Serum Level and Activity of Butylcholinesterase: A Biomarker for Post-Stroke Dementia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Clinical Information
2.3. Sample Preparation for Activities Assay, Protein Assay, and Genotyping Assay
2.4. Cholinesterase Activities Assay
2.5. Plasma AChE and BChE Protein Assay
2.6. Functional Single Nucleotide Polymorphisms in AChE, BChE, and APOE
2.7. Statistics
3. Results
3.1. Characteristics of Patients with Ischemic Stroke
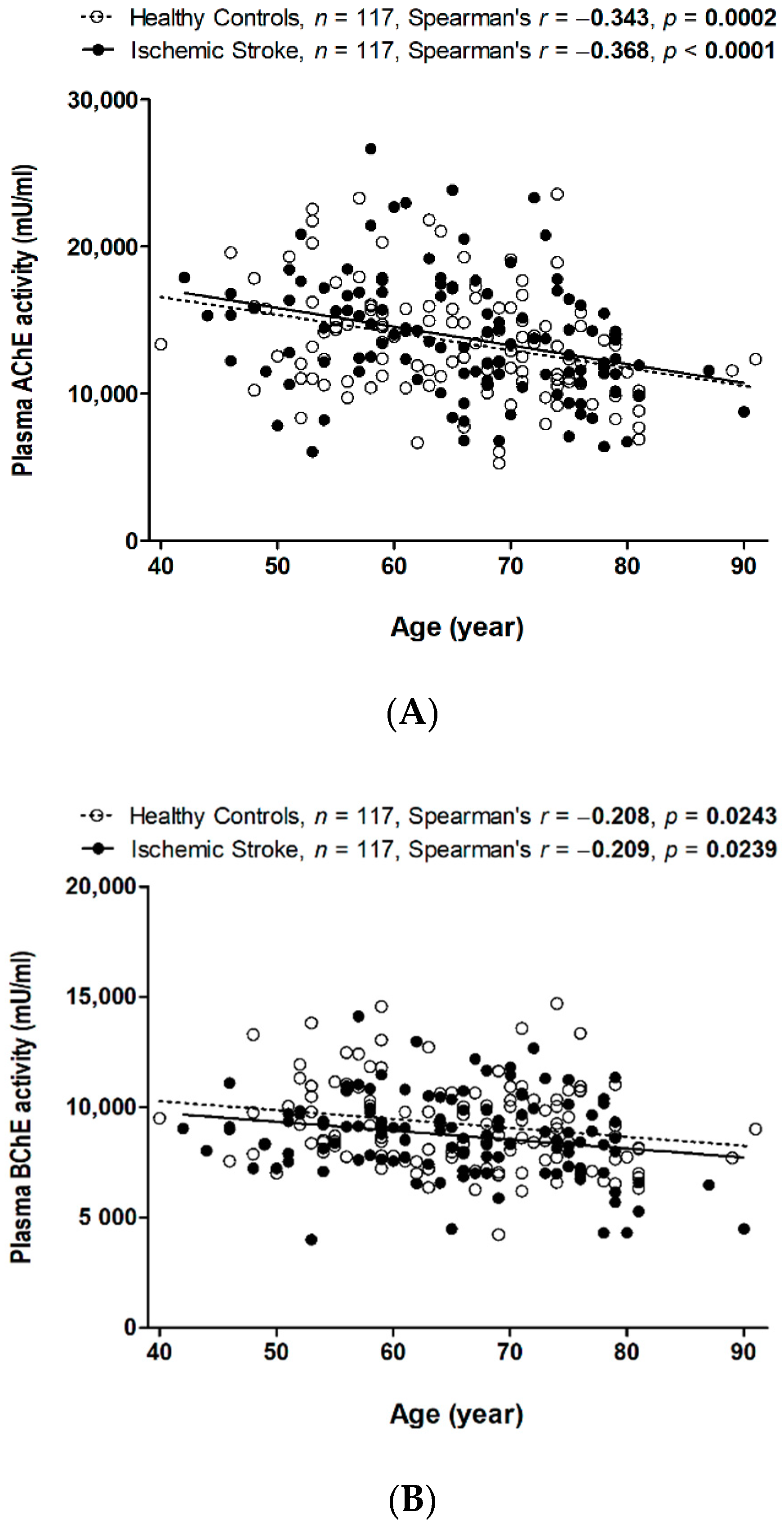
3.2. Decreased Plasma AChE and BChE Activity with Aging in Patients with and without Stroke
3.3. Genetic Influences of Functional SNPs on AChE and BChE in Ischemic Stroke
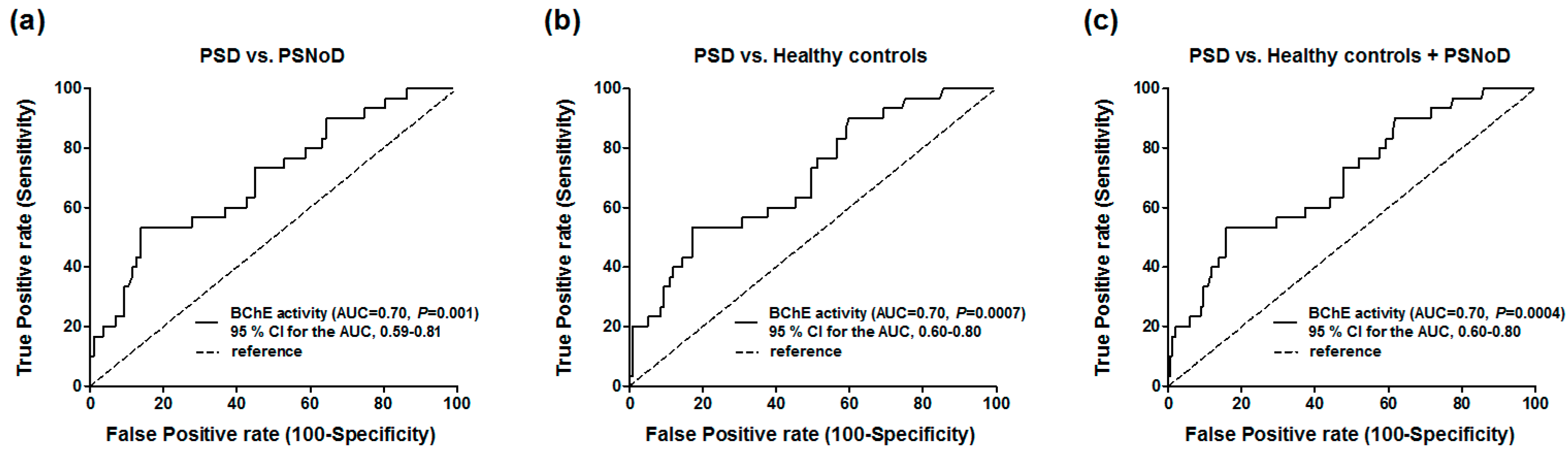
3.4. Optimal Cut-off Point Calculated by Receiver Operating Characteristic Curve (ROC) Analysis for PSD Diagnosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dichgans, M.; Leys, D. Vascular Cognitive Impairment. Circ. Res. 2017, 120, 573–591. [Google Scholar] [CrossRef]
- Mijajlovic, M.D.; Pavlovic, A.; Brainin, M.; Heiss, W.D.; Quinn, T.J.; Ihle-Hansen, H.B.; Hermann, D.M.; Assayag, E.B.; Richard, E.; Thiel, A.; et al. Post-stroke dementia—A comprehensive review. BMC Med. 2017, 15, 11. [Google Scholar] [CrossRef] [PubMed]
- Posada-Duque, R.A.; Barreto, G.E.; Cardona-Gomez, G.P. Protection after stroke: Cellular effectors of neurovascular unit integrity. Front. Cell Neurosci. 2014, 8, 231. [Google Scholar] [CrossRef] [PubMed]
- Snowdon, D.A.; Greiner, L.H.; Mortimer, J.A.; Riley, K.P.; Greiner, P.A.; Markesbery, W.R. Brain infarction and the clinical expression of Alzheimer disease. The Nun Study. JAMA 1997, 277, 813–817. [Google Scholar] [CrossRef] [PubMed]
- Roman, G.C.; Kalaria, R.N. Vascular determinants of cholinergic deficits in Alzheimer disease and vascular dementia. Neurobiol. Aging 2006, 27, 1769–1785. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.P. Transcultural expression of subcortical vascular disease. J. Neurol. Sci. 2004, 226, 45–47. [Google Scholar] [CrossRef]
- Dubois, M.F.; Hebert, R. The incidence of vascular dementia in Canada: A comparison with Europe and East Asia. Neuroepidemiology 2001, 20, 179–187. [Google Scholar] [CrossRef]
- Taly, A.; Corringer, P.J.; Guedin, D.; Lestage, P.; Changeux, J.P. Nicotinic receptors: Allosteric transitions and therapeutic targets in the nervous system. Nat. Rev. Drug Discov. 2009, 8, 733–750. [Google Scholar] [CrossRef]
- Akaike, A.; Takada-Takatori, Y.; Kume, T.; Izumi, Y. Mechanisms of neuroprotective effects of nicotine and acetylcholinesterase inhibitors: Role of alpha4 and alpha7 receptors in neuroprotection. J. Mol. Neurosci. 2010, 40, 211–216. [Google Scholar] [CrossRef]
- Zivkovic, A.R.; Schmidt, K.; Sigl, A.; Decker, S.O.; Brenner, T.; Hofer, S. Reduced serum butyrylcholinesterase activity indicates severe systemic inflammation in critically ill patients. Mediat. Inflamm. 2015, 2015, 274607. [Google Scholar] [CrossRef]
- Tracey, K.J. The inflammatory reflex. Nature 2002, 420, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Santos Samary, C.; Pelosi, P.; Leme Silva, P.; Rieken Macedo Rocco, P. Immunomodulation after ischemic stroke: Potential mechanisms and implications for therapy. Crit. Care 2016, 20, 391. [Google Scholar] [CrossRef] [PubMed]
- Ben Assayag, E.; Shenhar-Tsarfaty, S.; Ofek, K.; Soreq, L.; Bova, I.; Shopin, L.; Berg, R.M.; Berliner, S.; Shapira, I.; Bornstein, N.M.; et al. Serum cholinesterase activities distinguish between stroke patients and controls and predict 12-month mortality. Mol. Med. 2010, 16, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Roman, G.C. Cholinergic dysfunction in vascular dementia. Curr. Psychiatry Rep. 2005, 7, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Tohgi, H.; Abe, T.; Kimura, M.; Saheki, M.; Takahashi, S. Cerebrospinal fluid acetylcholine and choline in vascular dementia of Binswanger and multiple small infarct types as compared with Alzheimer-type dementia. J. Neural Transm. 1996, 103, 1211–1220. [Google Scholar] [CrossRef] [PubMed]
- Whyte, E.M.; Lenze, E.J.; Butters, M.; Skidmore, E.; Koenig, K.; Dew, M.A.; Penrod, L.; Mulsant, B.H.; Pollock, B.G.; Cabacungan, L.; et al. An open-label pilot study of acetylcholinesterase inhibitors to promote functional recovery in elderly cognitively impaired stroke patients. Cerebrovasc. Dis. 2008, 26, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, N.; Asanuma, M.; Tanaka, K.; Hirata, H.; Kondo, Y.; Goto, M.; Kawauchi, M.; Ogura, T. Long-term time course of regional changes in cholinergic indices following transient ischemia in the spontaneously hypertensive rat brain. Brain Res. 1996, 712, 60–68. [Google Scholar] [CrossRef]
- Lin, Y.T.; Wu, P.H.; Chen, C.S.; Yang, Y.H.; Yang, Y.H. Association between acetylcholinesterase inhibitors and risk of stroke in patients with dementia. Sci. Rep. 2016, 6, 29266. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.C.; Chou, W.H.; Tsou, H.H.; Fang, C.P.; Liu, T.H.; Tsao, H.H.; Hsu, W.C.; Weng, Y.C.; Wang, Y.; Liu, Y.L. A Post-hoc Study of D-Amino Acid Oxidase in Blood as an Indicator of Post-stroke Dementia. Front. Neurol. 2019, 10, 402. [Google Scholar] [CrossRef]
- Qian, L.; Ding, L.; Cheng, L.; Zhu, X.; Zhao, H.; Jin, J.; Guan, D.; Zhang, B.; Chen, X.; Xu, Y. Early biomarkers for post-stroke cognitive impairment. J. Neurol. 2012, 259, 2111–2118. [Google Scholar] [CrossRef]
- Kliper, E.; Bashat, D.B.; Bornstein, N.M.; Shenhar-Tsarfaty, S.; Hallevi, H.; Auriel, E.; Shopin, L.; Bloch, S.; Berliner, S.; Giladi, N.; et al. Cognitive decline after stroke: Relation to inflammatory biomarkers and hippocampal volume. Stroke 2013, 44, 1433–1435. [Google Scholar] [CrossRef]
- Rothenburg, L.S.; Herrmann, N.; Swardfager, W.; Black, S.E.; Tennen, G.; Kiss, A.; Gladstone, D.J.; Ween, J.; Snaiderman, A.; Lanctot, K.L. The relationship between inflammatory markers and post stroke cognitive impairment. J. Geriatr. Psychiatry Neurol. 2010, 23, 199–205. [Google Scholar] [CrossRef]
- Narasimhalu, K.; Lee, J.; Leong, Y.L.; Ma, L.; De Silva, D.A.; Wong, M.C.; Chang, H.M.; Chen, C. Inflammatory markers and their association with post stroke cognitive decline. Int. J. Stroke Offi. J. Int. Stroke Soc. 2015, 10, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, H.Y.; Tang, X.C. Cholinergic deficiency involved in vascular dementia: Possible mechanism and strategy of treatment. Acta Pharmacol. Sin. 2009, 30, 879–888. [Google Scholar] [CrossRef] [PubMed]
- Roman, G.C.; Tatemichi, T.K.; Erkinjuntti, T.; Cummings, J.L.; Masdeu, J.C.; Garcia, J.H.; Amaducci, L.; Orgogozo, J.M.; Brun, A.; Hofman, A.; et al. Vascular dementia: Diagnostic criteria for research studies. Report of the NINDS-AIREN International Workshop. Neurology 1993, 43, 250–260. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet. Med. A J. Br. Diabet. Assoc. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- Schoenborn, C.A.; Adams, P.E. Health behaviors of adults: United States, 2005–2007. Vital Health Stat. Ser. 10 Data Natl. Health Surv. 2010, 245, 132. [Google Scholar]
- Coupland, C.A.C.; Hill, T.; Dening, T.; Morriss, R.; Moore, M.; Hippisley-Cox, J. Anticholinergic Drug Exposure and the Risk of Dementia: A Nested Case-Control Study. JAMA Intern. Med. 2019. [Google Scholar] [CrossRef]
- Valle, A.M.; Radic, Z.; Rana, B.K.; Mahboubi, V.; Wessel, J.; Shih, P.A.; Rao, F.; O’Connor, D.T.; Taylor, P. Naturally occurring variations in the human cholinesterase genes: Heritability and association with cardiovascular and metabolic traits. J. Pharmacol. Exp. Ther. 2011, 338, 125–133. [Google Scholar] [CrossRef]
- Lockridge, O.; Norgren, R.B., Jr.; Johnson, R.C.; Blake, T.A. Naturally Occurring Genetic Variants of Human Acetylcholinesterase and Butyrylcholinesterase and Their Potential Impact on the Risk of Toxicity from Cholinesterase Inhibitors. Chem. Res. Toxicol. 2016, 29, 1381–1392. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, P.; Pramesh, C.S.; Aggarwal, R. Common pitfalls in statistical analysis: Logistic regression. Perspect. Clin. Res. 2017, 8, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.A.; Maltby, S.; Plank, M.W.; Kluge, M.; Nilsson, M.; Foster, P.S.; Walker, F.R. Peripheral immune cells infiltrate into sites of secondary neurodegeneration after ischemic stroke. Brain Behav. Immun. 2018, 67, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Famakin, B.M. The Immune Response to Acute Focal Cerebral Ischemia and Associated Post-stroke Immunodepression: A Focused Review. Aging Dis. 2014, 5, 307–326. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Conner, J.M.; Nagahara, A.H.; Tuszynski, M.H. Rehabilitation drives enhancement of neuronal structure in functionally relevant neuronal subsets. Proc. Natl. Acad. Sci. USA 2016, 113, 2750–2755. [Google Scholar] [CrossRef] [Green Version]
- Shytle, R.D.; Mori, T.; Townsend, K.; Vendrame, M.; Sun, N.; Zeng, J.; Ehrhart, J.; Silver, A.A.; Sanberg, P.R.; Tan, J. Cholinergic modulation of microglial activation by alpha 7 nicotinic receptors. J. Neurochem. 2004, 89, 337–343. [Google Scholar] [CrossRef]
- Wang, H.; Yu, M.; Ochani, M.; Amella, C.A.; Tanovic, M.; Susarla, S.; Li, J.H.; Wang, H.; Yang, H.; Ulloa, L.; et al. Nicotinic acetylcholine receptor alpha7 subunit is an essential regulator of inflammation. Nature 2003, 421, 384–388. [Google Scholar] [CrossRef]
- Furukawa, S.; Sameshima, H.; Yang, L.; Ikenoue, T. Activation of acetylcholine receptors and microglia in hypoxic-ischemic brain damage in newborn rats. Brain Dev. 2013, 35, 607–613. [Google Scholar] [CrossRef]
- Kalappa, B.I.; Sun, F.; Johnson, S.R.; Jin, K.; Uteshev, V.V. A positive allosteric modulator of alpha7 nAChRs augments neuroprotective effects of endogenous nicotinic agonists in cerebral ischaemia. Br. J. Pharmacol. 2013, 169, 1862–1878. [Google Scholar] [CrossRef]
- Kavirajan, H.; Schneider, L.S. Efficacy and adverse effects of cholinesterase inhibitors and memantine in vascular dementia: A meta-analysis of randomised controlled trials. Lancet Neurol. 2007, 6, 782–792. [Google Scholar] [CrossRef]
- Farooq, M.U.; Min, J.; Goshgarian, C.; Gorelick, P.B. Pharmacotherapy for Vascular Cognitive Impairment. CNS Drugs 2017, 31, 759–776. [Google Scholar] [CrossRef] [PubMed]
- Malouf, R.; Birks, J. Donepezil for vascular cognitive impairment. Cochrane Database Syst. Rev. 2004. [Google Scholar] [CrossRef] [PubMed]
- Birks, J.; McGuinness, B.; Craig, D. Rivastigmine for vascular cognitive impairment. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erkinjuntti, T.; Kurz, A.; Gauthier, S.; Bullock, R.; Lilienfeld, S.; Damaraju, C.V. Efficacy of galantamine in probable vascular dementia and Alzheimer’s disease combined with cerebrovascular disease: A randomised trial. Lancet 2002, 359, 1283–1290. [Google Scholar] [CrossRef]
- Auchus, A.P.; Brashear, H.R.; Salloway, S.; Korczyn, A.D.; De Deyn, P.P.; Gassmann-Mayer, C.; Group, G.-I.-S. Galantamine treatment of vascular dementia: A randomized trial. Neurology 2007, 69, 448–458. [Google Scholar] [CrossRef]
- Gorelick, P.B.; Scuteri, A.; Black, S.E.; Decarli, C.; Greenberg, S.M.; Iadecola, C.; Launer, L.J.; Laurent, S.; Lopez, O.L.; Nyenhuis, D.; et al. Vascular contributions to cognitive impairment and dementia: A statement for healthcare professionals from the american heart association/american stroke association. Stroke 2011, 42, 2672–2713. [Google Scholar] [CrossRef]
- Debette, S.; Beiser, A.; DeCarli, C.; Au, R.; Himali, J.J.; Kelly-Hayes, M.; Romero, J.R.; Kase, C.S.; Wolf, P.A.; Seshadri, S. Association of MRI markers of vascular brain injury with incident stroke, mild cognitive impairment, dementia, and mortality: The Framingham Offspring Study. Stroke 2010, 41, 600–606. [Google Scholar] [CrossRef]
- Hankey, G.J.; Ford, A.H.; Yi, Q.; Eikelboom, J.W.; Lees, K.R.; Chen, C.; Xavier, D.; Navarro, J.C.; Ranawaka, U.K.; Uddin, W.; et al. Effect of B vitamins and lowering homocysteine on cognitive impairment in patients with previous stroke or transient ischemic attack: A prespecified secondary analysis of a randomized, placebo-controlled trial and meta-analysis. Stroke 2013, 44, 2232–2239. [Google Scholar] [CrossRef]
- Arbel, Y.; Shenhar-Tsarfaty, S.; Waiskopf, N.; Finkelstein, A.; Halkin, A.; Revivo, M.; Berliner, S.; Herz, I.; Shapira, I.; Keren, G.; et al. Decline in serum cholinesterase activities predicts 2-year major adverse cardiac events. Mol. Med. 2014, 20, 38–45. [Google Scholar] [CrossRef]
- Santarpia, L.; Grandone, I.; Contaldo, F.; Pasanisi, F. Butyrylcholinesterase as a prognostic marker: A review of the literature. J. Cachexia Sarcopenia Muscle 2013, 4, 31–39. [Google Scholar] [CrossRef]
- Dong, M.X.; Xu, X.M.; Hu, L.; Liu, Y.; Huang, Y.J.; Wei, Y.D. Serum Butyrylcholinesterase Activity: A Biomarker for Parkinson’s Disease and Related Dementia. BioMed Res. Int. 2017, 2017, 1524107. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Tsao, H.H.; Chu, Y.C.; Wang, J.J.; Lee, J.D.; Chang, P.Y.; Hsu, W.C. Exploring the Spectrum of Subcortical Hyperintensities and Cognitive Decline. J. Neuropsychiatry Clin. Neurosci. 2018, 30, 130–138. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Healthy Controls | Ischemic Stroke | p-Value |
|---|---|---|---|
| n, Mean ± SD | n, Mean ± SD | ||
| Age | 117, 65.48 ± 10.07 | 117, 65.60 ± 10.11 | 0.89 |
| Gender | 1.00 | ||
| Female | 43 (36.75%) | 43 (36.75%) | |
| Male | 74 (63.25%) | 74 (63.25%) | |
| Education duration (years) | 4, 12.50 ± 4.73 | 109, 7.39 ± 4.30 | 0.040 |
| HTN | 0.010 | ||
| No | 50 (43.48%) | 32 (27.35%) | |
| Yes | 65 (56.52%) | 85 (72.65%) | |
| DM | 0.0006 | ||
| No | 90 (78.26%) | 67 (57.26%) | |
| Yes | 25 (21.74%) | 50 (42.74%) | |
| Alcohol drinking | 0.42 | ||
| No | 103 (88.03%) | 97 (84.35%) | |
| Yes | 14 (11.97%) | 18 (15.65%) | |
| Smoking | 0.009 | ||
| No | 100 (85.47%) | 82 (71.30%) | |
| Yes | 17 (14.53%) | 33 (28.70%) | |
| CDR | - | 117, 0.32 ± 0.61 | - |
| 30-day MRS | - | 117, 0.98 ± 1.02 | - |
| Post-stroke dementia (%) | - | 30, 25.64% | - |
| Stroke subtypes | - | ||
| Lacunar infarction | - | 75 (64.10%) | |
| Atherothrombotic infarction | - | 42 (35.90%) | |
| Anticholinergic drugs | 0.21 | ||
| No | 102 (87.18%) | 95 (81.20%) | |
| Yes | 15 (12.82%) | 22 (18.80%) | |
| Plasma AChE (pg/mL) | 67, 1271.41 ± 292.19 | 73, 1245.73 ± 404.16 | 0.28 |
| Plasma BChE (ng/mL) | 76, 3822.30 ± 782.08 | 76, 3731.58 ± 682.61 | 0.42 |
| ChE activity (mU/mL) | 117, 22,723.16 ± 4974.9 | 117, 22,549.4 ± 5321 | 0.84 |
| BChE activity (mU/mL) | 117, 9240.96 ± 1979.02 | 117, 8711.68 ± 1875.64 | 0.12 |
| AChE activity (mU/mL) | 117, 13,482.21 ± 3738.36 | 117, 13,837.72 ± 4072.74 | 0.47 |
| APOE e4 carrier | 18 (16.51%) | 12 (11.43%) | 0.28 |
| Variable | PSNoD | PSD | Unadjusted/Adjusted p-Value |
|---|---|---|---|
| n, Mean ± SD | n, Mean ± SD | ||
| Age | 87, 62.98 ± 9.23 | 30, 73.20 ± 8.68 | <0.0001 |
| Sex | 0.67 | ||
| Female | 31 (35.63%) | 12 (40.00%) | |
| Male | 56 (64.37%) | 18 (60.00%) | |
| Education (years) | 80, 8.74 ± 3.56 | 29, 3.69 ± 4.05 | <0.0001/<0.0001 1 |
| HTN | 0.0001/0.96 1 | ||
| No | 32 (36.78%) | 0 (0.00%) | |
| Yes | 55 (63.22%) | 30 (100.00%) | |
| DM | 0.027/0.14 1 | ||
| No | 55 (63.22%) | 12 (40.00%) | |
| Yes | 32 (36.78%) | 18 (60.00%) | |
| Alcohol drinking | 0.86/0.25 1 | ||
| No | 72 (84.71%) | 25 (83.33%) | |
| Yes | 13 (15.29%) | 5 (16.67%) | |
| Smoking | 0.45/0.84 1 | ||
| No | 59 (69.41%) | 23 (76.67%) | |
| Yes | 26 (30.59%) | 7 (23.33%) | |
| 30- day MRS | 87, 0.76 ± 0.75 | 30, 1.63 ± 1.38 | 0.0013/0.003 1 |
| Post-stroke time (years) | 87, 2.15 ± 2.98 | 30, 2.79 ± 2.90 | 0.17/0.84 1 |
| CDR | 87, 0.03 ± 0.12 | 30, 1.15 ± 0.70 | <0.0001/<0.0001 1 |
| Stroke subtypes | 0.32 / 0.42 1 | ||
| Lacunar infarction | 58 (66.67%) | 17 (56.67%) | |
| Atherothrombotic infarction | 29 (33.33%) | 13 (43.33%) | |
| Anticholinergic drugs | 0.004 | ||
| No | 76 (87.36%) | 19 (63.33%) | |
| Yes | 11 (12.64%) | 11 (36.67%) | |
| Plasma AChE (pg/mL) | 56, 1279.02 ± 428.62 | 17, 1136.07 ± 294.71 | 0.28/0.16 2 |
| Plasma BChE (ng/mL) | 59, 3855.74 ± 677.60 | 17, 3300.66 ± 515.35 | 0.0033/0.025 2 |
| ChE activity (mU/mL) | 87, 23,579.08 ± 5251.55 | 30, 19,563.33 ± 4366.03 | 0.0008/0.014 2 |
| BChE activity (mU/mL) | 87, 9077.72 ± 1727.28 | 30, 7650.17 ± 1912.29 | 0.0012/0.002 2 |
| AChE activity (mU/mL) | 87, 14,501.36 ± 4197.17 | 30, 11,913.17 ± 2992.42 | 0.0029/0.08 2 |
| APOE e4 carrier | 10 (12.99%) | 2 (7.14%) | 0.41/0.48 1 |
| Gene/SNP | Healthy Controls | Ischemic Stroke | p-Value | ||
|---|---|---|---|---|---|
| n | (%) | n | (%) | ||
| AChE/rs1799806 | 0.037 | ||||
| GG | 93 | (85.32%) | 75 | (71.43%) | |
| GC | 16 | (14.68%) | 29 | (27.62%) | |
| CC | 0 | (0.00%) | 1 | (0.95%) | |
| BChE/rs1803274 | 0.063 | ||||
| CC | 92 | (84.40%) | 77 | (73.33%) | |
| CT | 16 | (14.68%) | 28 | (26.67%) | |
| TT | 1 | (0.92%) | 0 | (0.00%) | |
| APOE type | 0.242 | ||||
| ε3/ε3 | 77 | (70.64%) | 84 | (80.00%) | |
| ε3/ε4 | 14 | (12.84%) | 12 | (11.43%) | |
| ε2/ε3 | 14 | (12.84%) | 9 | (8.57%) | |
| ε4/ε4 | 3 | (2.75%) | 0 | (0.00%) | |
| ε1/ε3 or ε2/ε4 | 1 | (0.92%) | 0 | (0.00%) | |
| APOE ε4 | 0.28 | ||||
| non-carriers | 91 | (83.49%) | 93 | (88.57%) | |
| carriers | 18 | (16.51%) | 12 | (11.43%) | |
| Group | rs1803274 Genotype | n | Mean ± SD | p-Value | |
|---|---|---|---|---|---|
| Group | rs1803274 | ||||
| Healthy controls | CC | 92 | 9416.40 ± 1884.43 | 0.098 | 0.027 |
| CT | 16 | 7721.56 ±1582.06 | |||
| TT | 1 | 7753.00 | |||
| Ischemic Stroke | CC | 77 | 8708.75 ± 1708.44 | ||
| CT | 28 | 8473.50 ± 1993.10 | |||
| TT | 0 | - | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-C.; Chou, W.-H.; Fang, C.-P.; Liu, T.-H.; Tsou, H.-H.; Wang, Y.; Liu, Y.-L. Serum Level and Activity of Butylcholinesterase: A Biomarker for Post-Stroke Dementia. J. Clin. Med. 2019, 8, 1778. https://doi.org/10.3390/jcm8111778
Chen Y-C, Chou W-H, Fang C-P, Liu T-H, Tsou H-H, Wang Y, Liu Y-L. Serum Level and Activity of Butylcholinesterase: A Biomarker for Post-Stroke Dementia. Journal of Clinical Medicine. 2019; 8(11):1778. https://doi.org/10.3390/jcm8111778
Chicago/Turabian StyleChen, Yi-Chun, Wen-Hai Chou, Chiu-Ping Fang, Tung-Hsia Liu, Hsiao-Hui Tsou, Yun Wang, and Yu-Li Liu. 2019. "Serum Level and Activity of Butylcholinesterase: A Biomarker for Post-Stroke Dementia" Journal of Clinical Medicine 8, no. 11: 1778. https://doi.org/10.3390/jcm8111778