Modified Colon Leakage Score to Predict Anastomotic Leakage in Patients Who Underwent Left-Sided Colorectal Surgery


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Surgery and Diagnosis of AL
2.3. Clinical Variables Used in Generating Modified CLS
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics According to the Anastomotic Leakage
3.2. Comparison of Patient Characteristics between the Training Set and the Validation Set
3.3. Feature Selection and Generation of Modified CLS
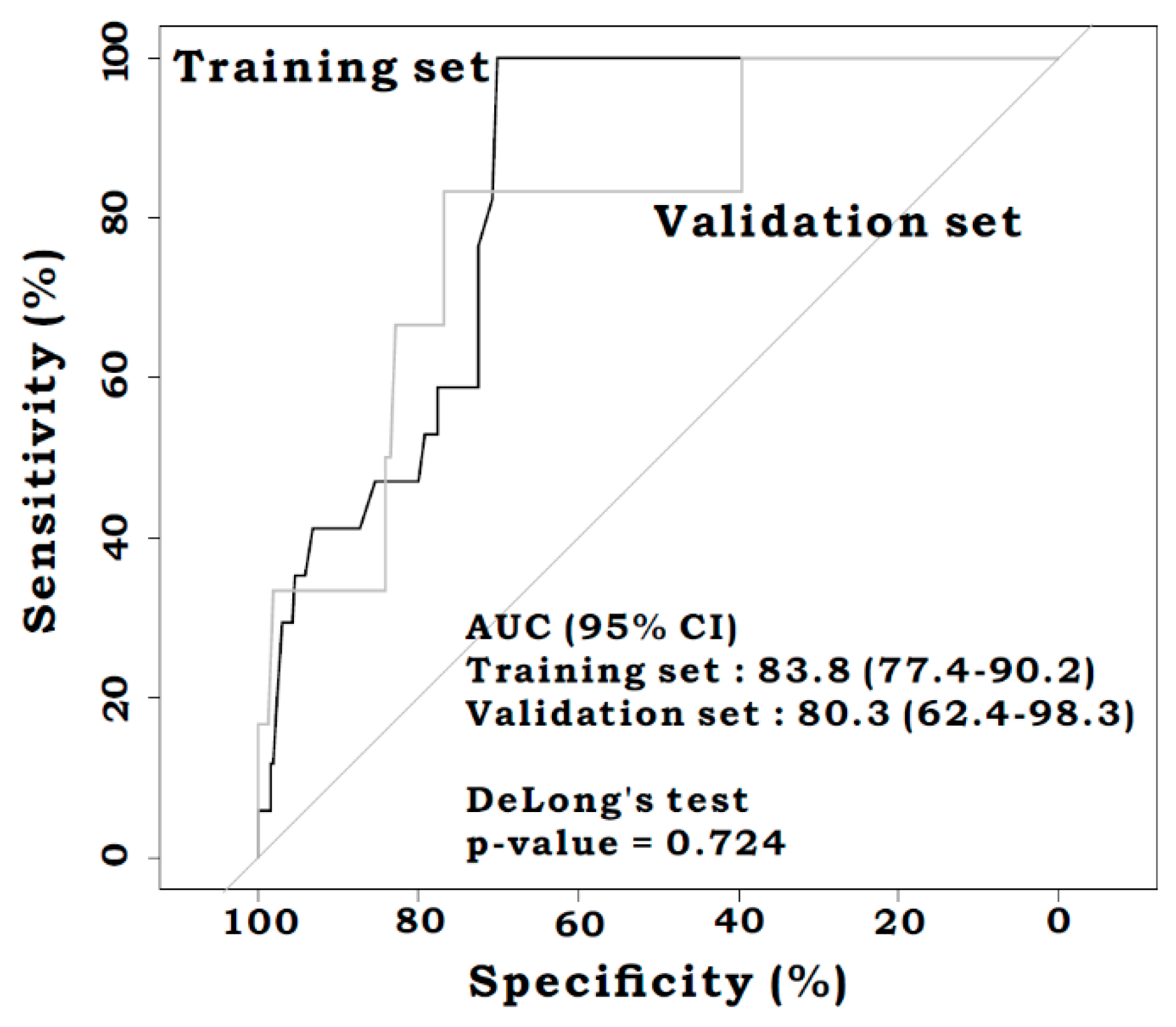
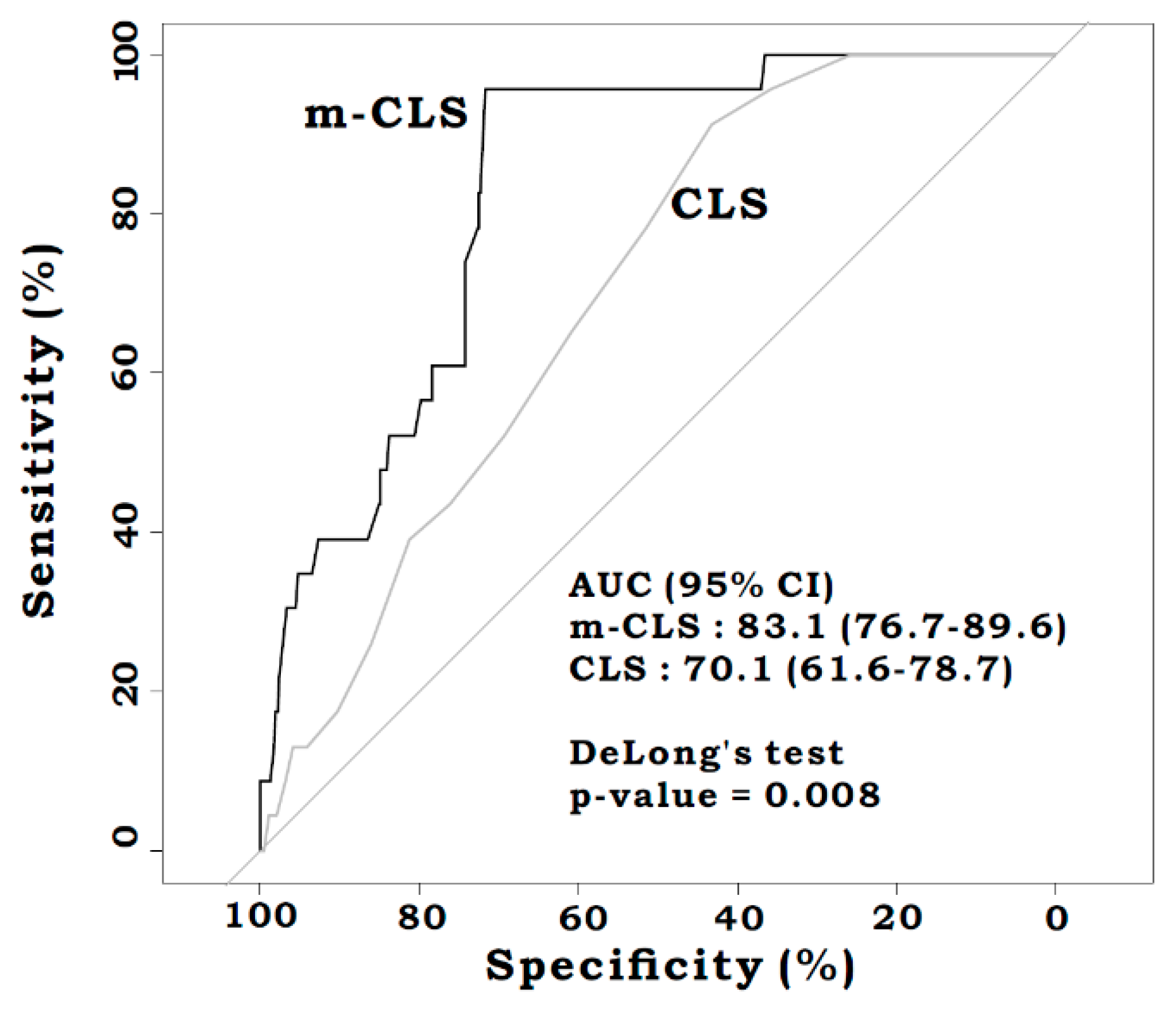
3.4. AUROC Comparison
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Peeters, K.C.; Tollenaar, R.A.; Marijnen, C.A.; Klein Kranenbarg, E.; Steup, W.H.; Wiggers, T.; Rutten, H.J.; van de Velde, C.J. Risk factors for anastomotic failure after total mesorectal excision of rectal cancer. Br. J. Surg. 2005, 92, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Matthiessen, P.; Hallbook, O.; Rutegard, J.; Simert, G.; Sjodahl, R. Defunctioning stoma reduces symptomatic anastomotic leakage after low anterior resection of the rectum for cancer: A randomized multicenter trial. Ann. Surg. 2007, 246, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Yeh, C.Y.; Changchien, C.R.; Wang, J.Y.; Chen, J.S.; Chen, H.H.; Chiang, J.M.; Tang, R. Pelvic drainage and other risk factors for leakage after elective anterior resection in rectal cancer patients: A prospective study of 978 patients. Ann. Surg. 2005, 241, 9–13. [Google Scholar] [PubMed]
- Trencheva, K.; Morrissey, K.P.; Wells, M.; Mancuso, C.A.; Lee, S.W.; Sonoda, T.; Michelassi, F.; Charlson, M.E.; Milsom, J.W. Identifying important predictors for anastomotic leak after colon and rectal resection: Prospective study on 616 patients. Ann. Surg. 2013, 257, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Marra, F.; Steffen, T.; Kalak, N.; Warschkow, R.; Tarantino, I.; Lange, J.; Zünd, M. Anastomotic leakage as a risk factor for the long-term outcome after curative resection of colon cancer. Eur. J. Surg. Oncol. 2009, 35, 1060–1064. [Google Scholar] [CrossRef] [PubMed]
- Bostrom, P.; Haapamaki, M.M.; Rutegard, J.; Matthiessen, P.; Rutegard, M. Population-based cohort study of the impact on postoperative mortality of anastomotic leakage after anterior resection for rectal cancer. BJS Open 2019, 3, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Choi, G.S.; Oh, J.H.; Kim, N.K.; Park, J.S.; Kim, M.J.; Lee, K.Y.; Baik, S.H. Multicenter analysis of long-term oncologic impact of anastomotic leakage after laparoscopic total mesorectal excision: The korean laparoscopic colorectal surgery study group. Medicine 2015, 94, e1202. [Google Scholar] [CrossRef] [PubMed]
- Mirnezami, A.; Mirnezami, R.; Chandrakumaran, K.; Sasapu, K.; Sagar, P.; Finan, P. Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: Systematic review and meta-analysis. Ann. Surg. 2011, 253, 890–899. [Google Scholar] [CrossRef] [PubMed]
- Branagan, G.; Finnis, D. Prognosis After Anastomotic Leakage in Colorectal Surgery. Dis. Colon Rectum 2005, 48, 1021–1026. [Google Scholar] [CrossRef]
- Dulk, M.D.; Marijnen, C.A.M.; Collette, L.; Putter, H.; Påhlman, L.; Folkesson, J.; Bosset, J.-F.; Rodel, C.; Bujko, K.; Van De Velde, C.J.H. Multicentre analysis of oncological and survival outcomes following anastomotic leakage after rectal cancer surgery. Br. J. Surg. Inc. Eur. J. Surg. Swiss Surg. 2009, 96, 1066–1075. [Google Scholar] [CrossRef]
- Rutegard, M.; Hemmingsson, O.; Matthiessen, P.; Rutegard, J. High tie in anterior resection for rectal cancer confers no increased risk of anastomotic leakage. Br. J. Surg. 2012, 99, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Zeng, J.; Su, G. High ligation of the inferior mesenteric artery during sigmoid colon and rectal cancer surgery increases the risk of anastomotic leakage: A meta-analysis. World J. Surg. Oncol. 2018, 16, 157. [Google Scholar] [CrossRef] [PubMed]
- Allaix, M.E.; Lena, A.; Degiuli, M.; Arezzo, A.; Passera, R.; Mistrangelo, M.; Morino, M. Intraoperative air leak test reduces the rate of postoperative anastomotic leak: Analysis of 777 laparoscopic left-sided colon resections. Surg. Endosc. 2019, 33, 1592–1599. [Google Scholar] [CrossRef] [PubMed]
- Kawada, K.; Sakai, Y. Preoperative, intraoperative and postoperative risk factors for anastomotic leakage after laparoscopic low anterior resection with double stapling technique anastomosis. World J. Gastroenterol. 2016, 22, 5718–5727. [Google Scholar] [CrossRef] [PubMed]
- Kingham, T.P.; Pachter, H.L. Colonic Anastomotic Leak: Risk Factors, Diagnosis, and Treatment. J. Am. Coll. Surg. 2009, 208, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Kologlu, M.; Yorganci, K.; Renda, N.; Sayek, I. Effect of local and remote ischemia-reperfusion injury on healing of colonic anastomoses. Surgery 2000, 128, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Hinoi, T.; Okajima, M.; Shimomura, M.; Egi, H.; Ohdan, H.; Konishi, F.; Sugihara, K.; Watanabe, M. Effect of Left Colonic Artery Preservation on Anastomotic Leakage in Laparoscopic Anterior Resection for Middle and Low Rectal Cancer. World J. Surg. 2013, 37, 2935–2943. [Google Scholar] [CrossRef] [PubMed]
- Buunen, M.; Lange, M.M.; Ditzel, M.; Kleinrensink, G.-J.; Van De Velde, C.J.H.; Lange, J.F. Level of arterial ligation in total mesorectal excision (TME): An anatomical study. Int. J. Color. Dis. 2009, 24, 1317–1320. [Google Scholar] [CrossRef] [PubMed]
- Hüser, N.; Michalski, C.W.; Erkan, M.; Schuster, T.; Rosenberg, R.; Kleeff, J.; Friess, H. Systematic Review and Meta-Analysis of the Role of Defunctioning Stoma in Low Rectal Cancer Surgery. Ann. Surg. 2008, 248, 52–60. [Google Scholar] [CrossRef]
- Shiomi, A.; Ito, M.; Maeda, K.; Kinugasa, Y.; Ota, M.; Yamaue, H.; Shiozawa, M.; Horie, H.; Kuriu, Y.; Saito, N. Effects of a Diverting Stoma on Symptomatic Anastomotic Leakage after Low Anterior Resection for Rectal Cancer: A Propensity Score Matching Analysis of 1,014 Consecutive Patients. J. Am. Coll. Surg. 2015, 220, 186–194. [Google Scholar] [CrossRef]
- Kaidar-Person, O.; Person, B.; Wexner, S.D. Complications of Construction and Closure of Temporary Loop Ileostomy. J. Am. Coll. Surg. 2005, 201, 759–773. [Google Scholar] [CrossRef] [PubMed]
- Phatak, U.R.; Kao, L.S.; You, Y.N.; Rodriguez-Bigas, M.A.; Skibber, J.M.; Feig, B.W.; Nguyen, S.; Cantor, S.B.; Chang, G.J. Impact of ileostomy-related complications on the multidisciplinary treatment of rectal cancer. Ann. Surg. Oncol. 2014, 21, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Hanna, M.H.; Vinci, A.; Pigazzi, A. Diverting ileostomy in colorectal surgery: When is it necessary? Langenbeck’s Arch. Surg. 2015, 400, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Cheong, J.; Kang, J.; Kim, I.-K.; Kim, N.K.; Sohn, S.-K.; Lee, K.Y. Feasibility and Safety of a Fold-Over Diverting Ileostomy Reversal After Rectal Cancer Surgery: Case-Matched Comparison to the Resection Technique. Ann. Coloproctology 2014, 30, 118–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messaris, E.; Sehgal, R.; Deiling, S.; Koltun, W.A.; Stewart, D.; McKenna, K.; Poritz, L.S. Dehydration Is the Most Common Indication for Readmission After Diverting Ileostomy Creation. Dis. Colon Rectum 2012, 55, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.-K.; Kang, J.; Baik, S.H.; Lee, K.Y.; Kim, N.K.; Sohn, S.-K. Impact of prior abdominal surgery on postoperative prolonged ileus after ileostomy repair. Asian J. Surg. 2018, 41, 86–91. [Google Scholar] [CrossRef] [Green Version]
- Gustavsson, K.; Gunnarsson, U.; Jestin, P. Postoperative complications after closure of a diverting ileostoma--differences according to closure technique. Int. J. Colorectal Dis. 2012, 27, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.-S.; Remzi, F.H.; Gorgun, E.; Arrigain, S.; Church, J.M.; Preen, M.; Fazio, V.W. Loop Ileostomy Closure After Restorative Proctocolectomy: Outcome in 1,504 Patients. Dis. Colon Rectum 2005, 48, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Kim, Y.S.; Park, S.C.; Sohn, D.K.; Kim, D.Y.; Chang, H.J.; Oh, J.H. Risk factors for permanent stoma after rectal cancer surgery with temporary ileostomy. Surgery 2016, 159, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Holmgren, K.; Kverneng Hultberg, D.; Haapamaki, M.M.; Matthiessen, P.; Rutegard, J.; Rutegard, M. High stoma prevalence and stoma reversal complications following anterior resection for rectal cancer: A population-based multicentre study. Colorectal Dis. 2017, 19, 1067–1075. [Google Scholar] [CrossRef]
- Dekker, J.W.T.; Liefers, G.J.; Otterloo, J.C.D.M.V.; Putter, H.; Tollenaar, R.A. Predicting the Risk of Anastomotic Leakage in Left-sided Colorectal Surgery Using a Colon Leakage Score. J. Surg. Res. 2011, 166, e27–e34. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.-Q.; Zhao, B.; Zhou, W.-P.; Han, L.-Z.; Cai, G.-H.; Fang, Z.-W.; Peng, Y.-H.; Yuan, B. Utility of colon leakage score in left-sided colorectal surgery. J. Surg. Res. 2016, 202, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Sammour, T.; Cohen, L.; Karunatillake, A.I.; Lewis, M.; Lawrence, M.J.; Hunter, A.; Moore, J.W.; Thomas, M.L. Validation of an online risk calculator for the prediction of anastomotic leak after colon cancer surgery and preliminary exploration of artificial intelligence-based analytics. Tech. Coloproctol. 2017, 21, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Sacks, G.D.; Dawes, A.J.; Ettner, S.L.; Brook, R.H.; Fox, C.R.; Maggard-Gibbons, M.; Ko, C.Y.; Russell, M.M. Surgeon Perception of Risk and Benefit in the Decision to Operate. Ann. Surg. 2016, 264, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Sacks, G.D.; Dawes, A.J.; Ettner, S.L.; Brook, R.H.; Fox, C.R.; Russell, M.M.; Ko, C.Y.; Maggard-Gibbons, M. Impact of a risk calculator on risk perception and surgical decision making: A randomized trial. Ann. Surg. 2016, 264, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Sammour, T.; Lewis, M.; Thomas, M.L.; Lawrence, M.J.; Hunter, A.; Moore, J.W. A simple web-based risk calculator (www.Anastomoticleak.Com) is superior to the surgeon’s estimate of anastomotic leak after colon cancer resection. Tech. Coloproctology 2017, 21, 35–41. [Google Scholar] [CrossRef]
- Watson, D.; Krutzinna, J.; Bruce, I.; Griffiths, C.; McInnes, I.; Barnes, M.; Floridi, L. Clinical Applications of Machine Learning Algorithms: Beyond the Black Box. BMJ 2019, 364, 886. [Google Scholar] [CrossRef] [PubMed]
- Harvin, J.A.; Green, C.E.; Pedroza, C.; Tyson, J.E.; Moore, L.J.; Wade, C.E.; Holcomb, J.B.; Kao, L.S. Using Machine Learning to Identify Change in Surgical Decision Making in Current Use of Damage Control Laparotomy. J. Am. Coll. Surg. 2019, 228, 255–264. [Google Scholar] [CrossRef]
- Tibshirani, R. The lasso method for variable selection in the cox model. Stat. Med. 1997, 16, 385–395. [Google Scholar] [CrossRef]
- Bohning, D.; Holling, H.; Patilea, V. A limitation of the diagnostic-odds ratio in determining an optimal cut-off value for a continuous diagnostic test. Stat. Methods Med Res. 2011, 20, 541–550. [Google Scholar] [CrossRef]
- Moran, B. Predicting the risk and diminishing the consequences of anastomotic leakage after anterior resection for rectal cancer. Acta Chir. Iugosl. 2010, 57, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Slieker, J.C.; Komen, N.; Mannaerts, G.H.; Karsten, T.M.; Willemsen, P.; Murawska, M.; Jeekel, J.; Lange, J.F. Long-term and perioperative corticosteroids in anastomotic leakage: A prospective study of 259 left-sided colorectal anastomoses. Arch. Surg. 2012, 147, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Suding, P.; Jensen, E.; Abramson, M.A.; Itani, K.; Wilson, S.E. Definitive risk factors for anastomotic leaks in elective open colorectal resection. Arch. Surg. 2008, 143, 907–912. [Google Scholar] [CrossRef] [PubMed]
- Konishi, T.; Watanabe, T.; Kishimoto, J.; Nagawa, H. Risk Factors for Anastomotic Leakage after Surgery for Colorectal Cancer: Results of Prospective Surveillance. J. Am. Coll. Surg. 2006, 202, 439–444. [Google Scholar] [CrossRef]
- Wang, H.; Wang, Y.; Xing, H.; Zhou, Y.; Zhao, J.; Jiang, J.; Liu, Q. Laparoscopic Surgery Within an Enhanced Recovery after Surgery (ERAS) Protocol Reduced Postoperative Ileus by Increasing Postoperative Treg Levels in Patients with Right-Side Colon Carcinoma. Med. Sci. Monit. 2018, 24, 7231. [Google Scholar] [CrossRef]
- Rushfeldt, C.F.; Agledahl, U.C.; Sveinbjørnsson, B.; Søreide, K.; Wilsgaard, T. Effect of Perioperative Dexamethasone and Different NSAIDs on Anastomotic Leak Risk: A Propensity Score Analysis. World J. Surg. 2016, 40, 2782–2789. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wan, X.; Wang, G.; Ren, Y.; Cheng, Y.; Zhao, Y.; Han, G. A scoring system to predict the risk of anastomotic leakage after anterior resection for rectal cancer. J. Surg. Oncol. 2014, 109, 122–125. [Google Scholar] [CrossRef]
- Park, J.S.; Choi, G.S.; Kim, S.H.; Kim, H.R.; Kim, N.K.; Lee, K.Y.; Kang, S.B.; Kim, J.Y.; Lee, K.Y.; Kim, B.C.; et al. Multicenter analysis of risk factors for anastomotic leakage after laparoscopic rectal cancer excision: The korean laparoscopic colorectal surgery study group. Ann. Surg. 2013, 257, 665–671. [Google Scholar] [CrossRef]
- Rojas-Machado, S.A.; Romero-Simo, M.; Arroyo, A.; Rojas-Machado, A.; Lopez, J.; Calpena, R. Prediction of anastomotic leak in colorectal cancer surgery based on a new prognostic index procole (prognostic colorectal leakage) developed from the meta-analysis of observational studies of risk factors. Int. J. Colorectal Dis. 2016, 31, 197–210. [Google Scholar] [CrossRef]
- Frasson, M.; Flor-Lorente, B.; Rodriguez, J.L.; Granero-Castro, P.; Hervas, D.; Alvarez Rico, M.A.; Brao, M.J.; Sanchez Gonzalez, J.M.; Garcia-Granero, E. Risk factors for anastomotic leak after colon resection for cancer: Multivariate analysis and nomogram from a multicentric, prospective, national study with 3193 patients. Ann. Surg. 2015, 262, 321–330. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| AL (n = 23) n (%) | No Leakage (n = 543) n (%) | P | ||
|---|---|---|---|---|
| Age (years) | Mean ± SD | 60.8 ± 12.6 | 62.1 ± 10.9 | 0.574 |
| Gender | Male | 17 (73.9) | 346 (63.7) | 0.438 |
| Female | 6 (26.1) | 197 (36.3) | ||
| ASA grade a | I | 16 (69.6) | 272 (50.1) | 0.076 b |
| II | 4 (17.4) | 226 (41.6) | ||
| III | 3 (13) | 44 (8.1) | ||
| IV | 0 | 1 (0.2) | ||
| BMI c (kg/m2) | Mean ± SD | 23.7 ± 3.5 | 23.4 ± 3.2 | 0.672 |
| Smoking | (any) | 10 (43.5) | 185 (34.1) | 0.375 |
| Alcohol | (3U/day) | 9 (39.1) | 109 (20.1) | 0.036 b |
| Steroids | (present use, excluding inhaler) | 2 (8.7) | 2 (0.4) | 0.009 b |
| Neoadjuvant therapy | Radiotherapy | 0 | 3 (0.6) | >0.999 b |
| Chemoradiation | 5 (21.7) | 69 (12.7) | 0.207 b | |
| Emergency surgery | Obstruction | 4 (17.4) | 100 (18.4) | >0.999 b |
| Bleeding | 0 | 8 (1.5) | >0.999 b | |
| Perforation | 0 | 12 (2.2) | >0.999 b | |
| Distance of anastomosis to anal verge (cm) | <5 | 10 (43.5) | 110 (20.3) | <0.001 b |
| 5–10 | 12 (52.2) | 186 (34.3) | ||
| >10 | 1 (4.3) | 247 (45.5) | ||
| Additional procedures | 1 (4.3) | 139 (25.6) | 0.023 | |
| Blood loss (mL) | Mean ± SD | 282.6 ± 280.6 | 287.9 ± 455.5 | 0.933 |
| Duration of operation (min) | Mean ± SD | 294.5 ± 76.8 | 272.6 ± 104.8 | 0.322 |
| Diversion | 2 (8.7) | 4 (0.7) | 0.021 b | |
| Tumor location | Colon | 1 (4.3) | 249 (45.9) | <0.001 |
| Rectum | 22 (95.7) | 294 (54.1) | ||
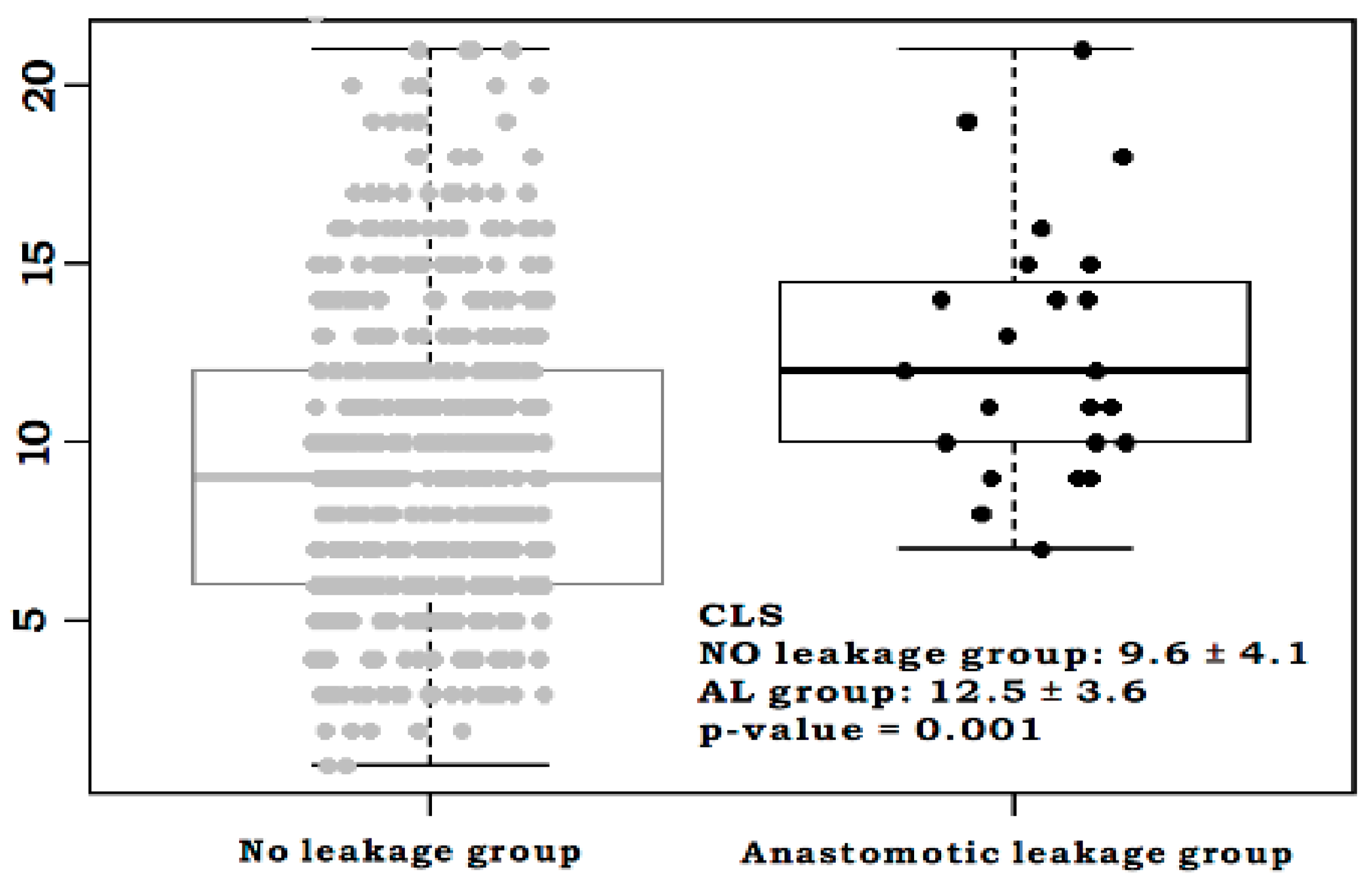
| CLS d | Mean ± SD | 12.5 ± 3.6 | 9.6 ± 4.2 | 0.001 |
| Surgery type | Open | 7 (30.4) | 175 (32.2) | 0.458 |
| Laparoscopy | 8 (34.8) | 239 (44) | ||
| Robot | 8 (34.8) | 129 (23.8) |
| Training Set (n = 396) n (%) | Validation Set (n = 170) n (%) | P | ||
|---|---|---|---|---|
| Age (years) | Mean ± SD | 62.5 ± 10.8 | 61.2 ± 11.5 | 0.186 |
| Gender | Male | 251 (63.4) | 112 (65.9) | 0.637 |
| Female | 145 (36.6) | 58 (34.1) | ||
| ASA grade a | I | 195 (49.2) | 93 (54.7) | 0.417 |
| II | 169 (42.7) | 61 (35.9) | ||
| III | 31 (7.8) | 16 (9.4) | ||
| IV | 1 (0.3) | 0 | ||
| BMI b (kg/m2) | Mean ± SD | 23.6 ± 3.1 | 23.1 ± 3.3 | 0.102 |
| Smoking | (any) | 135 (34.1) | 60 (35.3) | 0.857 |
| Alcohol | (3U/day) | 75 (18.9) | 43 (25.3) | 0.111 |
| Steroids | (present use, excluding inhaler) | 3 (0.8) | 1 (0.6) | >0.999 |
| Neoadjuvant therapy | Radiotherapy | 1 (0.3) | 2 (1.2) | 0.449 |
| Chemoradiation | 51 (12.9) | 23 (13.5) | 0.941 | |
| Emergency surgery | Obstruction | 76 (19.2) | 28 (16.5) | 0.517 |
| Bleeding | 7 (1.8) | 1 (0.6) | 0.446 b | |
| Perforation | 10 (2.5) | 2 (1.2) | 0.482 | |
| Distance of anastomosis to anal verge (cm) | <5 | 85 (21.5) | 35 (20.6) | 0.575 |
| 5–10 | 143 (36.1) | 55 (32.4) | ||
| >10 | 168 (42.4) | 80 (47.1) | ||
| Additional procedures | 96 (24.2) | 44 (25.9) | 0.758 | |
| Blood loss (mL) | Mean ± SD | 280.3 ± 421.4 | 304.9 ± 510.2 | 0.580 |
| Duration of operation (min) | Mean ± SD | 275.9 ± 109.5 | 267.6 ± 89.1 | 0.345 |
| Diversion | 3 (0.8) | 3 (1.8) | 0.532 | |
| Tumor location | Colon | 206 (52) | 89 (52.4) | >0.999 |
| Rectum | 190 (48) | 81 (47.6) | ||
| CLS c | Mean ± SD | 9.8 ± 4 | 9.7 ± 4.6 | 0.942 |
| Anastomotic leakage | 17 (4.3) | 6 (3.5) | 0.850 | |
| Surgery type | Open | 131 (33.1) | 51 (30) | 0.656 |
| Laparoscopy | 168 (42.4) | 79 (46.5) | ||
| Robot | 97 (24.5) | 40 (23.5) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, S.U.; Park, E.J.; Baik, S.H.; Lee, K.Y.; Kang, J. Modified Colon Leakage Score to Predict Anastomotic Leakage in Patients Who Underwent Left-Sided Colorectal Surgery. J. Clin. Med. 2019, 8, 1450. https://doi.org/10.3390/jcm8091450
Yang SU, Park EJ, Baik SH, Lee KY, Kang J. Modified Colon Leakage Score to Predict Anastomotic Leakage in Patients Who Underwent Left-Sided Colorectal Surgery. Journal of Clinical Medicine. 2019; 8(9):1450. https://doi.org/10.3390/jcm8091450
Chicago/Turabian StyleYang, Seung Up, Eun Jung Park, Seung Hyuk Baik, Kang Young Lee, and Jeonghyun Kang. 2019. "Modified Colon Leakage Score to Predict Anastomotic Leakage in Patients Who Underwent Left-Sided Colorectal Surgery" Journal of Clinical Medicine 8, no. 9: 1450. https://doi.org/10.3390/jcm8091450