A Prospective Assessment of the Diagnostic Value of Contrast-Enhanced Ultrasound, Dynamic Computed Tomography and Magnetic Resonance Imaging for Patients with Small Liver Tumors


Abstract
:1. Introduction
2. Experimental Section
2.1. Trial Design and Participants
2.2. Examinations and Procedures
2.3. Data Interpretation
2.4. Outcomes and Statistical Analysis
3. Results
3.1. Patient Characteristics and Safety
3.2. Diagnostic Performance of CEUS, MRI, and CT
3.3. Diagnostic Specificity When Combining Two Imaging Modalities
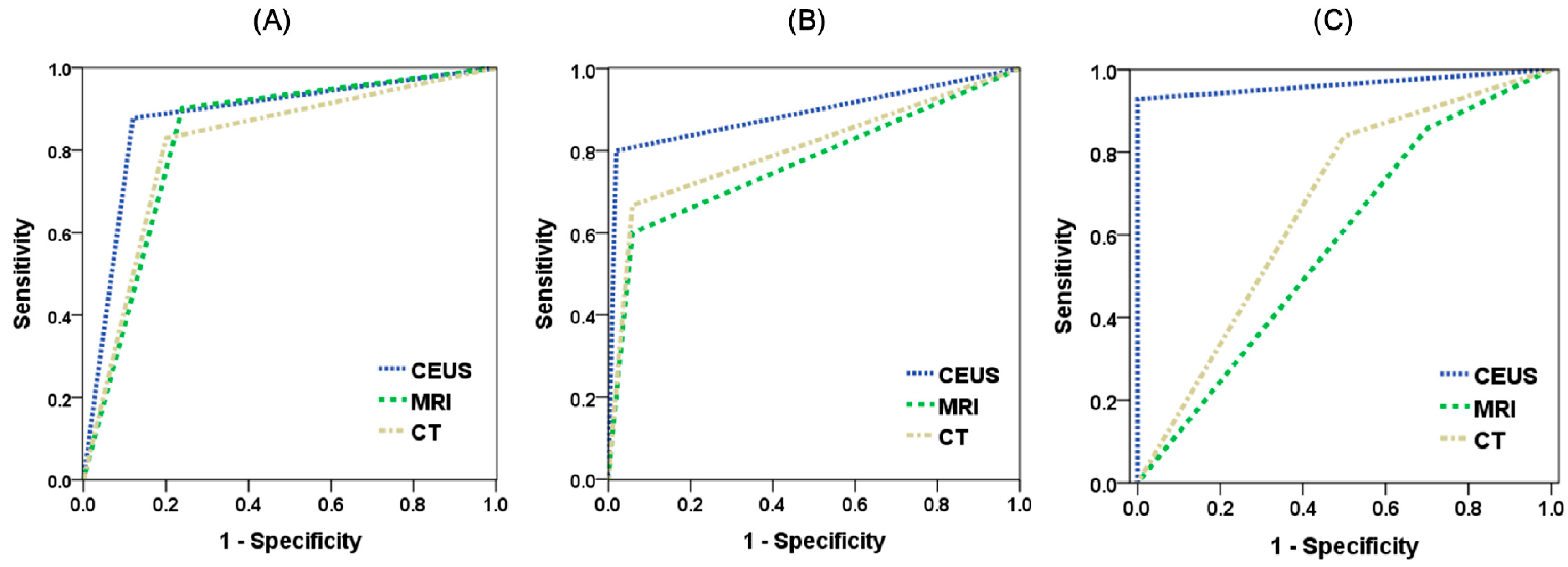
3.4. ROC Curve and AUC
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Hanna, R.F.; Miloushev, V.Z.; Tang, A.; Finklestone, L.A.; Brejt, S.Z.; Sandhu, R.S.; Santillan, C.S.; Wolfson, T.; Gamst, A.; Sirlin, C.B. Comparative 13-year meta-analysis of the sensitivity and positive predictive value of ultrasound, CT, and MRI for detecting hepatocellular carcinoma. Abdom. Radiol. 2016, 41, 71–90. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M. Defect Reperfusion Imaging with Sonazoid(R): A breakthrough in hepatocellular carcinoma. Liver Cancer 2016, 5, 1–7. [Google Scholar] [PubMed]
- Kim, T.K.; Jang, H.J. Contrast-enhanced ultrasound in the diagnosis of nodules in liver cirrhosis. World J. Gastroenterol. 2014, 20, 3590–3596. [Google Scholar] [CrossRef] [PubMed]
- D'Onofrio, M.; Crosara, S.; De Robertis, R.; Canestrini, S.; Mucelli, R.P. Contrast-enhanced ultrasound of focal liver lesions. Am. J. Roentgenol. 2015, 205, W56–W66. [Google Scholar] [CrossRef]
- Cantisani, V.; David, E.; Meloni, F.M.; Dietrich, C.F.; Badea, R.; Messineo, D.; D’Ambrosio, F.; Piscaglia, F. Recall strategies for patients found to have a nodule in cirrhosis: Is there still a role for CEUS? Med. Ultrason. 2015, 17, 515–520. [Google Scholar]
- Moriyasu, F.; Itoh, K. Efficacy of perflubutane microbubble-enhanced ultrasound in the characterization and detection of focal liver lesions: Phase 3 multicenter clinical trial. Am. J. Roentgenol. 2009, 193, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.-H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B. Hepatocellular carcinoma. N. Engl. J. Med. 2011, 365, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Mortality, G.B.D. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.-L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arita, J.; Takahashi, M.; Hata, S.; Shindoh, J.; Beck, Y.; Sugawara, Y.; Hasegawa, K.; Kokudo, N. Usefulness of contrast-enhanced intraoperative ultrasound using Sonazoid in patients with hepatocellular carcinoma. Ann. Surg. 2011, 254, 992–999. [Google Scholar] [CrossRef] [PubMed]
- Mandai, M.; Koda, M.; Matono, T.; Nagahara, T.; Sugihara, T.; Ueki, M.; Ohyama, K.; Murawaki, Y. Assessment of hepatocellular carcinoma by contrast-enhanced ultrasound with perfluorobutane microbubbles: Comparison with dynamic CT. Br. J. Radiol. 2011, 84, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Niu, Y.; Huang, T.; Lian, F.; Li, F. Contrast-enhanced ultrasonography for the diagnosis of small hepatocellular carcinoma: A meta-analysis and meta-regression analysis. Tumour Biol. 2013, 34, 3667–3674. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.J.; Kim, T.K.; Burns, P.N.; Wilson, S.R. CEUS: An essential component in a multimodality approach to small nodules in patients at high-risk for hepatocellular carcinoma. Eur. J. Radiol. 2015, 84, 1623–1635. [Google Scholar] [CrossRef] [PubMed]
- Hatanaka, K.; Kudo, M.; Minami, Y.; Maekawa, K. Sonazoid-enhanced ultrasonography for diagnosis of hepatic malignancies: Comparison with contrast-enhanced CT. Oncology 2008, 75, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Westwood, M.; Joore, M.; Grutters, J.; Redekop, K.; Armstrong, N.; Lee, K.; Gloy, V.; Raatz, H.; Misso, K.; Severens, J.; et al. Contrast-enhanced ultrasound using SonoVue(R) (sulphur hexafluoride microbubbles) compared with contrast-enhanced computed tomography and contrast-enhanced magnetic resonance imaging for the characterisation of focal liver lesions and detection of liver metastases: A systematic review and cost-effectiveness analysis. Health Technol. Assess. 2013, 17, 1–243. [Google Scholar] [PubMed]
- Friedrich-Rust, M.; Klopffleisch, T.; Nierhoff, J.; Herrmann, E.; Vermehren, J.; Schneider, M.D.; Zeuzem, S.; Bojunga, J. Contrast-Enhanced Ultrasound for the differentiation of benign and malignant focal liver lesions: A meta-analysis. Liver Int. 2013, 33, 739–755. [Google Scholar] [CrossRef] [PubMed]
- Glas, A.S.; Lijmer, J.G.; Prins, M.H.; Bonsel, G.J.; Bossuyt, P.M. The diagnostic odds ratio: A single indicator of test performance. J. Clin. Epidemiol. 2003, 56, 1129–1135. [Google Scholar] [CrossRef]
- Brenner, D.J.; Hall, E.J. Computed tomography--an increasing source of radiation exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CEUS | Dynamic CT | MRI | |
|---|---|---|---|
| Ionizing radiation | No | Yes | No |
| Nephrotoxicity | No | Yes | Yes |
| Time needed | 15 min | 10 min | 40 min |
| Technical need | Yes | No | No |
| Cost | 260 USD | 220 USD | 500 USD |
| Characteristic | Overall Participants (n = 66) |
|---|---|
| Gender (male:female) | 45:21 |
| Age (year) | 63.3 ± 9.3 |
| Body-mass index | 22.8 ± 2.4 |
| Liver characteristics | |
| normal | 33 (50.0) |
| cirrhosis | 26 (39.4) |
| fatty liver | 7 (10.6) |
| Tumor size (cm) | 1.6 ± 0.7 |
| <1 cm | 16 (24.2) |
| 1–2 cm | 27 (40.9) |
| 2–3 cm | 23 (34.8) |
| Pathology result | |
| no tumor | 4 (6.1) |
| hepatocellular carcinoma | 41 (62.1) |
| metastatic tumor | 15 (22.7) |
| benign tumor | 6 (9.1) |
| HCC | Liver Metastasis | All Malignancy | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sen | Spe | DOR (95% CI) | PPV | NPV | Sen | Spe | DOR (95% CI) | PPV | NPV | Sen | Spe | DOR (95% CI) | PPV | NPV | |
| CEUS | 87.8 | 88 | 52.8 (11.4–243) | 92.3 | 81.5 | 80 | 98 | 200 (19.1–2095) | 92.3 | 94.3 | 92.9 | 100 | 260 (12.7–5310) | 100 | 71.4 |
| MRI | 90.2 | 76 | 29.29 (7.36–116) | 86 | 82.6 | 60 | 94.1 | 24 (5.05–114) | 75 | 88.9 | 85.7 | 30 | 2.57 (0.55–12.1) | 87.3 | 27.3 |
| CT | 82.9 | 80 | 19.43 (5.44–69.4) | 87.2 | 74.1 | 66.7 | 94.1 | 32 (6.56–156) | 76.9 | 90.6 | 83.9 | 50 | 5.22 (1.25–21.8) | 90.4 | 35.7 |
| Combination * | HCC | Liver Metastasis | All Malignancy |
|---|---|---|---|
| Specificity | Specificity | Specificity | |
| CEUS + CT | 96 | 100 | 100 |
| CEUS + MRI | 92 | 100 | 100 |
| MRI + CT | 92 | 98 | 90 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiao, C.-Y.; Chen, P.-D.; Huang, K.-W. A Prospective Assessment of the Diagnostic Value of Contrast-Enhanced Ultrasound, Dynamic Computed Tomography and Magnetic Resonance Imaging for Patients with Small Liver Tumors. J. Clin. Med. 2019, 8, 1353. https://doi.org/10.3390/jcm8091353
Hsiao C-Y, Chen P-D, Huang K-W. A Prospective Assessment of the Diagnostic Value of Contrast-Enhanced Ultrasound, Dynamic Computed Tomography and Magnetic Resonance Imaging for Patients with Small Liver Tumors. Journal of Clinical Medicine. 2019; 8(9):1353. https://doi.org/10.3390/jcm8091353
Chicago/Turabian StyleHsiao, Chih-Yang, Po-Da Chen, and Kai-Wen Huang. 2019. "A Prospective Assessment of the Diagnostic Value of Contrast-Enhanced Ultrasound, Dynamic Computed Tomography and Magnetic Resonance Imaging for Patients with Small Liver Tumors" Journal of Clinical Medicine 8, no. 9: 1353. https://doi.org/10.3390/jcm8091353