Endothelin Receptor Antagonists: Status Quo and Future Perspectives for Targeted Therapy

 ,
, 
Abstract
:1. Endothelin in Health and Disease
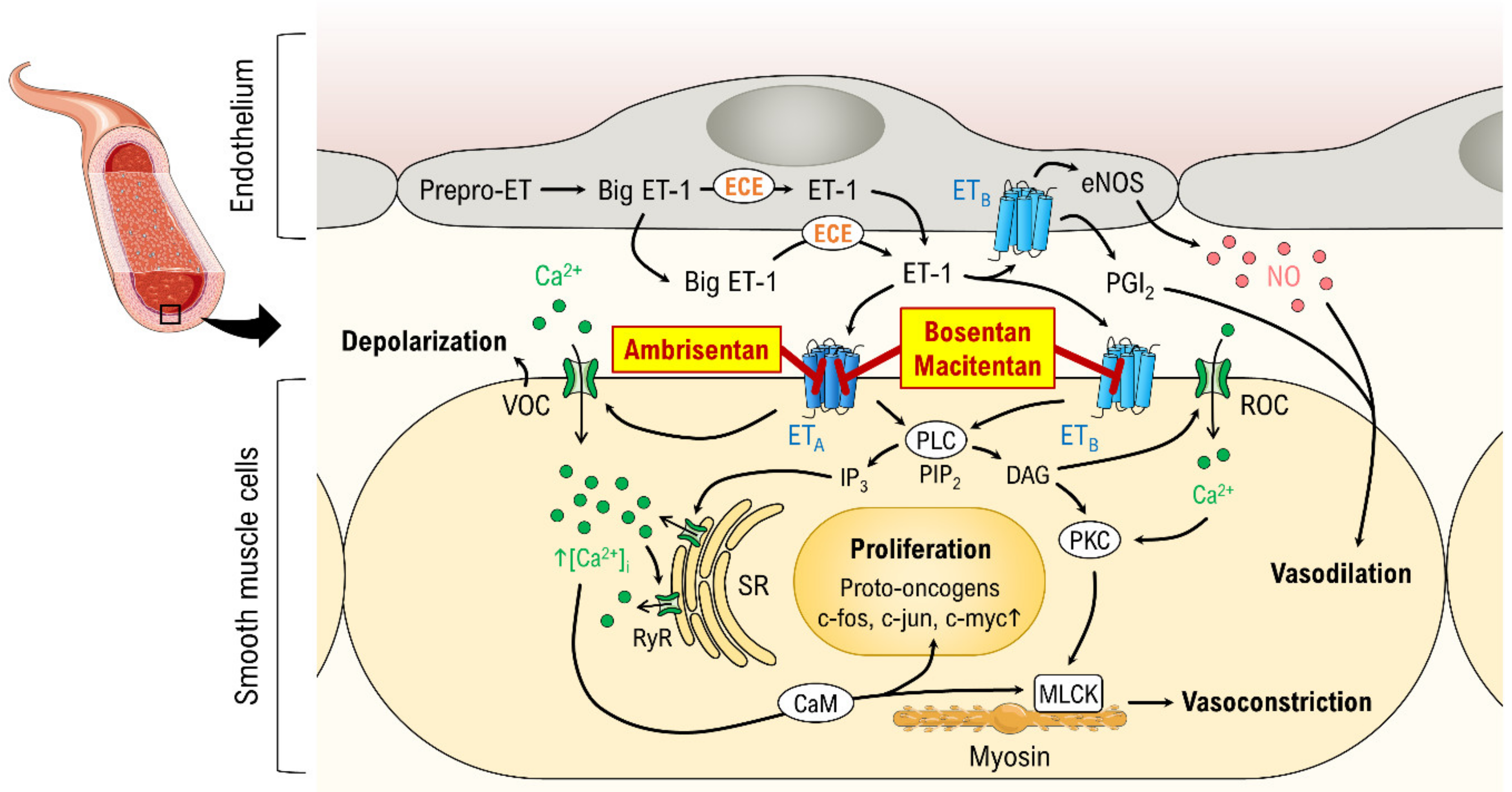
2. Endothelin and the Canonical Endothelin Pathway
3. Endothelin Receptor Antagonists (ERAs)
3.1. Pharmacodynamics
3.2. Pharmacokinetics
3.3. Interactions and Contraindications
3.4. Adverse Effects
4. Pulmonary Arterial Hypertension (PAH)
5. Cancer
6. Renal Disease
7. Fibrotic Diseases
8. Cerebral Vasospasm
9. Systemic Scleroderma
10. Pain Management
11. Conclusions
12. Outlook
Author Contributions
Funding
Conflicts of Interest
References
- Aubert, J.D.; Juillerat-Jeanneret, L. Endothelin-Receptor Antagonists beyond Pulmonary Arterial Hypertension: Cancer and Fibrosis. J. Med. Chem. 2016, 59, 8168–8188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macarthur, H.; Warner, T.D.; Wood, E.G.; Corder, R.; Vane, J.R. Endothelin-1 Release from Endothelial Cells in Culture Is Elevated Both Acutely and Chronically by Short Periods of Mechanical Stretch. Biochem. Biophys. Res. Commun. 1994, 200, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Malek, A.; Izumo, S. Physiological fluid shear stress causes downregulation of endothelin-1 mRNA in bovine aortic endothelium. Am. J. Physiol. Cell Physiol. 1992, 263, C389–C396. [Google Scholar] [CrossRef] [PubMed]
- Wesson, D.E.; Simoni, J.; Green, D.F. Reduced extracellular pH increases endothelin-1 secretion by human renal microvascular endothelial cells. J. Clin. Investig. 1998, 101, 578–583. [Google Scholar] [CrossRef]
- Matsuura, A.; Yamochi, W.; Hirata, K.; Kawashima, S.; Yokoyama, M. Stimulatory interaction between vascular endothelial growth factor and endothelin-1 on each gene expression. Hypertension 1998, 32, 89–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peifley, K.A.; Winkles, J.A. Angiotensin II and Endothelin-1 Increase Fibroblast Growth Factor-2 mRNA Expression in Vascular Smooth Muscle Cells. Biochem. Biophys. Res. Commun. 1998, 242, 202–208. [Google Scholar] [CrossRef]
- Aro, A.; Teirilä, J.; Gref, C.-G. Dose-dependent effect on serum cholesterol and apoprotein B concentrations by consumption of boiled, non-filtered coffee. Atherosclerosis 1990, 83, 257–261. [Google Scholar] [CrossRef]
- Yang, Z.; Krasnici, N.; Luscher, T.F. Endothelin-1 potentiates human smooth muscle cell growth to PDGF: Effects of ETA and ETB receptor blockade. Circulation 1999, 100, 5–8. [Google Scholar] [CrossRef] [Green Version]
- Davenport, A.P.; Hyndman, K.A.; Dhaun, N.; Southan, C.; Kohan, D.E.; Pollock, J.S.; Pollock, D.M.; Webb, D.J.; Maguire, J.J. Endothelin. Pharmacol. Rev. 2016, 68, 357–418. [Google Scholar] [CrossRef] [Green Version]
- Barton, M.; Yanagisawa, M. Endothelin: 30 Years From Discovery to Therapy. Hypertension 2019, 74, 1232–1265. [Google Scholar] [CrossRef]
- Shemyakin, A.; Salehzadeh, F.; Bohm, F.; Al-Khalili, L.; Gonon, A.; Wagner, H.; Efendic, S.; Krook, A.; Pernow, J. Regulation of glucose uptake by endothelin-1 in human skeletal muscle in vivo and in vitro. J. Clin. Endocrinol. Metab. 2010, 95, 2359–2366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohan, D.E.; Rossi, N.F.; Inscho, E.W.; Pollock, D.M. Regulation of blood pressure and salt homeostasis by endothelin. Physiol. Rev. 2011, 91, 1–77. [Google Scholar] [CrossRef] [PubMed]
- Houde, M.; Desbiens, L.; D’Orleans-Juste, P. Endothelin-1: Biosynthesis, Signaling and Vasoreactivity. Adv. Pharmacol. 2016, 77, 143–175. [Google Scholar] [CrossRef] [PubMed]
- Nasser, S.A.; El-Mas, M.M. Endothelin ETA receptor antagonism in cardiovascular disease. Eur. J. Pharmacol. 2014, 737, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Barst, R.J.; Langleben, D.; Frost, A.; Horn, E.M.; Oudiz, R.; Shapiro, S.; McLaughlin, V.; Hill, N.; Tapson, V.F.; Robbins, I.M.; et al. Sitaxsentan therapy for pulmonary arterial hypertension. Am. J. Respir. Crit. Care Med. 2004, 169, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Jimeno, A.; Carducci, M. Atrasentan: A novel and rationally designed therapeutic alternative in the management of cancer. Expert Rev. Anticancer Ther. 2005, 5, 419–427. [Google Scholar] [CrossRef]
- Van Giersbergen, P.L.; Dingemanse, J. Tolerability, pharmacokinetics, and pharmacodynamics of clazosentan, a parenteral endothelin receptor antagonist. Eur. J. Clin. Pharmacol. 2007, 63, 151–158. [Google Scholar] [CrossRef]
- Morris, C.D.; Rose, A.; Curwen, J.; Hughes, A.M.; Wilson, D.J.; Webb, D.J. Specific inhibition of the endothelin A receptor with ZD4054: Clinical and pre-clinical evidence. Br. J. Cancer 2005, 92, 2148–2152. [Google Scholar] [CrossRef] [Green Version]
- Tomkinson, H.; Kemp, J.; Oliver, S.; Swaisland, H.; Taboada, M.; Morris, T. Pharmacokinetics and tolerability of zibotentan (ZD4054) in subjects with hepatic or renal impairment: Two open-label comparative studies. BMC Clin. Pharmacol. 2011, 11, 3. [Google Scholar] [CrossRef] [Green Version]
- Dingemanse, J.; van Giersbergen, P.L. Clinical pharmacology of bosentan, a dual endothelin receptor antagonist. Clin. Pharmacokinet. 2004, 43, 1089–1115. [Google Scholar] [CrossRef]
- Buckley, M.S.; Wicks, L.M.; Staib, R.L.; Kirejczyk, A.K.; Varker, A.S.; Gibson, J.J.; Feldman, J.P. Pharmacokinetic evaluation of ambrisentan. Expert Opin. Drug Metab. Toxicol. 2011, 7, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Clozel, M.; Maresta, A.; Humbert, M. Endothelin receptor antagonists. Handb. Exp. Pharmacol. 2013, 218, 199–227. [Google Scholar] [CrossRef] [PubMed]
- Benedict, N.J. Sitaxsentan in the management of pulmonary arterial hypertension. Am. J. Health Syst. Pharm. 2007, 64, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Carducci, M.A.; Nelson, J.B.; Bowling, M.K.; Rogers, T.; Eisenberger, M.A.; Sinibaldi, V.; Donehower, R.; Leahy, T.L.; Carr, R.A.; Isaacson, J.D.; et al. Atrasentan, an endothelin-receptor antagonist for refractory adenocarcinomas: Safety and pharmacokinetics. J. Clin. Oncol. 2002, 20, 2171–2180. [Google Scholar] [CrossRef] [PubMed]
- Clarkson-Jones, J.A.; Kenyon, A.S.; Kemp, J.; Lenz, E.M.; Oliver, S.D.; Swaisland, H. Disposition and metabolism of the specific endothelin A receptor antagonist zibotentan (ZD4054) in healthy volunteers. Xenobiotica 2012, 42, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Sidharta, P.N.; Melchior, M.; Kankam, M.K.; Dingemanse, J. Single- and multiple-dose tolerability, safety, pharmacokinetics, and pharmacodynamics of the dual endothelin receptor antagonist aprocitentan in healthy adult and elderly subjects. Drug Des. Dev. Ther. 2019, 13, 949–964. [Google Scholar] [CrossRef] [Green Version]
- Weber, C.; Schmitt, R.; Birnboeck, H.; Hopfgartner, G.; van Marle, S.P.; Peeters, P.A.; Jonkman, J.H.; Jones, C.R. Pharmacokinetics and pharmacodynamics of the endothelin-receptor antagonist bosentan in healthy human subjects. Clin. Pharmacol. Ther. 1996, 60, 124–137. [Google Scholar] [CrossRef]
- Sidharta, P.N.; Krahenbuhl, S.; Dingemanse, J. Pharmacokinetic and pharmacodynamic evaluation of macitentan, a novel endothelin receptor antagonist for the treatment of pulmonary arterial hypertension. Expert Opin. Drug Metab. Toxicol. 2015, 11, 437–449. [Google Scholar] [CrossRef]
- Dhaun, N.; Melville, V.; Kramer, W.; Stavros, F.; Coyne, T.; Swan, S.; Goddard, J.; Webb, D.J. The pharmacokinetic profile of sitaxsentan, a selective endothelin receptor antagonist, in varying degrees of renal impairment. Br. J. Clin. Pharmacol. 2007, 64, 733–737. [Google Scholar] [CrossRef] [Green Version]
- Van Giersbergen, P.L.; Dingemanse, J. Effect of gender on the tolerability, safety and pharmacokinetics of clazosentan following long-term infusion. Clin. Drug Investig. 2007, 27, 797–802. [Google Scholar] [CrossRef]
- Ryan, C.W.; Vogelzang, N.J.; Vokes, E.E.; Kindler, H.L.; Undevia, S.D.; Humerickhouse, R.; Andre, A.K.; Wang, Q.; Carr, R.A.; Ratain, M.J. Dose-ranging study of the safety and pharmacokinetics of atrasentan in patients with refractory malignancies. Clin. Cancer Res. 2004, 10, 4406–4411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esvelt, M.A.; Freeman, Z.T.; Pearson, A.T.; Harkema, J.R.; Clines, G.T.; Clines, K.L.; Dyson, M.C.; Hoenerhoff, M.J. The Endothelin-A Receptor Antagonist Zibotentan Induces Damage to the Nasal Olfactory Epithelium Possibly Mediated in Part through Type 2 Innate Lymphoid Cells. Toxicol. Pathol. 2019, 47, 150–164. [Google Scholar] [CrossRef] [PubMed]
- Mathier, M.A.; Ishizawar, D. Bosentan. Expert Opin. Pharmacother. 2010, 11, 1023–1034. [Google Scholar] [CrossRef] [PubMed]
- Peacock, A.J.; Zamboni, W.; Vizza, C.D. Ambrisentan for the treatment of adults with pulmonary arterial hypertension: A review. Curr. Med. Res. Opin. 2015, 31, 1793–1807. [Google Scholar] [CrossRef] [PubMed]
- Chaumais, M.C.; Guignabert, C.; Savale, L.; Jais, X.; Boucly, A.; Montani, D.; Simonneau, G.; Humbert, M.; Sitbon, O. Clinical pharmacology of endothelin receptor antagonists used in the treatment of pulmonary arterial hypertension. Am. J. Cardiovasc. Drugs 2015, 15, 13–26. [Google Scholar] [CrossRef]
- Dingemanse, J.; Sidharta, P.N.; Maddrey, W.C.; Rubin, L.J.; Mickail, H. Efficacy, safety and clinical pharmacology of macitentan in comparison to other endothelin receptor antagonists in the treatment of pulmonary arterial hypertension. Expert Opin. Drug Saf. 2014, 13, 391–405. [Google Scholar] [CrossRef]
- Bedan, M.; Grimm, D.; Wehland, M.; Simonsen, U.; Infanger, M.; Krüger, M. A Focus on Macitentan in the Treatment of Pulmonary Arterial Hypertension. Basic Clin. Pharmacol. Toxicol. 2018, 123, 103–113. [Google Scholar] [CrossRef] [Green Version]
- Frampton, J.E. Ambrisentan. Am. J. Cardiovasc. Drugs 2011, 11, 215–226. [Google Scholar] [CrossRef]
- Croxtall, J.D.; Keam, S.J. Ambrisentan. Drugs 2008, 68, 2195–2204. [Google Scholar] [CrossRef]
- Venitz, J.; Zack, J.; Gillies, H.; Allard, M.; Regnault, J.; Dufton, C. Clinical pharmacokinetics and drug-drug interactions of endothelin receptor antagonists in pulmonary arterial hypertension. J. Clin. Pharmacol. 2012, 52, 1784–1805. [Google Scholar] [CrossRef]
- European Medicines Agency. Opsumit, INN-Macitentan, Annex. Available online: https://ec.europa.eu/health/documents/community-register/2013/20131220127396/anx_127396_en.pdf (accessed on 28 January 2020).
- Khadka, A.; Singh Brashier, D.B.; Tejus, A.; Sharma, A.K. Macitentan: An important addition to the treatment of pulmonary arterial hypertension. J. Pharmacol. Pharmacother. 2015, 6, 53–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oldfield, V.; Lyseng-Williamson, K.A. Bosentan: A review of its use in pulmonary arterial hypertension and systemic sclerosis. Am. J. Cardiovasc. Drugs 2006, 6, 189–208. [Google Scholar] [CrossRef] [PubMed]
- Benedict, N.; Seybert, A.; Mathier, M.A. Evidence-based pharmacologic management of pulmonary arterial hypertension. Clin. Ther. 2007, 29, 2134–2153. [Google Scholar] [CrossRef] [PubMed]
- Nagendran, J.; Sutendra, G.; Paterson, I.; Champion, H.C.; Webster, L.; Chiu, B.; Haromy, A.; Rebeyka, I.M.; Ross, D.B.; Michelakis, E.D.; et al. Endothelin axis is upregulated in human and rat right ventricular hypertrophy. Circ. Res. 2013, 112, 347–354. [Google Scholar] [CrossRef] [Green Version]
- Trow, T.K.; Taichman, D.B. Endothelin receptor blockade in the management of pulmonary arterial hypertension: Selective and dual antagonism. Respir. Med. 2009, 103, 951–962. [Google Scholar] [CrossRef] [Green Version]
- Dhillon, S.; Keating, G.M. Bosentan: A review of its use in the management of mildly symptomatic pulmonary arterial hypertension. Am. J. Cardiovasc. Drugs 2009, 9, 331–350. [Google Scholar] [CrossRef]
- Galie, N.; Hoeper, M.M.; Simon, J.; Gibbs, R.; Simonneau, G. Liver toxicity of sitaxentan in pulmonary arterial hypertension. Eur. Heart J. 2011, 32, 386–387. [Google Scholar] [CrossRef] [Green Version]
- Montani, D.; Gunther, S.; Dorfmuller, P.; Perros, F.; Girerd, B.; Garcia, G.; Jais, X.; Savale, L.; Artaud-Macari, E.; Price, L.C.; et al. Pulmonary arterial hypertension. Orphanet J. Rare Dis. 2013, 8, 97. [Google Scholar] [CrossRef] [Green Version]
- Lai, Y.C.; Potoka, K.C.; Champion, H.C.; Mora, A.L.; Gladwin, M.T. Pulmonary arterial hypertension: The clinical syndrome. Circ. Res. 2014, 115, 115–130. [Google Scholar] [CrossRef] [Green Version]
- MacIver, D.H.; Adeniran, I.; MacIver, I.R.; Revell, A.; Zhang, H. Physiological mechanisms of pulmonary hypertension. Am. Heart J. 2016, 180, 1–11. [Google Scholar] [CrossRef]
- Prins, K.W.; Thenappan, T. World Health Organization Group I Pulmonary Hypertension: Epidemiology and Pathophysiology. Cardiol. Clin. 2016, 34, 363–374. [Google Scholar] [CrossRef] [Green Version]
- Klinger, J.R.; Elliott, G.; Levine, D.J.; Bossone, E.; Duvall, L.; Fagan, K.; Frantsve-Hawley, J.; Kawut, S.M.; Ryan, J.J.; Rosenzweig, E.B.; et al. Therapy for Pulmonary Arterial Hypertension in Adults 2018: Update of the CHEST Guideline and Expert Panel Report. Chest 2019, 155, 565–586. [Google Scholar] [CrossRef]
- Rubin, L.J.; Badesch, D.B.; Barst, R.J.; Galie, N.; Black, C.M.; Keogh, A.; Pulido, T.; Frost, A.; Roux, S.; Leconte, I.; et al. Bosentan therapy for pulmonary arterial hypertension. N. Engl. J. Med. 2002, 346, 896–903. [Google Scholar] [CrossRef]
- Galie, N.; Olschewski, H.; Oudiz, R.J.; Torres, F.; Frost, A.; Ghofrani, H.A.; Badesch, D.B.; McGoon, M.D.; McLaughlin, V.V.; Roecker, E.B.; et al. Ambrisentan for the treatment of pulmonary arterial hypertension: Results of the ambrisentan in pulmonary arterial hypertension, randomized, double-blind, placebo-controlled, multicenter, efficacy (ARIES) study 1 and 2. Circulation 2008, 117, 3010–3019. [Google Scholar] [CrossRef] [PubMed]
- Pulido, T.; Adzerikho, I.; Channick, R.N.; Delcroix, M.; Galie, N.; Ghofrani, H.A.; Jansa, P.; Jing, Z.C.; Le Brun, F.O.; Mehta, S.; et al. Macitentan and morbidity and mortality in pulmonary arterial hypertension. N. Engl. J. Med. 2013, 369, 809–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duo-Ji, M.M.; Long, Z.W. Comparative efficacy and acceptability of endothelin receptor antagonists for pulmonary arterial hypertension: A network meta-analysis. Int. J. Cardiol. 2017, 234, 90–98. [Google Scholar] [CrossRef] [PubMed]
- D’Uscio, L.V.; Barton, M.; Shaw, S.; Moreau, P.; Luscher, T.F. Structure and function of small arteries in salt-induced hypertension: Effects of chronic endothelin-subtype-A-receptor blockade. Hypertension 1997, 30, 905–911. [Google Scholar] [CrossRef]
- Barton, M.; d’Uscio, L.V.; Shaw, S.; Meyer, P.; Moreau, P.; Luscher, T.F. ET(A) receptor blockade prevents increased tissue endothelin-1, vascular hypertrophy, and endothelial dysfunction in salt-sensitive hypertension. Hypertension 1998, 31, 499–504. [Google Scholar] [CrossRef] [Green Version]
- Bakris, G.L.; Lindholm, L.H.; Black, H.R.; Krum, H.; Linas, S.; Linseman, J.V.; Arterburn, S.; Sager, P.; Weber, M. Divergent results using clinic and ambulatory blood pressures: Report of a darusentan-resistant hypertension trial. Hypertension 2010, 56, 824–830. [Google Scholar] [CrossRef] [Green Version]
- Weber, M.A.; Black, H.; Bakris, G.; Krum, H.; Linas, S.; Weiss, R.; Linseman, J.V.; Wiens, B.L.; Warren, M.S.; Lindholm, L.H. A selective endothelin-receptor antagonist to reduce blood pressure in patients with treatment-resistant hypertension: A randomised, double-blind, placebo-controlled trial. Lancet 2009, 374, 1423–1431. [Google Scholar] [CrossRef]
- Black, H.R.; Bakris, G.L.; Weber, M.A.; Weiss, R.; Shahawy, M.E.; Marple, R.; Tannoury, G.; Linas, S.; Wiens, B.L.; Linseman, J.V.; et al. Efficacy and safety of darusentan in patients with resistant hypertension: Results from a randomized, double-blind, placebo-controlled dose-ranging study. J. Clin. Hypertens Greenwich 2007, 9, 760–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barton, M.; Haudenschild, C.C.; d’Uscio, L.V.; Shaw, S.; Munter, K.; Luscher, T.F. Endothelin ETA receptor blockade restores NO-mediated endothelial function and inhibits atherosclerosis in apolipoprotein E-deficient mice. Proc. Natl. Acad. Sci. USA 1998, 95, 14367–14372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saitoh, S.; Matsumoto, K.; Kamioka, M.; Ohkawara, H.; Kaneshiro, T.; Ishibashi, T.; Maruyama, Y. Novel pathway of endothelin-1 and reactive oxygen species in coronary vasospasm with endothelial dysfunction. Coron. Artery Dis. 2009, 20, 400–408. [Google Scholar] [CrossRef]
- Kusuhara, M.; Yamaguchi, K.; Nagasaki, K.; Hayashi, C.; Suzaki, A.; Hori, S.; Handa, S.; Nakamura, Y.; Abe, K. Production of endothelin in human cancer cell lines. Cancer Res. 1990, 50, 3257–3261. [Google Scholar] [PubMed]
- Peduto Eberl, L.; Bovey, R.; Juillerat-Jeanneret, L. Endothelin-receptor antagonists are proapoptotic and antiproliferative in human colon cancer cells. Br. J. Cancer 2003, 88, 788–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moody, T.W.; Ramos-Alvarez, I.; Moreno, P.; Mantey, S.A.; Ridnour, L.; Wink, D.; Jensen, R.T. Endothelin causes transactivation of the EGFR and HER2 in non-small cell lung cancer cells. Peptides 2017, 90, 90–99. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.; Dashwood, R.H. Endothelins and their receptors in cancer: Identification of therapeutic targets. Pharmacol. Res. 2011, 63, 519–524. [Google Scholar] [CrossRef] [Green Version]
- Bagnato, A.; Catt, K.J. Endothelins as autocrine regulators of tumor cell growth. Trends Endocrinol. Metab. 1998, 9, 378–383. [Google Scholar] [CrossRef]
- Harris, A.L. Hypoxia—A key regulatory factor in tumour growth. Nat. Rev. Cancer 2002, 2, 38–47. [Google Scholar] [CrossRef]
- Smollich, M.; Gotte, M.; Kersting, C.; Fischgrabe, J.; Kiesel, L.; Wulfing, P. Selective ETAR antagonist atrasentan inhibits hypoxia-induced breast cancer cell invasion. Breast Cancer Res. Treat. 2008, 108, 175–182. [Google Scholar] [CrossRef]
- Masoud, G.N.; Li, W. HIF-1α pathway: Role, regulation and intervention for cancer therapy. Acta Pharm. Sin. B 2015, 5, 378–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knowles, J.; Loizidou, M.; Taylor, I. Endothelin-1 and angiogenesis in cancer. Curr. Vasc. Pharmacol. 2005, 3, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Irani, S.; Salajegheh, A.; Smith, R.A.; Lam, A.K. A review of the profile of endothelin axis in cancer and its management. Crit. Rev. Oncol. Hematol. 2014, 89, 314–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knowles, J.P.; Shi-Wen, X.; Haque, S.U.; Bhalla, A.; Dashwood, M.R.; Yang, S.; Taylor, I.; Winslet, M.C.; Abraham, D.J.; Loizidou, M.; et al. Endothelin-1 stimulates colon cancer adjacent fibroblasts. Int. J. Cancer 2012, 130, 1264–1272. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.; Bagnato, A.; Battistini, B.; Nisen, P. The endothelin axis: Emerging role in cancer. Nat. Rev. Cancer 2003, 3, 110–116. [Google Scholar] [CrossRef]
- Rosano, L.; Cianfrocca, R.; Spinella, F.; Di Castro, V.; Nicotra, M.R.; Lucidi, A.; Ferrandina, G.; Natali, P.G.; Bagnato, A. Acquisition of chemoresistance and EMT phenotype is linked with activation of the endothelin A receptor pathway in ovarian carcinoma cells. Clin. Cancer Res. 2011, 17, 2350–2360. [Google Scholar] [CrossRef] [Green Version]
- Coffman, L.; Mooney, C.; Lim, J.; Bai, S.; Silva, I.; Gong, Y.; Yang, K.; Buckanovich, R.J. Endothelin receptor-A is required for the recruitment of antitumor T cells and modulates chemotherapy induction of cancer stem cells. Cancer Biol. Ther. 2013, 14, 184–192. [Google Scholar] [CrossRef] [Green Version]
- Haque, S.U.; Dashwood, M.R.; Heetun, M.; Shiwen, X.; Farooqui, N.; Ramesh, B.; Welch, H.; Savage, F.J.; Ogunbiyi, O.; Abraham, D.J.; et al. Efficacy of the specific endothelin a receptor antagonist zibotentan (ZD4054) in colorectal cancer: A preclinical study. Mol. Cancer Ther. 2013, 12, 1556–1567. [Google Scholar] [CrossRef] [Green Version]
- Said, N.; Smith, S.; Sanchez-Carbayo, M.; Theodorescu, D. Tumor endothelin-1 enhances metastatic colonization of the lung in mouse xenograft models of bladder cancer. J. Clin. Investig. 2011, 121, 132–147. [Google Scholar] [CrossRef] [Green Version]
- Eltze, E.; Wild, P.J.; Wulfing, C.; Zwarthoff, E.C.; Burger, M.; Stoehr, R.; Korsching, E.; Hartmann, A. Expression of the endothelin axis in noninvasive and superficially invasive bladder cancer: Relation to clinicopathologic and molecular prognostic parameters. Eur. Urol. 2009, 56, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Wulfing, P.; Diallo, R.; Kersting, C.; Wulfing, C.; Poremba, C.; Rody, A.; Greb, R.R.; Bocker, W.; Kiesel, L. Expression of endothelin-1, endothelin-A, and endothelin-B receptor in human breast cancer and correlation with long-term follow-up. Clin. Cancer Res. 2003, 9, 4125–4131. [Google Scholar] [PubMed]
- Wulfing, P.; Kersting, C.; Tio, J.; Fischer, R.J.; Wulfing, C.; Poremba, C.; Diallo, R.; Bocker, W.; Kiesel, L. Endothelin-1-, endothelin-A-, and endothelin-B-receptor expression is correlated with vascular endothelial growth factor expression and angiogenesis in breast cancer. Clin. Cancer Res. 2004, 10, 2393–2400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, D.J.; Liu, Y.; Lu, D.C.; Kim, W.; Lee, J.H.; Maynard, J.; Deisseroth, A. Endothelin-3 growth factor levels decreased in cervical cancer compared with normal cervical epithelial cells. Hum. Pathol. 2007, 38, 1047–1056. [Google Scholar] [CrossRef] [PubMed]
- Hoosein, M.M.; Dashwood, M.R.; Dawas, K.; Ali, H.M.; Grant, K.; Savage, F.; Taylor, I.; Loizidou, M. Altered endothelin receptor subtypes in colorectal cancer. Eur. J. Gastroenterol. Hepatol. 2007, 19, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Liakou, P.; Tepetes, K.; Germenis, A.; Leventaki, V.; Atsaves, V.; Patsouris, E.; Roidis, N.; Hatzitheophilou, K.; Rassidakis, G.Z. Expression patterns of endothelin-1 and its receptors in colorectal cancer. J. Surg. Oncol. 2012, 105, 643–649. [Google Scholar] [CrossRef]
- Fukui, R.; Nishimori, H.; Hata, F.; Yasoshima, T.; Ohno, K.; Yanai, Y.; Kamiguchi, K.; Denno, R.; Sato, N.; Hirata, K.; et al. Inhibitory effect of endothelin A receptor blockade on tumor growth and liver metastasis of a human gastric cancer cell line. Gastric Cancer 2007, 10, 123–128. [Google Scholar] [CrossRef]
- Tao, K.; Wu, C.; Wu, K.; Li, W.; Han, G.; Shuai, X.; Wang, G. Quantitative analysis of promoter methylation of the EDNRB gene in gastric cancer. Med. Oncol. 2012, 29, 107–112. [Google Scholar] [CrossRef]
- Egidy, G.; Eberl, L.P.; Valdenaire, O.; Irmler, M.; Majdi, R.; Diserens, A.C.; Fontana, A.; Janzer, R.C.; Pinet, F.; Juillerat-Jeanneret, L.; et al. The endothelin system in human glioblastoma. Lab. Investig. 2000, 80, 1681–1689. [Google Scholar] [CrossRef] [Green Version]
- Vasaikar, S.; Tsipras, G.; Landazuri, N.; Costa, H.; Wilhelmi, V.; Scicluna, P.; Cui, H.L.; Mohammad, A.A.; Davoudi, B.; Shang, M.; et al. Overexpression of endothelin B receptor in glioblastoma: A prognostic marker and therapeutic target? BMC Cancer 2018, 18, 154. [Google Scholar] [CrossRef]
- Anguelova, E.; Beuvon, F.; Leonard, N.; Chaverot, N.; Varlet, P.; Couraud, P.O.; Daumas-Duport, C.; Cazaubon, S. Functional endothelin ET B receptors are selectively expressed in human oligodendrogliomas. Brain Res. Mol. Brain Res. 2005, 137, 77–88. [Google Scholar] [CrossRef]
- Ishimoto, S.; Wada, K.; Tanaka, N.; Yamanishi, T.; Ishihama, K.; Aikawa, T.; Okura, M.; Nakajima, A.; Kogo, M.; Kamisaki, Y.; et al. Role of endothelin receptor signalling in squamous cell carcinoma. Int. J. Oncol. 2012, 40, 1011–1019. [Google Scholar] [CrossRef] [Green Version]
- Wen, Y.F.; Qi, B.; Liu, H.; Mo, H.Y.; Chen, Q.Y.; Li, J.; Huang, P.Y.; Ye, Y.F.; Zhang, Y.; Deng, M.Q.; et al. Polymorphisms in the endothelin-1 and endothelin a receptor genes and survival in patients with locoregionally advanced nasopharyngeal carcinoma. Clin. Cancer Res. 2011, 17, 2451–2458. [Google Scholar] [CrossRef] [Green Version]
- Cong, N.; Li, Z.; Shao, W.; Li, J.; Yu, S. Activation of ETA Receptor by Endothelin-1 Induces Hepatocellular Carcinoma Cell Migration and Invasion via ERK1/2 and AKT Signaling Pathways. J. Membr. Biol. 2016, 249, 119–128. [Google Scholar] [CrossRef]
- Hsu, L.S.; Lee, H.C.; Chau, G.Y.; Yin, P.H.; Chi, C.W.; Lui, W.Y. Aberrant methylation of EDNRB and p16 genes in hepatocellular carcinoma (HCC) in Taiwan. Oncol. Rep. 2006, 15, 507–511. [Google Scholar] [CrossRef] [Green Version]
- Boldrini, L.; Gisfredi, S.; Ursino, S.; Faviana, P.; Lucchi, M.; Melfi, F.; Mussi, A.; Basolo, F.; Fontanini, G. Expression of endothelin-1 is related to poor prognosis in non-small cell lung carcinoma. Eur. J. Cancer 2005, 41, 2828–2835. [Google Scholar] [CrossRef]
- Blouquit-Laye, S.; Regnier, A.; Beauchet, A.; Zimmermann, U.; Devillier, P.; Chinet, T. Expression of endothelin receptor subtypes in bronchial tumors. Oncol. Rep. 2010, 23, 457–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demunter, A.; De Wolf-Peeters, C.; Degreef, H.; Stas, M.; van den Oord, J.J. Expression of the endothelin-B receptor in pigment cell lesions of the skin. Evidence for its role as tumor progression marker in malignant melanoma. Virchows Arch. 2001, 438, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.L.; Damato, B.E.; Scholes, A.G.; Nunn, J.; Field, J.K.; Heighway, J. Decreased endothelin receptor B expression in large primary uveal melanomas is associated with early clinical metastasis and short survival. Br. J. Cancer 2002, 87, 1308–1313. [Google Scholar] [CrossRef] [Green Version]
- Bagnato, A.; Salani, D.; Di Castro, V.; Wu-Wong, J.R.; Tecce, R.; Nicotra, M.R.; Venuti, A.; Natali, P.G. Expression of endothelin 1 and endothelin A receptor in ovarian carcinoma: Evidence for an autocrine role in tumor growth. Cancer Res. 1999, 59, 720–727. [Google Scholar] [PubMed]
- Rosano, L.; Spinella, F.; Di Castro, V.; Nicotra, M.R.; Dedhar, S.; de Herreros, A.G.; Natali, P.G.; Bagnato, A. Endothelin-1 promotes epithelial-to-mesenchymal transition in human ovarian cancer cells. Cancer Res. 2005, 65, 11649–11657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, N.; Brais, R.; Qian, W.; Hak, C.C.; Corrie, P.G. Endothelin-1 and endothelin B receptor expression in pancreatic adenocarcinoma. J. Clin. Pathol. 2015, 68, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Prajapati, A.; Gulati, M.; Gautam, S.K.; Kumar, S.; Dalal, V.; Talmon, G.A.; Rachagani, S.; Jain, M. Irreversible and sustained upregulation of endothelin axis during oncogene-associated pancreatic inflammation and cancer. Neoplasia 2020, 22, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, S.; Stummeyer, T.; Hotz, B.; Hines, O.J.; Reber, H.A.; Buhr, H.J.; Hotz, H.G. Selective inhibition of endothelin receptor A as an anti-angiogenic and anti-proliferative strategy for human pancreatic cancer. J. Gastrointest. Surg. 2005, 9, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Godara, G.; Pecher, S.; Jukic, D.M.; D’Antonio, J.M.; Akhavan, A.; Nelson, J.B.; Pflug, B.R. Distinct patterns of endothelin axis expression in primary prostate cancer. Urology 2007, 70, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.B.; Hedican, S.P.; George, D.J.; Reddi, A.H.; Piantadosi, S.; Eisenberger, M.A.; Simons, J.W. Identification of endothelin-1 in the pathophysiology of metastatic adenocarcinoma of the prostate. Nat. Med. 1995, 1, 944–949. [Google Scholar] [CrossRef]
- Herrmann, E.; Eltze, E.; Bierer, S.; Bogemann, M.; Brinkmann, O.A.; Balnowair, H.; Hertle, L.; Wulfing, C. Expression of the Endothelin-axis in the different histologic subtypes of renal cell carcinoma: A tissue microarray analysis. Oncol. Rep. 2007, 17, 275–280. [Google Scholar] [CrossRef] [Green Version]
- Douglas, M.L.; Richardson, M.M.; Nicol, D.L. Endothelin axis expression is markedly different in the two main subtypes of renal cell carcinoma. Cancer 2004, 100, 2118–2124. [Google Scholar] [CrossRef]
- Wuttig, D.; Zastrow, S.; Fussel, S.; Toma, M.I.; Meinhardt, M.; Kalman, K.; Junker, K.; Sanjmyatav, J.; Boll, K.; Hackermuller, J.; et al. CD31, EDNRB and TSPAN7 are promising prognostic markers in clear-cell renal cell carcinoma revealed by genome-wide expression analyses of primary tumors and metastases. Int. J. Cancer 2012, 131, E693–E704. [Google Scholar] [CrossRef]
- Yao, M.; Huang, Y.; Shioi, K.; Hattori, K.; Murakami, T.; Sano, F.; Baba, M.; Kondo, K.; Nakaigawa, N.; Kishida, T.; et al. A three-gene expression signature model to predict clinical outcome of clear cell renal carcinoma. Int. J. Cancer 2008, 123, 1126–1132. [Google Scholar] [CrossRef]
- Irani, S.; Salajegheh, A.; Gopalan, V.; Smith, R.A.; Lam, A.K. Expression profile of endothelin 1 and its receptor endothelin receptor A in papillary thyroid carcinoma and their correlations with clinicopathologic characteristics. Ann. Diagn. Pathol. 2014, 18, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Eltze, E.; Bertolin, M.; Korsching, E.; Wulfing, P.; Maggino, T.; Lelle, R. Expression and prognostic relevance of endothelin-B receptor in vulvar cancer. Oncol. Rep. 2007, 18, 305–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Askoxylakis, V.; Ferraro, G.B.; Badeaux, M.; Kodack, D.P.; Kirst, I.; Shankaraiah, R.C.; Wong, C.S.F.; Duda, D.G.; Fukumura, D.; Jain, R.K. Dual endothelin receptor inhibition enhances T-DM1 efficacy in brain metastases from HER2-positive breast cancer. NPJ Breast Cancer 2019, 5, 4. [Google Scholar] [CrossRef]
- Kim, S.J.; Kim, J.S.; Kim, S.W.; Brantley, E.; Yun, S.J.; He, J.; Maya, M.; Zhang, F.; Wu, Q.; Lehembre, F.; et al. Macitentan (ACT-064992), a tissue-targeting endothelin receptor antagonist, enhances therapeutic efficacy of paclitaxel by modulating survival pathways in orthotopic models of metastatic human ovarian cancer. Neoplasia 2011, 13, 167–179. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.J.; Hanibuchi, M.; Kim, S.J.; Yu, H.; Kim, M.S.; He, J.; Langley, R.R.; Lehembre, F.; Regenass, U.; Fidler, I.J. Treatment of experimental human breast cancer and lung cancer brain metastases in mice by macitentan, a dual antagonist of endothelin receptors, combined with paclitaxel. Neuro Oncol. 2016, 18, 486–496. [Google Scholar] [CrossRef] [PubMed]
- Cianfrocca, R.; Rosano, L.; Tocci, P.; Sestito, R.; Caprara, V.; Di Castro, V.; De Maria, R.; Bagnato, A. Blocking endothelin-1-receptor/beta-catenin circuit sensitizes to chemotherapy in colorectal cancer. Cell Death Differ. 2017, 24, 1811–1820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goda, K.; Bacso, Z.; Szabo, G. Multidrug resistance through the spectacle of P-glycoprotein. Curr. Cancer Drug Targets 2009, 9, 281–297. [Google Scholar] [CrossRef] [PubMed]
- Bradley, G.; Ling, V. P-glycoprotein, multidrug resistance and tumor progression. Cancer Metastasis Rev. 1994, 13, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Hartz, A.M.; Bauer, B.; Fricker, G.; Miller, D.S. Rapid regulation of P-glycoprotein at the blood-brain barrier by endothelin-1. Mol. Pharmacol. 2004, 66, 387–394. [Google Scholar] [CrossRef] [Green Version]
- Yang, K.M.; Russell, J.; Lupu, M.E.; Cho, H.; Li, X.-F.; Koutcher, J.A.; Ling, C.C. Atrasentan (ABT-627) enhances perfusion and reduces hypoxia in a human tumor xenograft model. Cancer Biol. Ther. 2009, 8, 1940–1946. [Google Scholar] [CrossRef] [Green Version]
- Lalich, M.; McNeel, D.G.; Wilding, G.; Liu, G. Endothelin receptor antagonists in cancer therapy. Cancer Investig. 2007, 25, 785–794. [Google Scholar] [CrossRef]
- Nelson, J.B.; Fizazi, K.; Miller, K.; Higano, C.; Moul, J.W.; Akaza, H.; Morris, T.; McIntosh, S.; Pemberton, K.; Gleave, M. Phase 3, randomized, placebo-controlled study of zibotentan (ZD4054) in patients with castration-resistant prostate cancer metastatic to bone. Cancer 2012, 118, 5709–5718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, P.; Chen, M.; Zhang, L.X.; Song, R.X.; He, Z.H.; Wang, Z.P. A Meta-Analysis and Indirect Comparison of Endothelin A Receptor Antagonist for Castration-Resistant Prostate Cancer. PLoS ONE 2015, 10, e0133803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosano, L.; Bagnato, A. Endothelin therapeutics in cancer: Where are we? Am. J. Physiol. Regul. Integr. Comp. Physiol. 2016, 310, R469–R475. [Google Scholar] [CrossRef] [Green Version]
- Miller, K.; Moul, J.W.; Gleave, M.; Fizazi, K.; Nelson, J.B.; Morris, T.; Nathan, F.E.; McIntosh, S.; Pemberton, K.; Higano, C.S. Phase III, randomized, placebo-controlled study of once-daily oral zibotentan (ZD4054) in patients with non-metastatic castration-resistant prostate cancer. Prostate Cancer Prostatic Dis. 2013, 16, 187–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fizazi, K.; Higano, C.S.; Nelson, J.B.; Gleave, M.; Miller, K.; Morris, T.; Nathan, F.E.; McIntosh, S.; Pemberton, K.; Moul, J.W. Phase III, randomized, placebo-controlled study of docetaxel in combination with zibotentan in patients with metastatic castration-resistant prostate cancer. J. Clin. Oncol. 2013, 31, 1740–1747. [Google Scholar] [CrossRef] [PubMed]
- Chouaid, C.; Nathan, F.; Pemberton, K.; Morris, T. A phase II, randomized, multicenter study to assess the efficacy, safety, and tolerability of zibotentan (ZD4054) in combination with pemetrexed in patients with advanced non-small cell lung cancer. Cancer Chemother. Pharmacol. 2011, 67, 1203–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, J.B.; Love, W.; Chin, J.L.; Saad, F.; Schulman, C.C.; Sleep, D.J.; Qian, J.; Steinberg, J.; Carducci, M. Phase 3, randomized, controlled trial of atrasentan in patients with nonmetastatic, hormone-refractory prostate cancer. Cancer 2008, 113, 2478–2487. [Google Scholar] [CrossRef]
- Carducci, M.A.; Saad, F.; Abrahamsson, P.A.; Dearnaley, D.P.; Schulman, C.C.; North, S.A.; Sleep, D.J.; Isaacson, J.D.; Nelson, J.B. A phase 3 randomized controlled trial of the efficacy and safety of atrasentan in men with metastatic hormone-refractory prostate cancer. Cancer 2007, 110, 1959–1966. [Google Scholar] [CrossRef]
- Quinn, D.I.; Tangen, C.M.; Hussain, M.; Lara, P.N., Jr.; Goldkorn, A.; Moinpour, C.M.; Garzotto, M.G.; Mack, P.C.; Carducci, M.A.; Monk, J.P.; et al. Docetaxel and atrasentan versus docetaxel and placebo for men with advanced castration-resistant prostate cancer (SWOG S0421): A randomised phase 3 trial. Lancet Oncol. 2013, 14, 893–900. [Google Scholar] [CrossRef] [Green Version]
- Lara, P.N., Jr.; Ely, B.; Quinn, D.I.; Mack, P.C.; Tangen, C.; Gertz, E.; Twardowski, P.W.; Goldkorn, A.; Hussain, M.; Vogelzang, N.J.; et al. Serum biomarkers of bone metabolism in castration-resistant prostate cancer patients with skeletal metastases: Results from SWOG 0421. J. Natl. Cancer Inst. 2014, 106, dju013. [Google Scholar] [CrossRef]
- Goldkorn, A.; Ely, B.; Quinn, D.I.; Tangen, C.M.; Fink, L.M.; Xu, T.; Twardowski, P.; Van Veldhuizen, P.J.; Agarwal, N.; Carducci, M.A.; et al. Circulating tumor cell counts are prognostic of overall survival in SWOG S0421: A phase III trial of docetaxel with or without atrasentan for metastatic castration-resistant prostate cancer. J. Clin. Oncol. 2014, 32, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Carducci, M.A.; Manola, J.; Nair, S.G.; Liu, G.; Rousey, S.; Dutcher, J.P.; Wilding, G. Atrasentan in Patients With Advanced Renal Cell Carcinoma: A Phase 2 Trial of the ECOG-ACRIN Cancer Research Group (E6800). Clin. Genitourin. Cancer 2015, 13, 531–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, R.; Chiorean, E.G.; Amin, M.; Rocha-Lima, C.M.S.; Gandhi, J.; Harris, W.P.; Song, T.; Portnoy, D. Phase 2 study of combination SPI-1620 with docetaxel as second-line advanced biliary tract cancer treatment. Br. J. Cancer 2017, 117, 189–194. [Google Scholar] [CrossRef] [Green Version]
- Kefford, R.; Beith, J.M.; Van Hazel, G.A.; Millward, M.; Trotter, J.M.; Wyld, D.K.; Kusic, R.; Shreeniwas, R.; Morganti, A.; Ballmer, A.; et al. A phase II study of bosentan, a dual endothelin receptor antagonist, as monotherapy in patients with stage IV metastatic melanoma. Investig. New Drugs 2007, 25, 247–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kefford, R.F.; Clingan, P.R.; Brady, B.; Ballmer, A.; Morganti, A.; Hersey, P. A randomized, double-blind, placebo-controlled study of high-dose bosentan in patients with stage IV metastatic melanoma receiving first-line dacarbazine chemotherapy. Mol. Cancer 2010, 9, 69. [Google Scholar] [CrossRef] [Green Version]
- De Jong, M.; Maina, T. Of mice and humans: Are they the same? Implications in cancer translational research. J. Nucl. Med. 2010, 51, 501–504. [Google Scholar] [CrossRef] [Green Version]
- Pollock, J.S.; Pollock, D.M. SONAR propels endothelin A receptor antagonists to success. Nat. Rev. Nephrol. 2019, 15, 461–462. [Google Scholar] [CrossRef]
- Kohan, D.E.; Barton, M. Endothelin and endothelin antagonists in chronic kidney disease. Kidney Int. 2014, 86, 896–904. [Google Scholar] [CrossRef] [Green Version]
- Mann, J.F.; Green, D.; Jamerson, K.; Ruilope, L.M.; Kuranoff, S.J.; Littke, T.; Viberti, G. Avosentan for overt diabetic nephropathy. J. Am. Soc. Nephrol. 2010, 21, 527–535. [Google Scholar] [CrossRef] [Green Version]
- Kohan, D.E.; Pritchett, Y.; Molitch, M.; Wen, S.; Garimella, T.; Audhya, P.; Andress, D.L. Addition of atrasentan to renin-angiotensin system blockade reduces albuminuria in diabetic nephropathy. J. Am. Soc. Nephrol. 2011, 22, 763–772. [Google Scholar] [CrossRef] [Green Version]
- Heerspink, H.J.L.; Parving, H.H.; Andress, D.L.; Bakris, G.; Correa-Rotter, R.; Hou, F.F.; Kitzman, D.W.; Kohan, D.; Makino, H.; McMurray, J.J.V.; et al. Atrasentan and renal events in patients with type 2 diabetes and chronic kidney disease (SONAR): A double-blind, randomised, placebo-controlled trial. Lancet 2019, 393, 1937–1947. [Google Scholar] [CrossRef]
- Dhaun, N.; MacIntyre, I.M.; Kerr, D.; Melville, V.; Johnston, N.R.; Haughie, S.; Goddard, J.; Webb, D.J. Selective endothelin-A receptor antagonism reduces proteinuria, blood pressure, and arterial stiffness in chronic proteinuric kidney disease. Hypertension 2011, 57, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Trachtman, H.; Nelson, P.; Adler, S.; Campbell, K.N.; Chaudhuri, A.; Derebail, V.K.; Gambaro, G.; Gesualdo, L.; Gipson, D.S.; Hogan, J.; et al. DUET: A Phase 2 Study Evaluating the Efficacy and Safety of Sparsentan in Patients with FSGS. J. Am. Soc. Nephrol. 2018, 29, 2745–2754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhaun, N.; Melville, V.; Blackwell, S.; Talwar, D.K.; Johnston, N.R.; Goddard, J.; Webb, D.J. Endothelin-A receptor antagonism modifies cardiovascular risk factors in CKD. J. Am. Soc. Nephrol. 2013, 24, 31–36. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.-W.; Mostafa, N.M.; Andress, D.L.; Brennan, J.J.; Klein, C.E.; Awni, W.M. Relationship Between Atrasentan Concentrations and Urinary Albumin to Creatinine Ratio in Western and Japanese Patients With Diabetic Nephropathy. Clin. Ther. 2018, 40, 242–251. [Google Scholar] [CrossRef]
- De Zeeuw, D.; Coll, B.; Andress, D.; Brennan, J.J.; Tang, H.; Houser, M.; Correa-Rotter, R.; Kohan, D.; Lambers Heerspink, H.J.; Makino, H.; et al. The endothelin antagonist atrasentan lowers residual albuminuria in patients with type 2 diabetic nephropathy. J. Am. Soc. Nephrol. 2014, 25, 1083–1093. [Google Scholar] [CrossRef] [Green Version]
- Kohan, D.E.; Lambers Heerspink, H.J.; Coll, B.; Andress, D.; Brennan, J.J.; Kitzman, D.W.; Correa-Rotter, R.; Makino, H.; Perkovic, V.; Hou, F.F.; et al. Predictors of Atrasentan-Associated Fluid Retention and Change in Albuminuria in Patients with Diabetic Nephropathy. Clin. J. Am. Soc. Nephrol. 2015, 10, 1568–1574. [Google Scholar] [CrossRef]
- Perez-Gomez, M.V.; Sanchez-Nino, M.D.; Sanz, A.B.; Martin-Cleary, C.; Ruiz-Ortega, M.; Egido, J.; Navarro-Gonzalez, J.F.; Ortiz, A.; Fernandez-Fernandez, B. Horizon 2020 in Diabetic Kidney Disease: The Clinical Trial Pipeline for Add-On Therapies on Top of Renin Angiotensin System Blockade. J. Clin. Med. 2015, 4, 1325–1347. [Google Scholar] [CrossRef] [Green Version]
- King, T.E., Jr.; Brown, K.K.; Raghu, G.; du Bois, R.M.; Lynch, D.A.; Martinez, F.; Valeyre, D.; Leconte, I.; Morganti, A.; Roux, S.; et al. BUILD-3: A randomized, controlled trial of bosentan in idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 2011, 184, 92–99. [Google Scholar] [CrossRef]
- King, T.E., Jr.; Behr, J.; Brown, K.K.; du Bois, R.M.; Lancaster, L.; de Andrade, J.A.; Stahler, G.; Leconte, I.; Roux, S.; Raghu, G. BUILD-1: A randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 2008, 177, 75–81. [Google Scholar] [CrossRef]
- Raghu, G.; Behr, J.; Brown, K.K.; Egan, J.J.; Kawut, S.M.; Flaherty, K.R.; Martinez, F.J.; Nathan, S.D.; Wells, A.U.; Collard, H.R.; et al. Treatment of idiopathic pulmonary fibrosis with ambrisentan: A parallel, randomized trial. Ann. Intern. Med. 2013, 158, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Million-Rousseau, R.; Morganti, A.; Perchenet, L.; Behr, J. Macitentan for the treatment of idiopathic pulmonary fibrosis: The randomised controlled MUSIC trial. Eur. Respir. J. 2013, 42, 1622–1632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macdonald, R.L.; Kassell, N.F.; Mayer, S.; Ruefenacht, D.; Schmiedek, P.; Weidauer, S.; Frey, A.; Roux, S.; Pasqualin, A. Clazosentan to overcome neurological ischemia and infarction occurring after subarachnoid hemorrhage (CONSCIOUS-1): Randomized, double-blind, placebo-controlled phase 2 dose-finding trial. Stroke 2008, 39, 3015–3021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macdonald, R.L.; Higashida, R.T.; Keller, E.; Mayer, S.A.; Molyneux, A.; Raabe, A.; Vajkoczy, P.; Wanke, I.; Bach, D.; Frey, A.; et al. Clazosentan, an endothelin receptor antagonist, in patients with aneurysmal subarachnoid haemorrhage undergoing surgical clipping: A randomised, double-blind, placebo-controlled phase 3 trial (CONSCIOUS-2). Lancet Neurol. 2011, 10, 618–625. [Google Scholar] [CrossRef]
- Macdonald, R.L.; Higashida, R.T.; Keller, E.; Mayer, S.A.; Molyneux, A.; Raabe, A.; Vajkoczy, P.; Wanke, I.; Bach, D.; Frey, A.; et al. Randomized trial of clazosentan in patients with aneurysmal subarachnoid hemorrhage undergoing endovascular coiling. Stroke 2012, 43, 1463–1469. [Google Scholar] [CrossRef] [Green Version]
- Khanna, D.; Denton, C.P.; Merkel, P.A.; Krieg, T.; Le Brun, F.O.; Marr, A.; Papadakis, K.; Pope, J.; Matucci-Cerinic, M.; Furst, D.E. Effect of Macitentan on the Development of New Ischemic Digital Ulcers in Patients With Systemic Sclerosis: DUAL-1 and DUAL-2 Randomized Clinical Trials. JAMA 2016, 315, 1975–1988. [Google Scholar] [CrossRef]
- Korn, J.H.; Mayes, M.; Matucci Cerinic, M.; Rainisio, M.; Pope, J.; Hachulla, E.; Rich, E.; Carpentier, P.; Molitor, J.; Seibold, J.R.; et al. Digital ulcers in systemic sclerosis: Prevention by treatment with bosentan, an oral endothelin receptor antagonist. Arthritis Rheum. 2004, 50, 3985–3993. [Google Scholar] [CrossRef]
- Matucci-Cerinic, M.; Denton, C.P.; Furst, D.E.; Mayes, M.D.; Hsu, V.M.; Carpentier, P.; Wigley, F.M.; Black, C.M.; Fessler, B.J.; Merkel, P.A.; et al. Bosentan treatment of digital ulcers related to systemic sclerosis: Results from the RAPIDS-2 randomised, double-blind, placebo-controlled trial. Ann. Rheum. Dis. 2011, 70, 32–38. [Google Scholar] [CrossRef]
- Rezus, E.; Burlui, A.M.; Gafton, B.; Stratulat, T.A.; Zota, G.R.; Cardoneanu, A.; Rezus, C. A patient-centered approach to the burden of symptoms in patients with scleroderma treated with Bosentan: A prospective single-center observational study. Exp. Ther. Med. 2020, 19, 1739–1746. [Google Scholar] [CrossRef] [Green Version]
- Farrah, T.E.; Anand, A.; Gallacher, P.J.; Kimmitt, R.; Carter, E.; Dear, J.W.; Mills, N.L.; Webb, D.J.; Dhaun, N. Endothelin Receptor Antagonism Improves Lipid Profiles and Lowers PCSK9 (Proprotein Convertase Subtilisin/Kexin Type 9) in Patients With Chronic Kidney Disease. Hypertension 2019, 74, 323–330. [Google Scholar] [CrossRef]
- Phelan, M.; Perrine, S.P.; Brauer, M.; Faller, D.V. Sickle erythrocytes, after sickling, regulate the expression of the endothelin-1 gene and protein in human endothelial cells in culture. J. Clin. Investig. 1995, 96, 1145–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tharaux, P.-L.; Hagège, I.; Placier, S.; Vayssairat, M.; Kanfer, A.; Girot, R.; Dussaule, J.-C. Urinary endothelin-1 as a marker of renal damage in sickle cell disease. Nephrol. Dial. Transplant. 2005, 20, 2408–2413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabaa, N.; de Franceschi, L.; Bonnin, P.; Castier, Y.; Malpeli, G.; Debbabi, H.; Galaup, A.; Maier-Redelsperger, M.; Vandermeersch, S.; Scarpa, A.; et al. Endothelin receptor antagonism prevents hypoxia-induced mortality and morbidity in a mouse model of sickle-cell disease. J. Clin. Investig. 2008, 118, 1924–1933. [Google Scholar] [CrossRef] [Green Version]
- Kasztan, M.; Fox, B.M.; Speed, J.S.; De Miguel, C.; Gohar, E.Y.; Townes, T.M.; Kutlar, A.; Pollock, J.S.; Pollock, D.M. Long-Term Endothelin-A Receptor Antagonism Provides Robust Renal Protection in Humanized Sickle Cell Disease Mice. J. Am. Soc. Nephrol. 2017, 28, 2443–2458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wynn, T.A. Cellular and molecular mechanisms of fibrosis. J. Pathol. 2008, 214, 199–210. [Google Scholar] [CrossRef] [Green Version]
- Katwa, L.C.; Guarda, E.; Weber, K.T. Endothelin receptors in cultured adult rat cardiac fibroblasts. Cardiovasc. Res. 1993, 27, 2125–2129. [Google Scholar] [CrossRef]
- Clozel, M.; Salloukh, H. Role of endothelin in fibrosis and anti-fibrotic potential of bosentan. Ann. Med. 2005, 37, 2–12. [Google Scholar] [CrossRef]
- Poncet, S.; Meyer, S.; Richard, C.; Aubert, J.D.; Juillerat-Jeanneret, L. The expression and function of the endothelin system in contractile properties of vaginal myofibroblasts of women with uterovaginal prolapse. Am. J. Obstet. Gynecol. 2005, 192, 426–432. [Google Scholar] [CrossRef]
- Xu, S.; Denton, C.P.; Holmes, A.; Dashwood, M.R.; Abraham, D.J.; Black, C.M. Endothelins: Effect on matrix biosynthesis and proliferation in normal and scleroderma fibroblasts. J. Cardiovasc. Pharmacol. 1998, 31 (Suppl. 1), S360–S363. [Google Scholar] [CrossRef]
- Rizvi, M.A.; Katwa, L.; Spadone, D.P.; Myers, P.R. The effects of endothelin-1 on collagen type I and type III synthesis in cultured porcine coronary artery vascular smooth muscle cells. J. Mol. Cell Cardiol. 1996, 28, 243–252. [Google Scholar] [CrossRef]
- Marini, M.; Carpi, S.; Bellini, A.; Patalano, F.; Mattoli, S. Endothelin-1 induces increased fibronectin expression in human bronchial epithelial cells. Biochem. Biophys. Res. Commun. 1996, 220, 896–899. [Google Scholar] [CrossRef] [PubMed]
- Shi-Wen, X.; Denton, C.P.; Dashwood, M.R.; Holmes, A.M.; Bou-Gharios, G.; Pearson, J.D.; Black, C.M.; Abraham, D.J. Fibroblast matrix gene expression and connective tissue remodeling: Role of endothelin-1. J. Investig. Dermatol. 2001, 116, 417–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, S.W.; Howat, S.L.; Renzoni, E.A.; Holmes, A.; Pearson, J.D.; Dashwood, M.R.; Bou-Gharios, G.; Denton, C.P.; du Bois, R.M.; Black, C.M.; et al. Endothelin-1 induces expression of matrix-associated genes in lung fibroblasts through MEK/ERK. J. Biol. Chem. 2004, 279, 23098–23103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, H.Q.; Weymouth, N.D.; Rockey, D.C. Endothelin antagonism in portal hypertensive mice: Implications for endothelin receptor-specific signaling in liver disease. Am. J. Physiol. Gastrointest. Liver Physiol. 2009, 297, G27–G33. [Google Scholar] [CrossRef] [Green Version]
- Rockey, D.C.; Chung, J.J. Endothelin antagonism in experimental hepatic fibrosis. Implications for endothelin in the pathogenesis of wound healing. J. Clin. Investig. 1996, 98, 1381–1388. [Google Scholar] [CrossRef]
- Antoniu, S.A. Targeting the endothelin pathway in the idiopathic pulmonary fibrosis: The role of bosentan. Expert Opin. Ther. Targets 2008, 12, 1077–1084. [Google Scholar] [CrossRef]
- Weng, C.M.; Yu, C.C.; Kuo, M.L.; Chen, B.C.; Lin, C.H. Endothelin-1 induces connective tissue growth factor expression in human lung fibroblasts by ETAR-dependent JNK/AP-1 pathway. Biochem. Pharmacol. 2014, 88, 402–411. [Google Scholar] [CrossRef]
- Wind, S.; Schmid, U.; Freiwald, M.; Marzin, K.; Lotz, R.; Ebner, T.; Stopfer, P.; Dallinger, C. Clinical Pharmacokinetics and Pharmacodynamics of Nintedanib. Clin. Pharmacokinet. 2019, 58, 1131–1147. [Google Scholar] [CrossRef] [Green Version]
- Park, S.H.; Saleh, D.; Giaid, A.; Michel, R.P. Increased endothelin-1 in bleomycin-induced pulmonary fibrosis and the effect of an endothelin receptor antagonist. Am. J. Respir. Crit. Care Med. 1997, 156, 600–608. [Google Scholar] [CrossRef]
- King, T.E., Jr. Bosentan for idiopathic pulmonary fibrosis. Curr. Opin. Investig. Drugs 2008, 9, 1171–1179. [Google Scholar]
- Zimmermann, M.; Seifert, V. Endothelin and subarachnoid hemorrhage: An overview. Neurosurgery 1998, 43, 863–875. [Google Scholar] [CrossRef] [PubMed]
- Chow, M.; Dumont, A.S.; Kassell, N.F. Endothelin receptor antagonists and cerebral vasospasm: An update. Neurosurgery 2002, 51, 1333–1341. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, R.L. Clazosentan: An endothelin receptor antagonist for treatment of vasospasm after subarachnoid hemorrhage. Expert Opin. Investig. Drugs 2008, 17, 1761–1767. [Google Scholar] [CrossRef] [PubMed]
- Armstead, W.M. Endothelins and the role of endothelin antagonists in the management of posttraumatic vasospasm. Curr. Pharm. Des. 2004, 10, 2185–2192. [Google Scholar] [CrossRef] [PubMed]
- Mayer Stephan, A.; Aldrich, E.F.; Bruder, N.; Hmissi, A.; Macdonald, R.L.; Viarasilpa, T.; Marr, A.; Roux, S.; Higashida Randall, T. Thick and Diffuse Subarachnoid Blood as a Treatment Effect Modifier of Clazosentan After Subarachnoid Hemorrhage. Stroke 2019, 50, 2738–2744. [Google Scholar] [CrossRef]
- Arefiev, K.; Fiorentino, D.F.; Chung, L. Endothelin Receptor Antagonists for the Treatment of Raynaud’s Phenomenon and Digital Ulcers in Systemic Sclerosis. Int. J. Rheumatol. 2011, 2011, 201787. [Google Scholar] [CrossRef] [Green Version]
- Cozzani, E.; Javor, S.; Laborai, E.; Drosera, M.; Parodi, A. Endothelin-1 levels in scleroderma patients: A pilot study. ISRN Dermatol. 2013, 2013, 125632. [Google Scholar] [CrossRef]
- Yamane, K.; Miyauchi, T.; Suzuki, N.; Yuhara, T.; Akama, T.; Suzuki, H.; Kashiwagi, H. Significance of plasma endothelin-1 levels in patients with systemic sclerosis. J. Rheumatol. 1992, 19, 1566–1571. [Google Scholar]
- Zamora, M.R.; O’Brien, R.F.; Rutherford, R.B.; Weil, J.V. Serum endothelin-1 concentrations and cold provocation in primary Raynaud’s phenomenon. Lancet 1990, 336, 1144–1147. [Google Scholar] [CrossRef]
- Kahaleh, M.B. Endothelin, an endothelial-dependent vasoconstrictor in scleroderma. Enhanced production and profibrotic action. Arthritis Rheum. 1991, 34, 978–983. [Google Scholar] [CrossRef]
- Richard, V.; Solans, V.; Favre, J.; Henry, J.P.; Lallemand, F.; Thuillez, C.; Marie, I. Role of endogenous endothelin in endothelial dysfunction in murine model of systemic sclerosis: Tight skin mice 1. Fundam. Clin. Pharmacol. 2008, 22, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Avouac, J.; Riemekasten, G.; Meune, C.; Ruiz, B.; Kahan, A.; Allanore, Y. Autoantibodies against Endothelin 1 Type A Receptor Are Strong Predictors of Digital Ulcers in Systemic Sclerosis. J. Rheumatol. 2015, 42, 1801–1807. [Google Scholar] [CrossRef] [PubMed]
- Kowal-Bielecka, O.; Fransen, J.; Avouac, J.; Becker, M.; Kulak, A.; Allanore, Y.; Distler, O.; Clements, P.; Cutolo, M.; Czirjak, L.; et al. Update of EULAR recommendations for the treatment of systemic sclerosis. Ann. Rheum. Dis. 2017, 76, 1327–1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabunga, P.; Coghlan, G. Endothelin receptor antagonism: Role in the treatment of pulmonary arterial hypertension related to scleroderma. Drugs 2008, 68, 1635–1645. [Google Scholar] [CrossRef]
- Shetty, N.; Derk, C.T. Endothelin receptor antagonists as disease modifiers in systemic sclerosis. Inflamm. Allergy Drug Targets 2011, 10, 19–26. [Google Scholar] [CrossRef]
- Raffa, R.B.; Schupsky, J.J.; Martinez, R.P.; Jacoby, H.I. Endothelin-1-induced nociception. Life Sci. 1991, 49, PL61–PL65. [Google Scholar] [CrossRef]
- Piovezan, A.P.; D’Orleans-Juste, P.; Tonussi, C.R.; Rae, G.A. Effects of endothelin-1 on capsaicin-induced nociception in mice. Eur. J. Pharmacol. 1998, 351, 15–22. [Google Scholar] [CrossRef]
- Khodorova, A.; Montmayeur, J.P.; Strichartz, G. Endothelin receptors and pain. J. Pain 2009, 10, 4–28. [Google Scholar] [CrossRef] [Green Version]
- Smith, T.P.; Haymond, T.; Smith, S.N.; Sweitzer, S.M. Evidence for the endothelin system as an emerging therapeutic target for the treatment of chronic pain. J. Pain Res. 2014, 7, 531–545. [Google Scholar] [CrossRef] [Green Version]
- Furukawa, A.; Shinoda, M.; Kubo, A.; Honda, K.; Akasaka, R.; Yonehara, Y.; Iwata, K. Endothelin Signaling Contributes to Modulation of Nociception in Early-stage Tongue Cancer in Rats. Anesthesiology 2018, 128, 1207–1219. [Google Scholar] [CrossRef]
- Tang, Y.; Peng, H.; Liao, Q.; Gan, L.; Zhang, R.; Huang, L.; Ding, Z.; Yang, H.; Yan, X.; Gu, Y.; et al. Study of breakthrough cancer pain in an animal model induced by endothelin-1. Neurosci. Lett. 2016, 617, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Lutz, B.M.; Wu, S.; Gu, X.; Atianjoh, F.E.; Li, Z.; Fox, B.M.; Pollock, D.M.; Tao, Y.X. Endothelin type A receptors mediate pain in a mouse model of sickle cell disease. Haematologica 2018, 103, 1124–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selenko-Gebauer, N.; Duschek, N.; Minimair, G.; Stingl, G.; Karlhofer, F. Successful treatment of patients with severe secondary Raynaud’s phenomenon with the endothelin receptor antagonist bosentan. Rheumatology Oxford 2006, 45 (Suppl. 3), iii45–iii48. [Google Scholar] [CrossRef] [Green Version]
- Williams, J.T.; Christie, M.J.; Manzoni, O. Cellular and synaptic adaptations mediating opioid dependence. Physiol. Rev. 2001, 81, 299–343. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, K.; Abe, I.; Fukuhara, M.; Tominaga, M.; Tsuchihashi, T.; Kobayashi, K.; Fujishima, M. Naloxone augments sympathetic outflow induced by centrally administered endothelin in conscious rabbits. Am. J. Physiol. 1994, 266, R1403–R1410. [Google Scholar] [CrossRef] [PubMed]
- Modanlou, H.D.; Beharry, K. Biochemical and molecular endothelin responses to morphine sulfate infusion in conscious newborn piglets. Can. J. Physiol. Pharmacol. 1998, 76, 443–450. [Google Scholar] [CrossRef]
- Puppala, B.L.; Matwyshyn, G.; Bhalla, S.; Gulati, A. Evidence that morphine tolerance may be regulated by endothelin in the neonatal rat. Biol. Neonate 2004, 86, 138–144. [Google Scholar] [CrossRef]
- Bhalla, S.; Matwyshyn, G.; Gulati, A. Morphine tolerance does not develop in mice treated with endothelin-A receptor antagonists. Brain Res. 2005, 1064, 126–135. [Google Scholar] [CrossRef]
- Quang, P.N.; Schmidt, B.L. Endothelin-A receptor antagonism attenuates carcinoma-induced pain through opioids in mice. J. Pain 2010, 11, 663–671. [Google Scholar] [CrossRef] [Green Version]
- Bhalla, S.; Pais, G.; Tapia, M.; Gulati, A. Endothelin ETA receptor antagonist reverses naloxone-precipitated opioid withdrawal in mice. Can. J. Physiol. Pharmacol. 2015, 93, 935–944. [Google Scholar] [CrossRef] [Green Version]
- Kohan, D.E.; Cleland, J.G.; Rubin, L.J.; Theodorescu, D.; Barton, M. Clinical trials with endothelin receptor antagonists: What went wrong and where can we improve? Life Sci. 2012, 91, 528–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gulati, A.; Sunila, E.S.; Kuttan, G. IRL-1620, an endothelin-B receptor agonist, enhanced radiation induced reduction in tumor volume in Dalton’s Lymphoma Ascites tumor model. Arzneimittelforschung 2012, 62, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Ji, L.; Dong, C.; Fan, R.; Qi, S. A high affinity nanobody against endothelin receptor type B: A new approach to the treatment of melanoma. Mol. Biol. Rep. 2020, 47, 2137–2147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangat, G.S.; Jaggi, A.S.; Singh, N. Ameliorative Effect of a Selective Endothelin ETA Receptor Antagonist in Rat Model of L-Methionine-induced Vascular Dementia. Korean J. Physiol. Pharmacol. 2014, 18, 201–209. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.; Gupta, S.; Sharma, B. Antagonism of Endothelin (ETA and ETB) Receptors During Renovascular Hypertension-Induced Vascular Dementia Improves Cognition. Curr. Neurovasc. Res. 2016, 13, 219–229. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bosentan [20] | Ambrisentan [21] | Macitentan [22] | Sitaxsentan [23] | Atrasentan [24] | Clazosentan [17] | Zibotentan [25] | Aprocitentan [26] | |
|---|---|---|---|---|---|---|---|---|
| Approval status | FDA: 2001 EMA: 2002 | FDA: 2007 EMA: 2008 | FDA: 2013 EMA: 2013 | Withdrawn | Experimental | Experimental | Experimental | Experimental |
| Receptor selectivity | Non-selective | Selective (ETA) | Non-selective | Selective (ETA) | Selective (ETA) | Selective (ETA) | Selective (ETA) | Non-selective |
| Administration and dose recommendation | Oral twice daily (62.5–125 mg) | Oral once daily (5–10 mg) | Oral once daily (10 mg) | Oral once daily (i.e., 100 mg) | Oral once daily (i.e., 40 mg) | Intravenous (30–60 mg/h for 6 h) | Oral once daily (10–100 mg [19]) | Well tolerated ≤100 mg/d for 10 days. |
| Oral bio-availability (%) | 49.8 [27] | 80 | 74 [28] | >90 | N.R. | N.R. | N.R. | Oral active |
| T½ (h) | 5 | 15 | 16 | ~10 | 24 | 1–2 | ~8 | N.R. |
| Tmax (h) | 3 | 2 | 8 | 1–2 | 1.5 | N.R. | 1 | N.R. |
| Metabolizing enzymes | CYP3A4 and CYP2C9 | CYP3A4, CYP2C19, UGTs 1A9S, 1A3S and 2B7S | CYP3A4, CYP2C19 | CYP2C9 [29] | Glucoronidation, CYP3A oxidation | CYP2C9 [30] | CYP3A4 | CYP3A4, CYP2C19 |
| Elimination pathway | Biliary excretion, bio-transformation | Biliary excretion, bio-transformation | Renal, fecal, bio-transformation | Renal, fecal | N.R. | Fecal, biliary excretion | Renal | Renal, fecal, bio-transformation |
| Common adverse effects | Headache, nausea, vomiting, flushing, palpitations | Peripheral edema, nasal congestion, headache, dizziness | Naso-pharyngitis, headache | Nausea, headache, peripheral edema, flushing | Headache, rhinitis, asthenia, peripheral edema | Headache, nausea, nasal obstruction, vomiting | Headache, nausea | Hypertension, headache, nasopharyngitis, decrease in hemoglobin and hematocrit |
| Serious adverse effects | Anemia, abnormal hepatic function | None known | Anemia | Serious impact on liver function | Hypotension, hyponatremia [31] | None known | Lesions of olfactory epithelium [32] | N.R. |
| Trial | Design | Objective | Study Size | Status |
|---|---|---|---|---|
| NCT01827059: A randomized placebo-controlled trial to analyze changes in pulmonary arterial pressures at peak exercise in congenital heart disease patients with exercise-induced PAH before and after treatment with bosentan, compared to placebo (BICYCLE) | Interventional, Randomized, Parallel assignment, Double-blind, Phase II | The objective of this trial is to analyse changes in pulmonary arterial pressure at peak exercise before and after treatment with bosentan, compared to placebo, in patients with con-genital heart disease. | 12 participants | Unknown |
| NCT01347216: Prospective registry of newly initiated therapies for pulmonary hypertension (COMPERA) | Observational, Cohort, Prospective | The aim of this trial is to compare the results of the manifold options for mono- and combination therapy in the treatment of PAH. | 10,000 participants | Recruiting |
| NCT01406327: Drug use investigation for VOLIBRIS® (ambrisentan) (PAH) | Observational | The goal of this trial is to evaluate the incidence of adverse events in Japanese PAH patients treated with ambrisentan. | 900 participants | Active, not recruiting |
| NCT03809156: Upfront riociguat and ambrisentan combination therapy for PAH: a safety and efficacy pilot study | Interventional, Single group assignment, No masking, Phase IV | The aim of this trial is to evaluate the efficacy and safety of first-line combination therapy using ambrisentan and riociguat in patients with PAH. | 20 participants | Recruiting |
| NCT01342952: An open-label, long-term extension study for treatment of pulmonary arterial hypertension in pediatric patients aged 8 years up to 18 years who have participated in AMB112529 and in whom continued treatment with ambrisentan is desired | Interventional, Single group assignment, No masking, Phase II | The primary objective of this trial is to assess the long-term tolerability and safety of ambrisentan in a pediatric PAH population. Secondary objectives include all-cause mortality and change from baseline on efficacy parameters in Study AMB112529. | 66 participants | Recruiting |
| NCT02932410: A multicenter, open-label, randomized, event-driven study to assess efficacy, safety and pharmacokinetics of macitentan versus standard of care in children with PAH (TOMORROW) | Interventional, Randomized Parallel assignment, No masking, Phase III | The goal of this trial is to evaluate the efficacy, safety and pharmacokinetics of macitentan in children with PAH. | 300 participants | Recruiting |
| NCT03422328: Multicenter, single-arm, open-label, long-term safety study with macitentan in patients with pulmonary arterial hypertension previously treated with macitentan in clinical studies (UMBRELLA) | Interventional, Single group assignment no masking, Phase III | The aim of this trial is to evaluate the long-term safety of mac-itentan, and to provide continued treatment with macitentan in patients with PAH who were treated with macitentan in previous clinical studies. | 94 participants | Enrolling by invitation |
| NCT00667823: Long-term single-arm open-label extension study of the SERAPHIN study, to assess the safety and tolerability of ACT 064992 in patients with symptomatic PAH (SERAPHIN OL) | Interventional, single group assignment, no masking, Phase III | The objective of this trial is to evaluate the long-term tolerability and safety of maci-tentan in patients with symptomatic PAH. | 550 participants | Active, not recruiting |
| NCT02126943: US-based, observational, drug registry of opsumit® (macitentan) new users in clinical practice (OPUS) | Observational, Cohort, Prospective | The goal of this trial is to assess safety and to describe outcomes and clinical characteristics of patients newly treated with macitentan. | 5000 participants | Recruiting |
| NCT03904693: Prospective, multi-center, double-blind, randomized, active-controlled, triple-dummy, parallel-group, group-sequential, adaptive phase 3 clinical study to compare the efficacy and safety of macitentan and tadalafil monotherapies with the corresponding fixed dose combination in subjects with PAH, followed by an open-label treatment period with macitentan and tadalafil fixed dose combination therapy | Interventional, Randomized, Parallel assignment, Double blind, Phase III | The aim of this trial is to assess the benefits of a fixed-dose combination therapy with macitentan and the phosphodiesterase type 5 inhibitor tadalafil compared to monotherapy with macitentan or tadalafil. | 170 participants | Recruiting |
| NCT03362047: ’Untersuchung des Einflusses PAH-spezifischer Medikation auf die rechtsventrikuläre Funktion bei Patienten mit PAH unter basalen Bedingungen’ | Interventional, Randomized, Parallel assignment, no masking, Phase II | The objective of this pilot study is to determine the therapeutic effect of two parallel groups treated with either macitentan or the soluble guanylate cyclase (sGC) stimulator riociguat. | 30 participants | Recruiting |
| Tumor Type | Endothelin Receptors | Effects Associated with Endothelin Receptor Expression | References |
|---|---|---|---|
| Bladder cancer | ETA, ETB | Reduced survival | [80,81] |
| Breast cancer | ETA | Reduced survival; increased invasion; bone metastasis | [82,83] |
| Cervical cancer | ETA | N.R. | [84] |
| Colorectal cancer | ETA | Reduced survival; increased tumor grade | [85,86] |
| Gastric cancer | ETA, loss of ETB | N.R. | [87,88] |
| Glioblastoma | ETA, ETB | N.R. | [89,90,91] |
| Head and neck cancer | ETA | Reduced survival | [92,93] |
| Hepatocellular carcinoma | ETA, loss of ETB | Cell migration; invasion | [94,95] |
| Lung cancer | NSCLC: ETA SCLC: ETB | NSCLC (adenocarcinoma): Reduced survival | [96,97] |
| Malignant melanoma | ETB | Aggressive phenotype; cancer progression; metastasis to lymph nodes | [98,99] |
| Ovarian cancer | ETA | Increased tumor grade; chemoresistance; metastasis | [100,101] |
| Pancreatic cancer | ETA, ETB | Proliferation; angiogenesis | [102,103,104] |
| Prostate cancer | ETA | Increased tumor grade; bone metastasis | [105,106] |
| Renal cell carcinoma | ETA, ETB | Reduced survival (ETB), increased tumor grade (ETA) | [107,108,109,110] |
| Thyroid cancer | ETA | PTC: Tumor growth; lymph node metastases | [111] |
| Vulvar cancer | ETB | Reduced survival | [112] |
| ERA + Combination | Receptor Antagonism | Tumor Type | Clinical Development | Results | Ref. |
|---|---|---|---|---|---|
| Zibotentan | ETA | Prostate cancer (non-metastatic CRPC) | Phase III | No significant effect. | [125] |
| Prostate cancer (metastatic CRPC) | Window Study, NCT01168141 | N.R. | |||
| Prostate cancer (non-metastatic HRPC) | Phase III, NCT00626548 | Study terminated. | |||
| Prostate cancer (metastatic HRPC) | Phase III, NCT00554229 | No significant effect on OS. | [122] | ||
| +Docetaxel | Phase III, NCT00617669 | No significant effect on OS. | [126] | ||
| +Pemetrexed | Lung cancer (NSCLC) | Phase II | No survival or progression advantage. | [127] | |
| Atrasentan | ETA | Prostate cancer (non-metastatic HRPC) | Phase III | No significant effect. | [128] |
| Prostate cancer (metastatic HRPC) | Phase III | No delay in disease progression. | [129] | ||
| +Docetaxel +Prednisone | Prostate cancer (metastatic CRPC) | Phase III, NCT00134056 | No effect on OS or PFS; patients with highly elevated markers of bone turnover may benefit from atrasentan. | [130,131,132] | |
| Metastatic renal cell carcinoma | Phase II | No significant effect. | [133] | ||
| YM598 | ETA | Prostate cancer | Phase II, NCT00050297 | N.R. | |
| Metastatic prostate cancer | Phase II, NCT00048659 | N.R. | |||
| SPI-1620 +Docetaxel | ETB | Biliary Cancer | Phase II, NCT01773785 | Study terminated. | [134] |
| Bosentan | ETA, ETB | Metastatic melanoma | Phase II, | Possible benefit in disease stabilization. | [135] |
| +Dacarbazine | Phase II, NCT01009177 | No effect on tumor progression. | [136] | ||
| +Nab-paclitaxel +Gemcitabine | Pancreatic cancer | Phase I, NCT04158635 | Not yet recruiting. | ||
| Macitentan + Temozolomide | ETA, ETB | Newly diagnosed glioblastoma | Phase I, NCT02254954 | Study terminated. | |
| Recurrent glioblastoma | Phase I, NCT01499251 | Study terminated. |
| Disease | ERA | Receptor Antagonism | Clinical Development | Results | Ref. |
|---|---|---|---|---|---|
| Chronic kidney disease | Sitaxsentan | ETA | Phase II, NCT00810732 | Reduced GFR, proteinuria and BP. | [143,145] |
| BQ-123 | ETA | Phase I, NCT00722215 | N.R. | ||
| Diabetic nephropathy | Avosentan | ETA | Phase III, NCT00120328 | Study terminated. | |
| Atrasentan | ETA | Phase II, NCT01399580 | Reduced urinary albumin/creatinine ratio. | [146] | |
| Phase II, NCT01356849 | |||||
| Phase II, NCT01424319 | Reduced urine albumin/creatinine ratios and albuminuria. | [146,147,148] | |||
| Phase II, NCT00920764 | Preserved estimated GFR. | [149] | |||
| Focal segmental glomerulosclerosis | Sparsentan | ETA (+ARB) | Phase II, NCT01613118 | Reduced proteinuria. | [144] |
| Sickle cell disease | Ambrisentan | ETA | Phase I, NCT02712346 | Not yet reported. | |
| Idiopathic pulmonary fibrosis | Bosentan | ETA, ETB | Phase III, NCT00391443 | Well tolerated; no significant effect. | [150] |
| Phase II, NCT00071461 | No effect on 6MWD; little improvement in QOL | [151] | |||
| Ambrisentan | ETA | Phase III, NCT00768300 | No significant effect. | [152] | |
| Macitentan | ETA, ETB | Phase II, NCT00903331 | No significant effect. | [153] | |
| Malignant hypertension | Aprocitentan | ETA, ETB | Phase III, NCT03541174 | Not yet reported. | |
| Cerebral vasospasm | Clazosentan | ETA | Phase II, NCT00111085 | Decreased the incidence of severe vasospasm. | [154] |
| Phase III, NCT00558311 | No significant effect. | [155] | |||
| Phase III, NCT00940095 | Reduced mobidity; no dose improved outcome. | [156] | |||
| Systemic sclerosis (digital ulcers) | Macitentan | ETA, ETB | Phase III, NCT01474109 | No significant effect. | [157] |
| Phase III, NCT 01474122 | Study terminated. | ||||
| Bosentan | ETA, ETB | RAPIDS-1 | Improvement in hand function. | [158] | |
| RAPIDS-2 | Reduced occurrence of new digital ulcers; no effect on healing. | [159] | |||
| Prospective observational study | Improvement of functionality and QOL by reducing disease-related symptoms. | [160] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Enevoldsen, F.C.; Sahana, J.; Wehland, M.; Grimm, D.; Infanger, M.; Krüger, M. Endothelin Receptor Antagonists: Status Quo and Future Perspectives for Targeted Therapy. J. Clin. Med. 2020, 9, 824. https://doi.org/10.3390/jcm9030824
Enevoldsen FC, Sahana J, Wehland M, Grimm D, Infanger M, Krüger M. Endothelin Receptor Antagonists: Status Quo and Future Perspectives for Targeted Therapy. Journal of Clinical Medicine. 2020; 9(3):824. https://doi.org/10.3390/jcm9030824
Chicago/Turabian StyleEnevoldsen, Frederik C., Jayashree Sahana, Markus Wehland, Daniela Grimm, Manfred Infanger, and Marcus Krüger. 2020. "Endothelin Receptor Antagonists: Status Quo and Future Perspectives for Targeted Therapy" Journal of Clinical Medicine 9, no. 3: 824. https://doi.org/10.3390/jcm9030824