Shock Index Predicts Outcome in Patients with Suspected Sepsis or Community-Acquired Pneumonia: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection Criteria
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Assessment
2.6. Data Analysis
3. Results
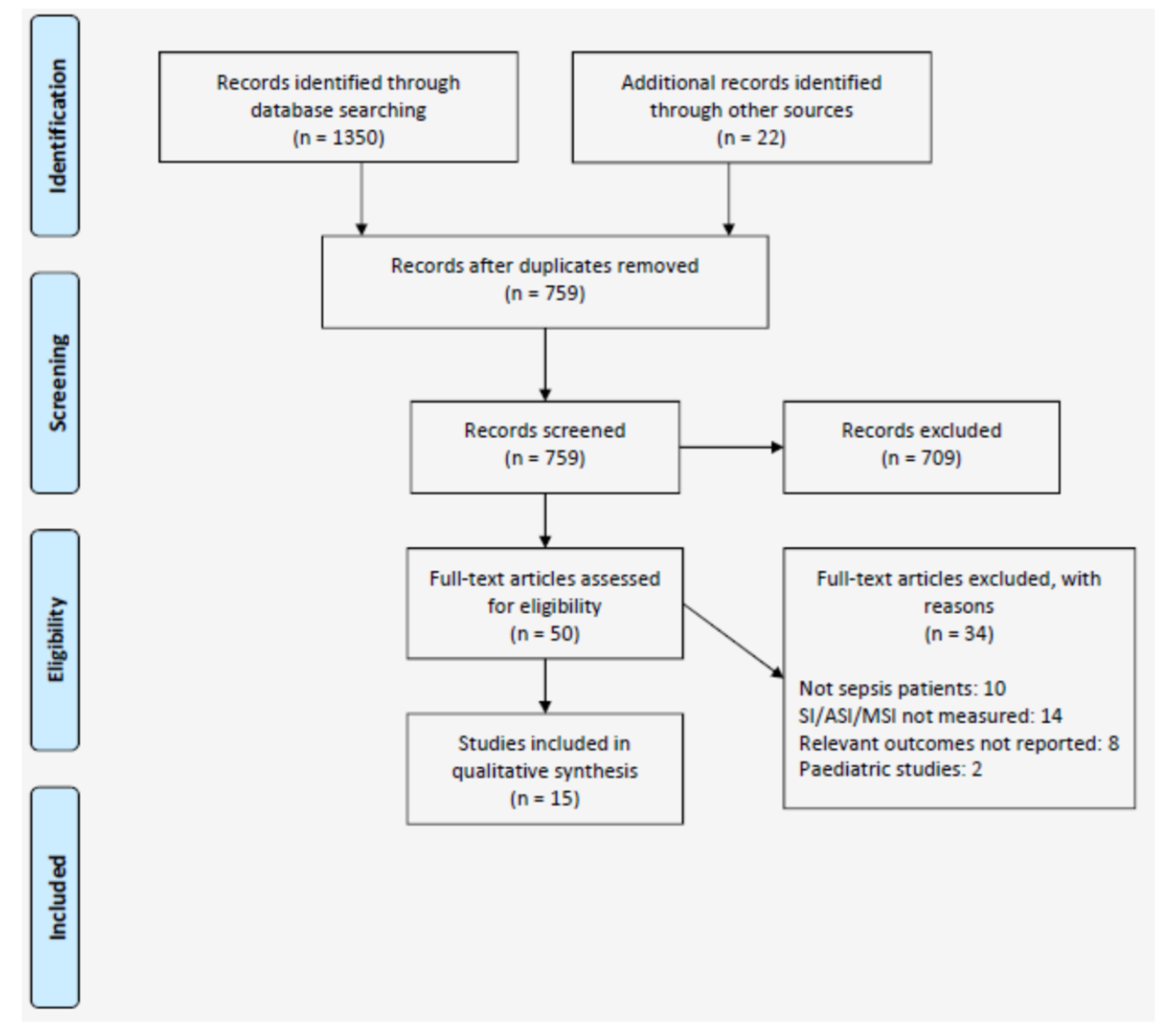
3.1. Search Results
3.2. Quality Assessment
3.3. Characteristics of Studies Included
3.3.1. Sepsis
3.3.2. Community-Acquired Pneumonia
3.4. Shock Index in Patients with Sepsis
3.4.1. Shock Index as a Predictor of Mortality in Patients with Sepsis
3.4.2. Shock Index as a Predictor of Morbidity in Sepsis
3.4.3. Modifications of Shock Index in Patients with Sepsis
3.5. Shock Index in Patients with CAP
3.5.1. Shock Index and Adjusted Shock Index as a Predictor of Mortality and Morbidity in Patients with CAP
3.5.2. Modifications of Shock Index and Adjusted Shock Index in Patients with CAP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). J. Am. Med. Assoc. 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Daniels, R.; Nutbeam, T. The Sepsis Manual, 4th ed.; The UK Sepsis Trust: Birmingham, UK, 2017; pp. 1–120. [Google Scholar]
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.J.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K. Assessment of global incidence and mortality of hospital-treated sepsis current estimates and limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef]
- Walden, A.P.; Clarke, G.M.; McKechnie, S.; Hutton, P.; Gordon, A.C.; Rello, J.; Chiche, J.D.; Stueber, F.; Garrard, C.S.; Hinds, C.J. Patients with community acquired pneumonia admitted to European intensive care units: An epidemiological survey of the GenOSept cohort. Crit. Care 2014, 18, R58. [Google Scholar] [CrossRef]
- Levy, M.M.; Dellinger, R.P.; Townsend, S.R.; Linde-Zwirble, W.T.; Marshall, J.C.; Bion, J.; Schorr, C.; Artigas, A.; Ramsay, G.; Beale, R.; et al. The surviving sepsis campaign: Results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med. 2010, 36, 222–231. [Google Scholar] [CrossRef]
- Daniels, R.; Nutbeam, T.; McNamara, G.; Galvin, C. The sepsis six and the severe sepsis resuscitation bundle: A prospective observational cohort study. Emerg. Med. J. 2011, 28, 507–512. [Google Scholar] [CrossRef]
- Liu, V.; Kipnis, P.; Rizk, N.W.; Escobar, G.J. Adverse outcomes associated with delayed intensive care unit transfers in an integrated healthcare system. J. Hosp. Med. 2012, 7, 224–230. [Google Scholar] [CrossRef]
- Frost, S.A.; Alexandrou, E.; Bogdanovski, T.; Salamonson, Y.; Parr, M.J.; Hillman, K.M. Unplanned admission to intensive care after emergency hospitalisation: Risk factors and development of a nomogram for individualising risk. Resuscitation 2009, 80, 224–230. [Google Scholar] [CrossRef]
- Delgado, M.K.; Liu, V.; Pines, J.M.; Kipnis, P.; Gardner, M.N.; Escobar, G.J. Risk factors for unplanned transfer to intensive care within 24 h of admission from the emergency department in an integrated healthcare system. J. Hosp. Med. 2013, 8, 13–19. [Google Scholar] [CrossRef]
- Churpek, M.M.; Snyder, A.; Han, X.; Sokol, S.; Pettit, N.; Howell, M.D.; Edelson, D.P. Quick sepsis-related organ failure assessment, systemic inflammatory response syndrome, and early warning scores for detecting clinical deterioration in infected patients outside theintensive care unit. Am. J. Respir. Crit. Care Med. 2017, 195, 906–911. [Google Scholar] [CrossRef]
- Goulden, R.; Hoyle, M.C.; Monis, J.; Railton, D.; Riley, V.; Martin, P.; Martina, R.; Nsutebu, E. QSOFA, SIRS and NEWS for predicting inhospital mortality and ICU admission in emergency admissions treated as sepsis. Emerg. Med. J. 2018, 35, 345–349. [Google Scholar] [CrossRef]
- Song, J.U.; Sin, C.K.; Park, H.K.; Shim, S.R.; Lee, J. Performance of the quick Sequential (sepsis-related) Organ Failure Assessment score as a prognostic tool in infected patients outside the intensive care unit: A systematic review and meta-analysis. Crit. Care 2018, 22, 1–13. [Google Scholar] [CrossRef]
- Olaussen, A.; Blackburn, T.; Mitra, B.; Fitzgerald, M. Review article: Shock Index for prediction of critical bleeding post-trauma: A systematic review. Emerg. Med. Australas 2014, 26, 223–228. [Google Scholar] [CrossRef]
- St-Cyr Bourque, J.; Cliché, J.; Chauny, J.; Daoust, R.; Paquet, J.; Piette, E. Accuracy of the shock index and various modif ed shock indexes to predict early mortality in patients suffering from gastrointestinal haemorrhage. Crit. Care 2013, 17, 219. [Google Scholar]
- Toosi, M.S.; Merlino, J.D.; Leeper, K.V. Prognostic Value of the Shock Index Along With Transthoracic Echocardiography in Risk Stratification of Patients With Acute Pulmonary Embolism. Am. J. Cardiol. 2008, 101, 700–705. [Google Scholar] [CrossRef]
- Myint, P.K.; Sheng, S.; Xian, Y.; Matsouaka, R.; Reeves, M.; Saver, J.L.; Bhatt, D.L.; Fonarow, G.C.; Schwamm, L.H.; Smith, E.E. Shock index predicts patient-related clinical outcomes in stroke. J. Am. Heart Assoc. 2018, 7, 1–12. [Google Scholar] [CrossRef]
- Musonda, P.; Sankaran, P.; Myint, P.K.; Kamath, A.V.; Subramanian, D.N.; Smith, A.C.; Prentice, P.; Tariq, S.M. Prediction of mortality in community-acquired pneumonia in hospitalized patients. Am. J. Med. Sci. 2011, 324, 489–493. [Google Scholar] [CrossRef]
- Liu, Y.C.; Liu, J.H.; Fang, Z.A.; Shan, G.L.; Xu, J.; Qi, Z.W.; Zhu, H.-D.; Wang, Z.; Yu, X.-Z. Modified shock index and mortality rate of emergency patients. World J. Emerg. Med. 2012, 3, 114–117. [Google Scholar] [CrossRef] [Green Version]
- Curtain, J.P.; Sankaran, P.; Kamath, A.V.; Myint, P.K. The usefulness of confusion, urea, respiratory rate, and shock index or adjusted shock index criteria in predicting combined mortality and/or ICU admission compared to CURB-65 in community-acquired pneumonia. Biomed. Res. Int. 2013, 1, 1–6. [Google Scholar] [CrossRef]
- Eldaboosy, S.A.M.; Halima, K.M.; Shaarawy, A.T.; Kanany, H.M.; Elgamal, E.M.; El-Gendi, A.A.; Nour, M.O.; Abuelhassan, U.G.; Alshamery, H.A. Comparison between CURB-65, PSI, and SIPF scores as predictors of ICU admission and mortality in community-acquired pneumonia. Egypt J. Crit. Care Med. 2015, 3, 37–44. [Google Scholar] [CrossRef]
- Nüllmann, H.; Pflug, M.A.; Wesemann, T.; Heppner, H.J.; Pientka, P.; Thiem, U. External validation of the CURSI criteria (confusion, urea, respiratory rate and shock index) in adults hospitalised for community-acquired pneumonia. BMC Infect. Dis. 2014, 14. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 337–384. [Google Scholar] [CrossRef]
- Baez, A.A.; Hanudel, P.; Wilcox, S.R. The prehospital sepsis project: Out-of-hospital physiologic predictors of sepsis outcomes. Prehosp. Disaster Med. 2013, 28, 632–635. [Google Scholar] [CrossRef]
- Jayaprakash, N.; Gajic, O.; Frank, R.D.; Smischney, N. Elevated modified shock index in early sepsis is associated with myocardial dysfunction and mortality. J. Crit. Care 2018, 43, 30–35. [Google Scholar] [CrossRef]
- Chung, J.Y.; Hsu, C.C.; Chen, J.H.; Chen, W.L.; Lin, H.J.; Guo, H.R.; Huang, C.C. Shock index predicted mortality in geriatric patients with influenza in the emergency department. Am. J. Emerg. Med. 2019, 37, 391–394. [Google Scholar] [CrossRef]
- Lombaard, H.; Adam, S.; Makin, J.; Sebola, P. An audit of the initial resuscitation of severely ill patients presenting with septic incomplete miscarriages at a tertiary hospital in South Africa. BMC Pregnancy Childbirth 2015, 15, 1–5. [Google Scholar] [CrossRef]
- Wira, C.; Francis, M.; Bhat, S.; Ehrman, R.; Conner, D.; Siegel, M. The Shock Index as a Predictor of Vasopressor Use in Emergency Department Patients with Severe Sepsis. West. J. Emerg. Med. 2014, 15, 60–66. [Google Scholar] [CrossRef] [Green Version]
- Yussof, S.J.M.; Zakaria, M.I.; Mohamed, F.L.; Bujang, M.A.; Lakshmanan, S.; Asaari, A.H. Value of shock index in prognosticating the short term outcome of death for patients presenting with severe sepsis and septic shock in the emergency department. Med. J. Malays. 2012, 65, 406–411. [Google Scholar]
- Sankaran, P.; Kamath, A.V.; Tariq, S.M.; Ruffell, H.; Smith, A.C.; Prentice, P.; Subramanian, D.N.; Musonda, P.; Myint, P.K. Are shock index and adjusted shock index useful in predicting mortality and length of stay in community-acquired pneumonia? Eur. J. Intern. Med. 2011, 22, 282–285. [Google Scholar] [CrossRef]
- Myint, P.K.; Musonda, P.; Sankaran, P.; Subramanian, D.N.; Ruffell, H.; Smith, A.C.; Prentice, P.; Tariq, S.M.; Kamath, A.V. Confusion, urea, respiratory rate and shock index or adjusted shock index (CURSI or CURASI) criteria predict mortality in community-acquired pneumonia. Eur. J. Intern. Med. 2010, 21, 429–433. [Google Scholar] [CrossRef]
- Berger, T.; Green, J.; Horeczko, T.; Hagar, Y.; Garg, N.; Suarez, A.; Panacek, E.; Shapiro, N. Shock Index and Early Recognition of Sepsis in the Emergency Department: Pilot Study. West J. Emerg. Med. 2013, 14, 168–174. [Google Scholar] [CrossRef] [Green Version]
- Jaimes, F.v.; Farbiarz, J.; Alvarez, D.; Martínez, C.; Martinez, C. Comparison between logistic regression and neural networks to predict death in patients with suspected sepsis in the emergency room. Crit. Care 2005, 9, R150–R156. [Google Scholar] [CrossRef] [Green Version]
- Talmor, D.; Jones, A.E.; Rubinson, L.; Howell, M.D.; Shapiro, N.I. Simple triage scoring system predicting death and the need for critical care resources for use during epidemics. Crit. Care Med. 2007, 35, 1251–1256. [Google Scholar] [CrossRef]
- Huang, B.; Yang, Y.; Zhu, J.; Liang, Y.; Tan, H.; Yu, L.; Gao, X.; Li, J. Usefulness of the admission shock index for predicting short-term outcomes in patients with ST-segment elevation myocardial infarction. Am. J. Cardiol. 2014, 114, 1315–1321. [Google Scholar] [CrossRef]
- Holler, J.G.; Bech, C.N.; Henriksen, D.P.; Mikkelsen, S.; Pedersen, C.; Lassenm, A.T. Nontraumatic hypotension and shock in the emergency department and the prehospital setting, prevalence, etiology, and mortality: A systematic review. PLoS ONE 2015, 10, ee0119331. [Google Scholar] [CrossRef]


{kind=link}
| Author/Year | Design | n | Location | Setting | Study Population | Mortality (%) | Admitted to ICU (%) | Index Test and Range | Outcome(s) of Interest |
|---|---|---|---|---|---|---|---|---|---|
| Sepsis studies | |||||||||
| Baez et al., 2013 [23] | Retrospective cohort | 63 | USA; 1 centre | Pre-hospital | Adults (≥ 18) with ICD-9 diagnostic code of sepsis, severe sepsis or septic shock | 34.9 | 68.3 | SI ≥ 0.7 | In-hospital mortality ICU admission |
| Berger et al., 2013 [31] | Retrospective cohort | 2524 | USA; 1 centre | ED | Adults (≥ 21) screened for sepsis using standardised blood order | 13.5 | - | SI ≥ 0.7; SI ≥ 1 | 28-day mortality |
| Chung et al., 2019 [25] | Retrospective cohort | 409 | Taiwan; 1 centre | ED | Elderly patients (≥ 65) with pyrexia confirmed influenza | 4.9 | - | SI ≥ 1.0 | 30-day mortality |
| Jaimes et al., 2005 [32] | Prospective cohort | 533 | Colombia; 2 centres | ED | Adults (≥ 16) suspected sepsis (2012 definition) | 18.9 | 14.1 | SI; full range | Multivariable modelling to predict 28-day mortality |
| Jayarakash et al., 2018 [24] | Retrospective cohort | 578 | USA; 1 centre | Medical ICU | Adults (≥ 18) admitted to ICU with severe sepsis or septic shock (2012 definition) | 19.9 | 100 | MSI ≥ 1.3 | In-hospital mortality |
| Lombaard et al., 2015 [26] | Audit | 47 | South Africa; 1 centre | Maternity ward | Adult patients with septic incomplete abortion | 19.2 | - | SI ≥ 1.0 | In-hospital mortality |
| Talmor et al., 2007 [33] | Prospective cohort | 3260 | Israel; 1 centre | ED | Adults (≥ 18) who had blood cultures taken | 4.7 | 12 | SI ≥ 1.0 | In-hospital mortality or ICU |
| Wira et al., 2014 [27] | Retrospective cohort | 295 | USA; 1 centre | ED | Adults (≥ 18) with severe sepsis (2012 definition) | 15.6 | - | SI ≥ 0.8 for ≥ 80% of ED values | Vasopressor dependence by 72-h 28-day mortality |
| Yussof et al., 2012 [28] | Retrospective cohort | 50 | Malaysia; 1 centre | ED | Adults (≥ 18) triaged to resuscitation area with sepsis or septic shock (2012 definition) | 54% | - | SI; entire range at presentation and 2 h | In-hospital mortality |
| Community-acquired pneumonia (CAP) studies | |||||||||
| Curtain et al., 2013 [19] | Prospective cohort | 95 | UK; 1 centre | Hospital ward | Adults (≥ 18) admitted with CAP (symptoms and new CXR shadow) | 8.4% | 9.5% | SI and ASI ≥ 1.0, as part of CURSI, CURASI score | 6-week mortality |
| Eldaboosy et al., 2015 [20] | Retrospective cohort | 100 | Egypt and Saudi Arabia; 2 centres | Hospital ward | Adults admitted with CAP (symptoms and new CXR shadow) | 9% | 34% | SI ≥ 0.7, as part of SIPF score | In-hospital mortality ICU admission |
| Musonda et al., 2011 [17] | Prospective cohort | 190 | UK; 3 centres | AMAU | Adults (≥ 18) admitted with CAP (symptoms and new CXR shadow) | 28.4% | - | SI ≥ 1.0, as part of CARSI and CARASI score | 42-day mortality |
| Myint et al., 2010 [30] | Prospective cohort | 190 | UK; 3 centres | AMAU | Adults (≥ 18) admitted with CAP (symptoms and new CXR shadow) | 28.4% | - | SI ≥ 1.0, as part of CURSI and CURASI score | 42-day mortality |
| Nullmann et al., 2014 [21] | Retrospective cohort | 553 | Germany; 1 centre | Hospital ward | Adults (≥ 18) admitted with CAP (symptoms and new CXR shadow) | 10.7% | 10.5% | SI ≥ 1.0, as part of CURSI score | 30-day mortality |
| Sankaran 2011 [29] | Prospective cohort | 190 | UK; 3 centres | AMAU | Adults (≥ 18) admitted with CAP (symptoms and new CXR shadow) | 28.4% | - | SI ≥ 1.0 ASI ≥ 1.0 | 42-day mortality |
| Author/Year | n | SI Threshold | Mortality (%) | Test Characteristics for Prediction of Mortality | ||||
|---|---|---|---|---|---|---|---|---|
| Sens | Spec | PPV | NPV | OR | ||||
| Baez et al., 2013 [23] | 63 | SI ≥ 0.7 | 34.9 | - | - | - | - | 1.66 (0.59–4.65) |
| Berger et al., 2013 [31] | 2524 | SI ≥ 0.7 | 13.5 | 0.71 (0.66–0.76) | 0.41 (0.39–0.43) | 0.17 (0.16–0.18) | 0.89 (0.88–0.91) | 1.68 (1.32–2.14) |
| - | SI ≥ 1.0 | - | 0.32 (0.27–0.36) | 0.79 (0.77–0.81) | 0.23 (0.20–0.26) | 0.85 (0.84–0.86) | 2.24 (1.81–2.91)) | |
| Chung et al., 2019 [25] | 409 | SI ≥ 1.0 | 4.9 | 0.30 (0.12–0.54) | 0.94 (0.91–0.96) | 0.21 (0.11–0.36) | 0.96 (0.95–0.97) | 6.78 (2.39–19.29) |
| Lombbard et al., 2015 [26] | 47 | SI ≥ 1.0 | 19.2 | 0.77 (0.40–0.97) | 0.29 (0.15–0.46) | 0.21 (0.15–0.28) | 0.85 (0.25–0.54) | 1.43 (0.26–7.97) |
| Talmor et al., 2007 [33] | 3260 | SI ≥ 1.0 | 4.7 | - | - | - | - | 2.8 (1.8–4.2) |
| Wira et al., 2014 [27] | 295 | SI ≥ 0.8 for > 80% of ED measurements | 15.6 | 0.59 (0.43–0.73) | 0.55 (0.48–0.61) | 0.19 (0.15–0.24) | 0.88 (0.83–0.91) | 1.71 (0.90–3.23) |
| Yussof et al., 2012 [28] | 50 | SI ≥ 1.2 on admission | 54 | 0.73 | 0.45 | - | - | - |
| - | SI ≥ 1.0 at 2 h | - | 0.81 | 0.79 | - | - | - | |
| Author/Year | n | SI Threshold | Mortality (%) | Test Characteristics for Prediction of Mortality | ||||
|---|---|---|---|---|---|---|---|---|
| Sensitivity | Specificity | PPV | NPV | OR | ||||
| Nullmann et al., 2014 [21] | 443 | SI ≥ 1.0 | 10.7 | 0.25 (0.15–0.38) | 0.87 (0.84–0.90) | 0.18 (0.12–0.26) | 0.92 (0.90–0.92) | 2.72 (1.42–5.21) |
| Sankaran 2011 [29] | 190 | SI ≥ 1.0 | 28.4 | 0.28 (0.16–0.41) | 0.83 (0.75–0.89) | 0.39 (0.27–0.54) | 0.74 (0.71–0.78) | 1.89 (0.90–3.98) |
| - | ASI ≥ 1.0 | - | 0.22 (0.12–0.36) | 0.90 (0.83–0.94) | 0.45 (0.30–0.63) | 0.74 (0.71–0.77) | 2.49 (1.07–5.81) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Middleton, D.J.; Smith, T.O.; Bedford, R.; Neilly, M.; Myint, P.K. Shock Index Predicts Outcome in Patients with Suspected Sepsis or Community-Acquired Pneumonia: A Systematic Review. J. Clin. Med. 2019, 8, 1144. https://doi.org/10.3390/jcm8081144
Middleton DJ, Smith TO, Bedford R, Neilly M, Myint PK. Shock Index Predicts Outcome in Patients with Suspected Sepsis or Community-Acquired Pneumonia: A Systematic Review. Journal of Clinical Medicine. 2019; 8(8):1144. https://doi.org/10.3390/jcm8081144
Chicago/Turabian StyleMiddleton, David J., Toby O. Smith, Rachel Bedford, Mark Neilly, and Phyo Kyaw Myint. 2019. "Shock Index Predicts Outcome in Patients with Suspected Sepsis or Community-Acquired Pneumonia: A Systematic Review" Journal of Clinical Medicine 8, no. 8: 1144. https://doi.org/10.3390/jcm8081144