The Surgical Benefit of Hysterolaparoscopy in Endometriosis-Related Infertility: A Single Centre Retrospective Study with a Minimum 2-Year Follow-Up

 ,
,
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hughes, E.G.; Fedorkow, D.M.; Collins, J.A. A quantitative overview of controlled trials in endometriosis-associated infertility. Fertil. Steril. 1993, 59, 963–970. [Google Scholar] [CrossRef]
- Rizk, B.; Turki, R.; Lotfy, H.; Ranganathan, S.; Zahed, H.; Freeman, A.R.; Shilbayeh, Z.; Sassy, M.; Shalaby, M.; Malik, R. Surgery for endometriosis-associated infertility: Do we exaggerate the magnitude of effect? Facts Views Vis. ObGyn 2015, 7, 109–118. [Google Scholar] [PubMed]
- Berkes, E.; Bokor, A.; Rigó, J.J.R. Az endometriosis korszerű laparoszkópos sebészi kezelése. Orv. Hetil. 2010, 151, 1137–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, X.Z.; Beguerie, J.R. Laparoscopic surgery for subfertility related to endometriosis: A meta-analysis. Taiwan. J. Obstet. Gynecol. 2014, 53, 303–308. [Google Scholar] [CrossRef] [Green Version]
- Parasar, P.; Ozcan, P.; Terry, K.L. Endometriosis: Epidemiology, Diagnosis and Clinical Management. Curr. Obstet. Gynecol. Rep. 2017, 6, 34–41. [Google Scholar] [CrossRef] [Green Version]
- D’Hooge, T.; Debrock, S.; Hill, J.; Meuleman, C. Endometriosis and subfertility: Is the relationship resolved? Semin. Reprod. Med. 2003, 21, 243–254. [Google Scholar] [CrossRef]
- Nnoaham, K.E.; Hummelshoj, L.; Webster, P.; D’Hooghe, T.; De Cicco Nardone, F.; De Cicco Nardone, C.; Jenkinson, C.; Kennedy, S.H.; Zondervan, K.T.; World Endometriosis Research Foundation Global Study of Women’s Health Consortium. Impact of endometriosis on quality of life and work productivity: A multicentre study across ten countries. Fertil. Steril. 2011, 96, 366–373. [Google Scholar] [CrossRef] [Green Version]
- Nezhat, C.; Nezhat, F.; Nezhat, C. Endometriosis: Ancient disease, ancient treatments. Fertil. Steril. 2012, 98 (Suppl. S6), S1–S62. [Google Scholar] [CrossRef]
- Garai, J.; Molnar, V.; Varga, T.; Koppan, M.; Torok, A.; Bodis, J. Endometriosis: Harmful survival of an ectopic tissue. Front. Biosci. 2006, 11, 595–619. [Google Scholar] [CrossRef] [Green Version]
- Senapati, S.; Barnhart, K. Managing endometriosis-associated infertility. Clin. Obstet. Gynecol. 2011, 54, 720–726. [Google Scholar] [CrossRef] [Green Version]
- Sampson, J. Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am. J. Obstet. Gynecol. 1927, 14, 422–469. [Google Scholar] [CrossRef]
- Yeung, P.P., Jr.; Shwayder, J.; Pasic, R.P. Laparoscopic management of endometriosis: Comprehensive review of best evidence. J. Minim. Invasive Gynecol. 2009, 16, 269–281. [Google Scholar] [CrossRef]
- Macer, M.L.; Taylor, H.S. Endometriosis and infertility: A review of the pathogenesis and treatment of endometriosis-associated infertility. Obstet. Gynecol. Clin. 2012, 39, 535–549. [Google Scholar] [CrossRef] [Green Version]
- Shifren, J.L.; Tseng, J.F.; Zaloudek, C.J.; Ryan, I.P.; Meng, Y.G.; Ferrara, N.; Jaffe, R.B.; Taylor, R.N. Ovarian steroid regulation of vascular endothelial growth factor in human endometrium: Implication for angiogenesis during the menstrual cycle and in the pathogenesis of endometriosis. J. Clin. Endocrinol. Metab. 1996, 81, 3112–3118. [Google Scholar] [CrossRef] [Green Version]
- Burney, R.O.; Giudice, L.C. Pathogenesis and pathophysiology of endometriosis. Fertil. Steril. 2012, 98, 511–519. [Google Scholar] [CrossRef] [Green Version]
- Burney, R.; Talbi, S.; Hamilton, A. Gene expression analysis of endometrium reveals progesterone resistance and candidate susceptibility genes in women with endometriosis. Endocrinology 2007, 148, 3814–3826. [Google Scholar] [CrossRef] [Green Version]
- Holoch, K.J.; Lessey, B.A. Endometriosis and infertility. Clin. Obstet. Gynecol. 2010, 53, 429–438. [Google Scholar] [CrossRef]
- Nakahara, K.; Saito, H.; Saito, T.; Ito, M.; Ohta, N.; Sakai, N.; Tezuka, N.; Hiroi, M.; Watanabe, H. Incidence of apoptotic bodies in membrana granulosa of the patients participating in an in vitro fertilization program. Fertil. Steril. 1997, 67, 302–308. [Google Scholar] [CrossRef]
- Rock, J.A. The revised American Fertility Society classification of endometriosis: Reproducibility of scoring. Fertil. Steril. 1995, 63, 1108–1110. [Google Scholar] [CrossRef]
- Piva, M.; Horrowitz, G.; Sharpe-Timms, K.L. Interleukin-6 differentially stimulates haptoglobin production by peritoneal and endometriotic cells in vitro: A model for endometrial peritoneal interaction in endometriosis. J. Clin. Endocrinol. Metab. 2001, 2386, 2553–2561. [Google Scholar] [CrossRef]
- Lebovic, D.I.; Mueller, M.D.; Taylor, R.N. Immunobiology of endometriosis. Fertil. Steril. 2001, 75, 1–10. [Google Scholar] [CrossRef]
- Fadhlaoui, A.; Bouquet de la Jolinière, J.; Feki, A. Endometriosis and infertility: How and when to treat? Front. Surg. 2014, 1, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morassutto, C.; Monasta, L.; Ricci, G.; Barbone, F.; Ronfani, L. Incidence and estimated prevalence of endometriosis and adenomyosis in Northeast Italy: A data linkage study. PLoS ONE 2016, 11, e0154227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Hooghe, T.M.; Mihalyi, A.M.; Simsa, P.; Kyama, C.K.; Peeraer, K.; De Loecker, P.; Meeuwis, L.; Segal, L.; Meuleman, C. Why we need a noninvasive diagnostic test for minimal to mild endometriosis with a high sensitivity. Gynecol. Obstet. Investig. 2006, 62, 136–138. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, V.H.; Weil, C.; Chodick, G.; Shalev, V. Epidemiology of endometriosis: A large population-based database study from a healthcare provider with 2 million members. BJOG 2018, 125, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Sreekanth, A. Role of diagnostic laparoscopy and hysteroscopy in infertility. J. Evol. Med. Dent. Sci. 2017, 6, 2590–2596. [Google Scholar] [CrossRef]
- Godinjak, Z.; Idrizbegović, E. Should diagnostic hysteroscopy be a routine procedure during diagnostic laparoscopy in infertile women? Bosn. J. Basic Med. Sci. 2008, 8, 44–47. [Google Scholar] [CrossRef] [Green Version]
- Mascarenhas, M.N.; Flaxman, S.R.; Boerma, T.; Vanderpoel, S.; Stevens, G.A. National, regional, and global trends in infertility prevalence since 1990: A systematic analysis of 277 health surveys. PLoS Med. 2012, 9, e1001356. [Google Scholar] [CrossRef]
- Cui, W. Mother or nothing: The agony of infertility. Bull. World Health Organ. 2010, 88, 881–882. [Google Scholar] [CrossRef]
- Chachamovich, J.R.; Chachamovich, E.; Ezer, H.; Fleck, M.P.; Knauth, D.; Passos, E.P. Investigating quality of life and health-related quality of life in infertility: A systematic review. J. Psychosom. Obstet. Gynaecol. 2010, 31, 101–110. [Google Scholar] [CrossRef]
- Batt, R.E. A History of Endometriosis; Springer: London, UK, 2011; pp. 13–38. [Google Scholar]
- Jacobson, T.Z.; Duffy, J.M.N.; Barlow, D.; Farquhar, C.; Koninckx, P.R.; Olive, D. Laparoscopic surgery for subfertility associated with endometriosis. Cochrane Database Syst. Rev. 2002, 4, CD001398. [Google Scholar] [CrossRef]
- Marcoux, S.; Maheux, R.; Bérubé, S. Laparoscopic surgery in infertile women with minimal or mild endometriosis. Canadian Collaborative Group on Endometriosis. N. Eng. J. Med. 1997, 337, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Farquhar, C.; Rishworth, J.R.; Brown, J.; Nelen, W.L.M.; Marjoribanks, J. Assisted reproductive technology: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2018, 7, CD010537. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, F.; Raynal, P.; Salama, S.; Guillot, E.; Le Tohic, A.; Chis, C.; Panel, P. Reproductive outcome after laparoscopic treatment of endometriosis in infertile population. J. Gynecol. Obstet. Biol. Reprod. 2007, 36, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Snowden, E.U.; Jarrett, J.C.; Dawood, M.Y. Comparison of diagnostic accuracy of laparoscopy, hysteroscopy, and hysterosalpingography in evaluation of female infertility. Fertil. Steril. 1984, 41, 709–713. [Google Scholar] [CrossRef]
- Kennedy, S.; Bergqvist, A.; Chapron, C.; D’Hooghe, T.; Dunselman, G.; Greb, R.; Hummelshoj, L.; Prentice, A.; Saridogan, E.; ESHRE Special Interest Group for Endometriosis and Endometrium Guideline Development Group. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum. Reprod. 2005, 20, 2698–2704. [Google Scholar] [CrossRef]
- Kuivasaari, P.; Hippeläinen, M.; Anttila, M.; Heinonen, S. Effect of endometriosis on IVF/ICSI outcome: Stage III/IV endometriosis worsens cumulative pregnancy and live-born rates. Hum. Reprod. 2005, 20, 3130–3135. [Google Scholar] [CrossRef] [Green Version]
- Słabuszewska-Jóźwiak, A.; Ciebiera, M.; Baran, A.; Jakiel, G. Effectiveness of laparoscopic surgeries in treating infertility related to endometriosis. Ann. Agric. Environ. Med. 2015, 22, 329–331. [Google Scholar] [CrossRef] [Green Version]
- Nardo, G.L.; Moustafa, M.; Beynon, D.W.G. Laparoscopic treatment of pelvic pain associated with minimal and mild endometriosis with use of the Helica Thermal Coagulator. Fertil. Steril. 2005, 83, 735–738. [Google Scholar] [CrossRef]
- Ozkan, S.; Murk, W.; Arici, A. Endometriosis and infertility: Epidemiology and evidence-based treatments. Ann. N. Y. Acad. Sci. 2008, 11, 92–100. [Google Scholar] [CrossRef] [Green Version]
- Vineet, V.M.; Rashmi, A.G.; Rohina, A.; Sumesh, C.; Urmila, S.; Ushma, P. Prevalence; characteristics and management of endometriosis amongst infertile women: A one-year retrospective study. J. Clin. Diagn. Res. 2015, 9, QC01–QC03. [Google Scholar] [CrossRef]
- Trajkovic, S.P.; Popović, J.; Antić, V.; Radović, D.; Stefanović, M.; Vukomanović, P. Stages of endometriosis: Does it affect in vitro fertilization outcome. Taiwan. J. Obstet. Gynecol. 2015, 54, 224–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moini, A.; Bahar, L.; Ashrafinia, M.; Eslami, B.; Hosseini, R.; Ashrafinia, N. Fertility outcome after operative laparoscopy versus no treatment in infertile women with minimal or mild endometriosis. Int. J. Fertil. Steril. 2012, 5, 235–240. [Google Scholar] [PubMed]
- Zhang, E.; Zhang, Y.; Fang, L.; Li, Q.; Gu, J. Combined hysterolaparoscopy for the diagnosis of female infertility: A retrospective study of 132 patients in China. Mater. Socio Med. 2014, 26, 156–157. [Google Scholar] [CrossRef] [PubMed]
- Rantala, M.L. Causes and outcome of infertility in previously unexplained couples. Acta Obstet. Gynecol. Scand. 1988, 67, 429–432. [Google Scholar] [CrossRef] [PubMed]
- Bérubé, S.; Marcoux, S.; Langevin, M.; Maheux, R. Fecundity of infertile women with minimal or mild endometriosis and women with unexplained infertility. Fertil. Steril. 1998, 69, 1034–1041. [Google Scholar] [CrossRef]
- Bulletti, C.; Coccia, M.E.; Battistoni, S.; Borini, A. Endometriosis and infertility. J. Assist. Reprod. Genet. 2010, 27, 441–447. [Google Scholar] [CrossRef]
- Nesbitt-Hawes, E.M.; Campbell, N.; Maley, P.E.; Won, H.; Hooshmand, D.; Henry, A.; Ledger, W.; Abbott, J.A. The Surgical Treatment of Severe Endometriosis Positively Affects the Chance of Natural or Assisted Pregnancy Postoperatively. Biomed. Res. Int. 2015, 2015, 438790. [Google Scholar] [CrossRef] [Green Version]
- Alborzi, S.; Hosseini-Nohadani, A.; Poordast, T.; Shomali, Z. Surgical outcomes of laparoscopic endometriosis surgery: A 6-year experience. Curr. Med. Res. Opin. 2017, 33, 2229–2234. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Category | Total (n = 455) | No Pregnancy (n = 85) | Pregnancy (n = 370) | Chi2 Test | |||
|---|---|---|---|---|---|---|---|---|
| N | (Col.%) | N | (Row%) | N | (Row%) | p | ||
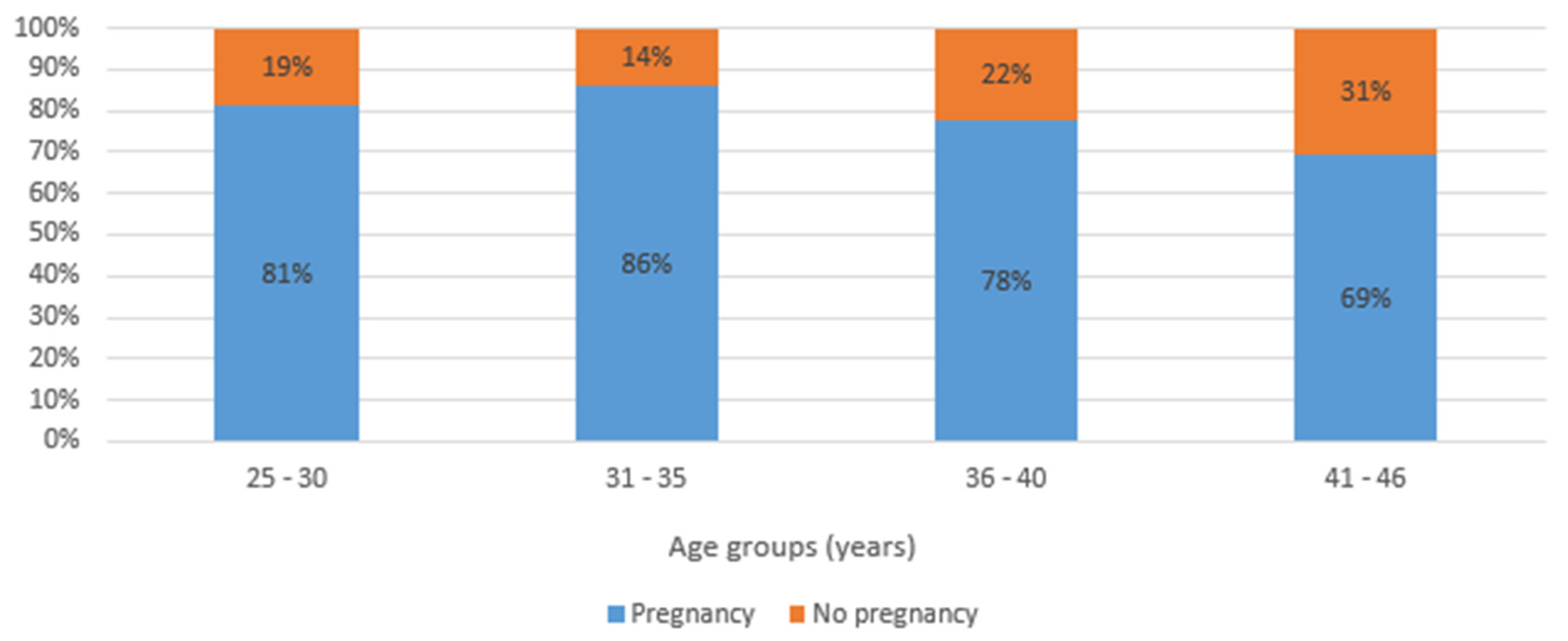
| Age (years) | 25-30 | 91 | (20.0%) | 17 | (18.7%) | 74 | (81.3%) | 0.099 |
| 31-35 | 179 | (39.3%) | 25 | (14.0%) | 154 | (86.0%) | ||
| 36-40 | 159 | (35.0%) | 35 | (22.0%) | 124 | (78.0%) | ||
| 41-46 | 26 | (5.7%) | 8 | (30.8%) | 18 | (69.2%) | ||
| Length of menstrual cycle (days) | ≤ 24 | 93 | (20.4%) | 18 | (19.4%) | 75 | (80.6%) | 0.409 |
| 25-35 | 338 | (74.3%) | 65 | (19.2%) | 273 | (80.8%) | ||
| 36+ | 24 | (5.3%) | 2 | (8.3%) | 22 | (91.7%) | ||
| Length of menstruation (days) | <4 | 125 | (27.5%) | 18 | (14.4%) | 107 | (85.6%) | 0.318 |
| 5-6 | 219 | (48.1%) | 46 | (21.0%) | 173 | (79.0%) | ||
| 7+ | 111 | (24.4%) | 21 | (18.9%) | 90 | (81.1%) | ||
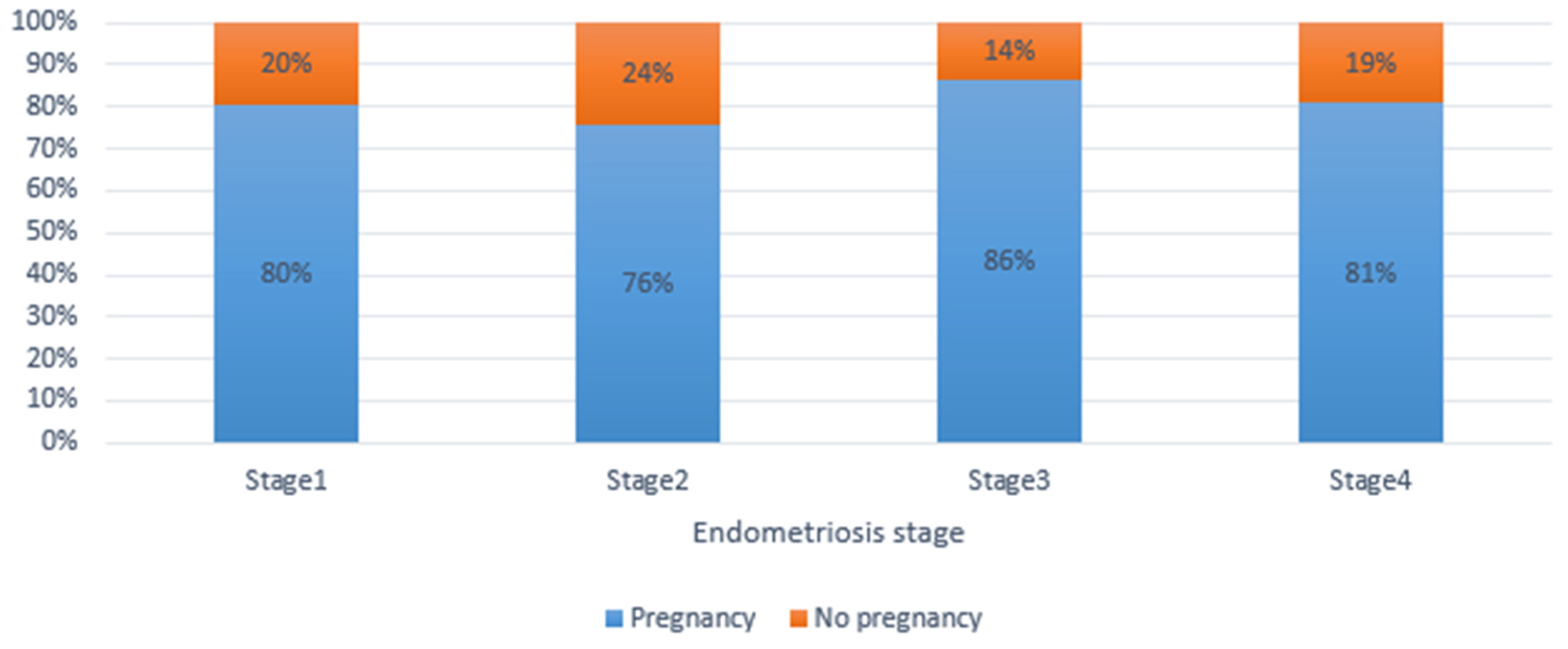
| Stage of endometriosis | 1 | 61 | (13.4%) | 12 | (19.7%) | 49 | (80.3%) | 0.138 |
| 2 | 132 | (29.0%) | 32 | (24.2%) | 100 | (75.8%) | ||
| 3 | 162 | (35.6%) | 22 | (13.6%) | 140 | (86.4%) | ||
| 4 | 100 | (22.0%) | 19 | (19.0%) | 81 | (81.0%) | ||
| Characteristics | Category | Total (n = 455) | No Pregnancy (n = 85) | Pregnancy (n = 370) | Chi2 Test |
|---|---|---|---|---|---|
| N (Col%) | N (Row%) | N (Row%) | p | ||
| Causes of infertility | Idiopathic factor | 213 (46.8%) | 38 (17.8%) | 175 (82.2%) | 0.001 |
| Female factor | 198 (43.5%) | 30 (15.2%) | 168 (84.8%) | ||
| Both parties | 44 (9.7%) | 17 (38.6%) | 27 (61.4%) | ||
| Duration of infertility (years) | 1–3 years | 339 (74.5%) | 61 (18.0%) | 278 (82.0%) | 0.343 |
| 4–6 years | 71 (15.6%) | 12 (16.9%) | 59 (83.1%) | ||
| >6 years | 45 (9.9%) | 12 (26.7%) | 33 (73.3%) | ||
| Tubal function | Normal tubal function | 239 (52.6%) | 47 (19.6%) | 193 (80.4%) | 0.497 |
| Normal right tubal function | 10 (2.2%) | 0 (0.0%) | 10 (100.0%) | ||
| Normal left tubal function | 3 (0.7%) | 0 (0.0%) | 3 (100.0%) | ||
| Both tubes blocked | 20 (4.4%) | 3 (15.0%) | 17 (85.0%) | ||
| Normal tube after adhsiolysis | 182 (40.1%) | 35 (19.2%) | 147 (80.8%) | ||
| Type of infertility | Primary infertility | 319 (70.1%) | 53 (16.6%) | 266 (83.4%) | 0.083 |
| Secondary infertility | 136 (29.9%) | 32 (23.5%) | 104 (76.5%) | ||
| Anatomical abnormalities | Adenofibroma | 80 (18.2%) | 17 (21.3%) | 63 (78.8%) | 0.469 |
| Endonmetrial polyp | 28 (6.4%) | 6 (18.8%) | 26 (81.3%) | ||
| Septum uteri/malformation | 39 (8.9%) | 6 (15.4%) | 33 (84.6%) | ||
| Ashermann/synechia | 5 (1.1%) | 1 (20.0%) | 4 (80.0%) | ||
| Chronic PID | 9 (2.0%) | 1 (11.1%) | 8 (88.9%) | ||
| Ovarium cyst | 1 (0.2%) | 1 (100.0%) | 0 (0.0%) | ||
| Scar defect (Niche) | 6 (1.4%) | 0 (0.0%) | 6 (100.0%) | ||
| No | 272 (61.8%) | 52 (19.6%) | 220 (80.9%) |
| Preoperative ART Treatment | Postoperative ART Treatment | No Pregnancy | Pregnancy | Total |
|---|---|---|---|---|
| N (Row%) | N (Row %) | N | ||
| No | No | 15 (16.3%) | 77 (83.7%) | 92 |
| Yes | 6 (13.6%) | 38 (86.4%) | 44 | |
| Total | 21 (15.4%) | 115 (84.6%) | 136 | |
| Yes | No | 14 (25.9%) | 40 (74.1%) | 54 |
| Yes | 7 (8.8%) | 73 (91.2%) | 80 | |
| Total | 21 (15.7%) | 113 (84.3%) | 134 | |
| Total | 42 (15.6%) | 228 (84.4%) | 270 | |
| Preoperative ART Treatment | Postoperative ART Treatment | No Pregnancy | Pregnancy | Total |
|---|---|---|---|---|
| N (Row%) | N (Row %) | N | ||
| No | No | 11 (42.3%) | 15 (57.7%) | 26 |
| Yes | 3 (16.7%) | 15 (83.3%) | 18 | |
| Total | 14 (31.8%) | 30 (68.2%) | 44 | |
| Yes | No | 14 (26.4%) | 39 (73.6%) | 53 |
| Yes | 15 (17.0%) | 73 (83.0%) | 88 | |
| Total | 29 (20.6%) | 112 (79.4%) | 141 | |
| Total | 43 (23.2%) | 142 (76.8%) | 185 | |
| Type of Laparoscopic Surgical Procedures Undertaken | No Pregnancy | Pregnancy | Total | ||
|---|---|---|---|---|---|
| N | (Row%) | N | (Row%) | ||
| CO2 laser not used | 29 | (16.8%) | 144 | (83.2%) | 173 |
| CO2 lazer evaporation technique used | 13 | (24.1%) | 41 | (75.9%) | 54 |
| Electrocoagulation excision of deep infiltrating endometriosis lesions & adhesiolysis | 6 | (20.7%) | 23 | (79.3%) | 29 |
| Electrocoagulation excision of superficial peritoneal & deep infiltrating lesion & endometrioma stripping& adhesiolysis | 13 | (13.7%) | 82 | (86.3%) | 95 |
| Cauterisation of bilateral ovarian endometriosis & Electrocoagulation excision of superficial peritoneal & deep infiltrating lesion & adhesiolysis | 2 | (16.7%) | 10 | (83.3%) | 12 |
| Endometrioma stripping & Adhesiolysis & Cauterisation of ovary endometriosis | 10 | (23.8%) | 32 | (76.2%) | 42 |
| Electrocoagulation excision of superficial peritoneal lesion & adhesiolysis | 2 | (28.6%) | 5 | (71.4%) | 7 |
| Electrocoagulation excision of superficial peritoneal & deep infiltrating lesion & adhesiolysis | 12 | (27.9%) | 31 | (72.1%) | 43 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ekine, A.A.; Fülöp, I.; Tekse, I.; Rúcz, Á.; Jeges, S.; Koppán, Á.; Koppán, M. The Surgical Benefit of Hysterolaparoscopy in Endometriosis-Related Infertility: A Single Centre Retrospective Study with a Minimum 2-Year Follow-Up. J. Clin. Med. 2020, 9, 507. https://doi.org/10.3390/jcm9020507
Ekine AA, Fülöp I, Tekse I, Rúcz Á, Jeges S, Koppán Á, Koppán M. The Surgical Benefit of Hysterolaparoscopy in Endometriosis-Related Infertility: A Single Centre Retrospective Study with a Minimum 2-Year Follow-Up. Journal of Clinical Medicine. 2020; 9(2):507. https://doi.org/10.3390/jcm9020507
Chicago/Turabian StyleEkine, Atombosoba Adokiye, István Fülöp, István Tekse, Árpád Rúcz, Sara Jeges, Ágnes Koppán, and Miklós Koppán. 2020. "The Surgical Benefit of Hysterolaparoscopy in Endometriosis-Related Infertility: A Single Centre Retrospective Study with a Minimum 2-Year Follow-Up" Journal of Clinical Medicine 9, no. 2: 507. https://doi.org/10.3390/jcm9020507