Persistence with Anticoagulation for Atrial Fibrillation: Report from the GLORIA-AF Phase III 1-Year Follow-up

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Therapy Persistence
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
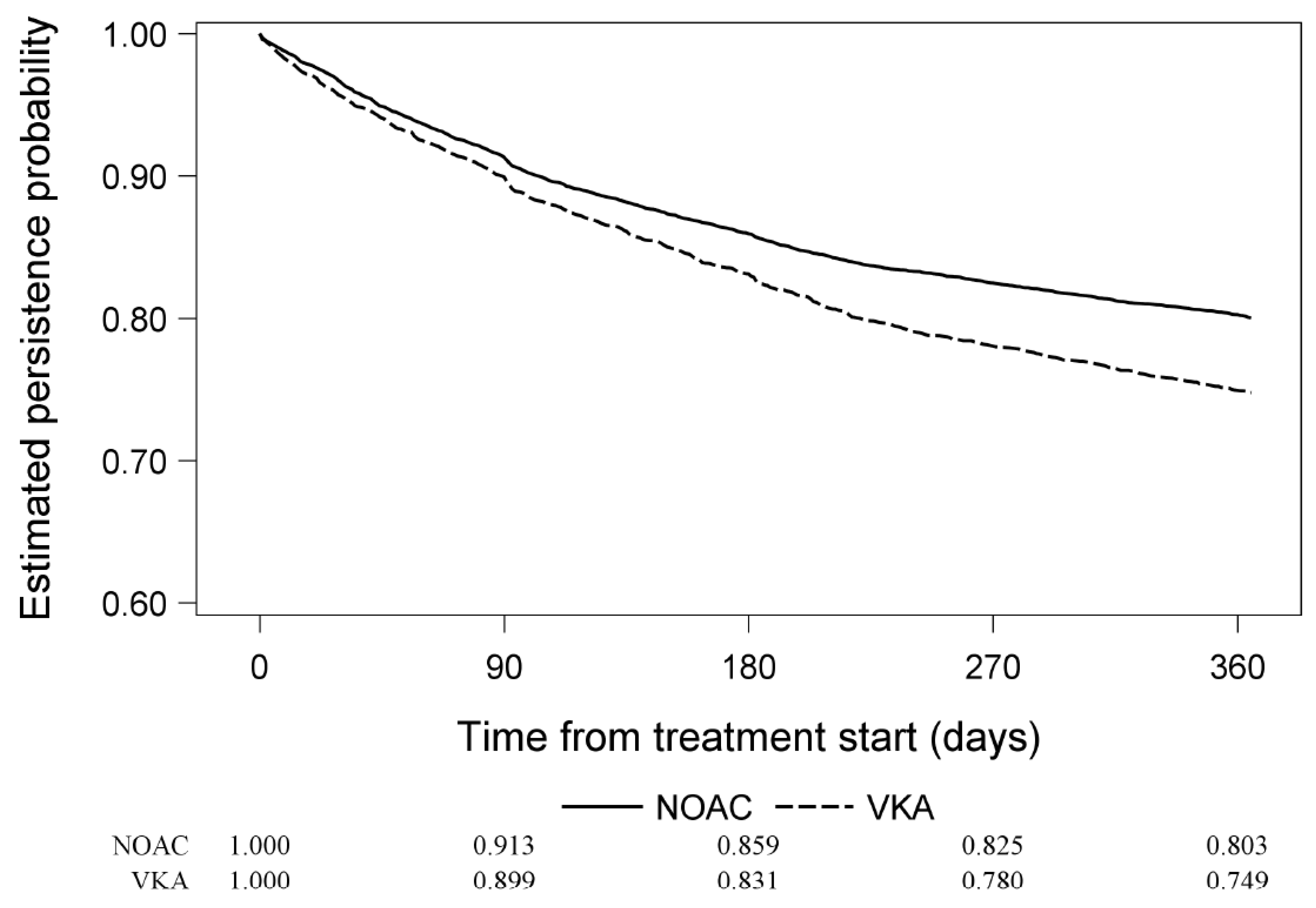
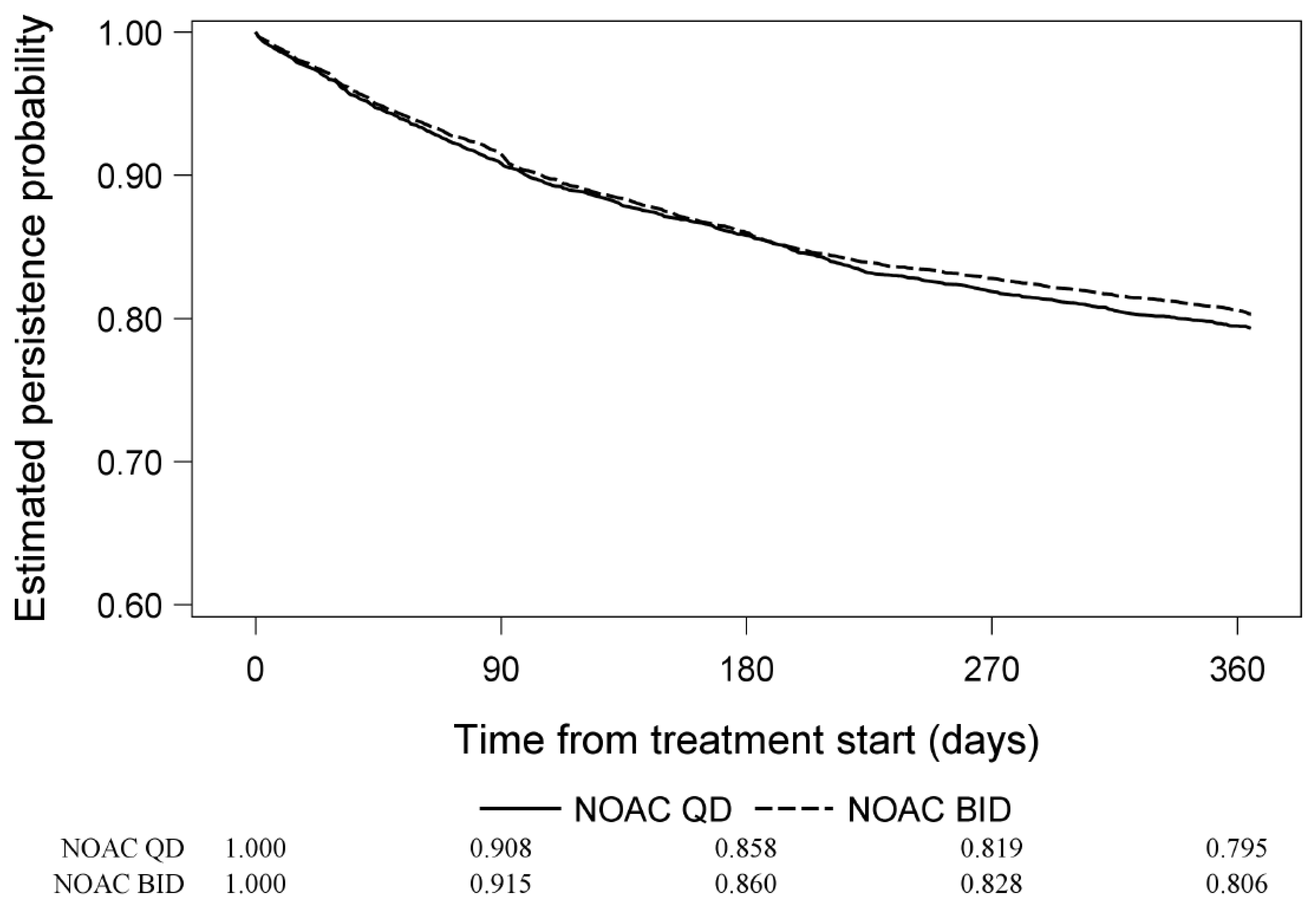
3.2. Overall Treatment Persistence (on Trimmed Patient Sets in Terms of Propensity Score)
3.3. Predictors of Treatment Persistence
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lip, G.; Freedman, B.; De Caterina, R.; Potpara, T.S. Stroke prevention in atrial fibrillationast, present and future. Comparing the guidelines and practical decision-making. Thromb. Haemost. 2017, 117, 1230–1239. [Google Scholar]
- Lip, G.Y.H.; Banerjee, A.; Boriani, G.; en Chiang, C.; Fargo, R.; Freedman, B.; Lane, D.A.; Ruff, C.T.; Turakhia, M.; Werring, D.; et al. Antithrombotic Therapy for Atrial Fibrillation: CHEST Guideline and Expert Panel Report. CHEST 2018, 154, 1121–1201. [Google Scholar] [CrossRef] [Green Version]
- Paquette, M.; França, L.R.; Teutsch, C.; Diener, H.-C.; Lu, S.; Dubner, S.J.; Rothman, J.K.; Zint, K.; Halperin, J.L.; Huisman, M.V.; et al. Persistence With Dabigatran Therapy at 2 Years in Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2017, 70, 1573–1583. [Google Scholar] [CrossRef]
- Vrijens, B.; Heidbuchel, H. Non-vitamin K antagonist oral anticoagulants: Considerations on once- vs. twice-daily regimens and their potential impact on medication adherence. Europace 2015, 17, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [Green Version]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef]
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Špinar, J.; Koretsune, Y.; et al. Edoxaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [Green Version]
- Huisman, M.V.; Lip, G.Y.; Diener, H.C.; Dubner, S.J.; Halperin, J.L.; Ma, C.S.; Rothman, K.J.; Teutsch, C.; Zint, K.; Ackermann, D.; et al. Design and rationale of Global Registry on Long-Term Oral Antithrombotic Treatment in Patients with Atrial Fibrillation: A global registry program on long-term oral antithrombotic treatment in patients with atrial fibrillation. Am. Heart J. 2014, 167, 329–334. [Google Scholar] [CrossRef]
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. CHEST 2010, 137, 263–272. [Google Scholar] [CrossRef]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.; Lip, G.Y. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The Euro Heart Survey. CHEST 2010, 138, 1093–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, P.C. Using the Standardized Difference to Compare the Prevalence of a Binary Variable Between Two Groups in Observational Research. Commun. Stat. Simul. Comput. 2009, 38, 1228–1234. [Google Scholar] [CrossRef]
- Rothman, K.J. Disengaging from statistical significance. Eur. J. Epidemiol. 2016, 31, 443–444. [Google Scholar] [CrossRef] [PubMed]
- Stürmer, T.; Rothman, K.J.; Avorn, J.; Glynn, R.J. Treatment effects in the presence of unmeasured confounding: Dealing with observations in the tails of the propensity score distribution—A simulation study. Am. J. Epidemiol. 2010, 172, 843–854. [Google Scholar] [CrossRef] [Green Version]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef]
- Monahan, T.; Fisher, J.A. Benefits of “Observer Effects”: Lessons from the Field. Qual. Res. 2010, 10, 357–376. [Google Scholar] [CrossRef] [Green Version]
- Martinez, C.; Katholing, A.; Wallenhorst, C.; Freedman, S.B. Therapy persistence in newly diagnosed non-valvular atrial fibrillation treated with warfarin or NOAC. A cohort study. Thromb. Haemost. 2016, 115, 31–39. [Google Scholar]
- Zalesak, M.; Siu, K.; Francis, K.; Yu, C.; Alvrtsyan, H.; Rao, Y.; Walker, D.; Sander, S.; Miyasato, G.; Matchar, D.; et al. Higher persistence in newly diagnosed nonvalvular atrial fibrillation patients treated with dabigatran versus warfarin. Circ. Cardiovasc. Qual. Outcomes 2013, 6, 567–574. [Google Scholar] [CrossRef] [Green Version]
- Laliberte, F.; Cloutier, M.; Nelson, W.W.; Coleman, C.I.; Pilon, D.; Olson, W.H.; Damaraju, C.V.; Schein, J.R.; Lefebvre, P. Real-world comparative effectiveness and safety of rivaroxaban and warfarin in nonvalvular atrial fibrillation patients. Curr. Med. Res. Opin. 2014, 30, 1317–1325. [Google Scholar] [CrossRef]
- Nelson, W.W.; Song, X.; Coleman, C.I.; Thomson, E.; Smith, D.M.; Damaraju, C.V.; Schein, J.R. Medication persistence and discontinuation of rivaroxaban versus warfarin among patients with non-valvular atrial fibrillation. Curr. Med. Res. Opin. 2014, 30, 2461–2469. [Google Scholar] [CrossRef]
- Liu, C.; Du, X.; Jiang, C.; He, L.; Chang, S.S.; Guo, X.-Y.; Yu, R.-H.; Bai, R.; Liu, N.; Sang, C.-H.; et al. Long-Term Persistence with Newly-Initiated Warfarin or Non-VKA Oral Anticoagulant (NOAC) in Patients with Non-Valvular Atrial Fibrillation: Insights from the Prospective China-AF Registry. Med. Sci. Monit. 2019, 25, 2649–2657. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Shortt, B.; Robinson, M.; Eikelboom, J.W. Adherence to anticoagulant treatment with dabigatran in a real-world setting. J. Thromb. Haemost. 2013, 11, 1295–1299. [Google Scholar] [CrossRef] [PubMed]
- Coleman, C.I.; Tangirala, M.; Evers, T. Medication adherence to rivaroxaban and dabigatran for stroke prevention in patients with non-valvular atrial fibrillation in the United States. Int. J. Cardiol. 2016, 212, 171–173. [Google Scholar] [CrossRef]
- Shiga, T.; Naganuma, M.; Nagao, T.; Maruyama, K.; Suzuki, A.; Murasaki, K.; Hagiwara, N. Persistence of non-vitamin K antagonist oral anticoagulant use in Japanese patients with atrial fibrillation: A single-center observational study. J. Arrhythm. 2015, 31, 339–344. [Google Scholar] [CrossRef] [Green Version]
- Jackevicius, C.A.; Tsadok, M.A.; Essebag, V.; Atzema, C.; Eisenberg, M.J.; Tu, J.V.; Lu, L.; Rahme, E.; Ho, P.M.; Turakhia, M.; et al. Early non-persistence with dabigatran and rivaroxaban in patients with atrial fibrillation. Heart 2017, 103, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Lamberts, M.; Staerk, L.; Olesen, J.B.; Fosbøl, E.L.; Hansen, M.L.; Harboe, L.; Lefevre, C.; Evans, D.; Gislason, G.H. Major Bleeding Complications and Persistence with Oral Anticoagulation in Non-Valvular Atrial Fibrillation: Contemporary Findings in Real-Life Danish Patients. J. Am. Heart Assoc. 2017, 6, e004517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forslund, T.; Wettermark, B.; Hjemdahl, P. Comparison of treatment persistence with different oral anticoagulants in patients with atrial fibrillation. Eur. J. Clin. Pharmacol. 2016, 72, 329–338. [Google Scholar] [CrossRef]
- Cataldo, N.; Pegoraro, V.; Ripellino, C.; Bertasi, V.; Di Turi, R.; Pastorello, M.; Gambera, M. Non-persistence risk and health care resource utilization of Italian patients with non-valvular atrial fibrillation. Recenti. Prog. Med. 2018, 109, 113–121. [Google Scholar]
- McHorney, C.A.; Crivera, C.; Laliberté, F.; Nelson, W.W.; Germain, G.; Bookhart, B.; Martin, S.; Schein, J.; Lefebvre, P.; Deitelzweig, S. Adherence to non-vitamin-K-antagonist oral anticoagulant medications based on the Pharmacy Quality Alliance measure. Curr. Med. Res. Opin. 2015, 31, 2167–2173. [Google Scholar] [CrossRef]
- Crivera, C.; Nelson, W.W.; Bookhart, B.; Martin, S.; Germain, G.; Laliberté, F.; Schein, J.; Lefebvre, P. Pharmacy quality alliance measure: Adherence to non-warfarin oral anticoagulant medications. Curr. Med. Res. Opin. 2015, 31, 1889–1895. [Google Scholar] [CrossRef]
- McHorney, C.A.; Peterson, E.D.; Laliberté, F.; Germain, G.; Nelson, W.W.; Crivera, C.; Schein, J.; Lefebvre, P. Comparison of Adherence to Rivaroxaban Versus Apixaban Among Patients With Atrial Fibrillation. Clin. Ther. 2016, 38, 2477–2488. [Google Scholar] [CrossRef]
- Sørensen, R.; Nielsen, B.J.; Pallisgaard, J.L.; Lee, C.J.-Y.; Torp-Pedersen, C. Adherence with oral anticoagulation in non-valvular atrial fibrillation: A comparison of vitamin K antagonists and non-vitamin K antagonists. Eur. Heart J. Cardiovasc. Pharmacother. 2017, 3, 151–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, J.; Han, S.; Bae, H.-J.; Jun, S.-W.; Choi, S.-W.; Lee, C.-H.; Kim, I.-C.; Cho, Y.-K.; Park, H.-S.; Kim, H.; et al. NOAC Adherence of Patients with Atrial Fibrillation in the Real World: Dosing Frequency Matters? Thromb. Haemost. 2020, 120, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Hohnloser, S.H.; Basic, E.; Nabauer, M. Changes in Oral Anticoagulation Therapy over One Year in 51,000 Atrial Fibrillation Patients at Risk for Stroke: A Practice-Derived Study. Thromb. Haemost. 2019, 119, 882–893. [Google Scholar] [PubMed]
- Saini, S.D.; Schoenfeld, P.; Kaulback, K.; Dubinsky, M.C. Effect of medication dosing frequency on adherence in chronic diseases. Am. J. Manag. Care 2009, 15, e22–e33. [Google Scholar] [PubMed]
- Laliberte, F.; Nelson, W.W.; Lefebvre, P.; Schein, J.R.; Rondeau-Leclaire, J.; Duh, M.S. Impact of daily dosing frequency on adherence to chronic medications among nonvalvular atrial fibrillation patients. Adv. Ther. 2012, 29, 675–690. [Google Scholar] [CrossRef]
- Beyer-Westendorf, J.; Förster, K.; Ebertz, F.; Gelbricht, V.; Schreier, T.; Göbelt, M.; Michalski, F.; Endig, H.; Sahin, K.; Tittl, L.; et al. Drug persistence with rivaroxaban therapy in atrial fibrillation patients-results from the Dresden non-interventional oral anticoagulation registry. Europace 2015, 17, 530–538. [Google Scholar] [CrossRef] [Green Version]
- Pritchett, R.V.; Bem, D.; Turner, G.M.; Thomas, G.N.; Clarke, J.L.; Fellows, R.; Lane, D.A.; Jolly, K. Improving the Prescription of Oral Anticoagulants in Atrial Fibrillation: A Systematic Review. Thromb. Haemost. 2019, 119, 294–307. [Google Scholar] [CrossRef] [Green Version]
- Hylek, E.M. Biomarkers for Prediction of Stroke and Bleeds in Atrial Fibrillation. Circulation 2019, 139, 772–774. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| VKAs | NOACs | NOACs QD | NOACs BID | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| <3 mo | 3–6 mo | 6–12 mo | <3 mo | 3–6 mo | 6–12 mo | <3 mo | 3–6 mo | 6–12 mo | <3 mo | 3–6 mo | 6–12 mo | |
| Cumulative * number at risk, n | 4478 (100.0) | 3950 (88.2) | 3602 (80.4) | 11,945 (100.0) | 10,748 (89.9) | 9987 (83.6) | 4097 (100.0) | 3670 (89.6) | 3422 (83.5) | 7855 (100.0) | 7076 (90.1) | 6567 (83.6) |
| Cumulative * discontinued, n (%) | 442 (9.9) | 742 (16.6) | 1090 (24.3) | 1012 (8.5) | 1649 (13.8) | 2303 (19.3) | 367 (9.0) | 573 (14.0) | 822 (20.1) | 651 (8.3) | 1079 (13.7) | 1488 (18.9) |
| Cumulative * censored, n (%) | 86 (1.9) | 134 (3.0) | 278 (6.2) | 185 (1.6) | 309 (2.6) | 749 (6.3) | 60 (1.5) | 102 (2.5) | 267 (6.5) | 128 (1.6) | 209 (2.7) | 489 (6.2) |
| Variable | Hazard Ratio | 95% Confidence Interval |
|---|---|---|
| NOACs vs. VKAs | 0.75 | 0.69–0.80 |
| Age (65–75 years vs. <65 years) | 0.85 | 0.78–0.93 |
| Age (≥75 years vs. <65 years) | 0.81 | 0.72–0.90 |
| Gender (female vs. male) | 0.92 | 0.86–1.00 |
| Hypertension (yes vs. no) | 0.91 | 0.84–0.99 |
| Type of atrial fibrillation (permanent vs. paroxysmal) | 0.83 | 0.73–0.95 |
| Medication usage predisposing to bleeding (yes vs. no) | 1.19 | 1.09–1.30 |
| Alcohol use (<1 drink/week vs. never) | 0.90 | 0.83–0.99 |
| Smoking status (current smoker vs. non-smoker) | 1.18 | 1.04–1.33 |
| Proton pump inhibitors (yes vs. no) | 1.10 | 1.01–1.20 |
| Categorization of atrial fibrillation (minimally symptomatic vs. symptomatic) | 0.82 | 0.76–0.89 |
| Categorization of atrial fibrillation (asymptomatic vs. symptomatic) | 0.73 | 0.67–0.80 |
| Region (Asia vs. Europe) | 1.97 | 1.79–2.18 |
| Region (North America vs. Europe) | 1.53 | 1.40–1.68 |
| Medical treatment reimbursement (private insurance vs. federal insurance) | 1.11 | 1.01–1.23 |
| Body mass index (<18.5 kg/m2 vs. ≥18.5 kg/m2) | 0.94 | 0.88–1.00 |
| Number of concomitant medications (≥median vs. <median) | 0.92 | 0.85–1.00 |
| Variable | Hazard Ratio | 95% Confidence Interval |
|---|---|---|
| NOACs twice daily vs. once daily | 0.95 | 0.88–1.04 |
| Age (65–75 vs. <65) | 0.80 | 0.72–0.90 |
| Age (≥75 vs. <65) | 0.80 | 0.70–0.91 |
| Gender (female vs. male) | 0.89 | 0.81–0.98 |
| Hypertension (yes vs. no) | 0.88 | 0.80–0.97 |
| Medication usage predisposing to bleeding (yes vs. no) | 1.20 | 1.08–1.34 |
| Smoking status (current smoker vs. non-smoker) | 1.22 | 1.06–1.41 |
| Categorization of AF (minimally symptomatic vs. symptomatic) | 0.78 | 0.71–0.86 |
| Categorization of AF (asymptomatic vs. symptomatic) | 0.66 | 0.60–0.74 |
| Region (Asia vs. Europe) | 2.33 | 2.06–2.63 |
| Region (North America vs. Europe) | 1.71 | 1.53–1.91 |
| Medical treatment reimbursement (self-pay/no coverage vs. federal insurance) | 0.67 | 0.54–0.84 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kozieł, M.; Mazurek, M.; Teutsch, C.; Diener, H.-C.; Dubner, S.J.; Halperin, J.L.; Ma, C.-S.; Rothman, K.J.; Brandes, A.; Paquette, M.; et al. Persistence with Anticoagulation for Atrial Fibrillation: Report from the GLORIA-AF Phase III 1-Year Follow-up. J. Clin. Med. 2020, 9, 1969. https://doi.org/10.3390/jcm9061969
Kozieł M, Mazurek M, Teutsch C, Diener H-C, Dubner SJ, Halperin JL, Ma C-S, Rothman KJ, Brandes A, Paquette M, et al. Persistence with Anticoagulation for Atrial Fibrillation: Report from the GLORIA-AF Phase III 1-Year Follow-up. Journal of Clinical Medicine. 2020; 9(6):1969. https://doi.org/10.3390/jcm9061969
Chicago/Turabian StyleKozieł, Monika, Michał Mazurek, Christine Teutsch, Hans-Christoph Diener, Sergio J. Dubner, Jonathan L. Halperin, Chang-Sheng Ma, Kenneth J. Rothman, Axel Brandes, Miney Paquette, and et al. 2020. "Persistence with Anticoagulation for Atrial Fibrillation: Report from the GLORIA-AF Phase III 1-Year Follow-up" Journal of Clinical Medicine 9, no. 6: 1969. https://doi.org/10.3390/jcm9061969