1. Introduction
By early February 2020, it was evident that the incidence of novel coronavirus infections (COVID-19) was growing exponentially [
1]. Accelerated by human migration, exported cases have been reported in various regions of the world, including Europe, Asia, North America, and Oceania [
2]. To minimize the rapid growth of cases via human-to-human transmission [
3,
4,
5], the government of China suspended all modes of transportation to and from Wuhan on 23 January 2020—including vehicles, trains, and flights—expecting that the intervention would prevent further spread of the disease [
6]. As of 12 February 2020, two additional cities outside of Hubei Province—Wenzhou (Zhejiang Province) and Shenzhen (Guangdong Province)—have been placed on complete lockdown (i.e., no cross-border movement to and from the closed city) to prevent further spatial spread of COVID-19. To our knowledge, such drastic movement restrictions are a historical first.
Since Wuhan was placed on lockdown, travel restriction and border control have been implemented by various countries, either as: (i) complete travel bans, (ii) travel restriction and quarantine—which allows for restriction of healthy individuals, (iii) entry screening for all incoming travelers, or some combination thereof. Most countermeasures are in line with (ii) and (iii), aside from the three cities on complete lockdown, while some countries at high risk refused any entry from China (e.g., Australia) or those from Hubei and Zhejiang provinces (e.g., Japan). All travel arrangements including tourist tours outbound from China (to international destinations) organized by Chinese travel agencies were cancelled, and all non-urgent travel with business purposes both inbound and outbound were greatly reduced.
The effectiveness of quarantine (i.e., lockdown) measures to prevent the spread of an epidemic due to a novel infectious pathogen where no vaccine is available has often been a subject of debate [
7,
8,
9]. Under ordinary circumstances, border control efforts do not go beyond entry screening. However, during the epidemic of severe acute respiratory syndrome (SARS) in 2002–2003, although entry screening at airports and other key locations was adopted, in most countries its effectiveness was estimated to be very limited due to the relatively long incubation period and low prevalence of SARS, which resulted in extremely low positive predictive values at screening locations [
10,
11,
12,
13]. In the ongoing COVID-19 epidemic, many countries have accompanied regular entry screening with drastic changes in travel restrictions. Although the effectiveness of entry screening is likely very limited as already shown elsewhere [
14], the epidemiological impact of the change in movement restrictions has yet to be explicitly evaluated.
In this study, we quantify the impact of the drastic reduction in travel volume—resulting from movement restrictions—on the transmission dynamics outside China. We aim to estimate reductions in the number of exported cases, probability of an outbreak occurring outside China, and any time delay to a major epidemic that may be gained with these policies. We use the example of Japan, the country in Asia that receives the largest number of visitors from China, to calculate our estimates.
2. Methods
2.1. Epidemiological Data
An epidemiological dataset of confirmed cases with COVID-19 infection diagnosed outside China was collected from government and news websites quoting official outbreak reports. For each case, the date of reporting and country of diagnosis were recorded. The data included only cases diagnosed outside China, but for whom infection may have occurred either in or outside China. The dataset is available as
Supplementary Material (Table S1). All cases were confirmed using reverse transcriptase polymerase chain reaction (RT-PCR) apart from two cases in Australia that were clinically diagnosed. The endpoint for data collection was set at 6 February 2020.
2.2. Statistical Model
We considered the impact of reduced travel volumes on COVID-19 transmission dynamics outside China. Specifically, we quantified the impact on: (i) the number of exported cases, (ii) the probability of a major epidemic, and (iii) the time delay to a major epidemic.
2.2.1. Reduced Number of Exported Cases
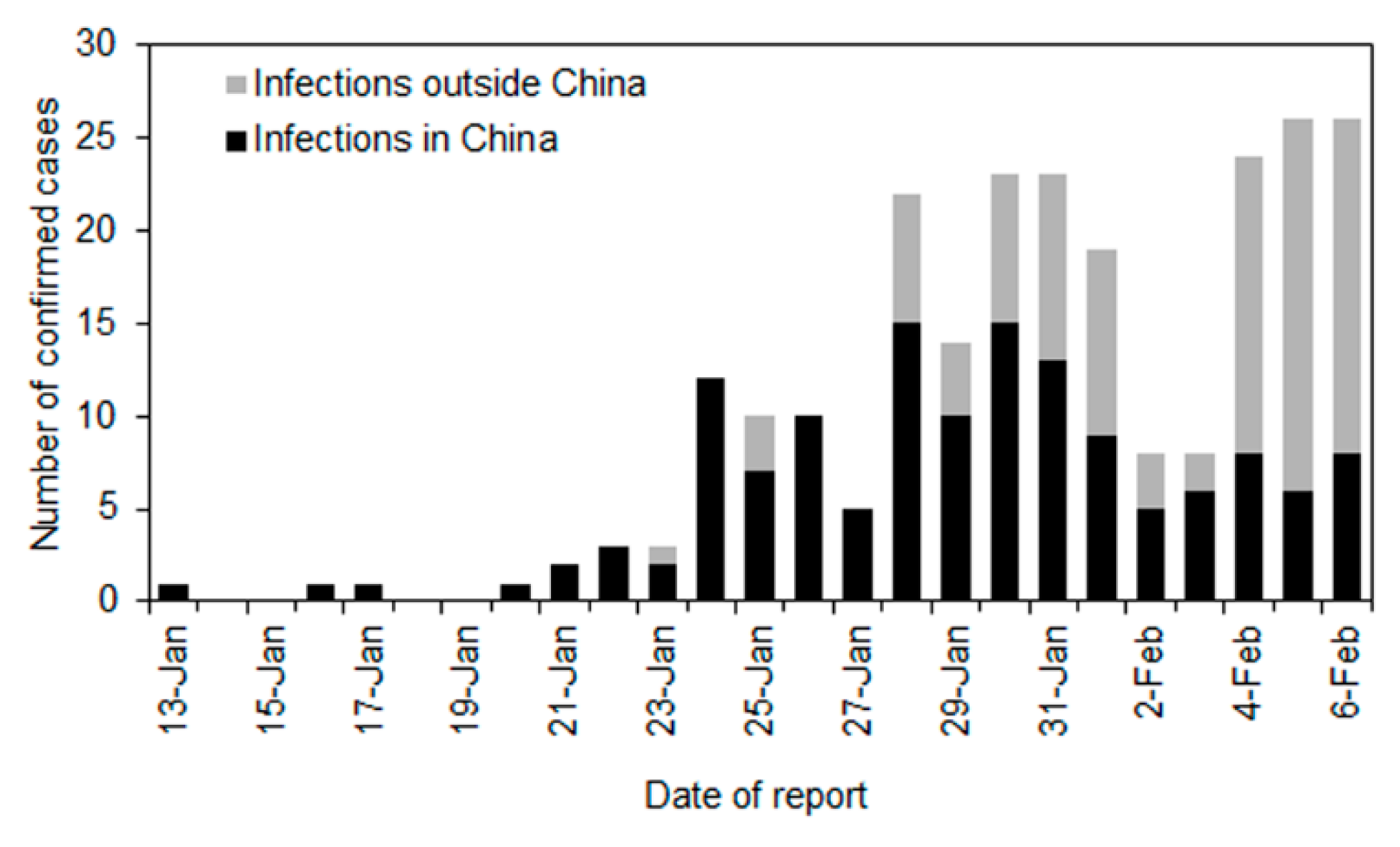
Figure 1 shows the observed number of infections in and outside China. The first exported case in Thailand was reported on 13 January 2020. Assuming the epidemic start date is set at 1 December 2019 (Day 0), the city of Wuhan was put in lockdown from Day 53 (or 23 January 2020). Considering that the mean incubation period of COVID-19 approximately is 5 days, the impact of reduced travel volumes would start to be interpretable from Day 58 (28 January 2020). We used data from Day 43 (13 January) onwards because the first case diagnosed outside China was reported on that day.
To estimate the reduced volume of exported cases, we employ a counterfactual model. If we let
c(
t) be the incidence of exported cases on Day
t, Poisson regression was used to fit the following model through Day 57:
where
is the initial value at
t = 0 and
r is the exponential growth rate of exported cases outside China. Using the estimated parameters and their covariance matrix, we obtain the expected number of exported cases from Day 58 onwards. Supposing that
h(
t) is the observed number of cases on day
t, the reduced travel volume of exported cases by Day 67 is calculated as:
2.2.2. Reduced Probability of a Major Epidemic Overseas
We assumed that the distribution of the number of secondary cases generated by a single primary case follows a negative binomial distribution with the basic reproduction number
R0, i.e., the average number of secondary cases generated by a single primary case, and the dispersion parameter
k. The probability of extinction
defined by the first generating moment [
15] is then modeled as:
R0 is estimated to range from 1.5 to 3.7, and here we adopt 1.5, 2.2, and 3.7 as plausible values for our calculations [
16,
17,
18]. The value of
k, a dispersion parameter, is assumed to be 0.54 as estimated elsewhere [
17].
Supposing that there are
n untraced cases that were independently introduced, the probability of a major epidemic is:
Now we compare two scenarios: the observed data as influenced by the reduction in travel volume, and a counterfactual scenario in which travel volume reduction does not take place. The cumulative number of exported COVID-19 cases observed in the former scenario is denoted
m, while
describes the number of cases in the counterfactual scenario. This leads to the following sums:
and
Accordingly, the reduced probability of a major epidemic is calculated as:
It should be noted that the probability of a major epidemic is evaluated at the country level, and only results for Japan are presented here. Whereas, the proposed method can equally handle the probability of a major epidemic for each importing country.
For the computation, we first subtracted
the integral of
, by the integral of
, assuming that all cases
were already traced, and then we multiplied the difference by 0.9, 0.7, or 0.5 if only 10%, 30%, or 50% of contacts were traced, respectively. For
m, we accounted for three symptomatic cases that were regarded as locally acquired infections in reports and diagnosed between Day 58 and Day 67. Assuming that the asymptomatic ratio was 50% [
19], we considered that in total there were
m = 6 untraced cases including the diagnosed cases.
2.2.3. Time Delay to a Major Epidemic Gained from the Reduction in Travel Volume
Lastly, we measured the time delay to a major epidemic gained from the reduction in travel volume using the hazard function of a major epidemic,
, in the absence of travel volume changes. We model the probability of a major epidemic by time
t in the absence of travel volume reduction as follows:
In the presence of travel volume reduction, the hazard is reduced by the relative reduction factor in the probability of a major epidemic:
Here, we consider the median time to a major epidemic in (8) and (9). Since an exponential growth of cases has been observed, we let the hazard be an exponential function. Then, the integral of the hazard function holds the form:
where
C is a constant (assumed to be one for the following calculation), and
r is the exponential growth rate estimated at 0.14 per day [
16]. The doubling time is then calculated as
td = ln(2)/
r = 4.95 days. The difference in the median date between (8) and (9) is thus described as:
All computations were conducted in JMP Version 14.0 (SAS Institute, Cary, North Carolina). The confidence intervals were calculated using profile likelihood method.
3. Results
As
Figure 1 shows, a total of 242 cases were diagnosed and reported outside of China in 27 countries between Day 43 (13 January) and Day 67 (6 February 2020). Of these, 140 cases were considered to have been infected in China and 102 cases were considered to have been infected outside China. The country with the highest number of exported cases infected inside China was Thailand (
n = 20), followed by Singapore (
n = 18), Australia (
n = 14), and Japan (
n = 12). Among 242 cases, we specifically focused on 140 cases who traveled while movement restrictions were in place and were likely affected by said restrictions.
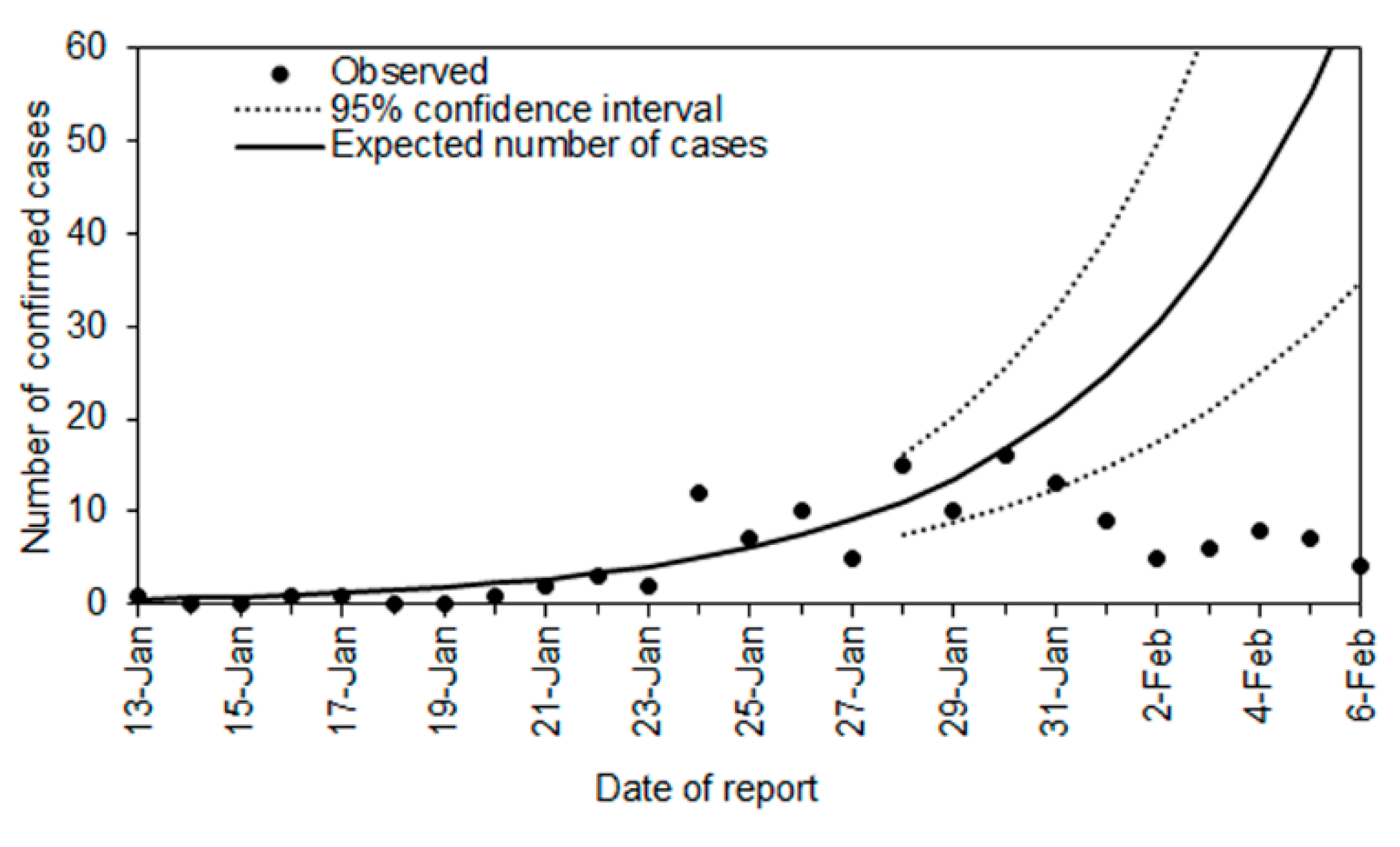
Figure 2 compares the observed and expected number of cases diagnosed outside China by date of report. The exponential growth of cases is consistent with the exponential growth of incidence in China, which qualitatively captures the observed pattern of incidence from Day 43 to Day 57. Using the predicted curve, the expected number of cases between Day 58 (28 January 2020) and Day 67 was 321 cases (95% confidence interval [CI]: 181, 544). In the empirical observation, a total of 95 cases were diagnosed, including 8 cases in Japan. That is, following the time that Wuhan city was put in lockdown, we estimate that 226 cases (95% CI: 86, 449) were prevented from being exported across the world. This corresponds to a reduction in the number of exported cases of 70.4% during that time period.
As another measure of impact, we estimated the probability of a major epidemic.
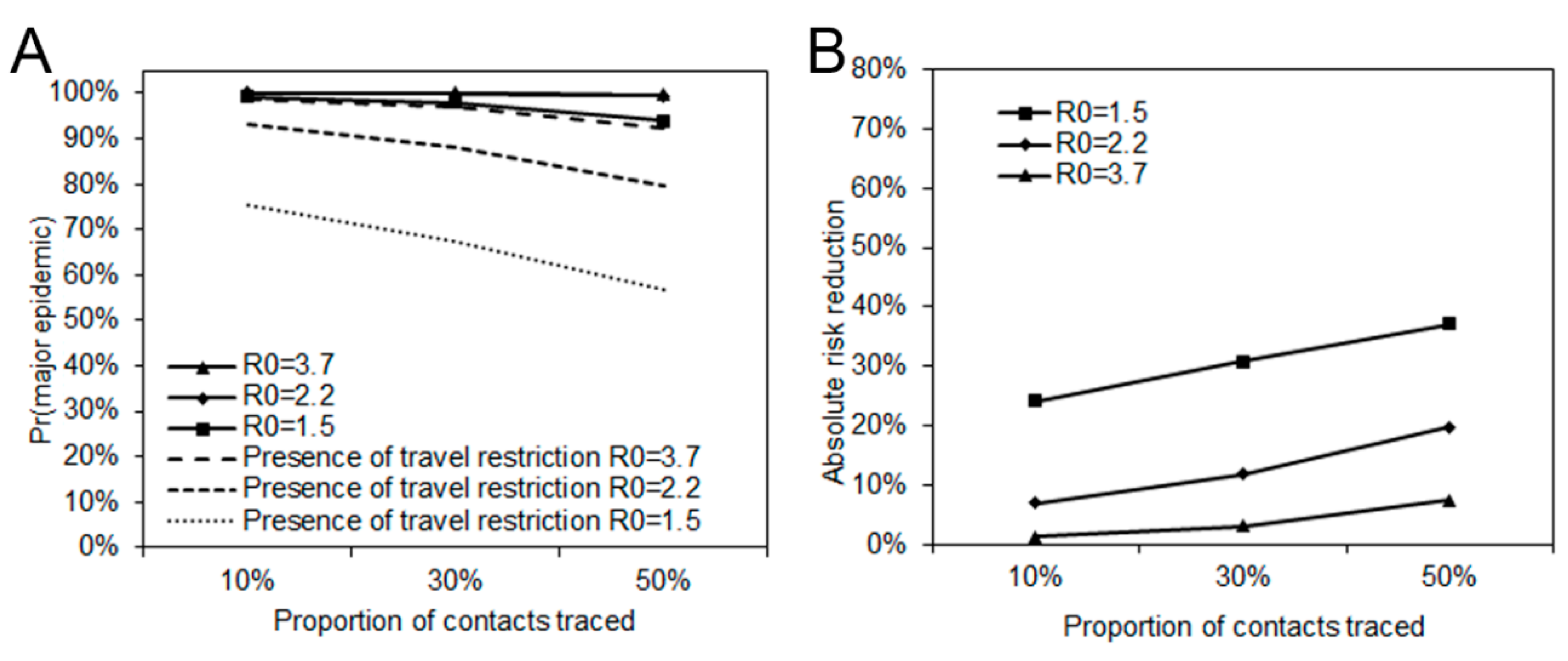
Figure 3A shows the probability of a major epidemic with three different levels of transmissibility assuming an
R0 of 1.5, 2.2, or 3.7, and three different levels of contact tracing resulting in a success rate of isolation of the traced contacts of 10%, 30%, or 50%. Without the reduction in the travel volume, the probability of a major epidemic exceeded 90% in most scenarios. However, considering there have been six untraced cases in Japan under travel restrictions, the probability of a major epidemic more broadly ranged from 56% to 98%.
Figure 3B shows the reduced probability of a major epidemic. Assuming an
R0 of 2.2, the absolute risk reduction was 7%, 12%, and 20%, respectively, for contact tracing levels leading to isolation at 10%, 30%, and 50%.
Figure 3B describes the absolute reduction in risk of a major epidemic. The largest reduction was 37% when
R0 = 1.5 and 50% of contacts were traced. The smallest reduction was 1% when
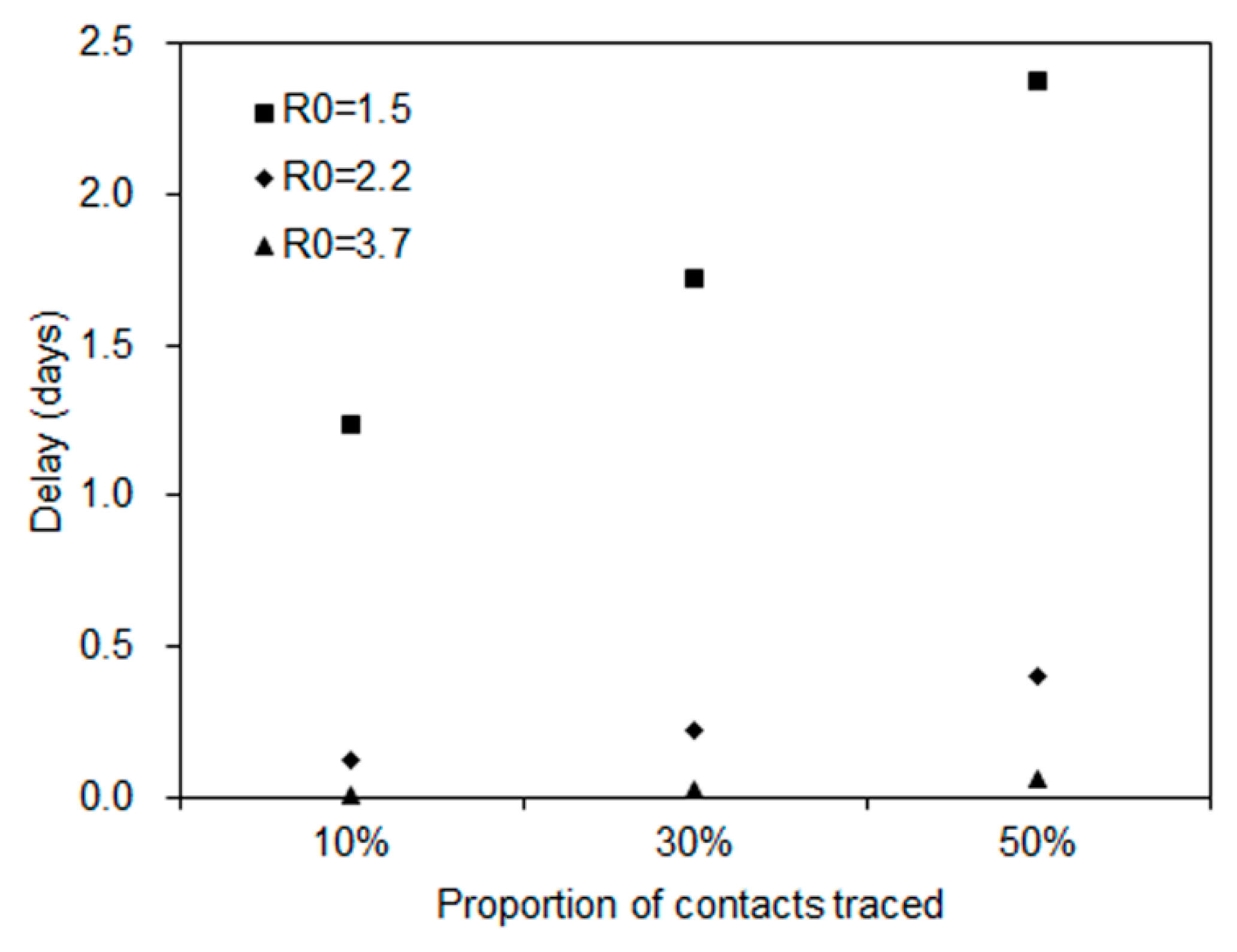
R0 = 3.7 and 10% of contacts were traced. Using those estimated relative reductions, the median time of delay gained by travel volume reduction is shown in
Figure 4. The time delay of a major epidemic was less than one day when
R0 is 2.2 and 3.7, and 1 to 2 days when
R0 is 1.5.
4. Discussion
The present study explicitly quantified the epidemiological impact of reduced travel volume to and from China on the transmission dynamics of COVID-19 outside China using simple statistical models. The three epidemiological outcomes we measured on the example of Japan were: (i) the number of exported cases, (ii) the probability of a major epidemic, and (iii) the time delay to a major epidemic. When the volume of exported cases outside China was considered to have been reduced by 70.4%, the probability of a major epidemic was estimated to be reduced by 7%–20% in Japan, and a 2-day delay was gained in the estimated time to a major epidemic between Day 58 and Day 67.
The reduced volume of exported cases was estimated to be as large as 226 cases outside China. Our estimate is consistent with an assessment by Chinazzi et al. [
20], which indicated that the exported cases would be reduced by 80% by the end of February. In addition to appropriately quantifying the impact on prevention of exported cases, we have estimated the median time delay to a major epidemic assuming plausible values of
R0 at 1.5, 2.2, and 3.7. With reduced probability of a major epidemic, the time delay to a major epidemic was estimated at a maximum of 2 days in Japan and a minimum of less than 1 day. The estimated effect of the delay to a major epidemic outside China is smaller than what was anticipated for cities in China other than Wuhan. Tian et al. [
21] estimated that the reduction in travel volume led to a 2.9-day delay in the spatial spread in China. To our knowledge, the present study is the first to have used simple stochastic process models to explicitly estimate the time delay to a major epidemic in Japan that gained by the drastic reduction in travel volume in and outside China.
Although the COVID-19 epidemic was declared a public health emergency of international concern (PHEIC) by the World Health Organization (WHO), the WHO specifically called upon member states to not restrict the freedom of movement of persons as a result of the epidemic [
22]. However, member states did not adhere to this recommendation and have varyingly restricted the free movement of people from China [
23]. Such restrictions were most drastic in China, where some cities were put on complete lockdown [
23]. These political decisions regarding movement restrictions must balance the expected epidemiological impact with predicted economic burden—the latter of which we did not examine. While securing a few days delay to epidemic spread in China would secure time for healthcare systems in Chinese cities that have not yet been affected to prepare for the appearance of case-patients [
21], the impact of such a delay outside China is not substantial enough to accomplish meaningful prevention, such as the development, manufacturing, and distribution of a vaccine.
In modern history, this epidemic is perhaps the first instance where a large city populated with more than 10 million people was placed on lockdown. While countermeasures to prevent epidemic spread require the sort of strong political decisions that resulted in strong movement restrictions, our study indicated that the delay to a major epidemic in countries other than China (using Japan as an example) was unfortunately minimal. While the complete lockdown of Wuhan, Wenzhou, and Shenzhen likely helped reduce case incidence outside of these cities, migration from other cities in China could still contribute to the spread of infection locally and internationally [
24,
25,
26]. To quantify the epidemiological impact for the entire course of the epidemic more precisely, a more detailed analysis using dynamic datasets, e.g., airline passenger data, should be explored in the future.
Limitations of the present study must be discussed. First, the present study relied on the volume of cases diagnosed outside China and did not directly examine human migration data. Second, we were unable to classify exported cases into those who acquired infection in Hubei versus elsewhere in China. Having this information may offer additional insight. Third, several rough assumptions (e.g., a fixed time delay from illness onset to reporting at 5 days) were imposed, and the results presented here should be regarded as a preliminary assessment.
5. Conclusions
In conclusion, the present study explored the impact of reduced travel volume to and from China on the transmission dynamics of COVID-19 outside China, estimating that the time delay to a major epidemic was on the order of 2 days by 7 February 2020 for Japan. A relatively short time period of gain is likely due to high contingency of the SARS-CoV-2, and also that the substantial fraction of infected individuals with milder symptoms are likely to escape the border control. Our proposed approach was kept simple and will be applicable to other emerging epidemics in the future.
Author Contributions
H.N. conceived the study, A.A. and T.K. collected the data and analyzed the empirical data using models. All authors participated in the study design. A.A, T.K. and H.N. drafted the manuscript. All authors gave comments on the earlier versions of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
H.N. received funding from the Japan Agency for Medical Research and Development (AMED) [grant number: JP18fk0108050]; the Japan Society for the Promotion of Science (JSPS) KAKENHI [grant numbers, H.N.: 17H04701, 17H05808, 18H04895 and 19H01074; R.K.: 18J21587; AS.: 19K24159], the Inamori Foundation, and the Japan Science and Technology Agency (JST) CREST program [grant number: JPMJCR1413]. SMJ and NML receive graduate study scholarships from the Ministry of Education, Culture, Sports, Science and Technology, Japan.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Novel Coronavirus—China, 2020. Available online: https://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/ (accessed on 11 February 2020).
- World Health Organization. Novel Coronavirus (2019-nCoV) Situation Report-21, 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200210-sitrep-21-ncov.pdf (accessed on 11 February 2020).
- Center for Disease Central and Prevention. 2019 Novel Coronavirus, Wuhan, China, 2020. Available online: https://www.cdc.gov/coronavirus/2019-nCoV/summary.html (accessed on 11 February 2020).
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N. Engl. J. Med. 2020. (In Press) [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, F.J.; Yuan, S.; Kok, K.H.; To, K.K.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.; Poon, R.W.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020. (In Press) [Google Scholar] [CrossRef] [Green Version]
- BBC NEWS. Coronavirus: Wuhan Shuts Public Transport over Outbreak, 2020. Available online: https://www.bbc.com/news/world-asia-china-51215348 (accessed on 11 February 2020).
- Barbera, J.; Macintyre, A.; Gostin, L.; Inglesby, T.; O’Toole, T.; DeAtley, C.; Tonat, K.; Layton, M. Large-scale quarantine following biological terrorism in the United States: Scientific examination, logistic and legal limits, and possible consequences. JAMA 2001, 286, 2711–2717. [Google Scholar] [CrossRef] [PubMed]
- Nishiura, H.; Wilson, N.; Baker, M.G. Quarantine for pandemic influenza control at the borders of small island nations. BMC Infect. Dis. 2009, 9, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbisch, D.; Koenig, K.L.; Shih, F.-Y. Is There a Case for Quarantine? Perspectives from SARS to Ebola. Disaster Med. Public Health Prep. 2015, 9, 547–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, Y.-H.; King, C.-C.; Chen, C.W.S.; Ho, M.-S.; Hsu, S.-B.; Wu, Y.-C. Impact of quarantine on the 2003 SARS outbreak: A retrospective modeling study. J. Theor. Biol. 2007, 244, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Pitman, R.J.; Cooper, B.S.; Trotter, C.L.; Gay, N.J.; Edmunds, W.J. Entry screening for severe acute respiratory syndrome (SARS) or influenza: Policy evaluation. BMJ 2005, 331, 1242–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samaan, G.; Patel, M.; Spencer, J.; Roberts, L. Border screening for SARS in Australia: What has been learnt? Med. J. Aust. 2004, 180, 220–223. [Google Scholar] [CrossRef] [PubMed]
- St John, R.K.; King, A.; de Jong, D.; Bodie-Collins, M.; Squires, S.G.; Tam, T.W.S. Border screening for SARS. Emerg. Infect. Dis. 2005, 11, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Akhmetzhanov, A.R.; Hayashi, K.; Linton, N.M.; Yang, Y.; Yuan, B.; Kobayashi, T.; Kinoshita, R.; Nishiura, H. Real time estimation of the risk of death from novel coronavirus (2019-nCoV) infection: Inference using exported cases. J. Clin. Med. 2020, 9, 523. [Google Scholar] [CrossRef] [Green Version]
- Britton, T. Stochastic epidemic models: A survey. Math. Biosci. 2010, 225, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Quilty, B.J.; Clifford, S.; CMMID nCoV working group; Flasche, S.; Eggo, R.M. Effectiveness of airport screening at detecting travellers infected with novel coronavirus (2019-nCoV). Eurosurveillance 2020, 25, 2000080. [Google Scholar] [CrossRef] [PubMed]
- Riou, J.; Althaus, C.L. Pattern of early human-to-human transmission of Wuhan 2019 novel coronavirus (2019-nCoV), December 2019 to January 2020. Eurosurveillance 2020, 25, 2000058. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Nishiura, H.; Kobayashi, T.; Miyama, T.; Suzuki, A.; Jung, S.; Hayashi, K.; Kinoshita, R.; Yang, Y.; Yuan, B.; Akhmetzhanov, A.R.; et al. Estimation of the Asymptomatic Ratio of Novel Coronavirus (2019-nCoV) Infections among Passengers on Evacuation Flights. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.02.03.20020248v1 (accessed on 13 February 2020).
- Chinazzi, M.; Davis, J.T.; Ajelli, M.; Gioannini, C.; Litvinova, M.; Merler, S.; Pastore, Y.; Piontti, A.; Rossi, L.; Sun, K.; et al. The Effect of Travel Restrictions on the Spread of the 2019 Novel Coronavirus (2019-nCoV) Outbreak. 2020. Available online: https://www.mobs-lab.org/uploads/6/7/8/7/6787877/modeling_travel_limitations_paper.pdf (accessed on 11 February 2020).
- Tian, H.; Li, Y.; Liu, Y.; Kraemer, M.U.G.; Chen, B.; Cai, J.; Li, B.; Xu, B.; Yang, Q.; Yang, P.; et al. Early Evaluation of the Wuhan City Travel Restrictions in Response to the 2019 Novel Coronavirus Outbreak. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.01.30.20019844v1 (accessed on 11 February 2020).
- World Health Organization. Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV), 2020. Available online: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 11 February 2020).
- BBC NEWS. Coronavirus: US Bars Foreigners Who Recently Visited CHINA, 2020. Available online: https://www.bbc.com/news/world-us-canada-51335278 (accessed on 11 February 2020).
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: A modelling study. Lancet 2020. (In Press) [Google Scholar] [CrossRef] [Green Version]
- Tang, B.; Wang, X.; Li, Q.; Bragazzi, N.L.; Tang, S.; Xiao, Y.; Wu, J. Estimation of the Transmission Risk of the 2019-nCoV and Its Implication for Public Health Interventions. J. Clin. Med. 2020, 9, 462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, R.N. Novel Coronavirus Outbreak in Wuhan, China, 2020: Intense Surveillance Is Vital for Preventing Sustained Transmission in New Locations. J. Clin. Med. 2020, 9, 498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).

 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}



