Prevalence of Thyroid Disease in Patients Surgically Treated for Pituitary Disease

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Patients
2.2. Definitions of the Diseases
2.3. Statistical Analysis
3. Results
3.1. Prevalence of Thyroid Disease Before TSA
3.2. Prevalence of Thyroid Disease According to Sex
3.3. Prevalence of Thyroid Disease According to Age
3.4. Prevalence of Thyroid Disease According to the Type of Pituitary Disease
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kasper, D.; Fauci, A.; Hauser, S.; Longo, D.; Jameson, J. Harrison’s Principles of Internal Medicine; McGraw-Hill Education: New York, NY, USA, 2015. [Google Scholar]
- Dayan, C.M. Interpretation of thyroid function tests. Lancet 2001, 357, 619–624. [Google Scholar] [CrossRef]
- Onnestam, L.; Berinder, K.; Burman, P.; Dahlqvist, P.; Engstrom, B.E.; Wahlberg, J.; Nystrom, H.F. National incidence and prevalence of tsh-secreting pituitary adenomas in sweden. J. Clin. Endocrinol. Metab. 2013, 98, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Persani, L. Clinical review: Central hypothyroidism: Pathogenic, diagnostic, and therapeutic challenges. J. Clin. Endocrinol. Metab. 2012, 97, 3068–3078. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Liu, S.; Yang, Z.; Shi, Y.B. Ectopic thyrotropin secreting pituitary adenoma concomitant with papillary thyroid carcinoma: Case report. Medicine 2017, 96, e8912. [Google Scholar] [CrossRef] [PubMed]
- Gasperi, M.; Martino, E.; Manetti, L.; Arosio, M.; Porretti, S.; Faglia, G.; Mariotti, S.; Colao, A.M.; Lombardi, G.; Baldelli, R.; et al. Prevalence of thyroid diseases in patients with acromegaly: Results of an italian multi-center study. J. Endocrinol. Investig. 2002, 25, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Babey, M.; Sahli, R.; Vajtai, I.; Andres, R.H.; Seiler, R.W. Pituitary surgery for small prolactinomas as an alternative to treatment with dopamine agonists. Pituitary 2011, 14, 222–230. [Google Scholar] [CrossRef]
- Kreutzer, J.; Buslei, R.; Wallaschofski, H.; Hofmann, B.; Nimsky, C.; Fahlbusch, R.; Buchfelder, M. Operative treatment of prolactinomas: Indications and results in a current consecutive series of 212 patients. Eur. J. Endocrinol. 2008, 158, 11–18. [Google Scholar] [CrossRef]
- Katznelson, L.; Laws, E.R., Jr.; Melmed, S.; Molitch, M.E.; Murad, M.H.; Utz, A.; Wass, J.A. Acromegaly: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2014, 99, 3933–3951. [Google Scholar] [CrossRef]
- Wilson, C.B. Surgical management of pituitary tumors. J. Clin. Endocrinol. Metab. 1997, 82, 2381–2385. [Google Scholar] [CrossRef]
- Nieman, L.K.; Biller, B.M.; Findling, J.W.; Murad, M.H.; Newell-Price, J.; Savage, M.O.; Tabarin, A. Treatment of cushing’s syndrome: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2015, 100, 2807–2831. [Google Scholar] [CrossRef]
- Park, S.H.; Hwang, S.; Han, S.; Shin, D.Y.; Lee, E.J. Thyroid isthmus length and iodine turnover as predictors of successful radioactive iodine therapy in patients with graves’ disease. Int. J. Endocrinol. 2017, 2017, 7354673. [Google Scholar] [CrossRef]
- Park, S.; Oh, C.M.; Cho, H.; Lee, J.Y.; Jung, K.W.; Jun, J.K.; Won, Y.J.; Kong, H.J.; Choi, K.S.; Lee, Y.J.; et al. Association between screening and the thyroid cancer “epidemic” in south korea: Evidence from a nationwide study. BMJ 2016, 355, i5745. [Google Scholar] [CrossRef]
- Kim, W.G.; Kim, W.B.; Woo, G.; Kim, H.; Cho, Y.; Kim, T.Y.; Kim, S.W.; Shin, M.H.; Park, J.W.; Park, H.L.; et al. Thyroid stimulating hormone reference range and prevalence of thyroid dysfunction in the korean population: Korea national health and nutrition examination survey 2013 to 2015. Endocrinol. Metab. 2017, 32, 106–114. [Google Scholar] [CrossRef]
- Kwon, H.; Jung, J.H.; Han, K.D.; Park, Y.G.; Cho, J.H.; Lee, D.Y.; Han, J.M.; Park, S.E.; Rhee, E.J.; Lee, W.Y. Prevalence and annual incidence of thyroid disease in korea from 2006 to 2015: A nationwide population-based cohort study. Endocrinol. Metab. 2018, 33, 260–267. [Google Scholar] [CrossRef]
- Korean Statistical Information Service. Cancer Statistics in Korea. Available online: http://kosis.kr/statHtml/statHtml.do?orgId=117&tblId=DT_117N_A00124&vw_cd=MT_ZTITLE&list_id=101_11744&seqNo=&lang_mode=ko&language=kor&obj_var_id=&itm_id=&conn_ (accessed on 29 April 2019).
- Lee, Y.; Ku, C.R.; Kim, E.H.; Hong, J.W.; Lee, E.J.; Kim, S.H. Early prediction of long-term response to cabergoline in patients with macroprolactinomas. Endocrinol. Metab. 2014, 29, 280–292. [Google Scholar] [CrossRef]
- Beck-Peccoz, P.; Persani, L.; Mannavola, D.; Campi, I. Pituitary tumours: Tsh-secreting adenomas. Best Pract. Res. Clin. Endocrinol. Metab. 2009, 23, 597–606. [Google Scholar] [CrossRef]
- Seo, G.H.; Chung, J.H. Incidence and prevalence of overt hypothyroidism and causative diseases in Korea as determined using claims data provided by the health insurance review and assessment service. Endocrinol. Metab. 2015, 30, 288–296. [Google Scholar] [CrossRef]
- Wong, A.; Eloy, J.A.; Couldwell, W.T.; Liu, J.K. Update on prolactinomas. Part 1: Clinical manifestations and diagnostic challenges. J. Clin. Neurosci. 2015, 22, 1562–1567. [Google Scholar] [CrossRef]
- Iglesias, P.; Arcano, K.; Trivino, V.; Garcia-Sancho, P.; Diez, J.J.; Villabona, C.; Cordido, F. Prevalence, clinical features, and natural history of incidental clinically non-functioning pituitary adenomas. Horm. Metab. Res. 2017, 49, 654–659. [Google Scholar] [CrossRef]
- Lim, C.T.; Korbonits, M. Update on the clinicopathology of pituitary adenomas. Endocr. Pract. 2018, 24, 473–488. [Google Scholar] [CrossRef]
- Duick, D.S.; Wahner, H.W. Thyroid axis in patients with cushing’s syndrome. Arch. Intern. Med. 1979, 139, 767–772. [Google Scholar] [CrossRef]
- Cohan, P.; Foulad, A.; Esposito, F.; Martin, N.A.; Kelly, D.F. Symptomatic rathke’s cleft cysts: A report of 24 cases. J. Endocrinol. Investig. 2004, 27, 943–948. [Google Scholar] [CrossRef]
- Gupta, V.; Lee, M. Central hypothyroidism. Indian J. Endocrinol. Metab. 2011, 15, S99–S106. [Google Scholar] [CrossRef]
- Tirosh, A.; Shimon, I. Complications of acromegaly: Thyroid and colon. Pituitary 2017, 20, 70–75. [Google Scholar] [CrossRef]
- Perticone, F.; Pigliaru, F.; Mariotti, S.; Deiana, L.; Furlani, L.; Mortini, P.; Losa, M. Is the incidence of differentiated thyroid cancer increased in patients with thyrotropin-secreting adenomas? Report of three cases from a large consecutive series. Thyroid 2015, 25, 417–424. [Google Scholar] [CrossRef]
- Tam, A.A.; Kaya, C.; Aydin, C.; Ersoy, R.; Cakir, B. Differentiated thyroid cancer in patients with prolactinoma. Turk. J. Med. Sci. 2016, 46, 1360–1365. [Google Scholar] [CrossRef]
- Moon, J.H.; Hyun, M.K.; Lee, J.Y.; Shim, J.I.; Kim, T.H.; Choi, H.S.; Ahn, H.Y.; Kim, K.W.; Park, D.J.; Park, Y.J.; et al. Prevalence of thyroid nodules and their associated clinical parameters: A large-scale, multicenter-based health checkup study. Korean J. Intern. Med. 2018, 33, 753–762. [Google Scholar] [CrossRef]
- Fernandez, A.; Karavitaki, N.; Wass, J.A. Prevalence of pituitary adenomas: A community-based, cross-sectional study in banbury (oxfordshire, uk). Clin. Endocrinol. 2010, 72, 377–382. [Google Scholar] [CrossRef]
- Park, H.H.; Kim, E.H.; Ku, C.R.; Lee, E.J.; Kim, S.H. Outcomes of aggressive surgical resection in growth hormone-secreting pituitary adenomas with cavernous sinus invasion. World Neurosurg. 2018, 117, e280–e289. [Google Scholar] [CrossRef]
- Kim, D.; Ku, C.R.; Park, S.H.; Moon, J.H.; Kim, E.H.; Kim, S.H.; Lee, E.J. Clinical parameters to distinguish silent corticotroph adenomas from other nonfunctioning pituitary adenomas. World Neurosurg. 2018, 115, e464–e471. [Google Scholar] [CrossRef]
- Benvenga, S.; Klose, M.; Vita, R.; Feldt-Rasmussen, U. Less known aspects of central hypothyroidism: Part 1—Acquired etiologies. J. Clin. Transl. Endocrinol. 2018, 14, 25–33. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Male | Female | p Value | |
|---|---|---|---|---|
| (n = 2202) | (n = 885) | (n = 1317) | ||
| Age (year) | 45.0 ± 13.5 | 47.4 ± 13.7 | 44.3 ± 13.2 | <0.001 |
| Type of pituitary tumor | ||||
| NFPA | 1167 (53.0) | 521 (58.9) | 646 (49.1) | <0.001 |
| GH | 488 (22.2) | 223 (25.2) | 265 (20.1) | 0.005 |
| PRL | 209 (9.5) | 19 (2.1) | 190 (14.4) | <0.001 |
| ACTH | 121 (5.5) | 22 (2.5) | 99 (7.5) | <0.001 |
| TSH | 28 (1.3) | 12 (1.4) | 16 (1.2) | 0.772 |
| RCC | 92 (4.2) | 37 (4.2) | 55 (4.2) | 0.996 |
| Craniopharyngioma | 51 (2.3) | 27 (3.1) | 24 (1.8) | 0.060 |
| aOthers | 46 (2.1) | 24 (2.7) | 22 (1.7) | 0.094 |
| Hyperthyroidism, n (%) | 44 (2.0) | 14 (1.6) | 30 (2.3) | 0.253 |
| Primary, n (%) | 14 (0.7) | 2 (0.2) | 12 (1.0) | 0.056 |
| Central, n (%) | 30 (1.4) | 12 (1.4) | 18 (1.4) | 0.904 |
| Hypothyroidism, n (%) | 218 (9.9) | 102 (11.5) | 116 (8.8) | 0.036 |
| Primary, n (%) | 53 (2.5) | 16 (1.8) | 37 (3.0) | 0.103 |
| Central, n (%) | 165 (7.8) | 86 (9.8) | 79 (6.3) | 0.003 |
| Post-thyroidectomy status, n (%) | 74 (3.4) | 11 (1.2) | 63 (4.8) | <0.001 |
| Cancer, n (%) | 59 (2.7) | 10 (1.1) | 49 (3.7) | <0.001 |
| Benign nodule, n (%) | 11 (0.5) | 0 (0.0) | 11 (0.8) | 0.004 |
| Unknown reason, n (%) | 4 (0.2) | 1 (0.1) | 3 (0.2) | >0.999 |
| Total | ~39 | 40~59 | 60~ | p for Trend | |
|---|---|---|---|---|---|
| (n = 2202) | (n = 802) | (n = 1058) | (n = 342) | ||
| Hyperthyroidism, n (%) | 44 (2.0) | 21 (2.6) | 22 (2.1) | 1 (0.3) | 0.017 |
| Primary, n (%) | 14 (0.6) | 6 (0.7) | 8 (0.8) | 0 | 0.231 |
| Central, n (%) | 30 (1.4) | 15 (1.9) | 14 (1.3) | 1 (0.3) | 0.039 |
| Hypothyroidism, n (%) | 218 (9.9) | 54 (6.7) | 114 (10.8) | 50 (14.5) | <0.001 |
| Primary, n (%) | 53 (2.4) | 12 (1.5) | 26 (2.5) | 15 (4.4) | 0.005 |
| Central, n (%) | 165 (7.5) | 42 (5.2) | 88 (8.3) | 35 (10.2) | 0.001 |
| Post-thyroidectomy status, n (%) | 74 (3.4) | 19 (2.4) | 42 (4.0) | 13 (3.8) | 0.108 |
| Cancer, n (%) | 59 (2.7) | 16 (2.0) | 32 (3.0) | 11 (3.2) | 0.165 |
| Benign nodule, n (%) | 11 (0.5) | 2 (0.2) | 8 (0.8) | 1 (0.3) | 0.573 |
| Unknown reason, n (%) | 4 (0.2) | 1 (0.1) | 2 (0.2) | 1 (0.3) | 0.547 |
| Total | NFPA | GH | PRL | ACTH | TSH | RCC | Craniopharyngioma | Others a | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|
| (n = 2202) | (n = 1167) | (n = 488) | (n = 209) | (n = 121) | (n = 28) | (n = 92) | (n = 51) | (n = 46) | ||
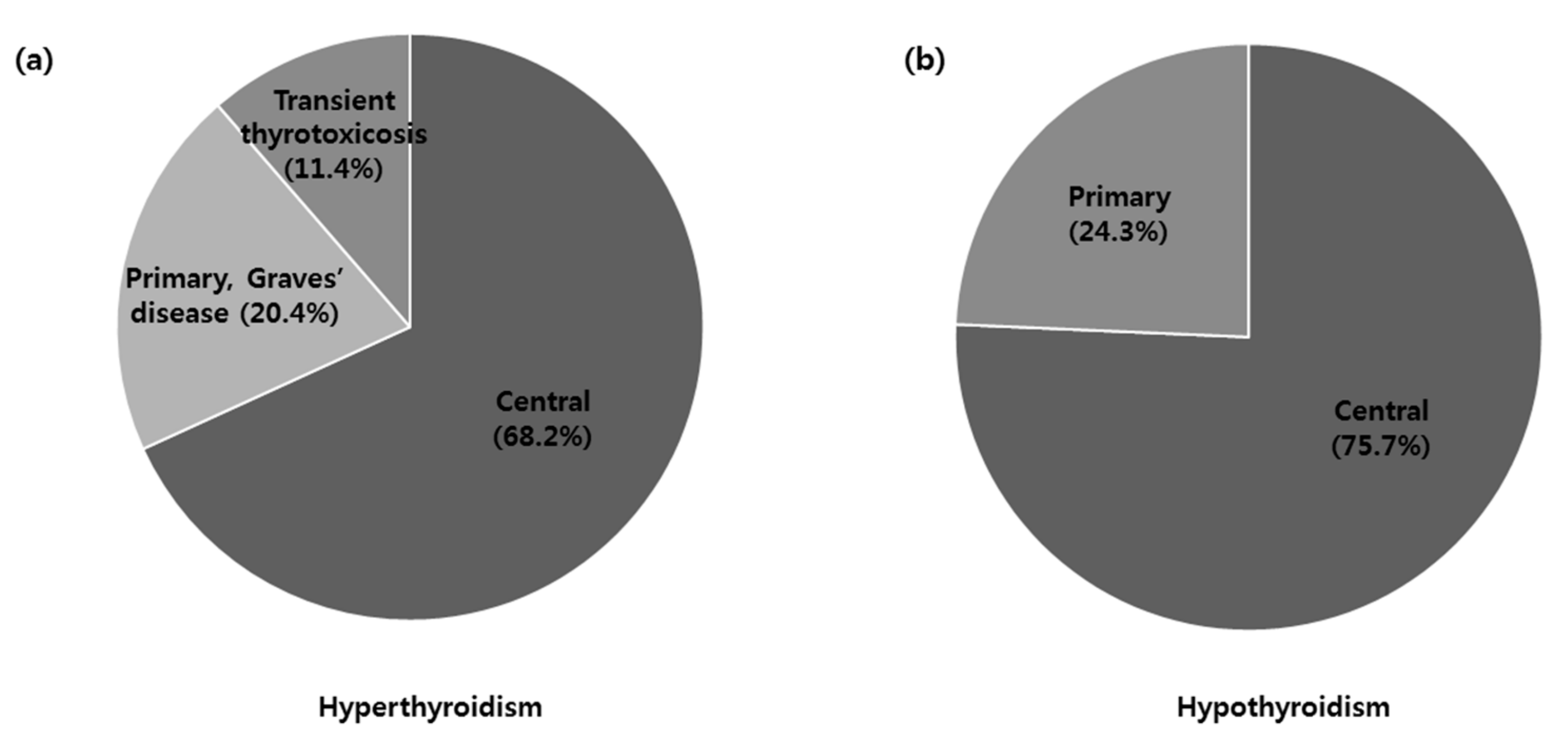
| Hyperthyroidism, n (%) | 44 (2.0) | 12 (1.0) | 5 (1.0) | 1 (0.5) | 0 | 26 (92.9) | 0 | 0 | 0 | <0.001 |
| Primary, n (%) | 14 (0.7) | 9 (0.8) | 5 (1.0) | 0 | 0 | 0 | 0 | 0 | 0 | 0.660 |
| Confirmed as Graves’ disease | 9 (0.4) | 8 (0.7) | 1 (0.2) | |||||||
| Confirmed as transient thyrotoxicosis | 5 (0.2) | 1 (0.1) | 4 (0.8) | |||||||
| Central, n (%) | 30 (1.4) | 3 (0.3) | 0 | 1 (0.5) | 0 | 26 (92.9) | 0 | 0 | 0 | <0.001 |
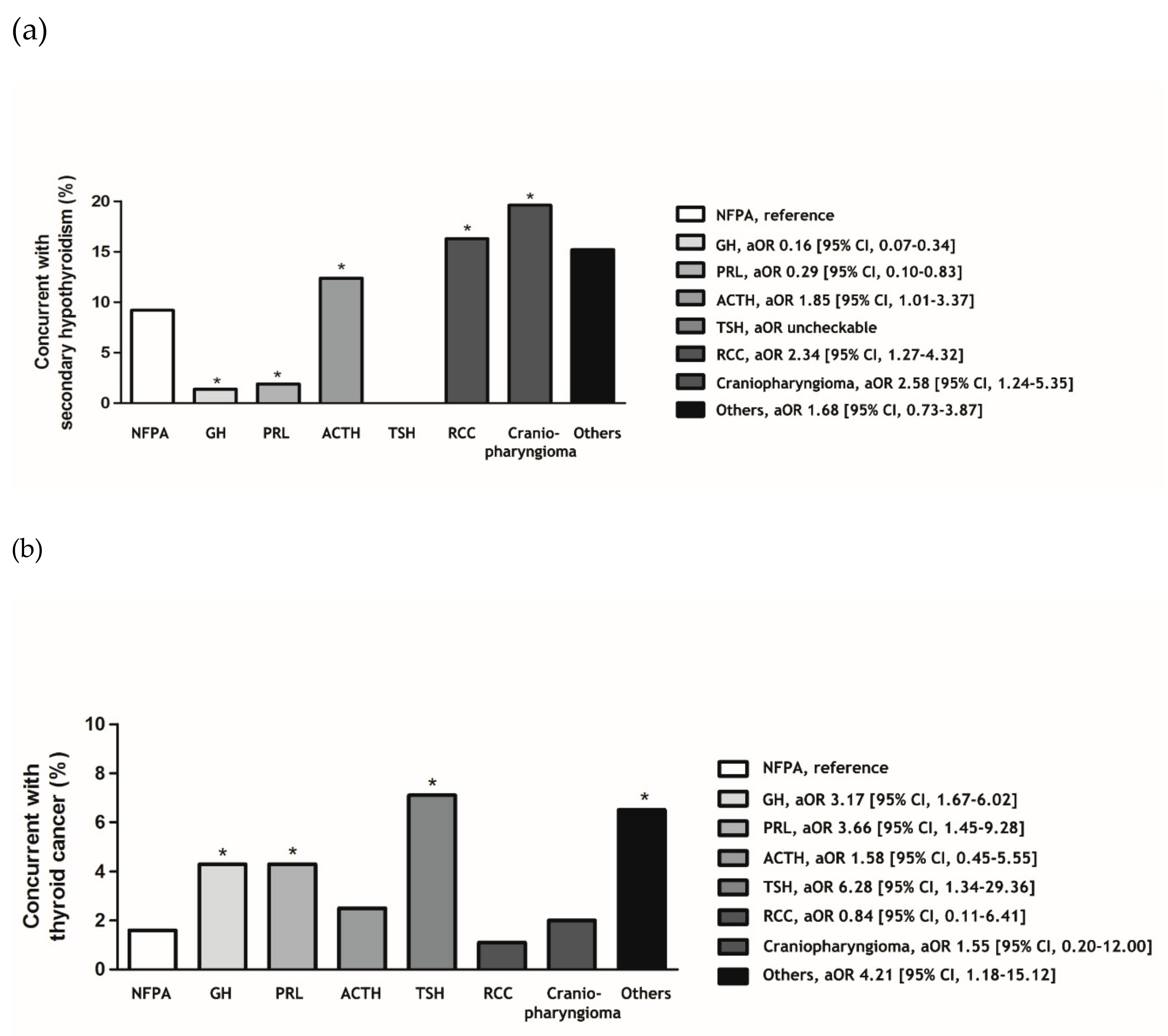
| Hypothyroidism, n (%) | 218 (9.9) | 147 (12.6) | 9 (1.8) | 7 (3.3) | 18 (14.9) | 0 | 16 (17.4) | 11 (21.6) | 10 (21.7) | <0.001 |
| Primary, n (%) | 53 (2.5) | 40 (3.4) | 2 (0.4) | 3 (1.4) | 3 (2.5) | 0 | 1 (1.1) | 1 (2.0) | 3 (6.5) | 0.008 |
| Central, n (%) | 165 (7.8) | 107 (9.2) | 7 (1.4) | 4 (1.9) | 15 (12.4) | 0 | 15 (16.3) | 10 (19.6) | 7 (15.2) | <0.001 |
| Post-thyroidectomy status, n (%) | 74 (3.4) | 26 (2.2) | 27 (5.5) | 10 (4.8) | 4 (3.3) | 2 (7.1) | 1 (1.1) | 1 (2.0) | 3 (6.5) | 0.014 |
| Cancer, n (%) | 59 (2.7) | 19 (1.6) | 21 (4.3) | 9 (4.3) | 3 (2.5) | 2 (7.1) | 1 (1.1) | 1 (2.0) | 3 (6.5) | 0.012 |
| Benign nodule, n (%) | 11 (0.5) | 5 (0.4) | 5 (1.0) | 0 | 1 (0.8) | 0 | 0 | 0 | 0 | 0.633 |
| Unknown reason, n (%) | 4 (0.2) | 2 (0.2) | 1 (0.2) | 1 (0.5) | 0 | 0 | 0 | 0 | 0 | 0.977 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.; Cho, Y.; Ku, C.R.; Jung, H.; Moon, J.H.; Kim, E.H.; Shin, D.Y.; Kim, S.H.; Lee, E.J. Prevalence of Thyroid Disease in Patients Surgically Treated for Pituitary Disease. J. Clin. Med. 2019, 8, 1142. https://doi.org/10.3390/jcm8081142
Kim D, Cho Y, Ku CR, Jung H, Moon JH, Kim EH, Shin DY, Kim SH, Lee EJ. Prevalence of Thyroid Disease in Patients Surgically Treated for Pituitary Disease. Journal of Clinical Medicine. 2019; 8(8):1142. https://doi.org/10.3390/jcm8081142
Chicago/Turabian StyleKim, Daham, Yongin Cho, Cheol Ryong Ku, Hyein Jung, Ju Hyung Moon, Eui Hyun Kim, Dong Yeob Shin, Sun Ho Kim, and Eun Jig Lee. 2019. "Prevalence of Thyroid Disease in Patients Surgically Treated for Pituitary Disease" Journal of Clinical Medicine 8, no. 8: 1142. https://doi.org/10.3390/jcm8081142