Multidiscipline Stroke Post-Acute Care Transfer System: Propensity-Score-Based Comparison of Functional Status



Abstract
:1. Introduction
2. Materials and Methods
2.1. The PAC Program
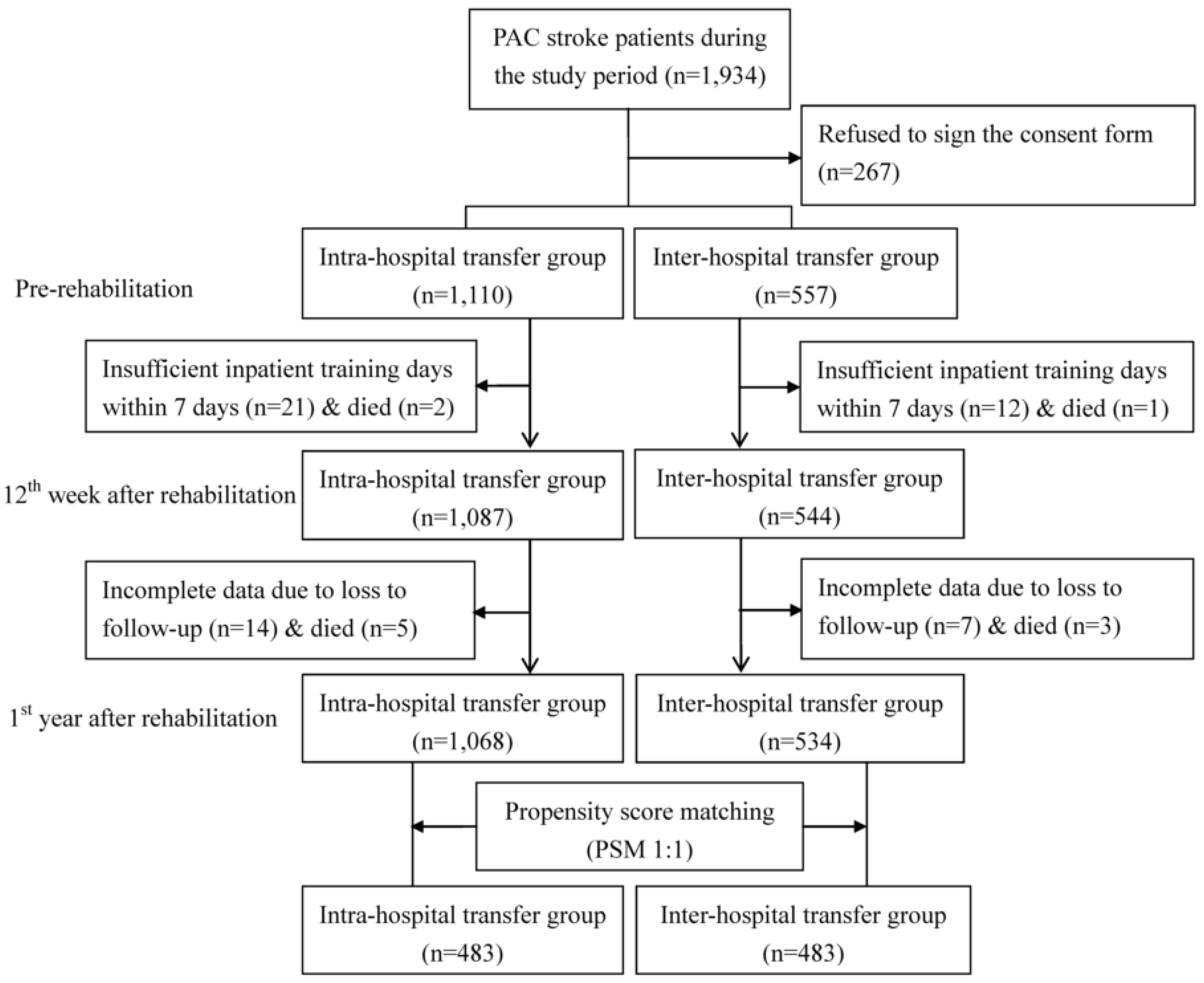
2.2. Study Design and Sample
2.3. Functional Status Instruments
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Prabhakaran, S.; Ruff, I.; Bernstein, R.A. Acute stroke intervention: A systematic review. JAMA 2015, 313, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Sturm, J.W.; Dewey, H.M.; Donnan, G.A.; Macdonell, R.A.; McNeil, J.J. Handicap after stroke: How does it relate to disability, perception of recovery, and stroke subtype? The north North East Melbourne Stroke Incidence Study (NEMESIS). Stroke 2002, 33, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Burke, R.E.; Juarez-Colunga, E.; Levy, C.; Prochazka, A.V.; Coleman, E.A.; Ginde, A.A. Rise of post-acute care facilities as a discharge destination of US hospitalizations. JAMA Intern. Med. 2015, 175, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Huckfeldt, P.J.; Mehrotra, A.; Hussey, P.S. The Relative Importance of Post-Acute Care and Readmissions for Post-Discharge Spending. Health Serv. Res. 2016, 51, 1919–1938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redberg, R.F. The role of post-acute care in variation in the Medicare program. JAMA Intern. Med. 2015, 175, 1058. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.C.; Cheng, S.H. Does pay-for-performance benefit patients with multiple chronic conditions? Evidence from a universal coverage health care system. Health Policy Plan. 2016, 31, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.C.; Chang, K.C.; Lan, C.F. Factors associated with prolonged hospital stay for acute stroke in Taiwan. Acta Neurol. Taiwan 2008, 17, 17–25. [Google Scholar] [PubMed]
- Wang, C.Y.; Chen, Y.R.; Hong, J.P.; Chan, C.C.; Chang, L.C.; Shi, H.Y. Rehabilitative post-acute care for stroke patients delivered by per-diem payment system in different hospitalization paths: A Taiwan pilot study. Int. J. Qual. Health Care 2017, 29, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.L.; Tsai, M.M.; Luo, J.Y.; Liao, W.C.; Hsu, P.S.; Chen, H.Y. Post-acute care for stroke—A retrospective cohort study in Taiwan. Patient Prefer. Adherence 2017, 11, 1309–1315. [Google Scholar] [CrossRef]
- Huang, S.T.; Yu, T.M.; Ke, T.Y.; Wu, M.J.; Chuang, Y.W.; Li, C.Y.; Chiu, C.W.; Lin, C.L.; Liang, W.M.; Chou, T.C.; et al. Intensive Periodontal Treatment Reduces Risks of Hospitalization for Cardiovascular Disease and All-Cause Mortality in the Hemodialysis Population. J. Clin. Med. 2018, 7, 344. [Google Scholar] [CrossRef]
- Cheng, C.Y.; Hsu, C.Y.; Wang, T.C.; Jeng, Y.C.; Yang, W.H. Evaluation of Cardiac Complications Following Hemorrhagic Stroke Using 5-Year Centers for Disease Control and Prevention (CDC) Database. J. Clin. Med. 2018, 7, 519. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for causal effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- D’Agostino, R.B. Tutorial in biostatistics. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Banks, J.L.; Marotta, C.A. Outcomes validity and reliability of the modified Rankin scale: Implications for stroke clinical trials: A literature review and synthesis. Stroke 2007, 38, 1091–1096. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, C.D.; Taub, N.A.; Woodrow, E.J.; Burney, P.G. Assessment of scales of disability and handicap for stroke patients. Stroke 1991, 22, 1242–1244. [Google Scholar] [CrossRef] [PubMed]
- Crary, M.A.; Mann, G.D.; Groher, M.E. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch. Phys. Med. Rehabil. 2005, 86, 1516–1520. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Alexandre, T.S.; Corona, L.P.; Nunes, D.P.; Santos, J.L.; Duarte, Y.A.; Lebrão, M.L. Disability in instrumental activities of daily living among older adults: Gender differences. Rev. Saude Publica 2014, 48, 379–389. [Google Scholar] [CrossRef]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef]
- Chou, C.Y.; Chien, C.W.; Hsueh, I.P.; Sheu, C.F.; Wang, C.H.; Hsieh, C.L. Developing a short form of the Berg Balance Scale for people with stroke. Phys. Ther. 2006, 86, 195–204. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1995, 12, 189–198. [Google Scholar] [CrossRef]
- Guo, N.W.; Lui, H.C.; Wong, P.F.; Liao, K.K.; Yan, S.H.; Lin, K.P. Chinese version and norms of the Mini-Mental State Examination. J. Rehabil. Med. Assoc. Taiwan 1988, 16, 52–59. [Google Scholar]
- Efron, B.; Tibshirani, R. An Introduction to the Bootstrap; Chapman & Hall: New York, NY, USA, 1993. [Google Scholar]
- Hsieh, C.Y.; Wu, D.P.; Sung, S.F. Trends in vascular risk factors, stroke performance measures, and outcomes in patients with first-ever ischemic stroke in Taiwan between 2000 and 2012. J. Neurol. Sci. 2017, 378, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.H.; Zhang, Z.; Ye, Q.; Ye, Z.S.; Xia, N.G. Characteristics of the ischemic stroke patients whose seizures occur at stroke presentation at a single institution in Eastern China. J. Neurol. Sci. 2018, 387, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, F.I.; Chiou, H.Y. Stroke: Morbidity, Risk Factors, and Care in Taiwan. J. Stroke 2014, 16, 59–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.; Wu, Y.L.; Ovbiagele, B. Trends in Incident and Recurrent Rates of First-Ever Ischemic Stroke in Taiwan between 2000 and 2011. J. Stroke 2016, 18, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Purvis, T.; Kilkenny, M.F.; Middleton, S.; Cadilhac, D.A. Influence of stroke coordinators on delivery of acute stroke care and hospital outcomes: An observational study. Int. J. Stroke 2018, 13, 585–591. [Google Scholar] [CrossRef]
- Bettger, J.P.; Thomas, L.; Liang, L.; Xian, Y.; Bushnell, C.D.; Saver, J.L.; Fonarow, G.C.; Peterson, E.D. Hospital Variation in Functional Recovery After Stroke. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e002391. [Google Scholar] [CrossRef]
- Graham, J.E.; Deutsch, A.; O’Connell, A.A.; Karmarkar, A.M.; Granger, C.V.; Ottenbacher, K.J. Inpatient rehabilitation volume and functional outcomes in stroke, lower extremity fracture, and lower extremity joint replacement. Med. Care 2013, 51, 404–412. [Google Scholar] [CrossRef]
- Alcusky, M.; Ulbricht, C.M.; Lapane, K.L. Postacute Care Setting, Facility Characteristics, and Poststroke Outcomes: A Systematic Review. Arch. Phys. Med. Rehabil. 2018, 99, 1124–1140. [Google Scholar] [CrossRef]
- Blattner, M.; Price, J.; Holtkamp, M.D. Socioeconomic class and universal healthcare: Analysis of stroke cost and outcomes in US military healthcare. J. Neurol. Sci. 2018, 386, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Fattore, G.; Torbica, A.; Susi, A.; Giovanni, A.; Benelli, G.; Gozzo, M.; Toso, V. The social and economic burden of stroke survivors in Italy: A prospective, incidence-based, multi-centre cost of illness study. BMC Neurol. 2012, 12, 137. [Google Scholar] [CrossRef] [PubMed]
- Rajsic, S.; Gothe, H.; Borba, H.H.; Sroczynski, G.; Vujicic, J.; Toell, T.; Siebert, U. Economic burden of stroke: A systematic review on post-stroke care. Eur. J. Health Econ. 2019, 20, 107–134. [Google Scholar] [CrossRef] [PubMed]
- Miyai, I.; Sonoda, S.; Nagai, S.; Takayama, Y.; Inoue, Y.; Kakehi, A.; Kurihara, M.; Ishikawa, M. Results of new policies for inpatient rehabilitation coverage in Japan. Neurorehabil. Neural. Repair. 2011, 25, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.N.; Lu, W.H.; Liang, C.K.; Chou, M.Y.; Chung, C.P.; Tsai, S.L.; Chen, Z.J.; Hsiao, F.Y.; Chen, L.K. Functional Outcomes, Subsequent Healthcare Utilization, and Mortality of Stroke Postacute Care Patients in Taiwan: A Nationwide Propensity Score-matched Study. J. Am. Med. Dir. Assoc. 2017, 18, 990.e7–990.e12. [Google Scholar] [CrossRef] [PubMed]
- Kuptniratsaikul, V.; Kovindha, A.; Massakulpan, P.; Permsirivanich, W.; Kuptniratsaikul, P.S. Inpatient rehabilitation services for patients after stroke in Thailand: A multi-centre study. J. Rehabil. Med. 2009, 41, 684–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, Z.H.; Hay, C.C.; Graham, J.E.; Lin, Y.L.; Karmarkar, A.M.; Ottenbacher, K.J. Social Support and Actual Versus Expected Length of Stay in Inpatient Rehabilitation Facilities. Arch. Phys. Med. Rehabil. 2016, 97, 2068–2075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, M.; Britt, E.; McHale, H.A.; Teasell, R. Length of stay benchmarks for inpatient rehabilitation after stroke. Disabil. Rehabil. 2012, 34, 1077–1081. [Google Scholar] [CrossRef] [PubMed]
- Verpillat, P.; Dorey, J.; Guilhaume-Goulant, C.; Dabbous, F.; Brunet, J.; Aballéa, S. A chart review of management of ischemic stroke patients in Germany. J. Mark. Access Health Policy 2015, 3. [Google Scholar] [CrossRef]
- Dewilde, S.; Annemans, L.; Peeters, A.; Hemelsoet, D.; Vandermeeren, Y.; Desfontaines, P.; Brouns, R.; Vanhooren, G.; Cras, P.; Michielsens, B.; et al. Modified Rankin scale as a determinant of direct medical costs after stroke. Int. J. Stroke 2017, 12, 392–400. [Google Scholar] [CrossRef]


{kind=link}
| Before Propensity Score Matching | After Propensity Score Matching | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Intra-Hospital Transfer Group (n = 1068) | Inter-Hospital Transfer Group (n = 534) | p Value | Intra-Hospital Transfer Group (n = 483) | Inter-Hospital Transfer Group (n = 483) | p Value | |
| Demographics | |||||||
| Age, years * | 65.67 ± 12.38 | 63.96 ± 13.50 | 0.024 | 63.61 ± 13.10 | 63.96 ± 13.24 | 0.834 | |
| Gender | Female | 450(42.1%) | 186(34.8%) | 0.014 | 171(35.4%) | 169(35.0%) | 0.784 |
| Male | 618(57.9%) | 348(65.2%) | 312(64.6%) | 314(65.0%) | |||
| Clinical Attributes | |||||||
| Stroke type | Ischemic | 942(88.2%) | 396(74.2%) | <0.001 | 363(75.0%) | 360(74.5%) | 0.880 |
| Hemorrhagic | 126(11.8%) | 138(25.8%) | 120(25.0%) | 123(25.5%) | |||
| Hypertension | Yes | 698(65.4%) | 405(75.8%) | <0.001 | 372(77.0%) | 367(76.0%) | 0.221 |
| Hyperlipidemia | Yes | 332(31.1%) | 227(42.5%) | <0.001 | 202(41.8%) | 206(42.6%) | 0.507 |
| Diabetes mellitus | Yes | 419(39.2) | 200(37.5%) | 0.570 | 182(37.7%) | 181(37.5%) | 0.990 |
| Atrial fibrillation | Yes | 67(6.3%) | 55(10.3%) | 0.013 | 47(9.7%) | 49(10.1%) | 0.887 |
| Previous stroke | Yes | 173(16.2%) | 98(18.4%) | 0.803 | 87(18.0%) | 89(18.4%) | 0.879 |
| Quality of Medical Care | |||||||
| Acute care LOS, days * | 13.01 ± 27.83 | 24.45 ± 34.61 | <0.001 | 23.75 ± 11.84 | 24.50 ± 11.56 | 0.356 | |
| PAC LOS, days * | 31.52 ± 17.75 | 37.1 ± 12.59 | <0.001 | 35.75 ± 12.34 | 36.50 ± 11.88 | 0.506 | |
| Pre-rehabilitation functional status | |||||||
| BI * | 41.91 ± 23.10 | 34.67 ± 23.48 | <0.001 | 35.75 ± 20.11 | 34.00 ± 18.21 | 0.269 | |
| FOIS * | 5.95 ± 3.04 | 5.38 ± 2.25 | <0.001 | 5.53 ± 2.75 | 5.14 ± 2.84 | 0.927 | |
| EQ5D * | 10.67 ± 1.86 | 10.40 ±1.78 | 0.015 | 10.80 ± 1.82 | 10.93 ± 2.05 | 0.261 | |
| IADL * | 1.41 ± 1.20 | 1.15 ± 1.12 | <0.001 | 1.32 ± 1.14 | 1.27 ± 1.05 | 0.694 | |
| BBS * | 15.30 ± 14.99 | 16.91 ± 17.27 | 0.097 | 14.00 ± 17.26 | 15.50 ± 17.71 | 0.972 | |
| MMSE * | 20.15 ± 7.90 | 18.50 ± 9.66 | 0.001 | 20.75 ± 11.15 | 19.75 ± 10.47 | 0.908 | |
| Functional Status Measure | Group | Before Rehabilitation (T1) | 12th Week After Rehabilitation (T2) | Difference † | p Value | First Year After Rehabilitation (T3) | Difference † | p Value |
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||||||
| BI | Intra-hospital transfer | 41.91 ± 23.10 | 51.50 ± 24.10 | 9.59 | <0.001 | 68.84 ± 26.49 | 17.34 | <0.001 |
| Inter-hospital transfer | 34.67 ± 23.48 | 42.28 ± 25.96 | 7.61 | <0.001 | 54.29 ± 27.20 | 12.01 | 0.002 | |
| Difference ‡ | 7.24 | 9.22 | 1.98 | <0.001 | 14.55 | 5.33 | <0.001 | |
| FOIS | Intra-hospital transfer | 5.95 ± 3.04 | 5.98 ± 1.82 | 0.03 | 0.037 | 6.41 ± 1.32 | 0.43 | 0.006 |
| Inter-hospital transfer | 5.38 ± 2.25 | 5.68 ± 1.89 | 0.30 | 0.002 | 6.26 ± 1.47 | 0.58 | 0.044 | |
| Difference ‡ | 0.57 | 0.30 | −0.27 | <0.001 | 0.15 | −0.15 | <0.001 | |
| EQ5D | Intra-hospital transfer | 10.67 ± 1.86 | 9.81 ± 1.65 | −0.86 | <0.001 | 8.15 ± 2.23 | −1.66 | <0.001 |
| Inter-hospital transfer | 10.40 ± 1.79 | 10.02 ± 1.70 | −0.38 | 0.004 | 9.19 ± 1.88 | −0.83 | 0.001 | |
| Difference ‡ | 0.27 | −0.21 | −0.48 | <0.001 | −1.04 | −0.83 | <0.001 | |
| IADL | Intra-hospital transfer | 1.41 ± 1.20 | 1.84 ± 1.32 | 0.43 | <0.001 | 2.87 ± 1.75 | 1.03 | <0.001 |
| Inter-hospital group | 1.15 ± 1.13 | 1.36 ± 1.31 | 0.21 | 0.054 | 1.86 ± 1.57 | 0.5 | 0.023 | |
| Difference ‡ | 0.26 | 0.48 | 0.22 | <0.001 | 1.01 | 0.53 | <0.001 | |
| BBS | Intra-hospital transfer | 15.30 ± 14.99 | 26.32 ± 17.56 | 11.02 | <0.001 | 34.58 ± 17.79 | 8.26 | <0.001 |
| Inter-hospital transfer | 16.91 ± 17.27 | 24.40 ± 19.25 | 7.49 | <0.001 | 29.91 ± 19.35 | 5.51 | 0.022 | |
| Difference ‡ | −1.61 | 1.92 | 3.53 | <0.001 | 4.67 | 2.75 | <0.001 | |
| MMSE | Intra-hospital transfer | 20.15 ± 7.90 | 21.62 ± 7.79 | 1.47 | 0.020 | 22.73 ± 7.39 | 1.11 | 0.078 |
| Inter-hospital transfer | 18.50 ± 9.66 | 19.64 ± 10.80 | 1.14 | 0.090 | 21.25 ± 9.41 | 1.61 | 0.260 | |
| Difference ‡ | 1.65 | 1.98 | 0.33 | <0.001 | 1.48 | −0.5 | <0.001 | |
| Model | BI | FOIS | EQ5D | IADL | BBS | MMSE | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| R2 | R2 Change | R2 | R2 Change | R2 | R2 Change | R2 | R2 Change | R2 | R2 Change | R2 | R2 Change | |
| 1st level | 0.64 | - | 0.28 | - | 0.38 | - | 0.51 | - | 0.48 | - | 0.79 | - |
| 2nd level | 0.64 | 0.00 | 0.28 | 0.00 | 0.39 | 0.01 | 0.52 | 0.01 | 0.48 | 0.00 | 0.79 | 0.00 |
| 3rd level | 0.64 | 0.00 | 0.29 | 0.01 | 0.44 | 0.06 | 0.55 | 0.04 | 0.51 | 0.03 | 0.79 | 0.00 |
| 4th level | 0.64 | 0.00 | 0.29 | 0.01 | 0.44 | 0.06 | 0.55 | 0.04 | 0.51 | 0.03 | 0.79 | 0.00 |
| 5th level | 0.67 | 0.03 | 0.29 | 0.01 | 0.49 | 0.11 | 0.58 | 0.07 | 0.53 | 0.05 | 0.79 | 0.00 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.-Y.; Hsien, H.-H.; Hung, K.-W.; Lin, H.-F.; Chiou, H.-Y.; Yeh, S.-C.J.; Yeh, Y.-J.; Shi, H.-Y. Multidiscipline Stroke Post-Acute Care Transfer System: Propensity-Score-Based Comparison of Functional Status. J. Clin. Med. 2019, 8, 1233. https://doi.org/10.3390/jcm8081233
Wang C-Y, Hsien H-H, Hung K-W, Lin H-F, Chiou H-Y, Yeh S-CJ, Yeh Y-J, Shi H-Y. Multidiscipline Stroke Post-Acute Care Transfer System: Propensity-Score-Based Comparison of Functional Status. Journal of Clinical Medicine. 2019; 8(8):1233. https://doi.org/10.3390/jcm8081233
Chicago/Turabian StyleWang, Chung-Yuan, Hong-Hsi Hsien, Kuo-Wei Hung, Hsiu-Fen Lin, Hung-Yi Chiou, Shu-Chuan Jennifer Yeh, Yu-Jo Yeh, and Hon-Yi Shi. 2019. "Multidiscipline Stroke Post-Acute Care Transfer System: Propensity-Score-Based Comparison of Functional Status" Journal of Clinical Medicine 8, no. 8: 1233. https://doi.org/10.3390/jcm8081233