Acute Kidney Injury and Septic Shock—Defined by Updated Sepsis-3 Criteria in Critically Ill Patients

 ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
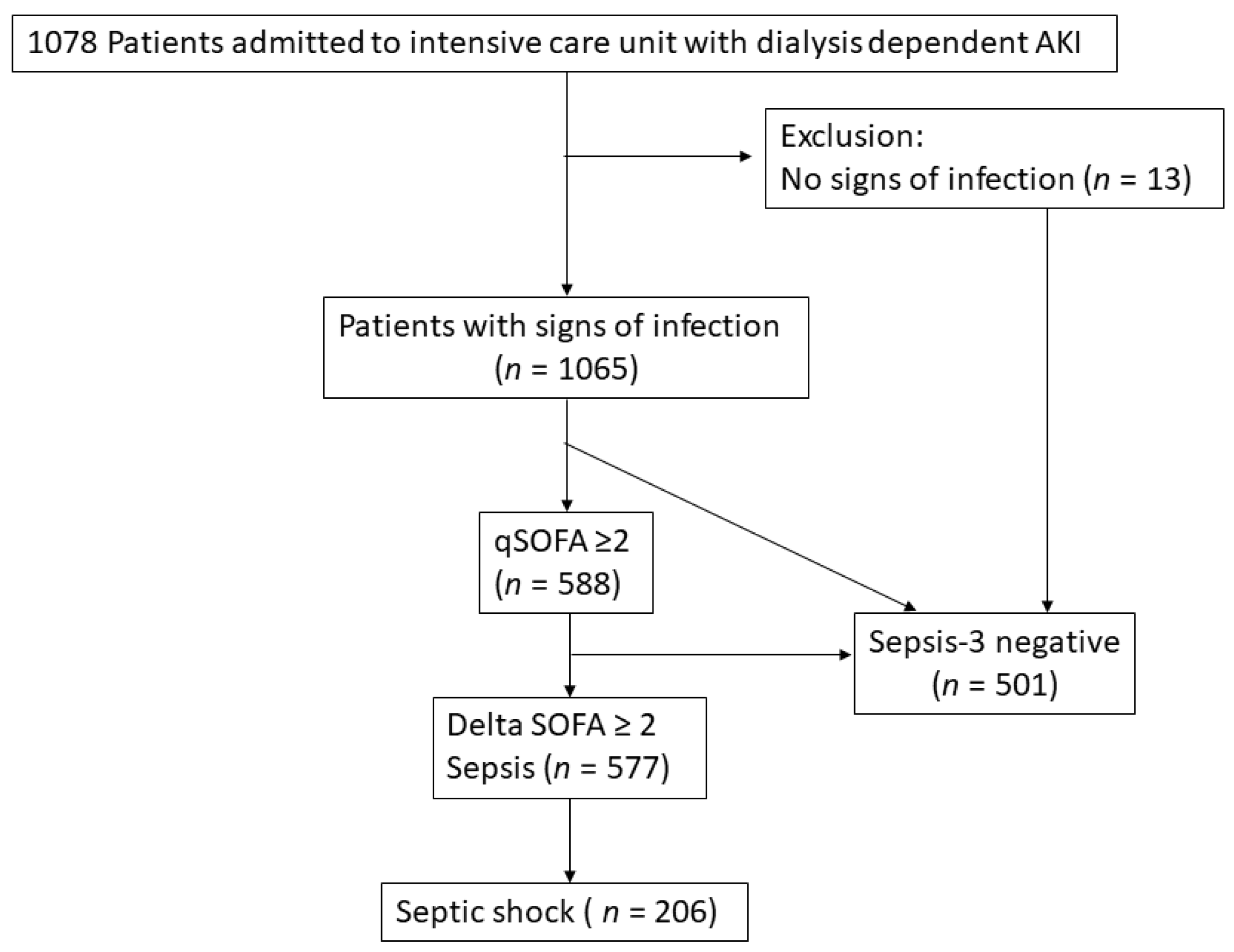
2.1. Study Population
2.2. Dialysis Initiation
2.3. Infection and Sepsis
2.4. Outcomes
2.5. Clinical Data Collection
2.6. Statistical Analyses
3. Results
3.1. Patient Cohort
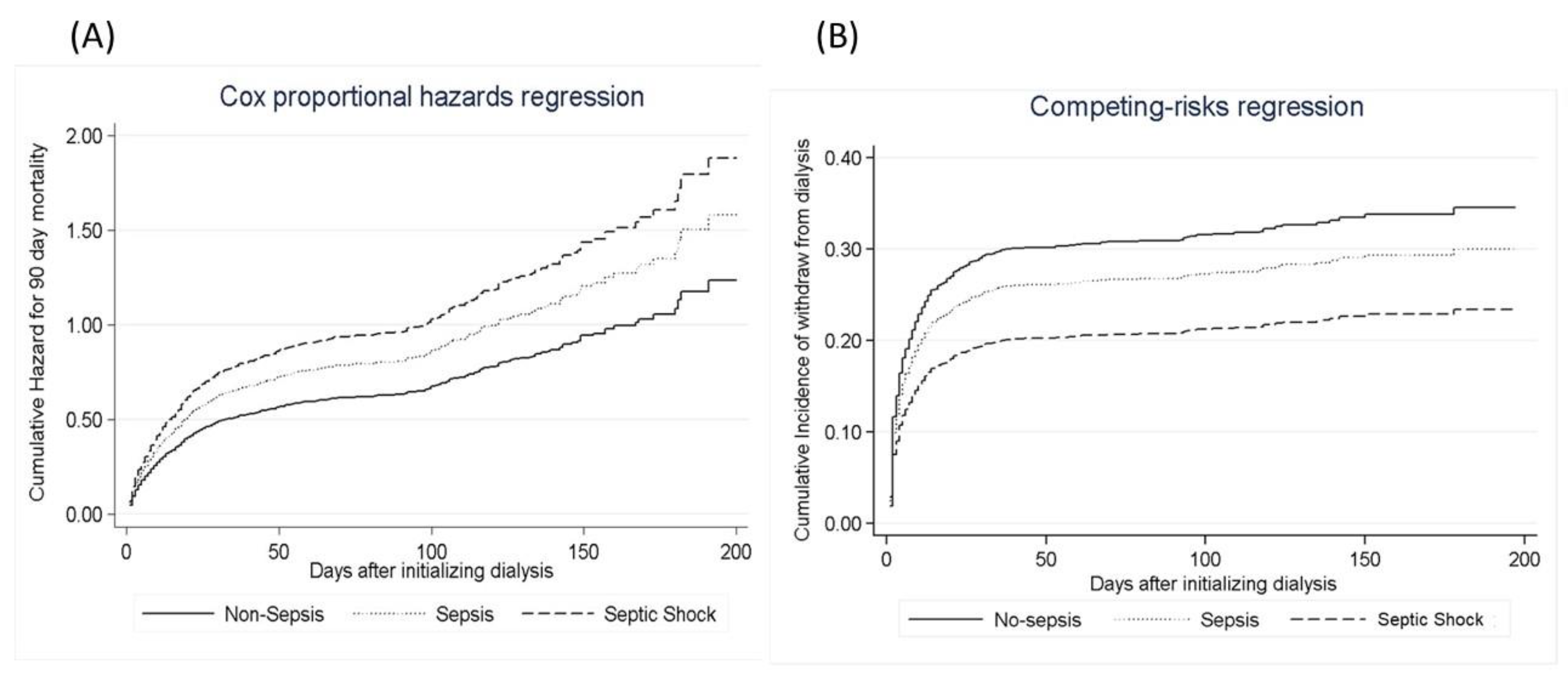
3.2. Impact of Sepsis
3.3. Comparison between 90-Day Survivors and Non-Survivors
3.4. Sepsis-3 Criteria versus 90-Day Outcomes
3.5. Sepsis per Sepsis-3 Criteria versus the Risk of Dialysis Dependence
3.6. Evaluation of Sepsis-3 Criteria in Combination with AKI Risk Prediction Score and SOFA Score versus the 90 Days Mortality
4. Discussion
4.1. Association of Mortality and Non-Recovery from Dialysis
4.2. Sepsis-3 Criteria and Outcome
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| APACHEII | Acute Physiology and Chronic Health Evaluation II |
| AKI | acute kidney injury |
| AKI-D | acute kidney injury with dialysis |
| MODS | multiple organ dysfunction syndrome |
| qSOFA | quick Sequential Organ Failure Assessment |
| RRT | renal replacement therapy |
| SOFA | Sequential Organ Failure Assessment |
| ICU | intensive care units |
References
- Hoste, E.A.; Bagshaw, S.M.; Bellomo, R.; Cely, C.M.; Colman, R.; Cruz, D.N.; Edipidis, K.; Forni, L.G.; Gomersall, C.D.; Govil, D.; et al. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensive Care Med. 2015, 41, 1411–1423. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.; Dantes, R.; Epstein, L.; Murphy, D.J.; Seymour, C.W.; Iwashyna, T.J.; Kadri, S.S.; Angus, D.C.; Danner, R.L.; Fiore, A.E.; et al. Incidence and Trends of Sepsis in US Hospitals Using Clinical vs Claims Data, 2009–2014. JAMA 2017, 318, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; McCulloch, C.E.; Fan, D.; Ordonez, J.D.; Chertow, G.M.; Go, A.S. Community-based incidence of acute renal failure. Kidney Int. 2007, 72, 208–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiao, C.C.; Wu, P.C.; Wu, V.C.; Lin, J.H.; Pan, H.C.; Yang, Y.F.; Lai, T.S.; Huang, T.M.; Wu, C.H.; Yang, W.S.; et al. Nationwide epidemiology and prognosis of dialysis-requiring acute kidney injury (NEP-AKI-D) study: Design and methods. Nephrology (Carlton) 2016, 21, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Wu, V.C.; Huang, W.C.; Yeh, Y.C.; Wu, M.S.; Huang, C.C.; Wu, K.D.; Fang, J.T.; Wu, C.J.; CAKS Group. Norepinephrine Administration Is Associated with Higher Mortality in Dialysis Requiring Acute Kidney Injury Patients with Septic Shock. J. Clin. Med. 2018, 7, 274. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Ko, W.J.; Chang, H.W.; Chen, Y.S.; Chen, Y.W.; Chen, Y.M.; Hu, F.C.; Lin, Y.H.; Tsai, P.R.; Wu, K.D. Early renal replacement therapy in patients with postoperative acute liver failure associated with acute renal failure: Effect on postoperative outcomes. J. Am. Coll. Surg. 2007, 205, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.F.; Ko, W.J.; Wu, V.C.; Chen, Y.S.; Chen, Y.M.; Hu, F.C.; Shiao, C.C.; Wu, M.S.; Chen, Y.W.; Li, W.Y.; et al. A modified sequential organ failure assessment score to predict hospital mortality of postoperative acute renal failure patients requiring renal replacement therapy. Blood Purif. 2008, 26, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Shiao, C.C.; Ko, W.J.; Wu, V.C.; Huang, T.M.; Lai, C.F.; Lin, Y.F.; Chao, C.T.; Chu, T.S.; Tsai, H.B.; Wu, P.C.; et al. U-curve association between timing of renal replacement therapy initiation and in-hospital mortality in postoperative acute kidney injury. PLoS ONE 2012, 7, e42952. [Google Scholar] [CrossRef] [PubMed]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [PubMed]
- Raith, E.P.; Udy, A.A.; Bailey, M.; McGloughlin, S.; MacIsaac, C.; Bellomo, R.; Pilcher, D.V. Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality Among Adults With Suspected Infection Admitted to the Intensive Care Unit. JAMA 2017, 317, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Ko, W.J.; Chang, H.W.; Chen, Y.W.; Lin, Y.F.; Shiao, C.C.; Chen, Y.M.; Chen, Y.S.; Tsai, P.R.; Hu, F.C.; et al. Risk factors of early redialysis after weaning from postoperative acute renal replacement therapy. Intensive Care Med. 2008, 34, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, R.; Kellum, J.A.; Ronco, C.; Wald, R.; Martensson, J.; Maiden, M.; Bagshaw, S.M.; Glassford, N.J.; Lankadeva, Y.; Vaara, S.T.; et al. Acute kidney injury in sepsis. Intensive Care Med. 2017, 43, 816–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demirjian, S.; Chertow, G.M.; Zhang, J.H.; O’Connor, T.Z.; Vitale, J.; Paganini, E.P.; Palevsky, P.M.; VA/NIH Acute Renal Failure Trial Network. Model to predict mortality in critically ill adults with acute kidney injury. Clin. J. Am. Soc. Nephrol. 2011, 6, 2114–2120. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.S.; Ko, W.J.; Lin, F.Y.; Huang, S.C.; Chou, T.F.; Chou, N.K.; Hsu, R.B.; Wang, S.S.; Chu, S.H. Preliminary result of an algorithm to select proper ventricular assist devices for high-risk patients with extracorporeal membrane oxygenation support. J. Heart Lung Transplant. 2001, 20, 850–857. [Google Scholar] [CrossRef]
- Shu, K.H.; Wang, C.H.; Wu, C.H.; Huang, T.M.; Wu, P.C.; Lai, C.H.; Tseng, L.J.; Tsai, P.R.; Connolly, R.; Wu, V.C. Urinary pi-glutathione S-transferase Predicts Advanced Acute Kidney Injury Following Cardiovascular Surgery. Sci. Rep. 2016, 6, 26335. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.J.; Chi, N.H.; Huang, T.M.; Connolly, R.; Chen, L.W.; Chueh, S.J.; Kan, W.C.; Lai, C.C.; Wu, V.C.; Fang, J.T.; et al. Urinary biomarkers predict advanced acute kidney injury after cardiovascular surgery. Crit. Care 2018, 22, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagshaw, S.M.; Uchino, S.; Bellomo, R.; Morimatsu, H.; Morgera, S.; Schetz, M.; Tan, I.; Bouman, C.; Macedo, E.; Gibney, N.; et al. Septic acute kidney injury in critically ill patients: Clinical characteristics and outcomes. Clin. J. Am. Soc. Nephrol. 2007, 2, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Venot, M.; Weis, L.; Clec’h, C.; Darmon, M.; Allaouchiche, B.; Goldgran-Toledano, D.; Garrouste-Orgeas, M.; Adrie, C.; Timsit, J.F.; Azoulay, E. Acute Kidney Injury in Severe Sepsis and Septic Shock in Patients with and without Diabetes Mellitus: A Multicenter Study. PLoS ONE 2015, 10, e0127411. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Non-Sepsis | Sepsis | Septic Shock | p Value | |
|---|---|---|---|---|
| (n = 501) | (n = 371) | (n = 206) | ||
| Patient characteristics | ||||
| Age, median (range) | 71.8 (60.6–80.3) | 69.3 (57.6–79.7) | 65.8 (54.3–76.3) | 0.011 |
| Male gender, n (%) | 299 (59.68%) | 228 (61.46%) | 146 (70.87%) | 0.018 |
| BMI, median (range) | 23.9 (21.4–27.2) | 24 (21–27.2) | 23.9 (21–26.9) | 0.579 |
| Charlson comorbidity index | 7 (5–9) | 7 (5–9) | 6 (5–8) | 0.020 |
| Baseline sCr (mg/dL), median (range) | 1.7 (1–3.3) | 1.4 (0.9–2.4) | 1 (0.8–1.7) | <0.001 |
| eGFR (ml/min/1.73 m2), median (range) | 32.5 (15.5–63.3) | 44 (21.9–73.8) | 63.9 (35.2–88) | <0.001 |
| Comorbidities, n (%) | ||||
| Diabetes mellitus, n (%) | 276 (55.09%) | 189 (50.94%) | 97 (47.09%) | 0.131 |
| Liver cirrhosis, n (%) | 56 (11.18%) | 58 (15.63%) | 40 (19.42%) | 0.011 |
| COPD, n (%) | 43 (8.58%) | 29 (7.82%) | 12 (5.83%) | 0.462 |
| CAD, n (%) | 156 (31.14%) | 102 (27.49%) | 52 (25.24%) | 0.233 |
| CVA, n (%) | 78 (15.57%) | 59 (15.90%) | 22 (10.68%) | 0.185 |
| Hemiplegia, n (%) | 22 (4.39%) | 20 (5.39%) | 6 (2.91%) | 0.383 |
| GI bleeding, n (%) | 129 (25.75%) | 109 (29.38%) | 58 (28.16%) | 0.479 |
| Dementia, n (%) | 11 (2.20%) | 12 (3.23%) | 9 (4.37%) | 0.282 |
| Cancer, n (%) | 86 (17.17%) | 79 (21.29%) | 63 (30.58%) | <0.001 |
| Congestive heart failure, n (%) | 194 (48.7%) | 159 (58.49%) | 68 (44.66%) | <0.001 |
| Laboratory data at ICU admission | ||||
| BUN (mg/dL), median (range) | 61 (34.5–95.9) | 57.7 (27–92) | 42 (23.2–68.8) | <0.001 |
| sCr (mg/dL), median (range) | 3.7 (2–6.4) | 2.7 (1.4–5) | 2.3 (1.3–3.8) | <0.001 |
| Lactate (mmol/L), median (range) | 2.5 (1.4–5.6) | 2.4 (1.3–4.8) | 6.3 (2.9–10) | <0.001 |
| Etiology of AKI (except sepsis), n (%) | ||||
| Shock | 225 (44.91%) | 203 (54.72%) | 188 (91.26%) | <0.001 |
| Cardiorenal syndrome | 206 (41.12%) | 134 (36.12%) | 53 (25.73%) | <0.001 |
| Drug nephrotoxicity | 26 (5.19%) | 18 (4.85%) | 10 (4.85%) | 0.969 |
| Rhabdomyolysis | 34 (6.79%) | 24 (6.47%) | 23 (11.17%) | 0.086 |
| Intravascular hemolysis | 16 (3.19%) | 10 (2.70%) | 8 (3.88%) | 0.735 |
| Hepatorenal | 26 (5.19%) | 22 (5.93%) | 21 (10.19%) | 0.043 |
| ATIN | 4 (0.80%) | 5 (1.35%) | 0 (0%) | 0.276 |
| Contrast | 38 (7.58%) | 24 (6.47%) | 13 (6.31%) | 0.750 |
| Obstructive | 8 (1.60%) | 3 (0.81%) | 1 (0.49%) | 0.472 |
| Others | 117 (23.35%) | 56 (15.09%) | 24 (11.65%) | <0.001 |
| At initiation of RRT | ||||
| Urine output (mL/24 h), median (range) | 450 (150–1095) | 250 (70–620) | 130 (50–418) | <0.001 |
| AKI risk prediction score, median (range) | 22 (17–28) | 27 (21–33) | 33.5 (26–40) | <0.001 |
| Lactate (mmol/L), median (range) | 2.2 (1.3–5.2) | 1.6 (1–3.1) | 6.6 (3.4–10.7) | <0.001 |
| SOFA score, median (range) | 10 (7–13) | 12 (10–15) | 15 (13–17) | <0.001 |
| qSOFA, median (range) | 1 (1–1) | 2 (2-3) | 2 (2–3) | <0.001 |
| APACHE II score, median (range) | 20 (16–25) | 25 (21–30) | 27 (22.8–33) | <0.001 |
| MODS score, median (range) | 9 (7–11) | 12 (10–14) | 12 (10–15) | <0.001 |
| Site of infection, n (%) | ||||
| Respiratory | 227 (45.31%) | 237 (63.88%) | 114 (55.34%) | <0.001 |
| GU | 156 (31.14%) | 129 (34.77%) | 53 (25.73%) | 0.080 |
| Bacteremia | 96 (19.16%) | 84 (22.64%) | 57 (27.67%) | 0.043 |
| Abdomen | 41 (8.18%) | 40 (10.78%) | 33 (16.02%) | 0.009 |
| Others | 56 (11.18%) | 38 (10.24%) | 21 (10.19%) | 0.880 |
| Indication for dialysis, n (%) | ||||
| Azotemia | 291 (58.08%) | 225 (60.65%) | 70 (33.98%) | <0.001 |
| Fluid overload | 245 (48.90%) | 225 (60.65%) | 134 (65.05%) | <0.001 |
| Electrolyte imbalance | 190 (37.92%) | 148 (39.89%) | 79 (38.35%) | 0.835 |
| Metabolic acidosis | 210 (41.92%) | 192 (51.75%) | 133 (64.56%) | <0.001 |
| Oliguria | 275 (54.89%) | 255 (68.73%) | 164 (79.61%) | <0.001 |
| Uremic encephalopathy | 46 (9.18%) | 26 (7.01%) | 6 (2.91%) | 0.014 |
| Dialysis modality, n (%) | <0.001 | |||
| CVVH | 128 (25.55%) | 110 (29.65%) | 133 (64.56%) | |
| IHD | 334 (66.67%) | 252 (67.92%) | 58 (28.16%) | |
| SLEDD | 39 (7.78%) | 9 (2.43%) | 15 (7.28%) | |
| Outcomes of interest | ||||
| Dialysis days in hospital, median (range) | 12 (4–26) | 10 (4–27) | 6 (3–15) | 0.012 |
| Hospital mortality, n (%) | 221 (44.11%) | 228 (61.46%) | 167 (81.07%) | <0.001 |
| 90-day ICU free days | 63 (0–85) | 1 (0–78) | 0 (0–0) | <0.001 |
| 90-day hospital free days | 30 (0–70) | 0 (0–53) | 0 (0–0) | <0.001 |
| 90-day mortality, n (%) | 246 (49.10%) | 253 (68.19%) | 172 (83.49%) | <0.001 |
| 90-day composite outcome, n (%) | 352 (70.26%) | 296 (79.78%) | 175 (84.95%) | <0.001 |
| All | 90 Day Survivors | 90 Day Mortality | p Value | No Dialysis Dependence or Mortality at 90 Days | Dialysis Dependence or Mortality at 90 Days | p Value | |
|---|---|---|---|---|---|---|---|
| (n = 1078) | (n = 406) | (n = 672) | (n = 254) | (n = 824) | |||
| Baseline characteristics | |||||||
| Age, median (range) | 70 (57.8–79.5) | 69 (56.7–77.4) | 71 (58.9–81) | 0.014 | 67.7 (53.9–76.8) | 70.9 (59.8–80.4) | <0.001 |
| Male gender, n (%) | 673 (62.43%) | 247 (60.84%) | 426 (63.39%) | 0.401 | 158 (62.20%) | 515 (62.50%) | 0.932 |
| BMI, median (range) | 23.95 (21.2–27.1) | 24.2 (21.5–27.6) | 23.7 (21–26.8) | 0.870 | 24.6 (22–27.9) | 23.7 (21–26.8) | 0.598 |
| Charlson comorbidity index, median (range) | 7 (5–9) | 7 (5–8.3) | 7 (5–9) | 0.001 | 6 (4–8) | 7 (5–9) | <0.001 |
| Baseline sCr (mg/dL), median (range) | 1.4 (0.9–2.7) | 1.8 (1–3.6) | 1.3 (0.9–2.3) | <0.001 | 1.2 (0.9–2.1) | 1.5 (0.9–2.8) | <0.001 |
| eGFR (mL/min/1.73 m2), median (range) | 41.79 (20.4–73.6) | 31.9 (14.6-64.3) | 48.2 (24.4-77.1) | <0.001 | 49.9 (25.3-78) | 40.5 (18.2-71.7) | 0.040 |
| Comorbidities | |||||||
| Diabetes mellitus, n (%) | 562 (52.13%) | 228 (56.16%) | 334 (49.70%) | 0.040 | 139 (54.72%) | 423 (51.33%) | 0.344 |
| Liver cirrhosis, n (%) | 154 (14.29%) | 26 (6.40%) | 128 (19.05%) | <0.001 | 19 (7.48%) | 135 (16.38%) | <0.001 |
| COPD, n (%) | 84 (7.79%) | 31 (7.64%) | 53 (7.89%) | 0.881 | 19 (7.48%) | 65 (7.89%) | 0.832 |
| CAD, n (%) | 310 (28.76%) | 130 (32.02%) | 180 (26.79%) | 0.066 | 77 (30.31%) | 233 (28.28%) | 0.530 |
| CVA, n (%) | 159 (14.75%) | 61 (15.02%) | 98 (14.58%) | 0.843 | 30 (11.81%) | 129 (15.66%) | 0.131 |
| Hemiplegia, n (%) | 48 (4.45%) | 19 (4.68%) | 29 (4.32%) | 0.779 | 11 (4.33%) | 37 (4.49%) | 0.914 |
| GI bleeding, n (%) | 296 (27.46%) | 89 (21.92%) | 207 (30.80%) | 0.002 | 53 (20.87%) | 243 (29.49%) | 0.007 |
| Dementia, n (%) | 32 (2.97%) | 7 (1.72%) | 25 (3.72%) | 0.061 | 6 (2.36%) | 26 (3.16%) | 0.515 |
| Cancer, n (%) | 228 (21.15%) | 60 (14.78%) | 168 (25.00%) | <0.001 | 40 (15.75%) | 188 (22.82%) | 0.016 |
| Congestive heart failure, n (%) | 553 (51.30%) | 205 (50.49%) | 348 (50.79%) | 0.787 | 122 (48.41%) | 431 (52.31%) | 0.019 |
| Parameters at ICU admission | |||||||
| BUN (mg/dL), median (range) | 56 (29.2–89) | 63 (35–91) | 50.5 (26.4–88) | 0.001 | 51 (26–80.5) | 57.7 (30–91.6) | 0.192 |
| sCr (mg/dL), median (range) | 3 (1.7–5.5) | 4.1 (2.2–6.9) | 2.6 (1.4–4.5) | <0.001 | 3 (1.9–5.3) | 3 (1.6–5.6) | 0.984 |
| Lactate (mmol/L), median (range) | 3.1 (1.7–7) | 2.6 (1.3–5.2) | 3.7 (2–8.6) | <0.001 | 3 (1.6–6.1) | 3.2 (1.7–7.3) | 0.030 |
| Etiology of AKI, n (%) | |||||||
| Shock, n (%) | 616 (57.14%) | 165 (40.64%) | 451 (67.11%) | <0.001 | 132 (51.97%) | 484 (58.74%) | 0.057 |
| Sepsis, n (%) | 770 (71.43%) | 242 (59.61%) | 528 (78.57%) | <0.001 | 153 (60.24%) | 617 (74.88%) | <0.001 |
| Cardiorenal syndrome, n (%) | 393 (36.46%) | 170 (41.87%) | 223 (33.18%) | 0.010 | 93 (36.61%) | 300 (36.41%) | 0.952 |
| Nephrotoxic drugs, n (%) | 54 (5.01%) | 27 (6.65%) | 27 (4.02%) | 0.055 | 22 (8.66%) | 32 (3.88%) | 0.002 |
| Rhabdomyolysis, n (%) | 81 (7.51%) | 33 (8.13%) | 48 (7.14%) | 0.552 | 28 (11.02%) | 53 (6.43%) | 0.015 |
| Intravascular hemolysis, n (%) | 34 (3.15%) | 14 (3.45%) | 20 (2.98%) | 0.667 | 11 (4.33%) | 23 (2.79%) | 0.220 |
| Hepatorenal syndrome, n (%) | 69 (6.40%) | 4 (0.99%) | 65 (9.67%) | <0.001 | 4 (1.57%) | 65 (7.89%) | <0.001 |
| ATIN, n (%) | 9 (0.83%) | 5 (1.23%) | 4 (0.60%) | 0.309 | 2 (0.79%) | 7 (0.85%) | 0.999 |
| Contrast exposure, n (%) | 75 (6.96%) | 33 (8.13%) | 42 (6.25%) | 0.240 | 22 (8.66%) | 53 (6.43%) | 0.222 |
| Obstruction, n (%) | 12 (1.11%) | 6 (1.48%) | 6 (0.89%) | 0.375 | 3 (1.18%) | 9 (1.09%) | 1.000 |
| Others, n (%) | 197 (18.27%) | 103 (25.37%) | 94 (13.99%) | <0.001 | 61 (24.02%) | 136 (16.50%) | 0.007 |
| Parameters at RRT initiation | |||||||
| Urine output (mL/24 h), median (range) | 300 (90–822.5) | 490 (160–1223) | 204 (70–595) | <0.001 | 520 (180–1305) | 250 (75–670) | <0.001 |
| AKI risk prediction score | 25 (19–33) | 21 (16–28.3) | 27.5 (22–35) | <0.001 | 22 (17–29.3) | 26 (21–34) | <0.001 |
| Lactate (mmol/L), median (range) | 3.2 (1.6–7.6) | 2.3 (1.2–5.4) | 3.9 (1.9–9.1) | <0.001 | 2.8 (1.4–6.5) | 3.3 (1.6–8.2) | 0.090 |
| SOFA score, median (range) | 12 (8–15) | 9 (7–12) | 13 (10–16) | <0.001 | 10 (7–13) | 12 (9–15) | <0.001 |
| qSOFA, median (range) | 2 (1–2) | 1 (1–2) | 2 (1–2) | <0.001 | 1 (1–2) | 2 (1–2) | <0.001 |
| qSOFA ≥ 2, n (%) | 582 (53.99%) | 153 (37.66%) | 429 (63.84%) | <0.001 | 107 (42.13%) | 475 (57.65%) | <0.001 |
| APACHE II score, median (range) | 24 (19–28) | 20 (16–25) | 25 (21–30) | <0.001 | 21 (16–26) | 24 (20–29) | <0.001 |
| MODS score, median (range) | 11 (9–13) | 10 (7–12) | 11 (9–14) | <0.001 | 10 (7.5–13) | 11 (9–13) | 0.008 |
| Sepsis 3 criteria | |||||||
| Sepsis, n (%) | 577 (53.53%) | 152 (37.44%) | 425 (63.24%) | <0.001 | 106 (41.73%) | 471 (57.16%) | <0.001 |
| Septic shock, n (%) | 206 (19.11%) | 34 (8.37%) | 172 (25.60%) | <0.001 | 31 (12.20%) | 175 (21.24%) | 0.001 |
| Site of infection, n (%) | |||||||
| Respiratory | 578 (53.62%) | 188 (46.31%) | 390 (58.04%) | <0.001 | 1113 (44.49%) | 465 (56.43%) | 0.001 |
| GU | 338 (31.35%) | 134 (33.00%) | 204 (30.36%) | 0.364 | 83 (32.68%) | 255 (30.95%) | 0.603 |
| Bacteremia | 237 (21.99%) | 60 (14.78%) | 177 (26.34%) | <0.001 | 43 (16.93%) | 194 (23.54%) | 0.026 |
| Abdomen | 114 (10.58%) | 39 (9.61%) | 75 (11.16%) | 0.421 | 32 (12.60%) | 82 (9.95%) | 0.230 |
| Others | 115 (10.67%) | 37 (9.11%) | 78 (11.61%) | 0.199 | 25 (9.84%) | 90 (10.92%) | 0.626 |
| Indication for RRT | |||||||
| Azotemia, n (%) | 586 (54.36%) | 220 (54.19%) | 366 (54.46%) | 0.929 | 113 (44.49%) | 473 (57.40%) | <0.001 |
| Fluid overload, n (%) | 604 (56.03%) | 200 (49.26%) | 404 (60.12%) | 0.001 | 132 (51.97%) | 472 (57.28%) | 0.136 |
| Electrolyte imbalance, n (%) | 417 (38.68%) | 160 (39.41%) | 257 (38.24%) | 0.704 | 108 (42.52%) | 309 (37.50%) | 0.151 |
| Metabolic acidosis, n (%) | 535 (49.63%) | 180 (44.33%) | 355 (52.83%) | 0.007 | 114 (44.88%) | 421 (51.09%) | 0.084 |
| Oliguria, n (%) | 694 (64.38%) | 205 (50.49%) | 489 (72.77%) | <0.001 | 122 (48.03%) | 572 (69.42%) | <0.001 |
| Uremic encephalopathy, n (%) | 78 (7.24%) | 38 (9.36%) | 40 (5.95%) | 0.036 | 16 (6.30%) | 62 (7.52%) | 0.510 |
| First Dialysis modality, n (%) | <0.001 | 0.239 | |||||
| CVVH | 371 (34.42%) | 97 (23.89%) | 274 (40.77%) | 79 (31.10%) | 292 (35.44%) | ||
| IHD | 644 (59.74%) | 289 (71.18%) | 355 (52.83%) | 163 (64.17%) | 481 (58.37%) | ||
| SLEDD | 63 (5.84%) | 20 (4.93%) | 43 (6.40%) | 12 (4.72%) | 51 (6.19%) | ||
| Outcomes of interest | |||||||
| 90-day ICU free days | 7 (0–81) | 81 (69–86) | 0(0–1) | <0.001 | 80 (68–86) | 0 (0–54.5) | <0.001 |
| 90-day hospital free days | 0 (0–59.25) | 63 (44.5–76) | 0(0–0) | <0.001 | 63 (42–76) | 0 (0–2.5) | <0.001 |
| Days of RRT in hospital, median (range) | 10 (4–24) | 11 (3–26) | 9.5 (4–22.8) | 0.461 | 5.5 (2–13.3) | 12 (4–27.8) | <0.001 |
| Sepsis | Non-Shock Sepsis vs Non-Sepsis | Septic Shock vs. Non-Sepsis | ||||
|---|---|---|---|---|---|---|
| Outcome of interests | Hazard Ratio | 95% CI | p | Hazard Ratio | 95% CI | p |
| Hospital mortality | 1.12 | 0.91–1.37 | 0.276 | 1.48 | 1.17–1.88 | 0.001 |
| Hospital composite outcomes | 0.97 | 0.80–1.17 | 0.732 | 1.24 | 1.08–1.47 | 0.047 |
| For 90-day mortality | 1.23 | 1.02–1.47 | 0.027 | 1.39 | 1.11–1.75 | 0.004 |
| For 90-day composite outcome | 1.26 | 1.03–1.53 | 0.022 | 1.45 | 1.15–1.83 | 0.002 |
| For 90-day weaning from dialysis | 0.96 | 0.76–1.22 | 0.760 | 0.65 | 0.45–0.95 | 0.026 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, V.-C.; Chueh, S.-C.J.; Chang, J.-T.; Hsu, B.-G.; Ostermann, M.; Chu, T.-S. Acute Kidney Injury and Septic Shock—Defined by Updated Sepsis-3 Criteria in Critically Ill Patients. J. Clin. Med. 2019, 8, 1731. https://doi.org/10.3390/jcm8101731
Wu V-C, Chueh S-CJ, Chang J-T, Hsu B-G, Ostermann M, Chu T-S. Acute Kidney Injury and Septic Shock—Defined by Updated Sepsis-3 Criteria in Critically Ill Patients. Journal of Clinical Medicine. 2019; 8(10):1731. https://doi.org/10.3390/jcm8101731
Chicago/Turabian StyleWu, Vin-Cent, Shih-Chieh Jeff Chueh, Jui-Ting Chang, Bang-Gee Hsu, Marlies Ostermann, and Tzong-Shinn Chu. 2019. "Acute Kidney Injury and Septic Shock—Defined by Updated Sepsis-3 Criteria in Critically Ill Patients" Journal of Clinical Medicine 8, no. 10: 1731. https://doi.org/10.3390/jcm8101731