Characterization of Intervertebral Disc Changes in Asymptomatic Individuals with Distinct Physical Activity Histories Using Three Different Quantitative MRI Techniques

 , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Ethical Approval and Subjects
2.2. Testing and MR Scanning Protocol
- Sagittal T2-mapping using spin-echo multi-echo sequences (8 echo times: 15.75, 36.75, 57.75, 78.75, 99.75, 120.75, 141.75 and 162.75 ms; repetition time: 2000 ms; number of slices: 12; slice thickness: 3 mm; interslice distance: 1.5 mm; field-of-view: 281 × 281 mm; resolution: 0.366 mm per pixel; acquisition time: 9 min 30 s).
- Sagittal T2w imaging (echo time: 70 ms; repetition time: 2600 ms; number of slices: 15; slice thickness: 3 mm; interslice distance: 1.5 mm; field-of-view: 357 × 357 mm; resolution: 0.532 mm per pixel; acquisition time: 3 min).
- Sagittal Dixon imaging (echo times: 2.45/3.67 ms; repetition time: 5.27 ms; number of slices: 20; slice thickness: 3 mm; interslice distance: 0 mm; bandwidth: 500; field-of-view: 400 × 400 mm; resolution: 0.833 mm per pixel; acquisition time: 1 min 20 s). A Dixon technique with asymmetrical echoes (mDIXON) was utilized [16].
2.3. Image Analysis
- T2-mapping: To reconstruct T2-maps, the T2-time in each pixel was calculated from the spin-echo multi-echo images using a linear fit to the natural logarithm of the image intensity in each of the eight MR echoes.
- T2w imaging: For normalization, the ratio of the average T2w signal intensity (T2w-SI) in the nucleus to the average T2w-SI in the anterior and posterior subregions (annulus) was calculated.
- Dixon imaging: An iterative algorithm with least-squares estimation was used to maximize the noise performance of the water signal [16].
2.4. Statistical Analyses
3. Results
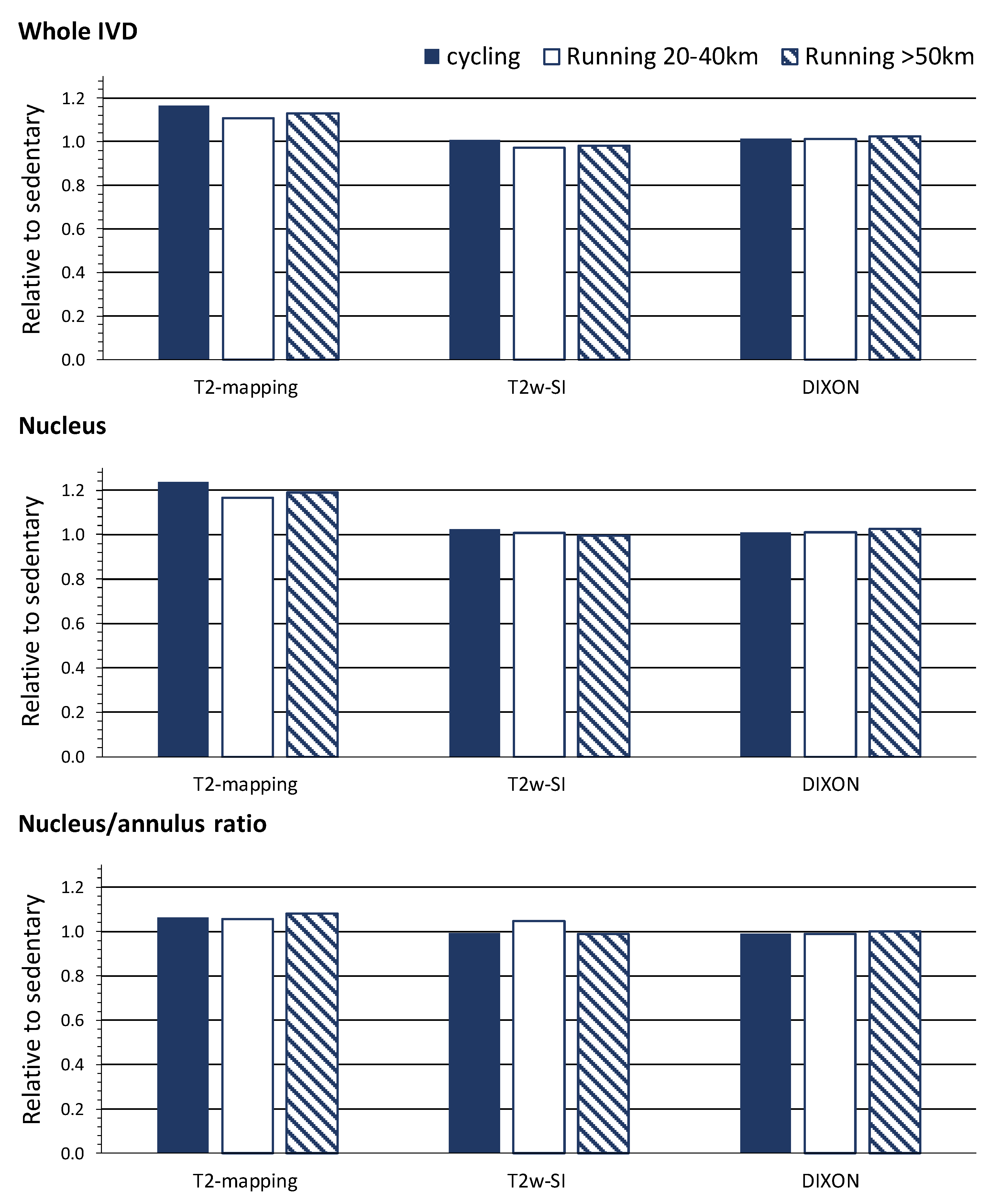
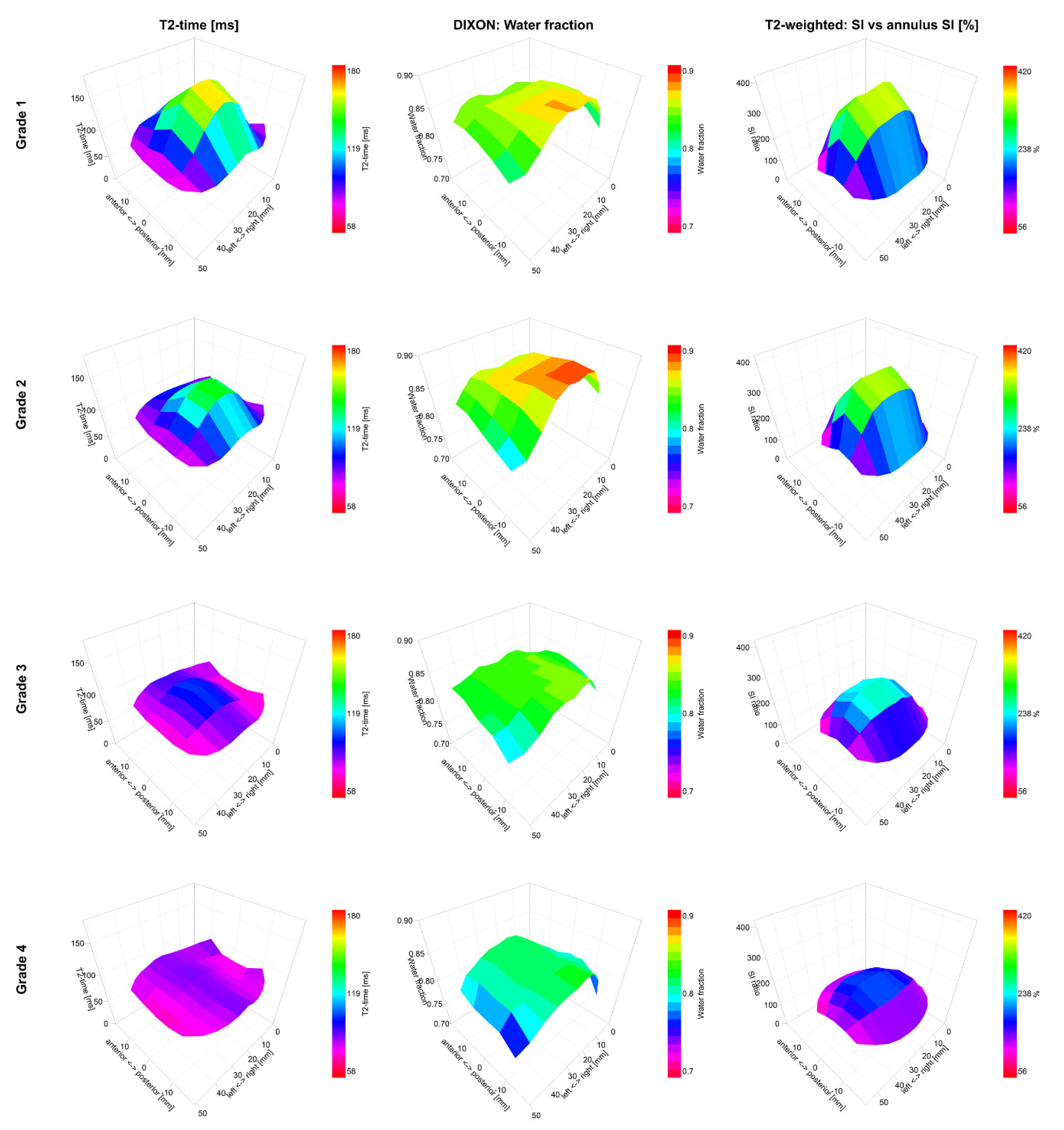
3.1. The T2-Mapping and T2w Imaging Techniques
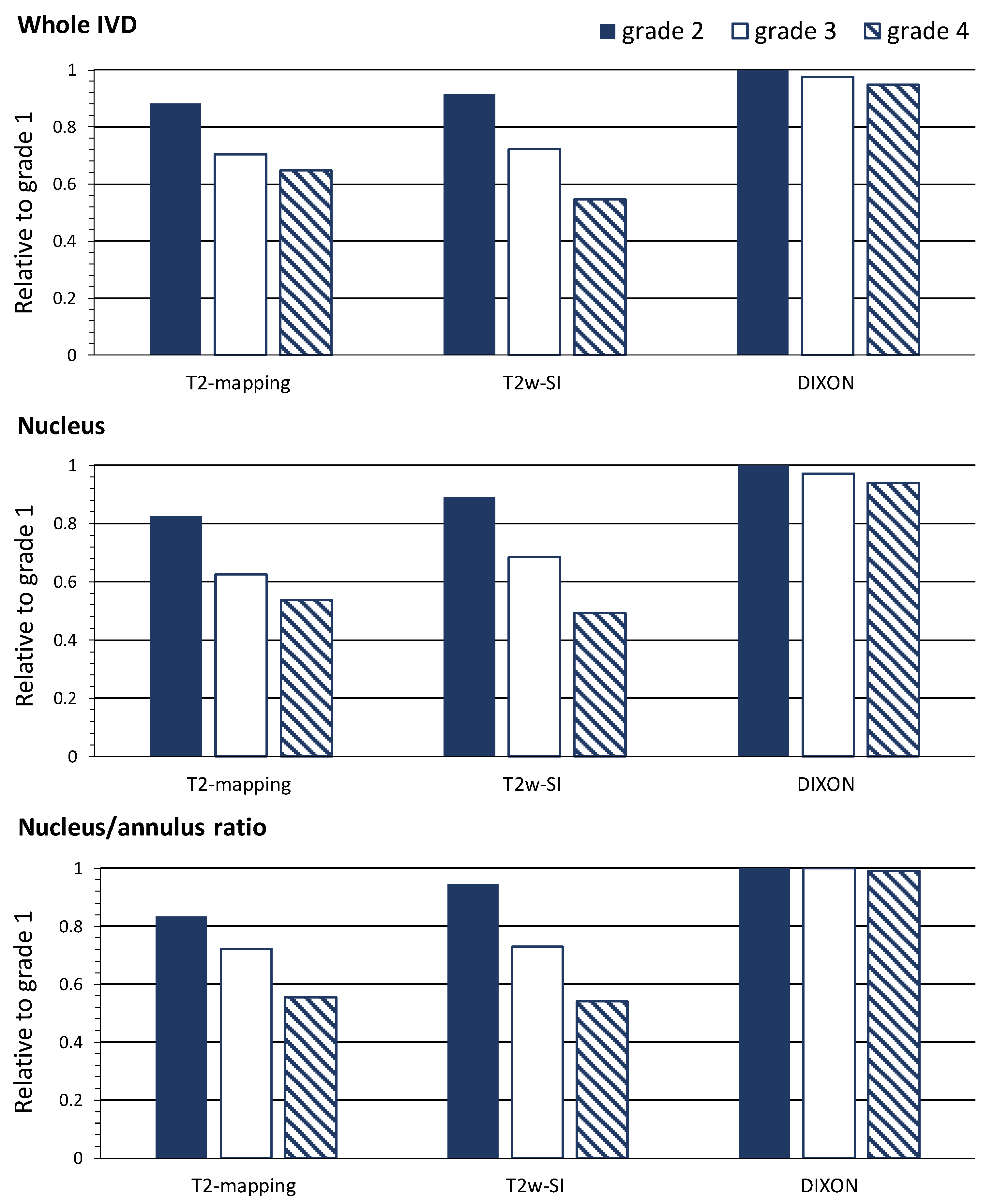
3.2. The Dixon Imaging Technique
3.3. Correlation Analyses
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Raj, P.P. Intervertebral disc: Anatomy-physiology-pathophysiology-treatment. Pain Pract. 2008, 8, 18–44. [Google Scholar] [CrossRef] [PubMed]
- Dowdell, J.; Erwin, M.; Choma, T.; Vaccaro, A.; Iatridis, J.; Cho, S.K. Intervertebral disk degeneration and repair. Neurosurgery 2017, 80, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Boos, N.; Weissbach, S.; Rohrbach, H.; Weiler, C.; Spratt, K.F.; Nerlich, A.G. Classification of age-related changes in lumbar intervertebral discs: 2002 Volvo award in basic science. Spine 2002, 27, 2631–2644. [Google Scholar] [CrossRef] [PubMed]
- Pfirrmann, C.W.; Metzdorf, A.; Zanetti, M.; Hodler, J.; Boos, N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine 2001, 26, 1873–1878. [Google Scholar] [CrossRef]
- Samartzis, D.; Borthakur, A.; Belfer, I. Novel diagnostic and prognostic methods for disc degeneration and low back pain. Spine 2015, 15, 1919–1932. [Google Scholar] [CrossRef] [Green Version]
- Waldenberg, C.; Hebelka, H.; Brisby, H.; Lagerstrand, K.M. MRI histogram analysis enables objective and continuous classification of intervertebral disc degeneration. Eur. Spine J. 2018, 27, 1042–1048. [Google Scholar] [CrossRef]
- Belavy, D.L.; Quittner, M.J.; Ridgers, N.; Ling, Y.; Connell, D.; Rantalainen, T. Running exercise strengthens the intervertebral disc. Sci. Rep. 2017, 7, 45975. [Google Scholar] [CrossRef] [Green Version]
- Belavy, D.L.; Quittner, M.; Ridgers, N.D. Beneficial intervertebral disc and muscle adaptations in high-volume road cyclists. Med. Sci. Sports Exerc. 2019, 51, 211–217. [Google Scholar] [CrossRef]
- Belavy, D.L.; Albracht, K.; Bruggemann, G.P.; Vergroesen, P.P.; van Dieen, J.H. Can exercise positively influence the intervertebral disc? Sports Med. 2016, 46, 473–485. [Google Scholar] [CrossRef]
- Owen, P.J.; Miller, C.T.; Rantalainen, T. Exercise for the intervertebral disc: A 6-month randomised controlled trial in chronic low back pain. Eur. Spine J. 2020, 24, 1–13. [Google Scholar] [CrossRef]
- Videman, T.; Gibbons, L.E.; Kaprio, J.; Battie, M.C. Challenging the cumulative injury model: Positive effects of greater body mass on disc degeneration. Spine J. 2010, 10, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Luoma, K.; Vehmas, T.; Riihimaki, H.; Raininko, R. Disc height and signal intensity of the nucleus pulposus on magnetic resonance imaging as indicators of lumbar disc degeneration. Spine 2001, 26, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Tertti, M.; Paajanen, H.; Laato, M.; Aho, H.; Komu, M.; Kormano, M. Disc degeneration in magnetic resonance imaging. A comparative biochemical, histologic, and radiologic study in cadaver spines. Spine 1991, 16, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Mwale, F.; Iatridis, J.C.; Antoniou, J. Quantitative MRI as a diagnostic tool of intervertebral disc matrix composition and integrity. Eur. Spine J. 2008, 17, 432–440. [Google Scholar] [CrossRef] [Green Version]
- Dixon, W.T. Simple proton spectroscopic imaging. Radiology 1984, 153, 189–194. [Google Scholar] [CrossRef]
- Takasu, M.; Kaichi, Y.; Tani, C. Iterative decomposition of water and fat with echo asymmetry and least-squares estimation (IDEAL) magnetic resonance imaging as a biomarker for symptomatic multiple myeloma. PLoS ONE 2015, 10, e0116842. [Google Scholar] [CrossRef] [Green Version]
- Tyrrell, A.R.; Reilly, T.; Troup, J.D. Circadian variation in stature and the effects of spinal loading. Spine 1985, 10, 161–164. [Google Scholar] [CrossRef]
- Marinelli, N.L.; Haughton, V.M.; Munoz, A.; Anderson, P.A. T2 relaxation times of intervertebral disc tissue correlated with water content and proteoglycan content. Spine 2009, 34, 520–524. [Google Scholar] [CrossRef]
- Antoniou, J.; Pike, G.B.; Steffen, T. Quantitative magnetic resonance imaging in the assessment of degenerative disc disease. Magn. Reson. Med. 1998, 40, 900–907. [Google Scholar] [CrossRef]
- Mok, G.S.P.; Zhang, D.; Chen, S.Z.; Yuan, J.; Griffith, J.F.; Wang, Y.X.J. Comparison of three approaches for defining nucleus pulposus and annulus fibrosus on sagittal magnetic resonance images of the lumbar spine. J. Orthop. Translat. 2016, 6, 34–41. [Google Scholar] [CrossRef] [Green Version]
- Urrutia, J.; Besa, P.; Campos, M. The Pfirrmann classification of lumbar intervertebral disc degeneration: An independent inter- and intra-observer agreement assessment. Eur. Spine J. 2016, 25, 2728–2733. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Group (Number of IVDs) | ||||
|---|---|---|---|---|
| Sedentary (n = 144) | High-Volume Cycling (n = 132) | Running: 20–40 km (n = 180) | Running: >50 km (n = 150) | |
| Whole IVD | ||||
| T2-mapping (ms) | 104.4 (1.7) | 121.6 (1.7) ‡ | 115.6 (1.5) ‡ | 117.9 (1.6) ‡ |
| T2w-SI (no unit) | 326.9 (4.9) | 329.7 (5.1) | 317.6 (4.4) | 320.5 (4.8) |
| Dixon (%) | 86.0 (0.6) | 87.1 (0.7) | 87.1 (0.6) | 88.1 (0.6) * |
| Nucleus | ||||
| T2-mapping (ms) | 111.4 (3.0) | 137.7 (3.1) ‡ | 129.8 (2.7) ‡ | 132.6 (2.9) ‡ |
| T2w-SI (no unit) | 423.6 (8.9) | 434.0 (9.3) | 426.4 (7.9) | 421.6 (8.7) |
| Dixon (%) | 87.2 (0.6) | 88.1 (0.7) | 88.1 (0.6) | 89.4 (0.6) * |
| Nucleus/Annulus Ratio | ||||
| T2-mapping (ms) | 1.40 (0.03) | 1.49 (0.03) * | 1.48 (0.02) * | 1.51 (0.03) † |
| T2w-SI (no unit) | 3.31 (0.07) | 3.29 (0.07) | 3.46 (0.06) | 3.27 (0.07) |
| Dixon (%) | 1.01 (0.00) | 1.00 (0.00) | 1.01 (0.00) | 1.01 (0.00) |
| Pfirrmann Grade (Number of IVDs) | ||||
|---|---|---|---|---|
| 1 (n = 47) | 2 (n = 457) | 3 (n = 60) | 4 (n = 42) | |
| Whole IVD | ||||
| T2-mapping (ms) | 133.9 (17.3) | 118.1 (56.8) ‡ | 94.4 (26.2) ‡ | 86.8 (23.9) ‡ |
| T2w-SI (no unit) | 368 (42) | 337 (138) ‡ | 266 (63) ‡ | 201 (58) ‡ |
| Dixon (%) | 87.0 (7.3) | 87.8 (24.0) | 84.8 (11.1) | 82.4 (10.1) † |
| Nucleus | ||||
| T2-mapping (ms) | 166.0 (25.0) | 137.1 (81.8) ‡ | 103.9 (37.7) ‡ | 89.0 (34.4) ‡ |
| T2w-SI (no unit) | 551 (72) | 492 (236) ‡ | 377 (109) ‡ | 271 (99) ‡ |
| Dixon (%) | 87.2 (7.9) | 88.1 (25.9) | 84.8 (11.9) | 81.9 (10.9) † |
| Nucleus/Annulus Ratio | ||||
| T2-mapping (ms) | 1.8 (0.3) | 1.5 (0.9) ‡ | 1.3 (0.4) ‡ | 1.0 (0.4) ‡ |
| T2w-SI (no unit) | 3.7 (0.7) | 3.5 (2.3) | 2.7 (1.1) ‡ | 2.0 (1.0) ‡ |
| Dixon (%) | 1.00 (0.03) | 1.01 (0.10) | 1.00 (0.05) | 0.99 (0.04) |
| Whole IVD | Nucleus | Nucleus/Annulus Ratio | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T2-mapping | Dixon | T2w-SI | T2-mapping | Dixon | T2w-SI | T2-mapping | Dixon | T2w-SI | ||
| Whole IVD | T2-mapping | 0.10 * | 0.5 ‡ | 0.93 ‡ | 0.10 * | 0.46 ‡ | 0.43 ‡ | 0.05 | 0.24 ‡ | |
| Dixon | 0.2 ‡ | 0.13 † | 0.99 ‡ | 0.25 ‡ | 0.16 ‡ | 0.38 ‡ | 0.16 ‡ | |||
| T2w-SI | 0.56 ‡ | 0.29 ‡ | 0.92 ‡ | 0.56 ‡ | 0.16 ‡ | 0.49 ‡ | ||||
| Central IVD | T2-mapping | 0.13 † | 0.61 ‡ | 0.69 ‡ | 0.03 | 0.41 ‡ | ||||
| Dixon | 0.26 ‡ | 0.16 ‡ | 0.51 ‡ | 0.16 ‡ | ||||||
| T2w-SI | 0.73 ‡ | 0.13 † | 0.74 ‡ | |||||||
| Nucleus/Annulus Ratio | T2-mapping | 0.03 | 0.66 ‡ | |||||||
| Dixon | 0.05 | |||||||||
| T2w-SI | ||||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belavy, D.L.; Brisby, H.; Douglas, B.; Hebelka, H.; Quittner, M.J.; Owen, P.J.; Rantalainen, T.; Trudel, G.; Lagerstrand, K.M. Characterization of Intervertebral Disc Changes in Asymptomatic Individuals with Distinct Physical Activity Histories Using Three Different Quantitative MRI Techniques. J. Clin. Med. 2020, 9, 1841. https://doi.org/10.3390/jcm9061841
Belavy DL, Brisby H, Douglas B, Hebelka H, Quittner MJ, Owen PJ, Rantalainen T, Trudel G, Lagerstrand KM. Characterization of Intervertebral Disc Changes in Asymptomatic Individuals with Distinct Physical Activity Histories Using Three Different Quantitative MRI Techniques. Journal of Clinical Medicine. 2020; 9(6):1841. https://doi.org/10.3390/jcm9061841
Chicago/Turabian StyleBelavy, Daniel L., Helena Brisby, Benjamin Douglas, Hanna Hebelka, Matthew J. Quittner, Patrick J. Owen, Timo Rantalainen, Guy Trudel, and Kerstin M. Lagerstrand. 2020. "Characterization of Intervertebral Disc Changes in Asymptomatic Individuals with Distinct Physical Activity Histories Using Three Different Quantitative MRI Techniques" Journal of Clinical Medicine 9, no. 6: 1841. https://doi.org/10.3390/jcm9061841