 28.7 | 66.9 ± 29.2 | 0.468 | 0.029 | 67.2 ± 28.2 | 67.1 ± 28.8 | 0.954 | 0.013 |
| Outcome | Overall Population | PS Matched Population | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean HbA1c < 7.0% (N = 1087) | Mean HbA1c ≥ 7.0% (N = 1489) | aHR (95% CI) | p Value | Mean HbA1c < 7.0% (N = 516) | Mean HbA1c ≥ 7.0% (N = 516) | aHR (95% CI) | p Value | |
| N (%) | N (%) | N (%) | N (%) | |||||
| MACE | 138 (12.7) | 197 (13.2) | 1.06 (0.82–1.37) | 0.672 | 73 (14.1) | 63 (12.2) | 1.17 (0.84–1.65) | 0.351 |
| All-cause death | 56 (5.2) | 79 (5.3) | 1.14 (0.75–1.72) | 0.553 | 33 (6.4) | 23 (4.5) | 1.44 (0.85–2.46) | 0.177 |
| Cardiac death | 34 (3.1) | 52 (3.5) | 1.06 (0.63–1.81) | 0.820 | 21 (4.1) | 12 (2.3) | 1.76 (0.87–3.36) | 0.119 |
| Non-fatal MI | 6 (0.6) | 22 (1.5) | 0.41 (0.15–1.16) | 0.093 | 3 (0.6) | 6 (1.2) | 0.50 (0.13–2.01) | 0.330 |
| Cardiac death + non-fatal MI | 40 (3.7) | 73 (4.9) | 0.90 (0.57–1.42) | 0.639 | 24 (4.7) | 18 (3.5) | 1.34 (0.72–2.46) | 0.354 |
| Stroke | 19 (1.7) | 16 (1.1) | 1.5 (0.68–3.59) | 0.295 | 8 (1.6) | 4 (0.8) | 2.00 (0.60–6.65) | 0.257 |
| Any revascularization | 104 (9.8) | 145 (9.7) | 1.05 (0.78–1.42) | 0.748 | 53 (10.3) | 52 (10.1) | 1.03 (0.71–1.52) | 0.866 |
| Target lesion revascularization | 49 (4.5) | 63 (4.2) | 1.12 (0.71–1.78) | 0.615 | 26 (5.0) | 23 (4.5) | 1.15 (0.65–2.01) | 0.634 |
| Outcome | Sustained HbA1c < 7.0% (N = 716) | Sustained HbA1c ≥ 7.0% (N = 532) | aHR (95% CI) | p Value | |
|---|---|---|---|---|---|
| N (%) | N (%) | ||||
| MACE | 62 (8.7) | 91 (17.1) |  | 1.15 (0.71–1.89) | 0.566 |
| All-cause Death | 22 (3.1) | 27 (5.1) | 2.70 (0.95–6.70) | 0.057 | |
| Cardiac Death | 13 (1.8) | 21 (3.9) | 1.26 (0.40–3.97) | 0.698 | |
| Non-fatal MI | 1 (0.1) | 12 (2.3) | 0.28 (0.03–3.09) | 0.301 | |
| Cardiac Death + Non-fatal MI | 14 (2.0) | 33 (6.2) | 0.90 (0.35–2.27) | 0.816 | |
| Stroke | 9 (1.6) | 10 (1.9) | 0.77 (0.17–3.45) | 0.730 | |
| Any revascularization | 51 (7.1) | 69 (13.0) | 1.34 (0.76–2.34) | 0.308 | |
| Target lesion revascularization | 28 (3.9) | 33 (6.2) | 1.85 (0.83–4.12) | 0.135 | |
| Outcome | Mean HbA1c ≤ 6.5% | Mean HbA1c ≥ 8.0% | aHR (95% CI) | p Value | |
|---|---|---|---|---|---|
| N (%) | N (%) | ||||
| MACE | 67 (12.2) | 79 (12.4) |  | 1.15 (0.71–1.86) | 0.583 |
| All-cause Death | 28 (5.1) | 29 (4.6) | 1.72 (0.75–3.90) | 0.198 | |
| Cardiac Death | 16 (2.9) | 18 (2.8) | 1.42 (0.47–4.24) | 0.531 | |
| Non-fatal MI | 2 (0.4) | 12 (1.9) | 0.19 (0.03–1.35) | 0.097 | |
| Cardiac Death + Non-fatal MI | 18 (3.3) | 30 (4.7) | 0.81 (0.34–1.93) | 0.638 | |
| Stroke | 7 (1.3) | 8 (1.3) | 0.62 (0.11–3.51) | 0.592 | |
| Any revascularization | 53 (9.7) | 60 (9.4) | 1.25 (0.72–2.18) | 0.428 | |
| Target lesion revascularization | 28 (5.1) | 27 (4.3) | 1.84 (0.80–4.27) | 0.154 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.; Han, J.-K.; Chang, M.; Ki, Y.-J.; Kang, J.; Yang, H.-M.; Cho, H.-J.; Park, K.W.; Kang, H.-J.; Koo, B.-K.; et al. Impact of Intensive Glucose Control in Patients with Diabetes Mellitus Undergoing Percutaneous Coronary Intervention: 3-Year Clinical Outcomes. J. Clin. Med. 2020, 9, 2464. https://doi.org/10.3390/jcm9082464
Park J, Han J-K, Chang M, Ki Y-J, Kang J, Yang H-M, Cho H-J, Park KW, Kang H-J, Koo B-K, et al. Impact of Intensive Glucose Control in Patients with Diabetes Mellitus Undergoing Percutaneous Coronary Intervention: 3-Year Clinical Outcomes. Journal of Clinical Medicine. 2020; 9(8):2464. https://doi.org/10.3390/jcm9082464
Chicago/Turabian StylePark, Jiesuck, Jung-Kyu Han, Mineok Chang, You-Jeong Ki, Jeehoon Kang, Han-Mo Yang, Hyun-Jai Cho, Kyung Woo Park, Hyun-Jae Kang, Bon-Kwon Koo, and et al. 2020. "Impact of Intensive Glucose Control in Patients with Diabetes Mellitus Undergoing Percutaneous Coronary Intervention: 3-Year Clinical Outcomes" Journal of Clinical Medicine 9, no. 8: 2464. https://doi.org/10.3390/jcm9082464