Impact of Simultaneous Consideration of Cardiac and Vascular Function on Long-Term All-Cause and Cardiovascular Mortality

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethics Statement
2.3. Echocardiographic Evaluation
2.4. Measurement of baPWV
2.5. Collection of Medical and Demographic Data
2.6. Definition of all-cause and CV mortality
2.7. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: Executive summary: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. J. Am. Coll. Cardiol. 2013, 128, 1810–1852. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Ferranti, S., de; Despres, J.P.; Fullerton, H.J.; Howard, V.J.; et al. Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation 2015, 131, 434–441. [Google Scholar] [CrossRef]
- Levy, W.C.; Mozaffarian, D.; Linker, D.T.; Sutradhar, S.C.; Anker, S.D.; Cropp, A.B.; Anand, I.; Maggioni, A.; Burton, P.; Sullivan, M.D.; et al. The Seattle Heart Failure Model: Prediction of survival in heart failure. Circulation 2006, 113, 1424–1433. [Google Scholar] [CrossRef] [PubMed]
- Pocock, S.J.; Ariti, C.A.; McMurray, J.J.; Maggioni, A.; Kober, L.; Squire, I.B.; Swedberg, K.; Dobson, J.; Poppe, K.K.; Whalley, G.A.; et al. Predicting survival in heart failure: A risk score based on 39,372 patients from 30 studies. Eur. Heart J. 2013, 34, 1404–1413. [Google Scholar] [CrossRef] [PubMed]
- Ouwerkerk, W.; Voors, A.A.; Zwinderman, A.H. Factors influencing the predictive power of models for predicting mortality and/or heart failure hospitalization in patients with heart failure. JACC Heart Fail. 2014, 2, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, K.; Bennett, D.; Conrad, N.; Williams, T.M.; Basu, J.; Dwight, J.; Woodward, M.; Patel, A.; McMurray, J.; MacMahon, S. Risk prediction in patients with heart failure: A systematic review and analysis. JACC Heart Fail. 2014, 2, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Breathett, K.; Allen, L.A.; Udelson, J.; Davis, G.; Bristow, M. Changes in left ventricular ejection fraction predict survival and hospitalization in heart failure with reduced ejection fraction. Circ. Heart Fail. 2016, 9, e002962. [Google Scholar] [CrossRef] [Green Version]
- Solomon, S.D.; Anavekar, N.; Skali, H.; McMurray, J.J.; Swedberg, K.; Yusuf, S.; Granger, C.B.; Michelson, E.L.; Wang, D.; Pocock, S.; et al. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation 2005, 112, 3738–3744. [Google Scholar] [CrossRef] [Green Version]
- St John Sutton, M.; Pfeffer, M.A.; Moye, L.; Plappert, T.; Rouleau, J.L.; Lamas, G.; Rouleau, J.; Parker, J.O.; Arnold, M.O.; Sussex, B.; et al. Cardiovascular death and left ventricular remodeling two years after myocardial infarction: Baseline predictors and impact of long-term use of captopril: Information from the Survival and Ventricular Enlargement (SAVE) trial. Circulation 1997, 96, 3294–3299. [Google Scholar] [CrossRef]
- McDermott, M.M.; Feinglass, J.; Lee, P.I.; Mehta, S.; Schmitt, B.; Lefevre, F.; Gheorghiade, M. Systolic function, readmission rates, and survival among consecutively hospitalized patients with congestive heart failure. Am. Heart J. 1997, 134, 728–736. [Google Scholar] [CrossRef]
- Mosterd, A.; Cost, B.; Hoes, A.W.; de Bruijne, M.C.; Deckers, J.W.; Hofman, A.; Grobbee, D.E. The prognosis of heart failure in the general population: The Rotterdam Study. Eur. Heart J. 2001, 22, 1318–1327. [Google Scholar] [CrossRef] [PubMed]
- Imanishi, R.; Seto, S.; Toda, G.; Yoshida, M.; Ohtsuru, A.; Koide, Y.; Baba, T.; Yano, K. High brachial-ankle pulse wave velocity is an independent predictor of the presence of coronary artery disease in men. Hypertens. Res. 2004, 27, 71–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattace-Raso, F.U.; van der Cammen, T.J.; Hofman, A.; van Popele, N.M.; Bos, M.L.; Schalekamp, M.A.; Asmar, R.; Reneman, R.S.; Hoeks, A.P.; Breteler, M.M.; et al. Arterial stiffness and risk of coronary heart disease and stroke: The Rotterdam Study. Circulation 2006, 113, 657–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willum-Hansen, T.; Staessen, J.A.; Torp-Pedersen, C.; Rasmussen, S.; Thijs, L.; Ibsen, H.; Jeppesen, J. Prognostic value of aortic pulse wave velocity as index of arterial stiffness in the general population. Circulation 2006, 113, 664–670. [Google Scholar] [CrossRef]
- Asmar, R.; Benetos, A.; Topouchian, J.; Laurent, P.; Pannier, B.; Brisac, A.M.; Target, R.; Levy, B.I. Assessment of arterial distensibility by automatic pulse wave velocity measurement. Validation and clinical application studies. Hypertension 1995, 26, 485–490. [Google Scholar] [CrossRef]
- Miyano, I.; Nishinaga, M.; Takata, J.; Shimizu, Y.; Okumiya, K.; Matsubayashi, K.; Ozawa, T.; Sugiura, T.; Yasuda, N.; Doi, Y. Association between brachial-ankle pulse wave velocity and 3-year mortality in community-dwelling older adults. Hypertens. Res. 2010, 33, 678–682. [Google Scholar] [CrossRef]
- Chen, Y.; Shen, F.; Liu, J.; Yang, G.Y. Arterial stiffness and stroke: De-stiffening strategy, a therapeutic target for stroke. Stroke Vasc. Neurol. 2017, 2, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Hsu, P.C.; Lin, T.H.; Lee, C.S.; Chu, C.Y.; Su, H.M.; Voon, W.C.; Lai, W.T.; Sheu, S.H. Impact of a systolic parameter, defined as the ratio of right brachial pre-ejection period to ejection time, on the relationship between brachial-ankle pulse wave velocity and left ventricular diastolic function. Hypertens. Res. 2011, 34, 462–467. [Google Scholar] [CrossRef] [Green Version]
- Tomiyama, H.; Yamashina, A.; Arai, T.; Hirose, K.; Koji, Y.; Chikamori, T.; Hori, S.; Yamamoto, Y.; Doba, N.; Hinohara, S. Influences of age and gender on results of noninvasive brachial-ankle pulse wave velocity measurement--a survey of 12517 subjects. Atherosclerosis 2003, 166, 303–309. [Google Scholar] [CrossRef]
- Yokoyama, H.; Shoji, T.; Kimoto, E.; Shinohara, K.; Tanaka, S.; Koyama, H.; Emoto, M.; Nishizawa, Y. Pulse wave velocity in lower-limb arteries among diabetic patients with peripheral arterial disease. J. Atheroscler. Thromb. 2003, 10, 253–258. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.S.; Gona, P.; Albano, I.; Larson, M.G.; Benjamin, E.J.; Levy, D.; Kannel, W.B.; Vasan, R.S. A systematic assessment of causes of death after heart failure onset in the community: Impact of age at death, time period, and left ventricular systolic dysfunction. Circ. Heart Fail. 2011, 4, 36–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, G.L.; Masoudi, F.A.; Vaccarino, V.; Radford, M.J.; Krumholz, H.M. Outcomes in heart failure patients with preserved ejection fraction: Mortality, readmission, and functional decline. J. Am. Coll. Cardiol. 2003, 41, 1510–1518. [Google Scholar] [CrossRef] [Green Version]
- Cohn, J.N.; Johnson, G. Heart failure with normal ejection fraction. The V-HeFT Study. Veterans Administration Cooperative Study Group. Circulation 1990, 81, III48–III53. [Google Scholar] [PubMed]
- Sugahara, M.; Kagiyama, N.; Hasselberg, N.E.; Blauwet, L.A.; Briller, J.; Cooper, L.; Fett, J.D.; Hsich, E.; Wells, G.; McNamara, D.; et al. IPAC Investigators. Global Left Ventricular Strain at Presentation Is Associated with Subsequent Recovery in Patients with Peripartum Cardiomyopathy. J. Am. Soc. Echocardiogr. 2019, 32, 1565–1573. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Lu, H.; Li, L. Reduced Left Ventricular Ejection Fraction Is a Risk Factor for In-Hospital Mortality in Patients after Percutaneous Coronary Intervention: A Hospital-Based Survey. Biomed Res. Int. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, H.; Munakata, M.; Kawano, Y.; Ohishi, M.; Shoji, T.; Sugawara, J.; Tomiyama, H.; Yamashina, A.; Yasuda, H.; Sawayama, T.; et al. Comparison between carotid-femoral and brachial-ankle pulse wave velocity as measures of arterial stiffness. J. Hypertens. 2009, 27, 2022–2027. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
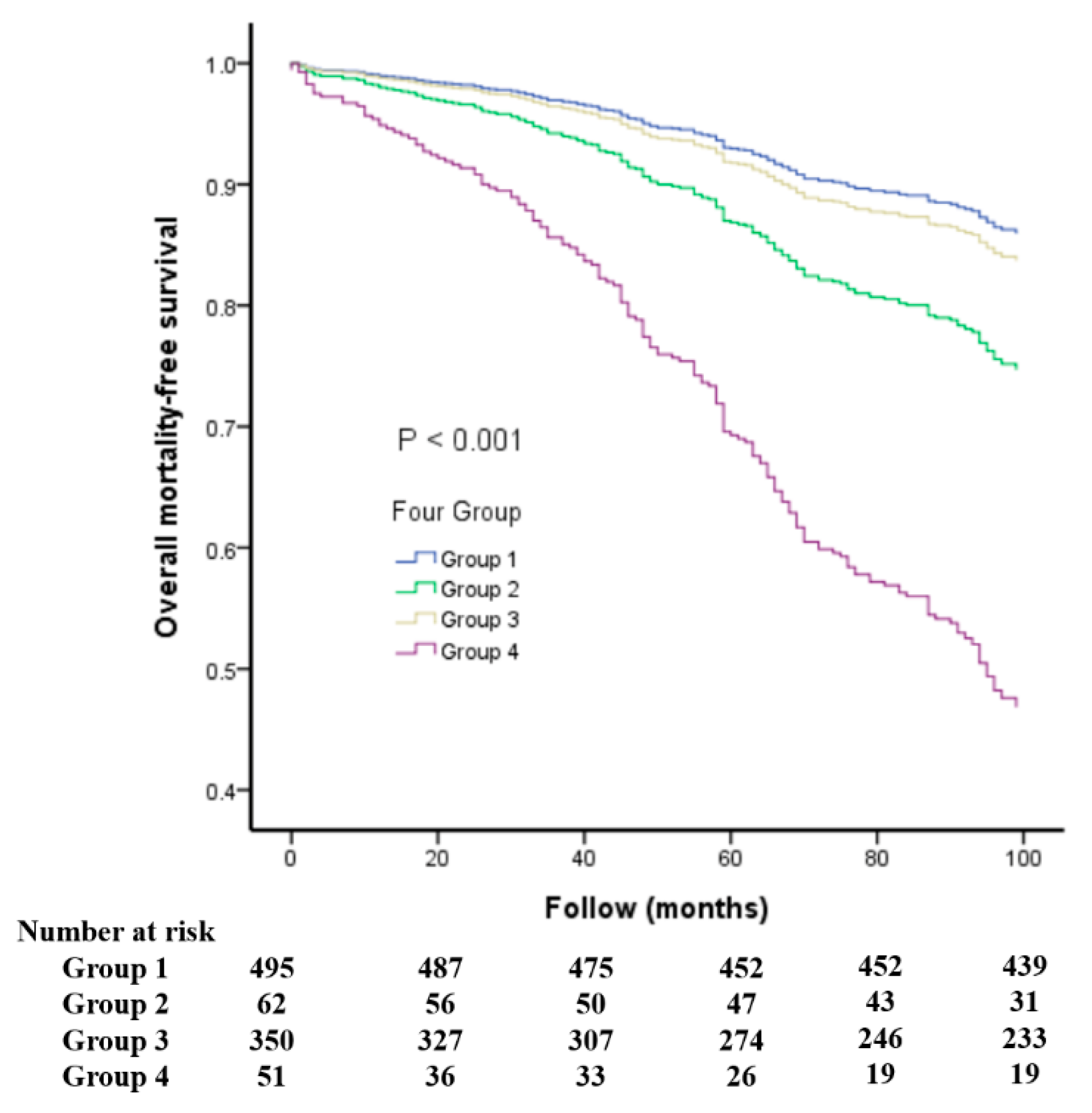
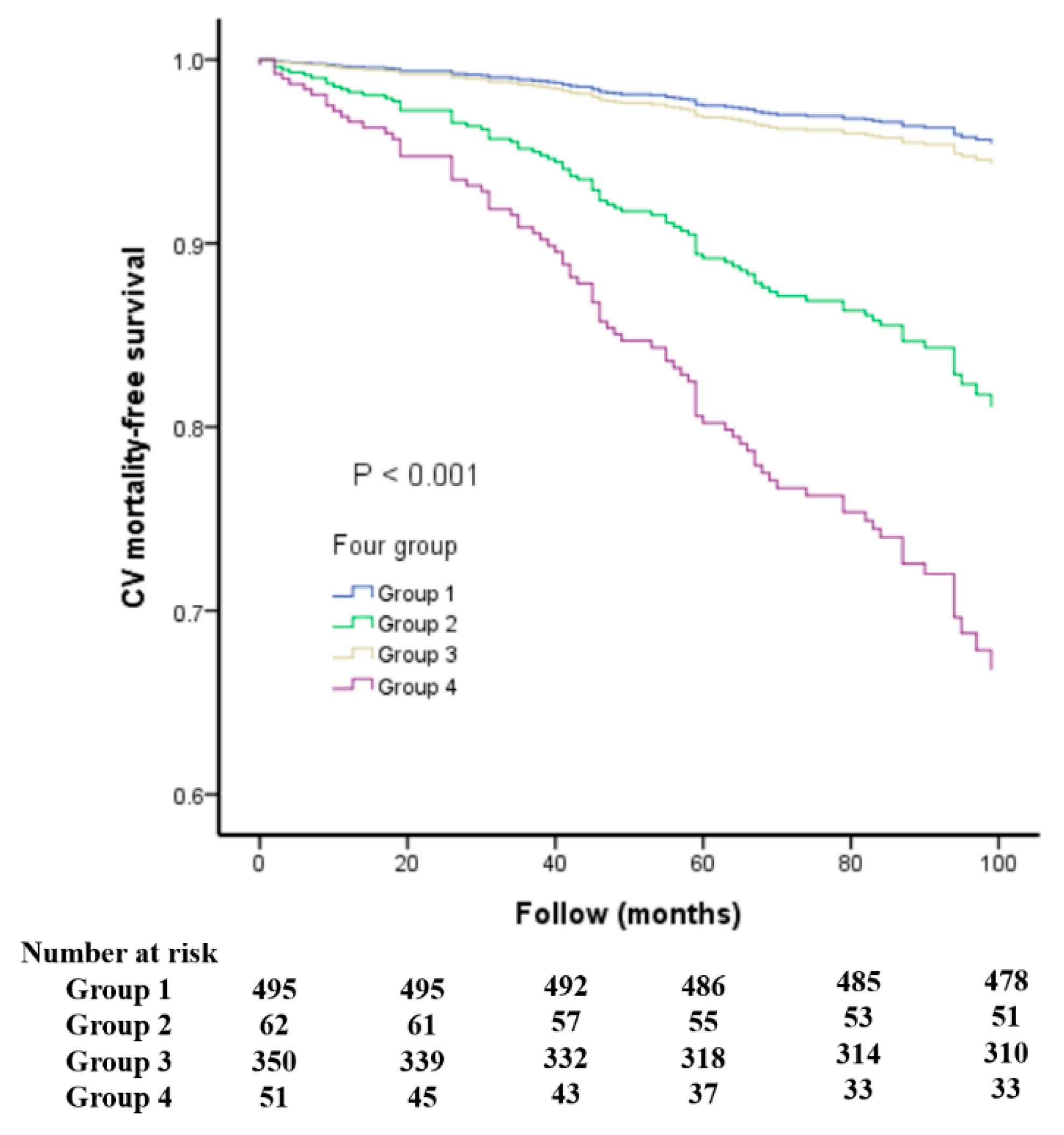
| Group1 (LVEF ≥ 50%, baPWV below the Median) | Group2 (LVEF < 50%, baPWV below the Median) | Group 3 (LVEF ≥ 50%, baPWV above the Median) | Group 4 (LVEF < 50%, baPWV above the Median) | p Value (ANOVA among Groups) | All Patients | |
|---|---|---|---|---|---|---|
| Number | 495 | 62 | 350 | 51 | 958 | |
| Age (years) | 56 ± 13 | 58 ± 16 | 70 ± 11 *,$ | 71 ± 12 *,$ | <0.001 | 62 ± 14 |
| Male Gender (%) | 59.0 | 75.4 * | 47.6 *,$ | 60.8 | <0.001 | 55.8 |
| DM (%) | 21.6 | 35.5 * | 37.7 * | 31.4 | <0.001 | 28.9 |
| CVD (%) | 20.8 | 54.8 * | 26.0 $ | 51.0 *,# | <0.001 | 26.5 |
| Mean blood pressure | 92 ± 12 | 87 ± 12 * | 103 ± 13 *,$ | 100 ± 15 *,$ | <0.001 | 96 ± 14 |
| Total cholesterol | 192 ± 39 | 176 ± 50 | 191 ± 40 | 183 ± 46 | 0.07 | 190 ± 41 |
| BMI (kg/m2) | 26.8 ± 4.0 | 26.5 ± 4.7 | 25.9 ± 3.8 * | 24.4 ± 3.5 *,$ | <0.001 | 26.3 ± 4.0 |
| Heart rate (beats/min) | 67 ± 10 | 75 ± 17 * | 70 ± 12 *,$ | 79 ± 17 *,# | <0.001 | 69 ± 12 |
| LVEF (%) | 67 ± 8 | 38 ± 9 * | 67 ± 8 $ | 38 ± 8 *,# | <0.001 | 64 ± 12 |
| baPWV (cm/s) | 1475 ± 173 | 1456 ± 178 | 2163 ± 387 *,$ | 2278 ± 668 *,$ | <0.001 | 1768 ± 466 |
| Numbers of Mortality | ||||||
| All-cause | 58 | 23 | 120 | 37 | <0.001 | 238 |
| Cardiovascular | 17 | 13 | 41 | 20 | <0.001 | 91 |
| Medications | ||||||
| Aspirin (%) | 30.2 | 47.5 * | 33.9 $ | 41.2 | 0.026 | 33.1 |
| β-blockers (%) | 40.7 | 67.2 * | 38.1 $ | 35.3 $ | <0.001 | 41.0 |
| CCBs (%) | 38.2 | 19.7 * | 46.4 *,$ | 25.5 # | <0.001 | 39.2 |
| ACEIs (%) | 5.9 | 21.3 * | 9.5 $ | 11.8 | <0.001 | 8.5 |
| ARBs (%) | 47.3 | 50.8 | 50.7 | 45.1 | 0.72 | 48.5 |
| Diuretics (%) | 24.9 | 59.0 * | 31.9 *,$ | 47.1 *,# | <0.001 | 30.7 |
| Parameter | Univariate | Multivariate (Forward) | ||
|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | |
| Age (+ 13.74 year) | 2.949 (2.494–3.486) | <0.001 | 3.159 (2.524–3.952) | <0.001 |
| Male gender (male vs. female) | 1.109 (0.852–1.444) | 0.44 | 1.573 (1.152–2.150) | 0.004 |
| Diabetes mellitus (yes vs. no) | 2.275 (1.750–2.957) | <0.001 | 2.411 (1.773–3.278) | <0.001 |
| Mean blood pressure (+13.80 mmHg) | 1.120 (0.983–1.276) | 0.09 | 1.300 (1.101–1.534) | 0.002 |
| Total cholesterol (−40.68 mg/dL) | 0.741 (0.631–0.872) | <0.001 | – | – |
| Heart rate (+12.20 beat/minute) | 1.242 (1.096–1.407) | 0.001 | – | – |
| Smoking (ever vs. no) | 0.775 (0.518–1.158) | 0.21 | ||
| Medications | ||||
| Aspirin use | 1.252 (0.954–1.642) | 0.11 | ||
| Beta blocker use | 1.037 (0.796–1.351) | 0.79 | ||
| Calcium channel blocker use | 1.127 (0.865–1.468) | 0.38 | ||
| ACEI use | 1.142 (0.736–1.773) | 0.55 | ||
| ARB use | 1.044 (0.804–1.354) | 0.75 | ||
| Diuretic use | 1.886 (1.449–2.454) | <0.001 | – | – |
| Study Group | <0.001 | <0.001 | ||
| Group 2 vs. Group 1 | 3.810 (2.307–6.292) | <0.001 | 1.954 (1.049–3.638) | 0.035 |
| Group 3 vs. Group 1 | 3.459 (2.516–4.756) | <0.001 | 1.150 (0.764–1.730) | 0.50 |
| Group 4 vs. Group 1 | 10.854 (7.014–16.797) | <0.001 | 4.693 (2.745–8.022) | <0.001 |
| Parameter | Univariate | Multivariate (Forward) | ||
|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | |
| Age (+13.74 year) | 3.035 (2.305–3.997) | <0.001 | 2.860 (2.103–3.889) | <0.001 |
| Male gender (male vs female) | 0.991 (0.647–1.516) | 0.97 | – | – |
| Diabetes mellitus (yes vs. no) | 2.727 (1.789–4.157) | <0.001 | 2.746 (1.772–4.256) | <0.001 |
| Mean blood pressure (+13.80 mmHg) | 1.208 (0.982–1.487) | 0.074 | 1.371 (1.086–1.731) | 0.008 |
| Total cholesterol (−40.68 mg/dL) | 0.774 (0.592–1.012) | 0.061 | ||
| Heart rate (+12.20 beat/minute) | 1.309 (1.073–1.598) | 0.008 | – | – |
| Smoking (ever vs. no) | 0.749 (0.388–1.448) | 0.39 | ||
| Medications | ||||
| Aspirin use | 1.318(0.852–2.039) | 0.22 | ||
| Beta blocker use | 1.271(0.834–1.938) | 0.26 | ||
| Calcium channel blocker use | 1.180(0.772–1.806) | 0.45 | ||
| ACEI use ARB use | 1.235(0.619–2.463) 1.283(0.841–1.956) | 0.55 0.25 | – | – |
| Diuretic use | 1.909(1.248–2.922) | 0.003 | – | – |
| Study Group | <0.001 | <0.001 | ||
| Group 2 vs. Group 1 | 6.612 (3.096–14.120) | <0.001 | 4.518 (2.050–9.955) | <0.001 |
| Group 3 vs. Group 1 | 3.881 (2.199–6.849) | <0.001 | 1.256 (0.661–2.387) | 0.49 |
| Group 4 vs. Group 1 | 20.443 (10.494–39.823) | <0.001 | 8.702 (4.283–17.679) | <0.001 |
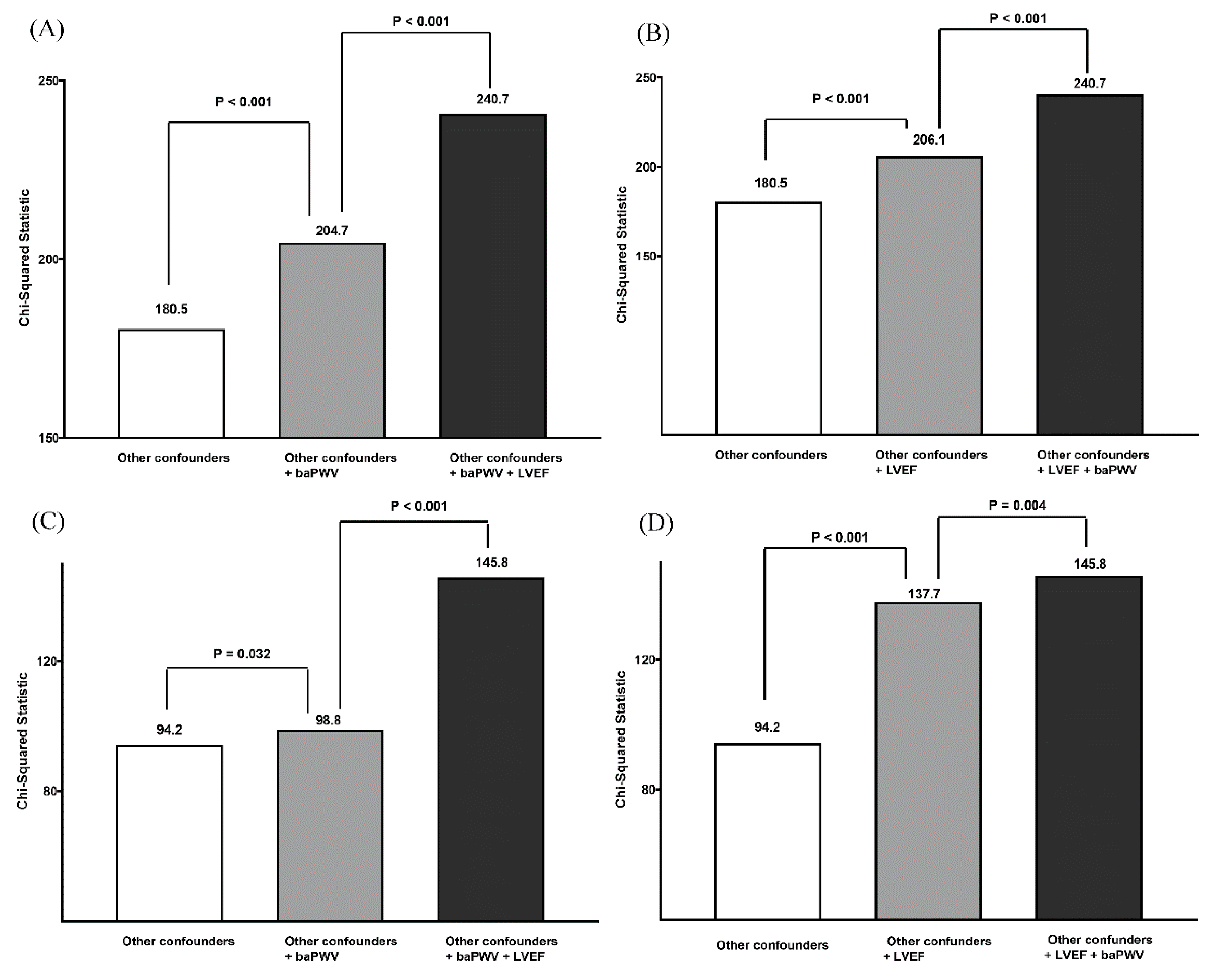
| Model | Variable | All-Cause Mortality Prediction | CV Mortality Prediction | ||
|---|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | ||
| Model 1: LVEF | LVEF | 0.648 (0.579–0.725) | <0.001 | 0.548 (0.464–0.648) | <0.001 |
| Model 2: LVEF + other confounders | LVEF | 0.655 (0.565–0.758) | <0.001 | 0.510 (0.423–0.614) | <0.001 |
| Model 3: baPWV | baPWV | 1.886 (1.713–2.076) | <0.001 | 1.831 (1.556–2.154) | <0.001 |
| Model 4: baPWV + other confounders | baPWV | 1.573 (1.356–1.825) | <0.001 | 1.272 (1.029–1.571) | 0.026 |
| Model 5: Other confounders + LVEF + baPWV | baPWV LVEF | 1.640(1.416–1.899) 0.628(0.541–0.729) | <0.001 <0.001 | 1.462 (1.205–1.774) 0.507 (0.422–0.609) | <0.001 <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, P.-C.; Lee, W.-H.; Tsai, W.-C.; Chu, C.-Y.; Chen, Y.-C.; Lee, M.-K.; Lin, T.-H.; Lee, C.-S.; Voon, W.-C.; Lai, W.-T.; et al. Impact of Simultaneous Consideration of Cardiac and Vascular Function on Long-Term All-Cause and Cardiovascular Mortality. J. Clin. Med. 2019, 8, 2145. https://doi.org/10.3390/jcm8122145
Hsu P-C, Lee W-H, Tsai W-C, Chu C-Y, Chen Y-C, Lee M-K, Lin T-H, Lee C-S, Voon W-C, Lai W-T, et al. Impact of Simultaneous Consideration of Cardiac and Vascular Function on Long-Term All-Cause and Cardiovascular Mortality. Journal of Clinical Medicine. 2019; 8(12):2145. https://doi.org/10.3390/jcm8122145
Chicago/Turabian StyleHsu, Po-Chao, Wen-Hsien Lee, Wei-Chung Tsai, Chun-Yuan Chu, Ying-Chih Chen, Meng-Kuang Lee, Tsung-Hsien Lin, Chee-Siong Lee, Wen-Chol Voon, Wen-Ter Lai, and et al. 2019. "Impact of Simultaneous Consideration of Cardiac and Vascular Function on Long-Term All-Cause and Cardiovascular Mortality" Journal of Clinical Medicine 8, no. 12: 2145. https://doi.org/10.3390/jcm8122145