Significance of Soluble CD93 in Type 2 Diabetes as a Biomarker for Diabetic Nephropathy: Integrated Results from Human and Rodent Studies

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Study Design and Population
2.2. Anthropometric and Biochemical Measurements
2.3. Cell Culture and Animal Experiment
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics of the Study Subjects
3.2. High Prevalence of DN in the High Serum sCD93 Group
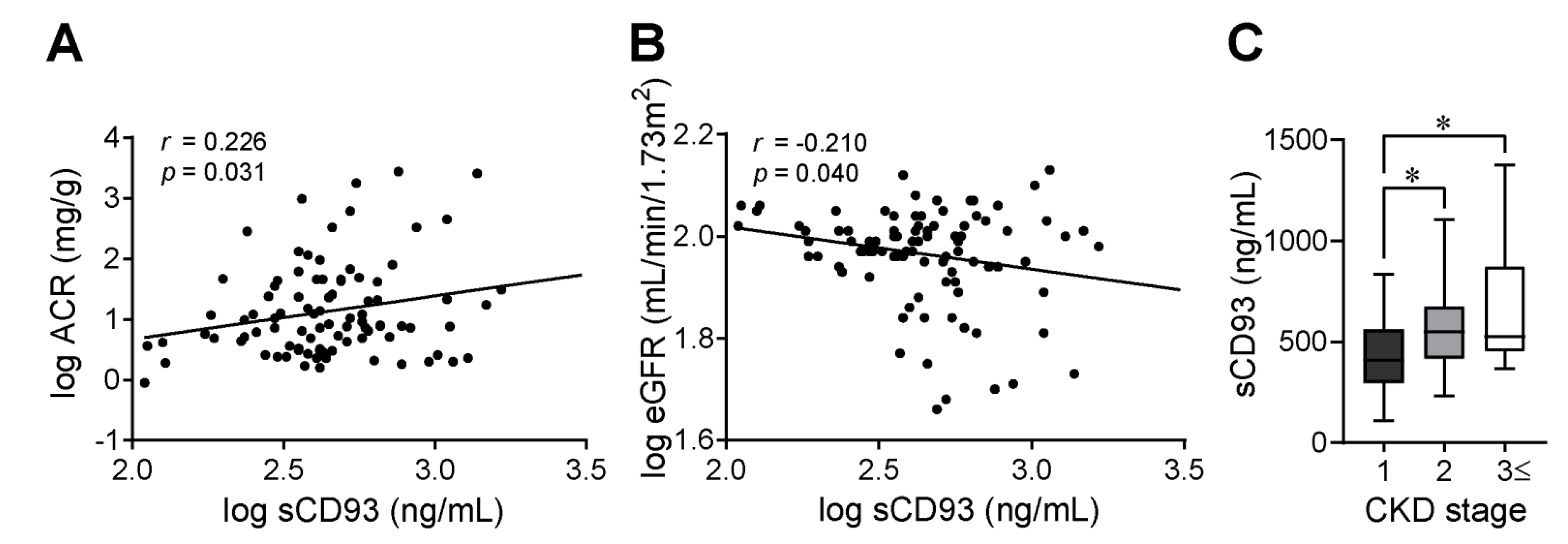
3.3. Significant Association between sCD93 Levels and DN Markers
3.4. Higher Prevalence of Renal Complications in Patients with High Serum sCD93 Levels
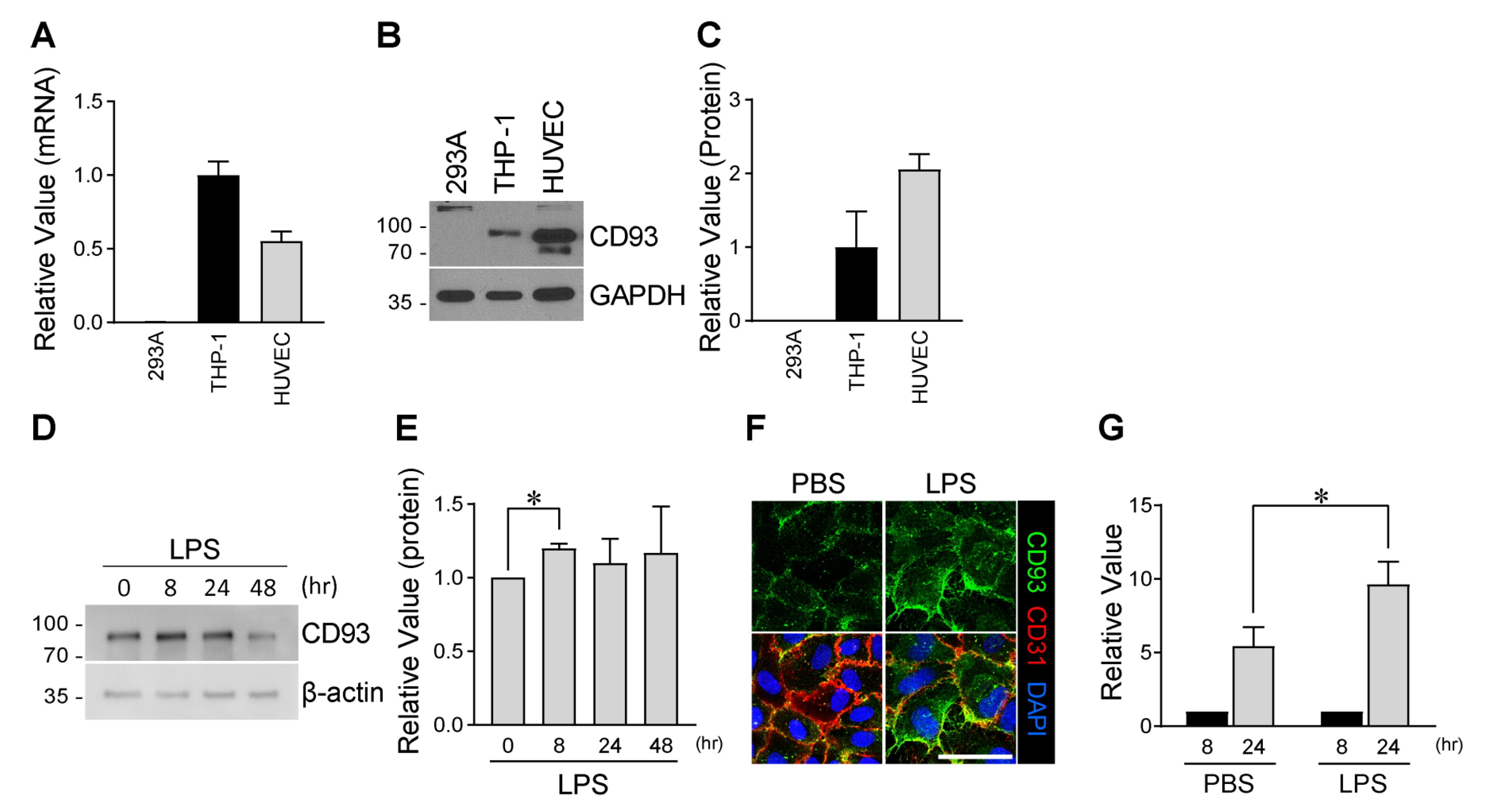
3.5. Enhanced Production of sCD93 from Vascular Endothelial Cells by Inflammation
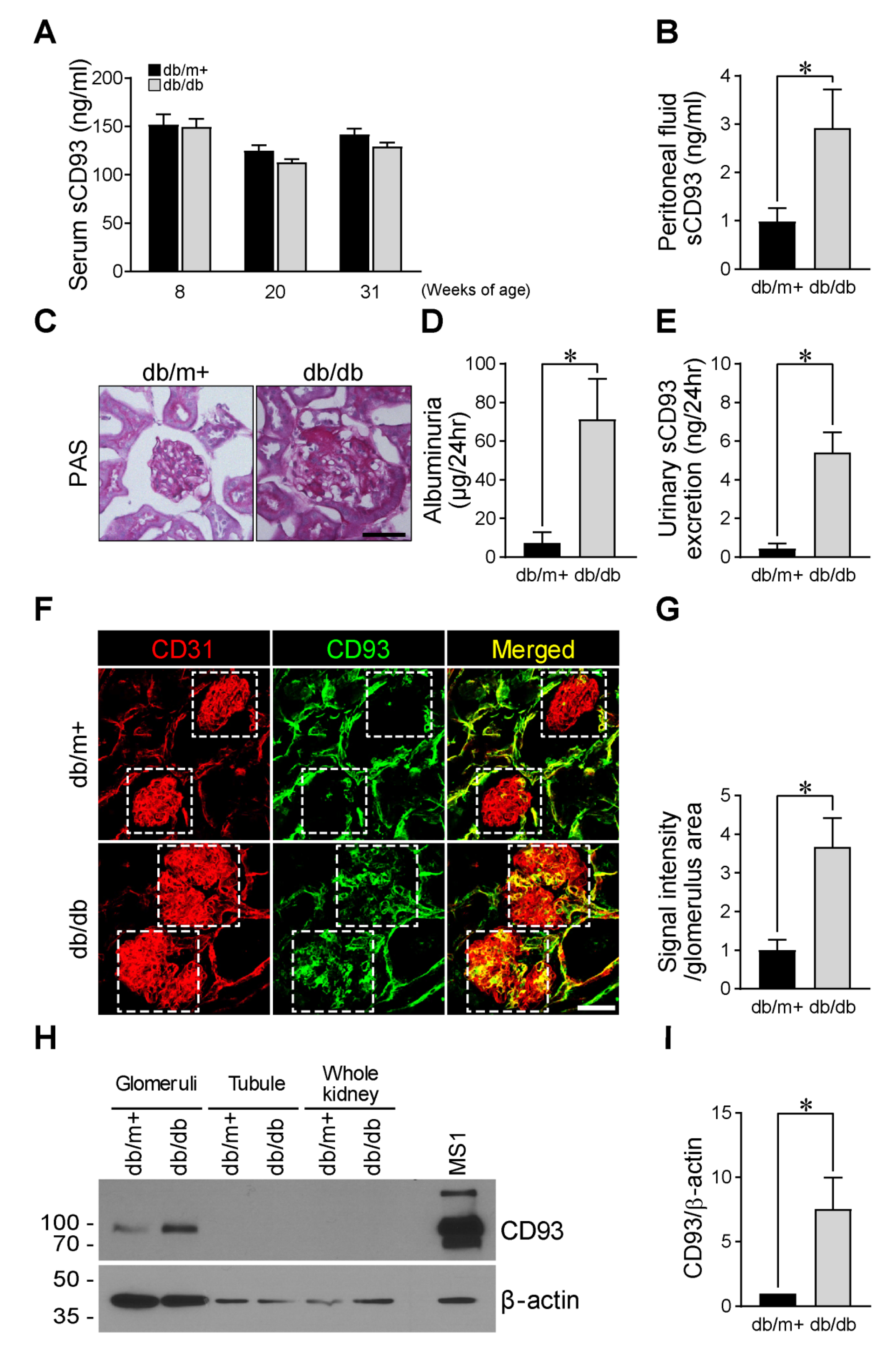
3.6. High Peritoneal sCD93 Levels and Enhanced CD93 Expression in the Glomerulus of Diabetic Mice
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethics Approval
Availability of Data and Materials
References
- Nepomuceno, R.R.; Henschen-Edman, A.H.; Burgess, W.H.; Tenner, A.J. Cdna cloning and primary structure analysis of c1qr(p), the human c1q/mbl/spa receptor that mediates enhanced phagocytosis in vitro. Immunity 1997, 6, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Fonseca, M.I.; Carpenter, P.M.; Park, M.; Palmarini, G.; Nelson, E.L.; Tenner, A.J. C1qr(p), a myeloid cell receptor in blood, is predominantly expressed on endothelial cells in human tissue. J. Leukoc. Biol. 2001, 70, 793–800. [Google Scholar] [PubMed]
- McGreal, E.P.; Ikewaki, N.; Akatsu, H.; Morgan, B.P.; Gasque, P. Human c1qrp is identical with cd93 and the mni-11 antigen but does not bind c1q. J. Immunol. 2002, 168, 5222–5232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohlson, S.S.; Silva, R.; Fonseca, M.I.; Tenner, A.J. Cd93 is rapidly shed from the surface of human myeloid cells and the soluble form is detected in human plasma. J. Immunol. 2005, 175, 1239–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenlee, M.C.; Sullivan, S.A.; Bohlson, S.S. Detection and characterization of soluble cd93 released during inflammation. Inflamm. Res. 2009, 58, 909–919. [Google Scholar] [CrossRef] [PubMed]
- Harhausen, D.; Prinz, V.; Ziegler, G.; Gertz, K.; Endres, M.; Lehrach, H.; Gasque, P.; Botto, M.; Stahel, P.F.; Dirnagl, U.; et al. Cd93/aa4.1: A novel regulator of inflammation in murine focal cerebral ischemia. J. Immunol. 2010, 184, 6407–6417. [Google Scholar] [CrossRef]
- Malarstig, A.; Silveira, A.; Wagsater, D.; Ohrvik, J.; Backlund, A.; Samnegard, A.; Khademi, M.; Hellenius, M.L.; Leander, K.; Olsson, T.; et al. Plasma cd93 concentration is a potential novel biomarker for coronary artery disease. J. Intern. Med. 2011, 270, 229–236. [Google Scholar] [CrossRef]
- Moosig, F.; Fahndrich, E.; Knorr-Spahr, A.; Bottcher, S.; Ritgen, M.; Zeuner, R.; Kneba, M.; Schroder, J.O. C1qrp (cd93) expression on peripheral blood monocytes in patients with systemic lupus erythematosus. Rheumatol. Int. 2006, 26, 1109–1112. [Google Scholar] [CrossRef]
- Sigari, N.; Jalili, A.; Mahdawi, L.; Ghaderi, E.; Shilan, M. Soluble cd93 as a novel biomarker in asthma exacerbation. Allergy Asthma Immunol. Res. 2016, 8, 461–465. [Google Scholar] [CrossRef] [Green Version]
- Bao, L.; Tang, M.; Zhang, Q.; You, B.; Shan, Y.; Shi, S.; Li, L.; Hu, S.; You, Y. Elevated expression of cd93 promotes angiogenesis and tumor growth in nasopharyngeal carcinoma. Biochem. Biophys. Res. Commun. 2016, 476, 467–474. [Google Scholar] [CrossRef]
- Postic, C.; Shiota, M.; Niswender, K.D.; Jetton, T.L.; Chen, Y.; Moates, J.M.; Shelton, K.D.; Lindner, J.; Cherrington, A.D.; Magnuson, M.A. Dual roles for glucokinase in glucose homeostasis as determined by liver and pancreatic beta cell-specific gene knock-outs using cre recombinase. J. Biol. Chem. 1999, 274, 305–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. 1. Improving care and promoting health in populations: Standards of medical care in diabetes-2018. Diabetes Care 2018, 41, S7–S12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, J.L.; de Azevedo, M.J.; Silveiro, S.P.; Canani, L.H.; Caramori, M.L.; Zelmanovitz, T. Diabetic nephropathy: Diagnosis, prevention, and treatment. Diabetes Care 2005, 28, 164–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 10. Microvascular complications and foot care: Standards of medical care in diabetes-2018. Diabetes Care 2018, 41, S105–S118. [Google Scholar] [CrossRef] [Green Version]
- Jeon, J.W.; Jung, J.G.; Shin, E.C.; Choi, H.I.; Kim, H.Y.; Cho, M.L.; Kim, S.W.; Jang, Y.S.; Sohn, M.H.; Moon, J.H.; et al. Soluble cd93 induces differentiation of monocytes and enhances tlr responses. J. Immunol. 2010, 185, 4921–4927. [Google Scholar] [CrossRef] [Green Version]
- Youn, J.C.; Yu, H.T.; Jeon, J.W.; Lee, H.S.; Jang, Y.; Park, Y.W.; Park, Y.B.; Shin, E.C.; Ha, J.W. Soluble cd93 levels in patients with acute myocardial infarction and its implication on clinical outcome. PLoS ONE 2014, 9, e96538. [Google Scholar] [CrossRef]
- Park, H.S.; Kim, H.Z.; Park, J.S.; Lee, J.; Lee, S.P.; Kim, H.; Ahn, C.W.; Nakaoka, Y.; Koh, G.Y.; Kang, S. Beta-cell-derived angiopoietin-1 regulates insulin secretion and glucose homeostasis by stabilizing the islet microenvironment. Diabetes 2019, 68, 774–786. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.; Lee, S.P.; Kim, K.E.; Kim, H.Z.; Memet, S.; Koh, G.Y. Toll-like receptor 4 in lymphatic endothelial cells contributes to lps-induced lymphangiogenesis by chemotactic recruitment of macrophages. Blood 2009, 113, 2605–2613. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, T. Isolation and enrichment of glomeruli using sieving techniques. In Renal and Urinary Proteomics: Methods and Protocols; Thongboonkerd, V., Ed.; Wiley-VCH Verlag GmbH & Co. KGaA: Weinheim, Germany, 2009; pp. 1–7. [Google Scholar] [CrossRef]
- Choi, J.W.; Jo, A.; Kim, M.; Park, H.S.; Chung, S.S.; Kang, S.; Park, K.S. Bnip3 is essential for mitochondrial bioenergetics during adipocyte remodelling in mice. Diabetologia 2016, 59, 571–581. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Vanhoutte, P.M. Macro- and microvascular endothelial dysfunction in diabetes. J. Diabetes 2017, 9, 434–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Z.; Zheng, F. Immune cells and inflammation in diabetic nephropathy. J. Diabetes Res. 2016, 2016, 1841690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heemken, R.; Gandawidjaja, L.; Hau, T. Peritonitis: Pathophysiology and local defense mechanisms. Hepatogastroenterology 1997, 44, 927–936. [Google Scholar] [PubMed]
- Galvagni, F.; Nardi, F.; Maida, M.; Bernardini, G.; Vannuccini, S.; Petraglia, F.; Santucci, A.; Orlandini, M. Cd93 and dystroglycan cooperation in human endothelial cell adhesion and migration adhesion and migration. Oncotarget 2016, 7, 10090–10103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girach, A.; Manner, D.; Porta, M. Diabetic microvascular complications: Can patients at risk be identified? A review. Int. J. Clin. Pract. 2006, 60, 1471–1483. [Google Scholar] [CrossRef] [PubMed]
- Valencia, W.M.; Florez, H. How to prevent the microvascular complications of type 2 diabetes beyond glucose control. BMJ 2017, 356, i6505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahlqvist, E.; van Zuydam, N.R.; Groop, L.C.; McCarthy, M.I. The genetics of diabetic complications. Nat. Rev. Nephrol. 2015, 11, 277–287. [Google Scholar] [CrossRef]
- Leung, A.; Amaram, V.; Natarajan, R. Linking diabetic vascular complications with lncrnas. Vascul. Pharmacol. 2019, 114, 139–144. [Google Scholar] [CrossRef]
- Liu, R.; Lee, K.; He, J.C. Genetics and epigenetics of diabetic nephropathy. Kidney Dis. (Basel) 2015, 1, 42–51. [Google Scholar] [CrossRef]
- Strawbridge, R.J.; Hilding, A.; Silveira, A.; Osterholm, C.; Sennblad, B.; McLeod, O.; Tsikrika, P.; Foroogh, F.; Tremoli, E.; Baldassarre, D.; et al. Soluble cd93 is involved in metabolic dysregulation but does not influence carotid intima-media thickness. Diabetes 2016, 65, 2888–2899. [Google Scholar] [CrossRef] [Green Version]
- King, G.L. The role of inflammatory cytokines in diabetes and its complications. J. Periodontol. 2008, 79, 1527–1534. [Google Scholar] [CrossRef] [PubMed]
- Hartge, M.M.; Unger, T.; Kintscher, U. The endothelium and vascular inflammation in diabetes. Diabetes Vasc. Dis. Res. 2007, 4, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Brosius, F.C., 3rd; Alpers, C.E.; Bottinger, E.P.; Breyer, M.D.; Coffman, T.M.; Gurley, S.B.; Harris, R.C.; Kakoki, M.; Kretzler, M.; Leiter, E.H.; et al. Mouse models of diabetic nephropathy. J. Am. Soc. Nephrol. 2009, 20, 2503–2512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, K.; McCue, P.; Dunn, S.R. Diabetic kidney disease in the db/db mouse. Am. J. Physiol. Renal Physiol. 2003, 284, F1138–F1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broche, F.; Tellado, J.M. Defense mechanisms of the peritoneal cavity. Curr. Opin. Crit. Care 2001, 7, 105–116. [Google Scholar] [CrossRef] [PubMed]
- Sinha, S.K.; Nicholas, S.B.; Sung, J.H.; Correa, A.; Rajavashisth, T.B.; Norris, K.C.; Lee, J.E. Hs-crp is associated with incident diabetic nephropathy: Findings from the jackson heart study. Diabetes Care 2019, 42, 2083–2089. [Google Scholar] [CrossRef] [PubMed]
- Matoba, K.; Takeda, Y.; Nagai, Y.; Kawanami, D.; Utsunomiya, K.; Nishimura, R. Unraveling the role of inflammation in the pathogenesis of diabetic kidney disease. Int. J. Mol. Sci. 2019, 20, 3393. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.K.; Yun, K.J.; Chun, H.J.; Jang, E.H.; Han, K.D.; Park, Y.M.; Baek, K.H.; Song, K.H.; Cha, B.Y.; Park, C.S.; et al. Clinical utility of serum beta-2-microglobulin as a predictor of diabetic complications in patients with type 2 diabetes without renal impairment. Diabetes Metab. 2014, 40, 459–465. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (N = 97) | Low Serum sCD93 (n = 49) | High Serum sCD93 (n = 48) | p | |
|---|---|---|---|---|
| sCD93 (ng/mL) | 520.41 ± 311.34 | 310.71 ± 95.14 | 734.48 ± 309.99 | <0.001 |
| log(sCD93) (ng/mL) | 2.65 ± 0.24 | 2.47 ± 0.16 | 2.84 ± 0.16 | <0.001 |
| Age (year) | 56.39 ± 11.09 | 56.41 ± 10.48 | 56.38 ± 11.78 | 0.988 |
| Male (n, %) | 75 (77.3) | 41 (83.7) | 34 (70.8) | 0.131 |
| Hypertension (n, %) | 57 (58.8) | 29 (59.2) | 28 (58.3) | >0.999 |
| Dyslipidemia (n, (%)) | 88 (90.7) | 44 (89.8) | 44 (91.7) | >0.999 |
| Duration of diabetes (year) | 7.40 ± 8.39 | 6.80 ± 6.90 | 8.02 ± 9.71 | 0.475 |
| DM medications (n, %) | ||||
| SU | 24 (24.7) | 12 (24.5) | 12 (25.0) | 0.954 |
| Metformin | 82 (84.5) | 44 (89.8) | 38 (79.2) | 0.148 |
| DPP4 inhibitor | 53 (54.6) | 28 (57.1) | 25 (52.1) | 0.617 |
| Insulin | 10 (10.3) | 3 (6.1) | 7 (14.6) | 0.199 |
| Other medications (n, %) | ||||
| ACE-I or ARB | 50 (51.5) | 26 (53.1) | 24 (50.0) | 0.763 |
| Statin | 56 (57.7) | 27 (55.1) | 29 (60.4) | 0.596 |
| Fibrate | 8 (8.2) | 6 (12.2) | 2 (4.2) | 0.268 |
| Omega3 | 1 (1.0) | 1 (2.0) | 0 (0.0) | >0.999 |
| BMI (Kg/m²) | 25.34 ± 3.20 | 25.77 ± 3.41 | 24.89 ± 2.95 | 0.174 |
| Fasting glucose (mg/dL) | 133.45 ± 29.77 | 136.06 ± 30.91 | 130.72 ± 28.62 | 0.382 |
| HbA1c (%) | 6.89 ± 0.82 | 6.94 ± 0.85 | 6.84 ± 0.79 | 0.545 |
| BUN (mg/dL) | 15.29 ± 5.08 | 14.98 ± 3.67 | 15.61 ± 6.25 | 0.548 |
| Creatinine (mg/dL) | 0.83 ± 0.21 | 0.80 ± 0.15 | 0.88 ± 0.25 | 0.058 |
| Protein (g/dL) | 7.74 ± 6.74 | 7.07 ± 0.34 | 8.45 ± 9.63 | 0.322 |
| Albumin (g/dL) | 4.53 ± 0.29 | 4.54 ± 0.27 | 4.52 ± 0.31 | 0.716 |
| ALT (IU/L) | 29.05 ± 22.89 | 29.06 ± 14.84 | 29.04 ± 29.19 | 0.997 |
| Total cholesterol (mg/dL) | 167.17 ± 33.43 | 167.98 ± 28.71 | 166.32 ± 38.03 | 0.809 |
| Triglyceride (mg/dL) | 159.80 ± 103.71 | 165.58 ± 108.39 | 153.76 ± 99.44 | 0.583 |
| HDL-cholesterol (mg/dL) | 43.59 ± 8.98 | 42.59 ± 8.75 | 44.65 ± 9.20 | 0.266 |
| LDL-cholesterol (mg/dL) | 91.33 ± 30.95 | 90.87 ± 30.59 | 91.80 ± 31.66 | 0.887 |
| ACR (mg/g) | 125.94 ± 441.96 | 45.17 ± 146.79 | 210.30 ± 605.97 | 0.081 |
| eGFR (CKD-EPI) (mL/min/1.73 m2) | 94.26 ± 18.25 | 97.92 ± 12.82 | 90.43 ± 22.07 | 0.047 |
| Total (n = 97) | Low Serum sCD93 (n = 49) | High Serum sCD93 (n = 48) | p | |
|---|---|---|---|---|
| Macrovascular complications (n, (%)) | ||||
| Cerebrovascular accident | 4 (4.1) | 2 (4.1) | 2 (4.2) | 0.983 |
| Coronary artery disease | 22 (22.7) | 11 (22.4) | 11 (22.9) | 0.956 |
| Peripheral arterial disease | 3 (3.1) | 1 (2.0) | 2 (4.2) | 0.545 |
| No. of macrovascular complications ≥ 2 | 4 (4.1) | 2 (4.1) | 2 (4.2) | 0.983 |
| Microvascular complications (n, (%)) | ||||
| Diabetic retinopathy | 19 (19.6) | 8 (16.3) | 11 (23.4) | 0.384 |
| Diabetic neuropathy | 9 (9.3) | 4 (8.2) | 5 (10.4) | 0.702 |
| Diabetic nephropathy | ||||
| CKD stage | ||||
| CKD, stage 2 (60 ≤ GFR < 90) | 22 (22.9) | 6 (12.2) | 16 (34.0) | 0.011 |
| CKD, stage ≥ 3 (GFR < 60) | 7 (7.3) | 1 (2.0) | 6 (12.7) | 0.043 |
| Proteinuria | ||||
| Microalbuminuria (30 ≤ ACR < 300) | 17 (18.5) | 10 (21.3) | 7 (15.6) | 0.480 |
| Macroalbuminuria (ACR ≥ 300) | 8 (8.2) | 1 (2.0) | 7 (14.6) | 0.029 |
| No. of microvascular complications ≥ 2 | 17 (17.5) | 6 (12.2) | 11 (22.9) | 0.167 |
| log(Serum sCD93) | ||
|---|---|---|
| r | p | |
| Age (year) | −0.032 | 0.753 |
| Duration of diabetes (year) | 0.056 | 0.586 |
| Body mass index (kg/m2) | −0.021 | 0.837 |
| Fasting plasma glucose (mg/dL) | −0.104 | 0.312 |
| HbA1c (%) | −0.029 | 0.781 |
| Calcium (mg/dL) | 0.049 | 0.637 |
| Phosphate (mg/dL) | −0.052 | 0.618 |
| Uric acid (mg/dL) | 0.041 | 0.692 |
| BUN (mg/dL) | 0.026 | 0.804 |
| Creatinine (mg/dL) | 0.175 | 0.088 |
| Protein (g/dL) | 0.048 | 0.642 |
| Albumin (g/dL) | −0.109 | 0.289 |
| ALT (IU/L) | −0.083 | 0.421 |
| Total cholesterol(mg/dL) | −0.001 | 0.991 |
| Triglyceride (mg/dL) | −0.025 | 0.811 |
| HDL-cholesterol (mg/dL) | −0.027 | 0.798 |
| LDL-cholesterol (mg/dL) | 0.049 | 0.645 |
| ACR (mg/g) | 0.229 | 0.028 |
| eGFR (CKD-EPI) (mL/min/1.73 m2) | −0.185 | 0.071 |
| Univariate Model | Multivariate Model | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| eGFR (CKD-EPI) | Regression Coefficient | SE | p Value | R2 | Regression Coefficient | SE | p Value | Adjusted R2 | |
| Age (year) | −1.054 | 0.130 | <0.001 | 0.413 | −0.886 | 0.130 | <0.001 | 0.523 | |
| Sex (reference: male) | −2.914 | 4.519 | 0.521 | 0.004 | 5.317 | 3.403 | 0.122 | ||
| Hypertension | −18.722 | 3.287 | <0.001 | 0.257 | −11.290 | 2.991 | <0.001 | ||
| Lipid-lowering medications | −9.422 | 3.792 | 0.015 | 0.062 | −3.451 | 2.851 | 0.229 | ||
| BMI (kg/m2) | −0.615 | 0.587 | 0.298 | 0.012 | −0.094 | 0.431 | 0.828 | ||
| HbA1c (%) | −2.540 | 2.324 | 0.277 | 0.013 | −1.228 | 1.642 | 0.457 | ||
| log(serum sCD93) | −14.025 | 7.681 | 0.071 | 0.034 | −14.734 | 5.564 | 0.010 | ||
| Univariate model | Multivariate Model | ||||||||
| ACR | Regression Coefficient | SE | p Value | R2 | Regression Coefficient | SE | p Value | Adjusted R2 | |
| Age (year) | 0.790 | 4.118 | 0.848 | <0.001 | −2.358 | 4.455 | 0.598 | 0.043 | |
| Sex (reference: male) | 93.021 | 111.901 | 0.408 | 0.008 | 13.971 | 115.827 | 0.904 | ||
| Hypertension | 187.124 | 93.374 | 0.048 | 0.043 | 193.456 | 103.357 | 0.065 | ||
| Lipid-lowering medications | 109.227 | 96.597 | 0.261 | 0.014 | 81.495 | 98.334 | 0.410 | ||
| BMI (kg/m2) | −7.305 | 14.701 | 0.620 | 0.003 | −14.443 | 14.694 | 0.328 | ||
| HbA1c (%) | −54.342 | 55.888 | 0.333 | 0.010 | −40.855 | 55.888 | 0.467 | ||
| log(serum sCD93) | 417.319 | 187.107 | 0.028 | 0.052 | 387.943 | 191.129 | 0.046 | ||
| GFR (CKD-EPI) < 60 (CKD, Stage ≥ 3) | |||
|---|---|---|---|
| Low Serum sCD93 | High Serum sCD93 | p | |
| Model 1 | 1.00 (reference) | 7.024 (0.812–60.766) | 0.077 |
| Model 2 | 1.00 (reference) | 7.080 (0.786–63.746) | 0.081 |
| Model 3 | 1.00 (reference) | 8.345 (0.846–82.353) | 0.069 |
| Macroalbuminuria (ACR ≥ 300) | |||
| Low Serum sCD93 | High Serum sCD93 | p | |
| Model 1 | 1.00 (reference) | 8.474 (0.998–71.941) | 0.050 |
| Model 2 | 1.00 (reference) | 8.571 (00.992–74.071) | 0.051 |
| Model 3 | 1.00 (reference) | 9.109 (0.990–83.837) | 0.051 |
| Diabetic Nephropathy (CKD, Stage ≥ 3 or Macroalbuminuria) | |||
| Low Serum sCD93 | High Serum sCD93 | p | |
| Model 1 | 1.00 (reference) | 5.566 (1.134–27.313) | 0.034 |
| Model 2 | 1.00 (reference) | 5.991 (1.145–31.341) | 0.034 |
| Model 3 | 1.00 (reference) | 7.212 (1.244–41.796) | 0.028 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.; Park, H.S.; Choi, M.Y.; Kim, H.Z.; Moon, S.J.; Ha, J.Y.; Choi, A.; Park, Y.W.; Park, J.S.; Shin, E.-C.; et al. Significance of Soluble CD93 in Type 2 Diabetes as a Biomarker for Diabetic Nephropathy: Integrated Results from Human and Rodent Studies. J. Clin. Med. 2020, 9, 1394. https://doi.org/10.3390/jcm9051394
Lee M, Park HS, Choi MY, Kim HZ, Moon SJ, Ha JY, Choi A, Park YW, Park JS, Shin E-C, et al. Significance of Soluble CD93 in Type 2 Diabetes as a Biomarker for Diabetic Nephropathy: Integrated Results from Human and Rodent Studies. Journal of Clinical Medicine. 2020; 9(5):1394. https://doi.org/10.3390/jcm9051394
Chicago/Turabian StyleLee, Minyoung, Ho Seon Park, Min Yeong Choi, Hak Zoo Kim, Sung Jin Moon, Ji Yoon Ha, ARim Choi, Young Woo Park, Jong Suk Park, Eui-Cheol Shin, and et al. 2020. "Significance of Soluble CD93 in Type 2 Diabetes as a Biomarker for Diabetic Nephropathy: Integrated Results from Human and Rodent Studies" Journal of Clinical Medicine 9, no. 5: 1394. https://doi.org/10.3390/jcm9051394