Pentaglobin® Efficacy in Reducing the Incidence of Sepsis and Transplant-Related Mortality in Pediatric Patients Undergoing Hematopoietic Stem Cell Transplantation: A Retrospective Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
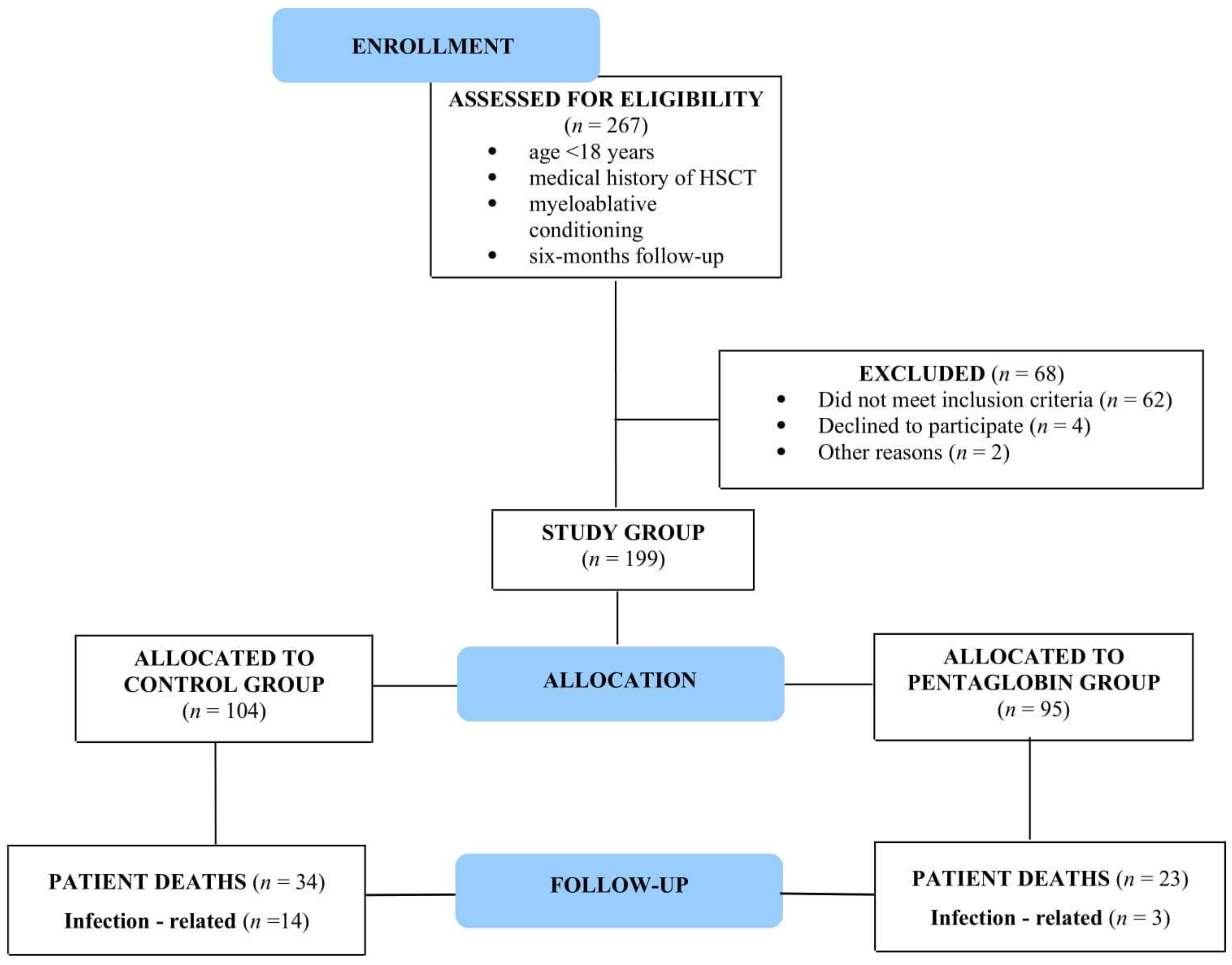
2.1. Study Design and Population
2.2. HSCT Procedure
2.3. Pentaglobin® Administration
2.4. Statistical Analysis
3. Results
3.1. Study Population
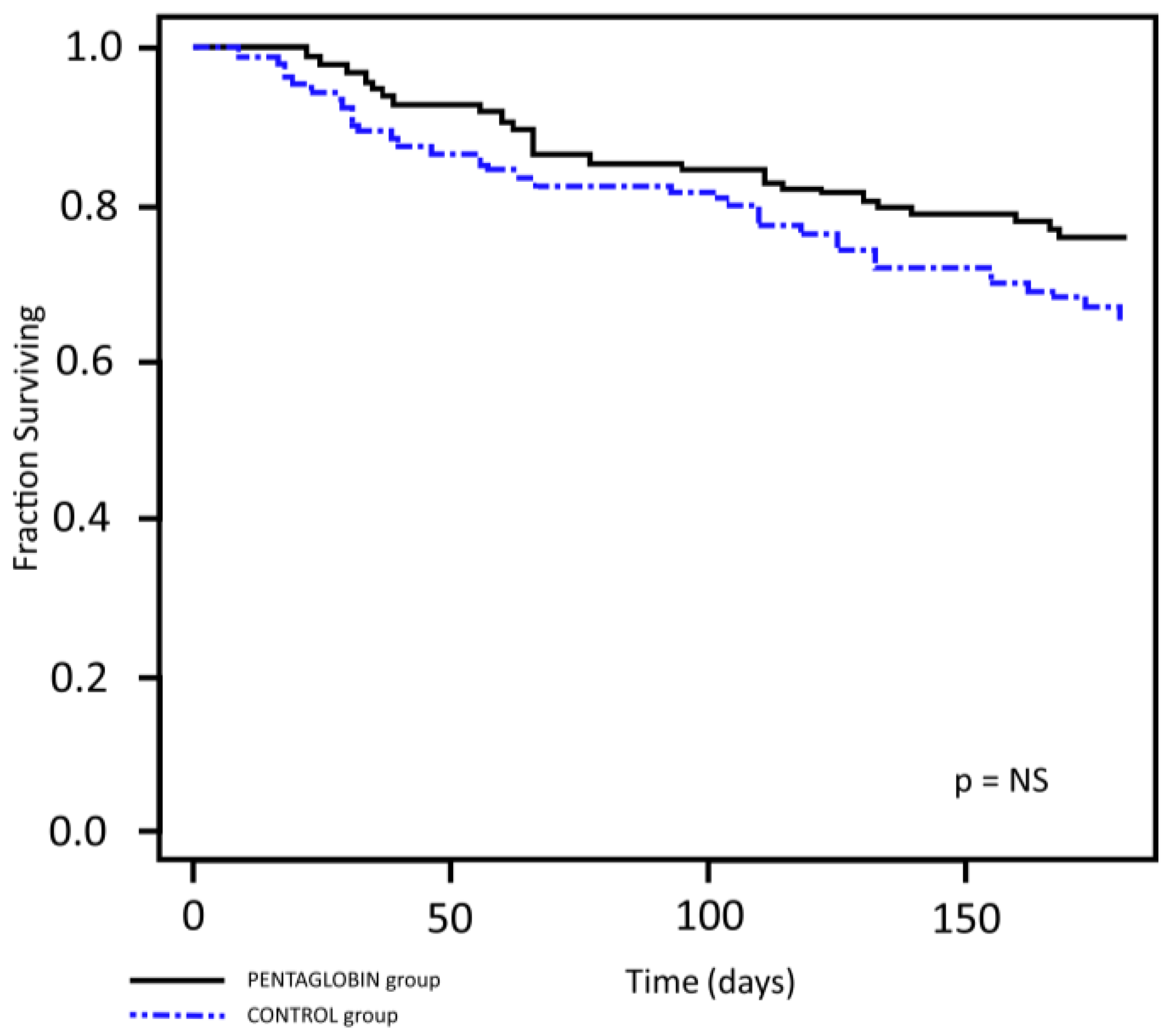
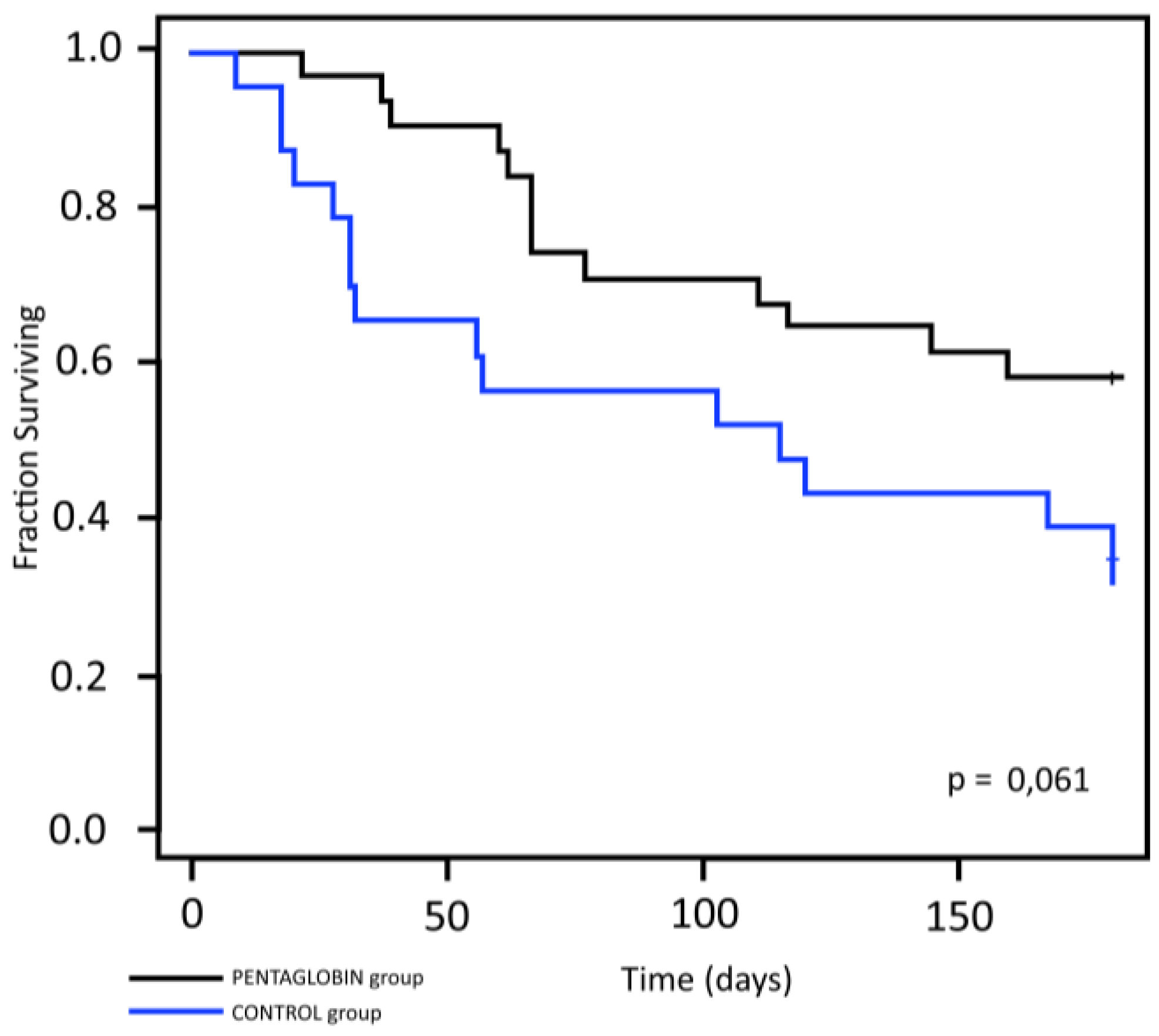
3.2. Primary Outcome: Six-Month Survival Rate
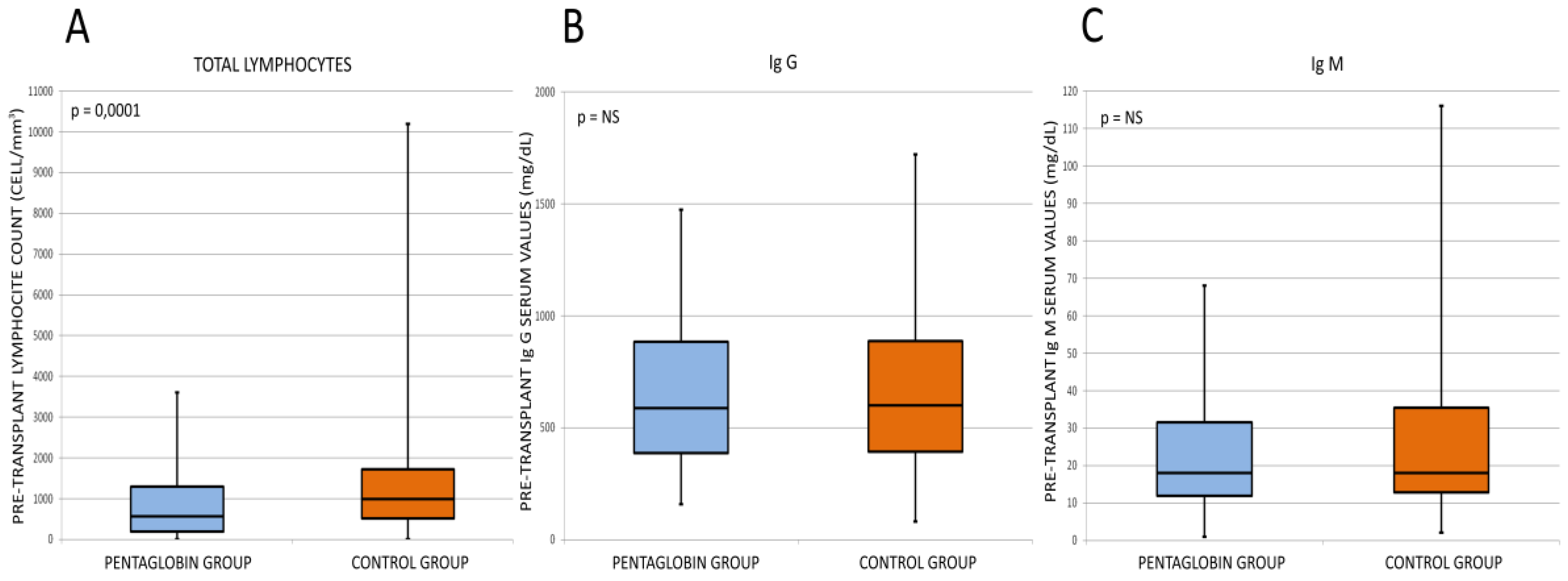
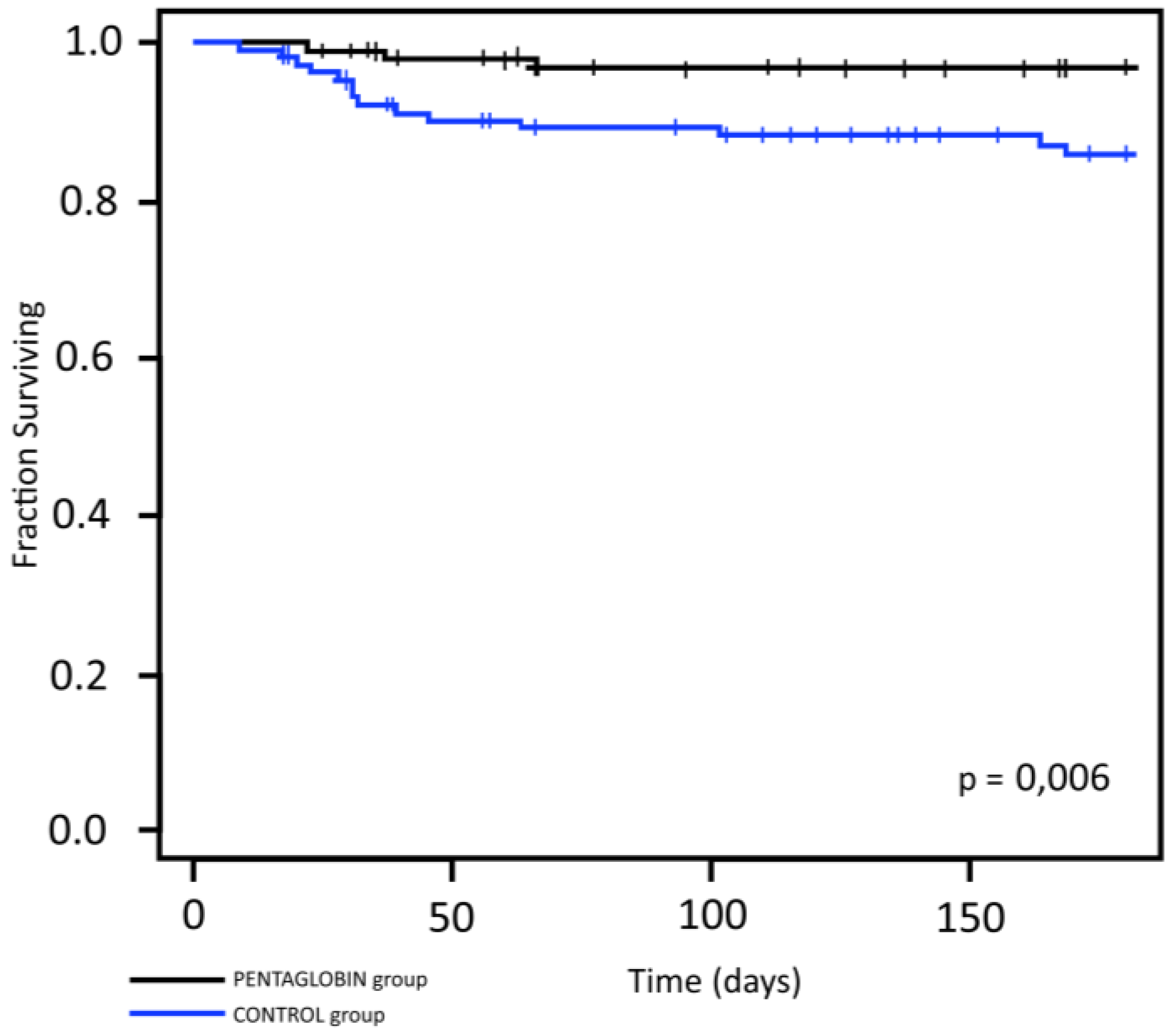
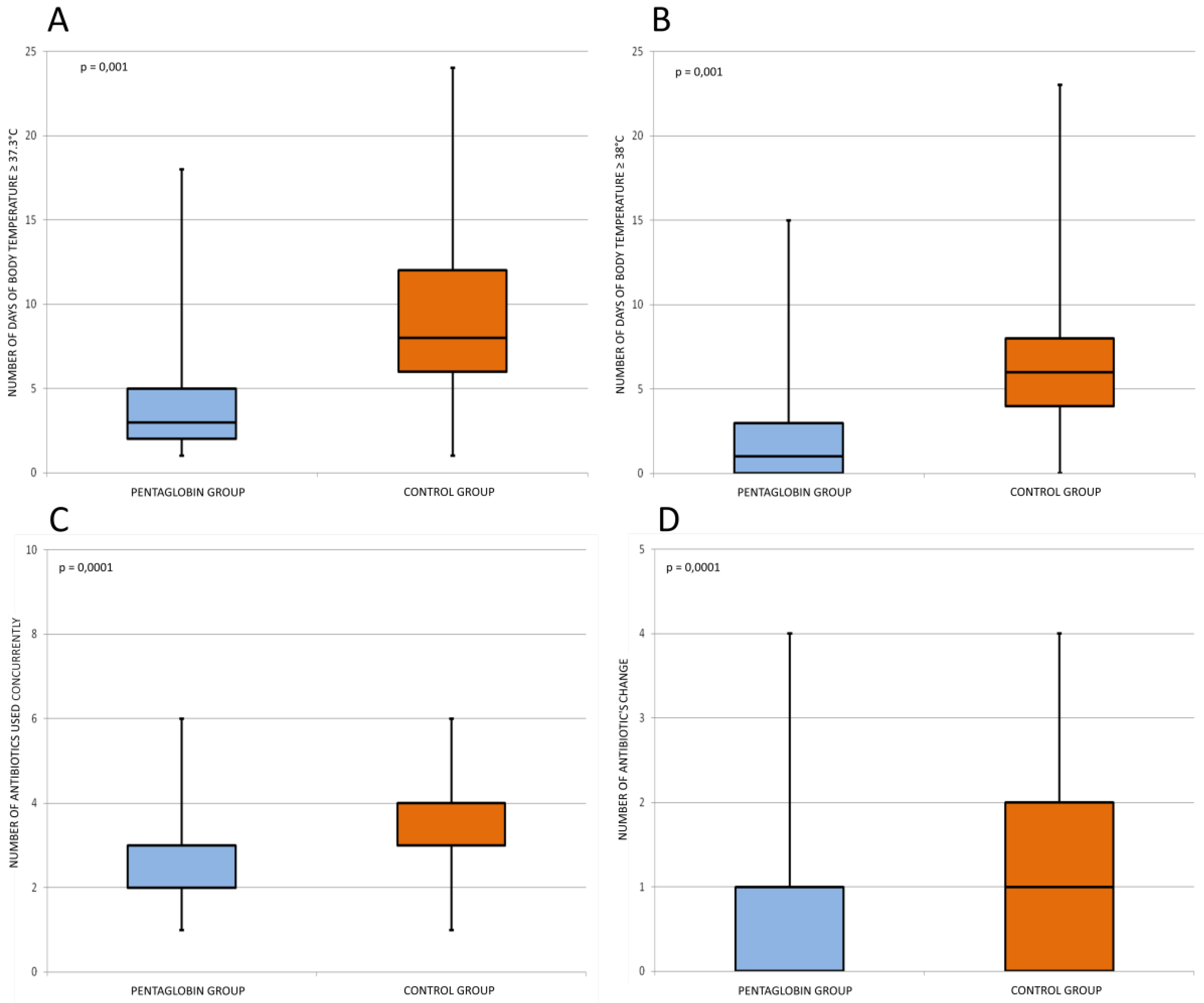
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Storb, R.; Gyurkocza, B.; Storer, B.E.; Sorror, M.L.; Blume, K.; Niederwieser, D.; Chauncey, T.R.; Pulsipher, M.A.; Petersen, F.B.; Sahebi, F.; et al. Graft-versus-host disease and graft-versus-tumor effects after allogenic hematopoietic cell transplantation. J. Clin. Oncol. 2013, 31, 1530–1538. [Google Scholar] [CrossRef] [PubMed]
- Stern, M.; de Wreede, L.C.; Brand, R.; van Biezen, A.; Dreger, P.; Mohty, M.; de Witte, T.M.; Kröger, N.; Ruutu, T. Sensitivity of haematological malignancies to graft-versus-host effects: An EBMT megafile analysis. Leukemia 2014, 28, 2235–2240. [Google Scholar] [CrossRef] [PubMed]
- Copelan, E.A. Hematopoietic Stem-Cell Transplantation. N. Engl. J. Med. 2006, 354, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Ricci, M.J.; Medin, J.A.; Foley, R.S. Advances in haplo-identical stem cell transplantation in adults with high-risk hematological malignancies. World J. Stem Cells 2014, 6, 380–390. [Google Scholar] [CrossRef] [PubMed]
- Mohty, B.; Mohty, M. Long-term complications and side effects after allogeneic hematopoietic stem cell transplantation: An update. Blood Canc. J. 2011, 1, 16. [Google Scholar] [CrossRef] [Green Version]
- Bakhtiar, S.; Salzmann-Manrique, E.; Hutter, M.; Hutter, M.; Krenn, T.; Duerken, M.; Faber, J.; Reinhard, H.; Kreyenberg, H.; Huenecke, S.; et al. AlloHSCT in paediatric ALL and AML in complete remission: Improvement over time impacted by accreditation? Bone Marr. Transp. 2019, 54, 737–745. [Google Scholar] [CrossRef]
- Busca, A.; Pagano, L. Antifungal Therapy in Hematopoietic Stem Cell Transplant Recipients. Mediterr. J. Hematol. Infect. Dis. 2016, 8, e2016039. [Google Scholar] [CrossRef] [Green Version]
- Dalle, J.H.; Balduzzi, A.; Bader, P.; Lankester, A.; Yaniv, I.; Wachowiak, J.; Pieczonka, A.; Bierings, M.; Yesilipek, A.; Sedlaçek, P.; et al. Allogenic Stem Cell Transplantation from HLA-Mismatched Donors for Pediatric Patients with Acute Lymphoblastic Leukemia Treated According to the 2003 BFM and 2007 International BFM Studies: Impact of Disease Risk on Outcomes. Biol. Blood Marr. Transp. 2018, 24, 1848–1855. [Google Scholar] [CrossRef] [Green Version]
- Mohty, M.; Apperley, J.F. Long-term physiological side effects after allogenic bone marrow transplantation. Hematol. Am. Soc. Hematol. Educ. Prog. 2010, 2010, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Gratwohl, A.; Pasquini, M.C.; Aljurf, M.; Atsuta, Y.; Baldomero, H.; Foeken, L.; Gratwohl, M.; Bouzas, L.F.; Confer, D.; Frauendorfer, K.; et al. One million haemopoietic stem-cell transplants: A retrospective observational study. Lancet Haematol. 2015, 2, 91–100. [Google Scholar] [CrossRef]
- Brissot, E.; Rialland, F.; Cahu, X.; Strullu, M.; Corradini, N.; Thomas, C.; Blin, N.; Rialland, X.; Thebaid, E.; Chevallier, P.; et al. Improvement of overall survival after allogenic hematopoietic stem cell transplantation for children and adolescents: A three decade experience of a single institution. Bone Marr. Transp. 2016, 51, 267–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolff, S.N. Second hematopoietic stem cell transplantation for the treatment of graft failure, graft rejection or relapse after allogenic transplantation. Bone Marr. Transp. 2002, 29, 545–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez, F.; Parker, P.; Nademanee, A.; Rodriguez, R.; Al-Kadhimi, Z.; Bhatia, R.; Cohen, S.; Falk, P.; Fung, H.; Kirschbaum, M.; et al. Efficacy of mycophenolate mofetil in the treatment of chronic graft-versus-host disease. Biol. Blood Marr. Transp. 2005, 11, 307–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gratwohl, A.; Stern, M.; Brand, R.; Apperley, J.; Baldomero, H.; de Witte, T.; Dini, G.; Rocha, V.; Passweg, J.; Sureda, A.; et al. Risk score for outcome after allogenic hematopoietic stem cell transplantation. Cancer 2009, 115, 4715–4726. [Google Scholar] [CrossRef]
- Hodby, K.A.; Marks, D.I. Recent Advances in the Management of Acute Lymphoblastic Leukaemia. Curr. Treat. Opt. Oncol. 2020, 21, 23. [Google Scholar] [CrossRef]
- Valero, C. New Panfungal Real-Time PCR Assay for Diagnosis of Invasive Fungal Infections. J. Clin. Microbiol. 2016, 54, 2910–2918. [Google Scholar] [CrossRef] [Green Version]
- Trotter, A.J.; Aydin, A.; Strinden, M.J.; O’Grady, J. Recent and emerging technologies for the rapid diagnosis of infection and antimicrobial resistance. Curr. Opin. Microbiol. 2019, 51, 39–45. [Google Scholar] [CrossRef]
- Pilmis, B.; Petitjean, G.; Lesprit, P.; Lafaurie, M.; El Helali, N.; Le Monnier, A. Continuous infusion of ceftolozane/tazobactam is associated with a higher probability of target attainment in patients infected with Pseudomonas aeruginosa. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1457–1461. [Google Scholar] [CrossRef]
- Hoegy, D.; Goutelle, S.; Garnier, N.; Rénard, C.; Faure-Conter, C.; Bergeron, C.; Bertrand, Y.; Bleyzac, N. Continuous intravenous vancomycin in children with normal renal function hospitalized in hematology-oncology: Prospective validation of a dosing regimen optimizing steady-state concentration. Fundam. Clin. Pharmacol. 2018, 32, 323–329. [Google Scholar] [CrossRef]
- Busca, A.; Candoni, A.; Pagano, L.; Scaglione, F.; Viscoli, C. Prophylaxis and treatment of invasive fungal infections in hematological patients. Rev. Health Care 2012, 3, 27–40. [Google Scholar] [CrossRef]
- Norrby-Teglund, A.; Haque, K.N.; Hammarstrom, L. Intravenous polyclonal IgM-enriched immunoglobulin therapy in sepsis: A review of clinical efficacy in relation to microbiological aetiology and severity of sepsis. Review. J. Intern. Med. 2006, 260, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Haque, K.N.; Remo, C.; Bahakim, H. Comparison of two types of intravenous immunoglobulins in the treatment of neonatal sepsis. Clin. Exp. Immunol. 1995, 101, 328–333. [Google Scholar] [CrossRef] [PubMed]
- El-Nawawy, A.; El-Kinany, H.; Hamdy El-Sayed, M.; Boshra, N. Intravenous polyclonal immunoglobulin administration to sepsis syndrome patients: A prospective study in a pediatric intensive care unit. J. Trop. Pediatr. 2005, 51, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azık, F.; Bayram, C.; Erkoçoğlu, M.; Tezer, H.; Yazal Erdem, A.; Işık, P.; Avcı, Z.; Özbek, N.; Tavil, B.; Tunc, B. Comparison of prophylactic use of intravenous immunoglobulin versus Pentaglobin in pediatric patients after hematopoietic stem cell transplantation. Pediatr. Transplant. 2016, 20, 276–283. [Google Scholar] [CrossRef]
- Poynton, C.H.; Jackson, S.; Fegan, C.; Barnes, R.A.; Whittaker, J.A. Use of Ig-M enriched intravenous immunoglobulin (Pentaglobin) in bone marrow transplantation. Bone Marr. Transp. 1992, 9, 451–457. [Google Scholar]
- Jackson, S.K.; Parton, J.; Barnes, R.A.; Poynton, C.H.; Fegan, C.D. Effect of Ig-M enriched intravenous immunoglobulin (Pentaglobin) on endotoxaemia and anti-endotoxin antibodies in bone marrow transplantation. Eur. J. Clin. Investig. 1993, 23, 540–545. [Google Scholar] [CrossRef]
- Behre, G.; Schedel, I.; Nentwig, B.; Wormann, B.; Essink, M.; Hiddermann, W. Endotoxin concentration in neutropenic patients with suspected gram-negative sepsis: Correlation with clinical outcome and determination of anti-endotoxin core antibodies during therapy with polyclonal immunoglobulin M-enriched immunoglobulins. Antimicrob. Agents Chemother. 1992, 36, 2139–2146. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Pentaglobin Group | Control Group |
|---|---|---|
| Number of patients (%) | 95 (48) | 104 (52) |
| Sex, number (%) | ||
| Male | 64 (67.4) | 69 (66.3) |
| Female | 31 (32.6) | 35 (33.7) |
| Age at transplant, years, mean (± SD) | 9.6 (±5.1) | 8.0 (±5.6) |
| Underlying disease, number (%): | ||
| Acute lymphoblastic leukaemia | 42 (44) | 32 (31) |
| Acute myeloid leukaemia | 16 (17) | 20 (19) |
| Myelodysplastic syndrome | 8 (8) | 10 (10) |
| Solid tumour | 20 (21) | 19 (18) |
| Other | 9 (10) | 23 (22) |
| Disease stage, number (%) * | ||
| Early | 22 (33) | 25 (40) |
| Intermediate | 25 (38) | 20 (32) |
| Late | 19 (29) | 17 (28) |
| Type of transplant, number (%) | ||
| Autologous | 15 (16) | 15 (14) |
| Allogeneic: | 80 (84) | 89 (86) |
| Matched related donor | 20 (25) | 33 (37) |
| Matched unrelated donor | 41 (51) | 38 (43) |
| Haploidentical donor | 19 (24) | 18 (20) |
| Myeloablative conditioning, number (%) | ||
| MCHT-based | 11 (12) | 24 (23) |
| TBI-based | 84 (88) | 80 (77) |
| Graft source, number (%) | ||
| Bone marrow | 70 (74) | 84 (81) |
| Peripheral blood stem cells | 25 (26) | 20 (19) |
| Variables | Pentaglobin Group | Control Group | p-Value |
|---|---|---|---|
| (95 Patients) | (104 Patients) | ||
| Type of infection, number (%): | |||
| Sepsis | 6 (6.3) | 14 (13.5) | 0.104 |
| Pneumonia | 7 (6.7) | 13 (13.7) | 0.106 |
| Pulmonary aspergillosis | 1 (1.0) | 1 (0.95) | 1 |
| Brain abscess | 4 (4.2) | 0 | 0.049 |
| Soft tissue infections | 1 (0.95) | 5 (5.3) | 0.104 |
| Cholangitis and biliary tract infection | 0 | 3 (3.2) | 0.105 |
| Mucositis- enterocolitis | 62 (65.3) | 81 (77.9) | 0.084 |
| Other | 1 (1.0) | 0 | 0.475 |
| Days with body temperature ≥ 37.3 °C, mean (± SD) | 4.2 (3.1) | 8.9 (4.9) | <0.0001 |
| Days with body temperature ≥ 38.0 °C, mean (± SD) | 2.1 (2.8) | 6.6 (4.3) | <0.0001 |
| Days on antibiotic treatment, mean (± SD) | 15.1 (5.4) | 16.8 (7.2) | 0.165 |
| Number of antibiotics used, mean (± SD) | 2.7 (1.0) | 3.3 (1.0) | <0.0001 |
| Antibiotic changes during infective episode, mean (± SD) | 0.6 (0.8) | 1.1 (1.0) | <0.0001 |
| Infective episode recovery, number (%) | 93 (97.9) | 96 (92.3) | 0.105 |
| Consecutive infections, number (%): | 33 (34.7) | 39 (37.1) | 0.769 |
| Bacterial | 1 (3.0) | 8 (20.5) | 0.037 |
| Fungal | 4 (12.1) | 5 (12.8) | 1 |
| Opportunistic | 1 (3.0) | 3 (7.7) | 0.623 |
| Virus | 27 (81.8) | 23 (59.0) | 0.328 |
| Overall survival at 6 months, number (%) | 72 (76) | 70 (67) | 0.081 |
| Cause of death, number (%): | |||
| Disease progression | 11 (47.8) | 9 (32.4) | 0.431 |
| Transplant-related mortality | 12 (52.2) | 23 (67.6) | 0.086 |
| of which infection | 3 (25) | 14 (60.8) | 0.04 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlone, G.; Torelli, L.; Maestro, A.; Zanon, D.; Barbi, E.; Maximova, N. Pentaglobin® Efficacy in Reducing the Incidence of Sepsis and Transplant-Related Mortality in Pediatric Patients Undergoing Hematopoietic Stem Cell Transplantation: A Retrospective Study. J. Clin. Med. 2020, 9, 1592. https://doi.org/10.3390/jcm9051592
Carlone G, Torelli L, Maestro A, Zanon D, Barbi E, Maximova N. Pentaglobin® Efficacy in Reducing the Incidence of Sepsis and Transplant-Related Mortality in Pediatric Patients Undergoing Hematopoietic Stem Cell Transplantation: A Retrospective Study. Journal of Clinical Medicine. 2020; 9(5):1592. https://doi.org/10.3390/jcm9051592
Chicago/Turabian StyleCarlone, Giorgia, Lucio Torelli, Alessandra Maestro, Davide Zanon, Egidio Barbi, and Natalia Maximova. 2020. "Pentaglobin® Efficacy in Reducing the Incidence of Sepsis and Transplant-Related Mortality in Pediatric Patients Undergoing Hematopoietic Stem Cell Transplantation: A Retrospective Study" Journal of Clinical Medicine 9, no. 5: 1592. https://doi.org/10.3390/jcm9051592