The Effect of Health-Related Behaviors on Disease Progression and Mortality in Early Stages of Chronic Kidney Disease: A Korean Nationwide Population-Based Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
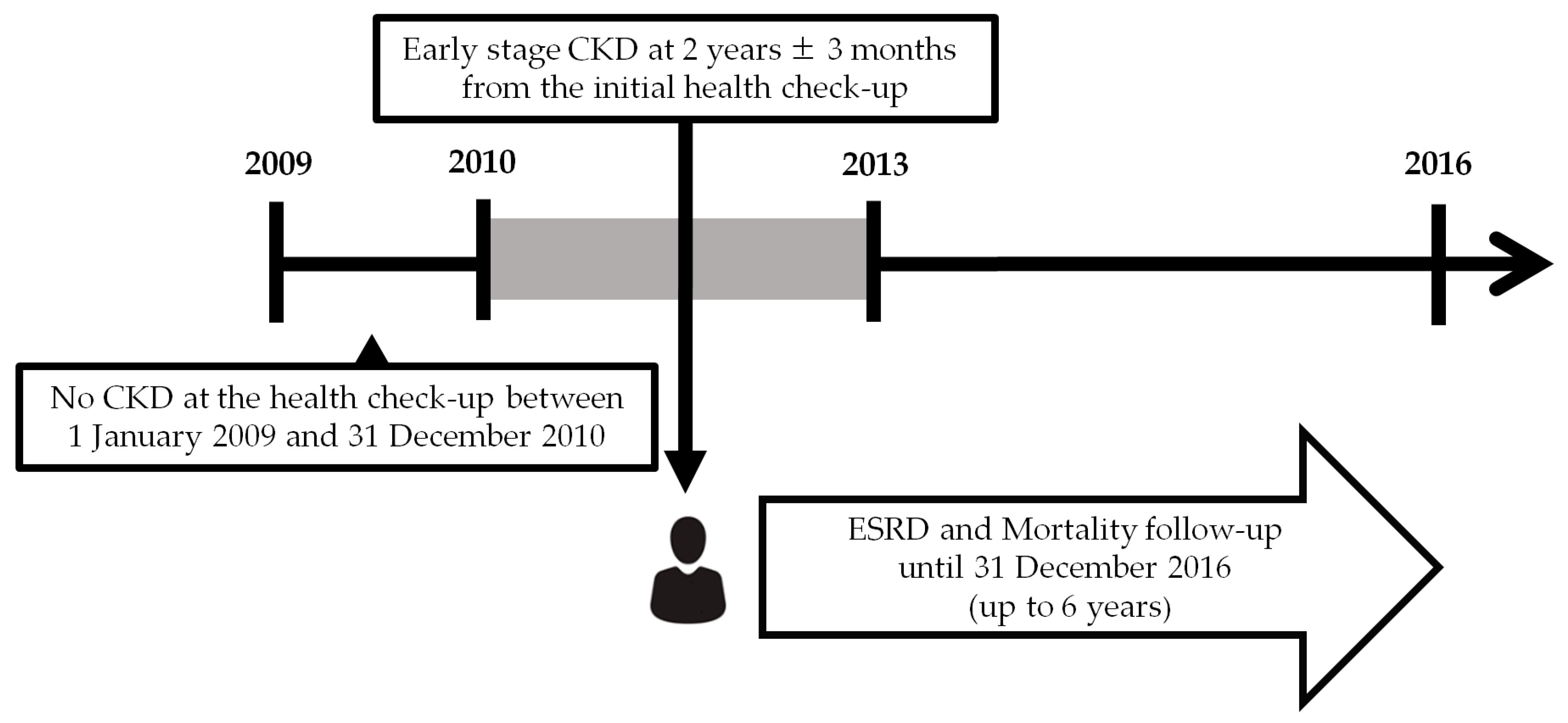
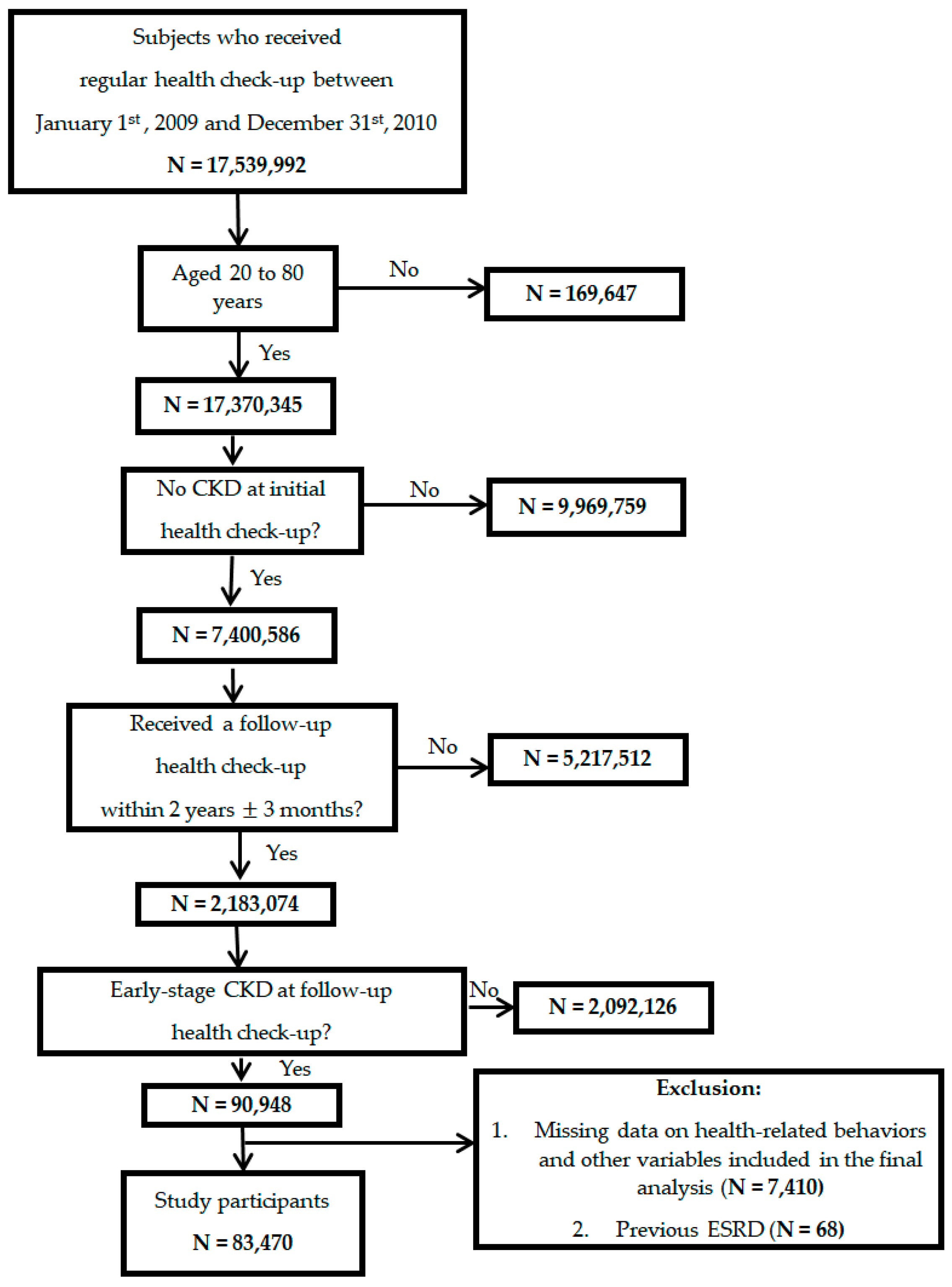
2.2. Study Cohort for Early Stages of CKD
2.3. Health-Related Behaviors
2.4. ESRD and Mortality
2.5. Covariate Data
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Health-Related Behaviors and Risk of ESRD and Death
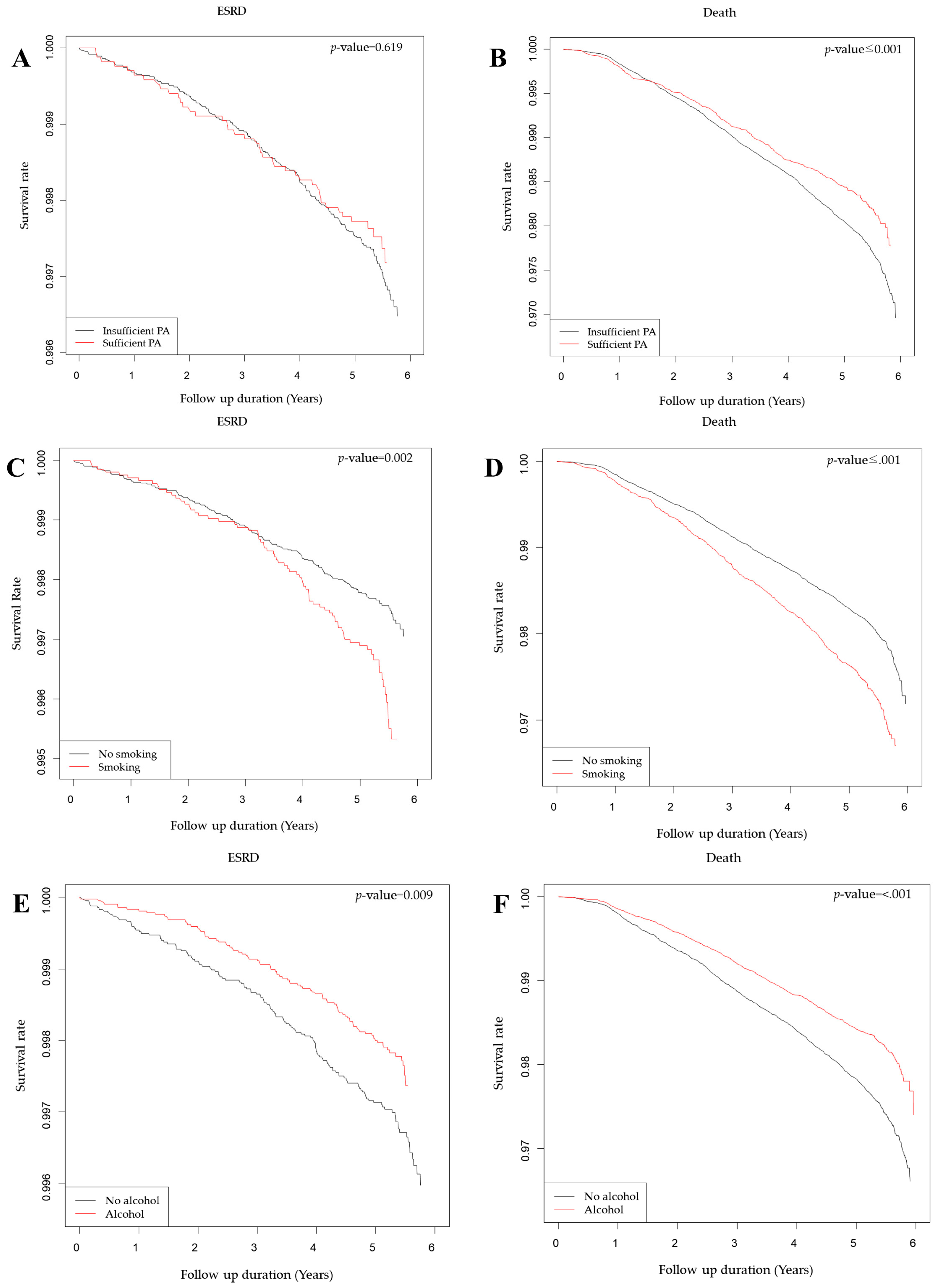
3.2.1. Physical Activity
3.2.2. Smoking
3.2.3. Alcohol Consumption
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; Callaghan, A.O.; Lasserson, D.S.; Hobbs, F.D.R. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.M.; Yang, C.W. Chronic kidney disease: Global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Nugent, R.A.; Fathima, S.F.; Feigl, A.B.; Chyung, D. The burden of chronic kidney disease on developing nations: A 21st century challenge in global health. Nephron Clin. Pract. 2011, 118, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Kanda, E.; Muneyuki, T.; Suwa, K.; Nakajima, K. Alcohol and exercise affect declining kidney function in healthy males regardless of obesity: A prospective cohort study. PLoS ONE 2015, 10, e0134937. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Thongprayoon, C.; Kittanamongkolchai, W.; Brabec, B.A.; O’corragain, O.A.; Edmonds, P.J.; Erickson, S.B. High alcohol consumption and the risk of renal damage: A systematic review and meta-analysis. QJM 2015, 108, 539–548. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Ma, Z.; Su, X.; Gao, Y.; Xia, J.; Wang, L.; Wang, Y.; Zhong, L. Cigarette smoking and chronic kidney disease in the general population: A systematic review and meta-analysis of prospective cohort studies. Nephrol. Dial. Transplant. 2017, 32, 475–487. [Google Scholar]
- Wakasugi, M.; Kazama, J.J.; Yamamoto, S.; Kawamura, K.; Narita, I. A combination of healthy lifestyle factors is associated with a decreased incidence of chronic kidney disease: A population-based cohort study. Hypertens. Res. 2013, 36, 328–333. [Google Scholar] [CrossRef]
- Willis, K.; Cheung, M.; Slifer, S. KDIGO 2012 Clinical Practice Guideline for Evaluation & Management of CKD. Kidney Int. Suppl. 2013, 3, 5–14. [Google Scholar]
- Izumi, A.; Kitamura, M.; Izawa, K.P. Effects of Exercise Training on Delaying Disease Progression in Patients with Chronic Kidney Disease: A Review of the Literature. Rev. Recent Clin. Trials 2016, 11, 333–341. [Google Scholar] [CrossRef]
- Shlipak, M.G.; Newman, A.; Peterson, D.; Siscovick, D.; Stehman-Breen, C.; Cushman, M.; Psaty, B.; Bleyer, A.; Fried, L.F.; Manolio, T.A. Cardiovascular Mortality Risk in Chronic Kidney Disease. JAMA 2005, 293, 1737–1745. [Google Scholar] [CrossRef] [Green Version]
- Barcellos, F.C.; Santos, I.S.; Umpierre, D.; Bohlke, M.; Hallal, P.C. Effects of exercise in the whole spectrum of chronic kidney disease: A systematic review. Clin. Kidney J. 2015, 8, 753–765. [Google Scholar] [CrossRef] [PubMed]
- Shankar, A.; Klein, R.; Klein, B.E.K. The association among smoking, heavy drinking, and chronic kidney disease. Am. J. Epidemiol. 2006, 164, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Ryoo, J.H.; Choi, J.M.; Oh, C.M.; Kim, M.G. The association between uric acid and chronic kidney disease in Korean men: A 4-year follow-up study. J. Korean Med. Sci. 2013, 28, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Song, S.O.; Jung, C.H.; Song, Y.D.; Park, C.Y.; Kwon, H.S.; Cha, B.S.; Park, J.Y.; Lee, K.U.; Ko, K.S.; Lee, B.W. Background and data configuration process of a nationwide population-based study using the Korean national health insurance system. Diabetes Metab. J. 2014, 38, 395–403. [Google Scholar] [CrossRef] [PubMed]
- International Physical Activity Questionnaire IPAQ Scoring Protocol. Available online: https://sites.google.com/site/theipaq/scoring-protocol (accessed on 13 February 2019).
- Cha, S.; Park, J.J.; Kim, S.; Ahn, H.Y.; Han, K.; Lee, Y.; Kim, W.S.; Paik, N.J. Need for Systematic Efforts to Modify Health-Related Behaviors After Acute Myocardial Infarction in Korea. Circ. J. 2018, 82, 2523–2529. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention Tobacco Glossary. Available online: https://www.cdc.gov/nchs/nhis/tobacco/tobacco_glossary.htm (accessed on 14 February 2019).
- Tolstrup, J.S.; Halkjær, J.; Heitmann, B.L.; Tjønneland, A.M.; Overvad, K.; Sørensen, T.I.; Grønbæk, M.N. Alcohol drinking frequency in relation to subsequent changes in waist circumference. Am. J. Clin. Nutr. 2008, 87, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Field, A.E.; Colditz, G.A.; Rimm, E.B. Alcohol intake and 8-year weight gain in women: A prospective study. Obes. Res. 2004, 12, 1386–1396. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders Duncan, L.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Robinson-Cohen, C.; Katz, R.; Mozaffarian, D.; Dalrymple, L.S.; de Boer, I.; Sarnak, M.; Shlipak, M.; Siscovick, D.; Kestenbaum, B. Physical Activity and Rapid Decline in Kidney Function. Arch. Intern. Med. 2010, 169, 2116–2123. [Google Scholar] [CrossRef]
- Altemtam, N.; Russell, J.; El Nahas, M. A study of the natural history of diabetic kidney disease (DKD). Nephrol. Dial. Transplant. 2012, 27, 1847–1854. [Google Scholar] [CrossRef]
- Stack, A.G.; Molony, D.A.; Rives, T.; Tyson, J.; Murthy, B.V.R. Association of physical activity with mortality in the US dialysis population. Am. J. Kidney Dis. 2005, 45, 690–701. [Google Scholar] [CrossRef] [PubMed]
- Wen, C.P.; Wai, J.P.M.; Tsai, M.K.; Yang, Y.C.; Cheng, T.Y.D.; Lee, M.C.; Chan, H.T.; Tsao, C.K.; Tsai, S.P.; Wu, X. Minimum amount of physical activity for reduced mortality and extended life expectancy: A prospective cohort study. Lancet 2011, 378, 1244–1253. [Google Scholar] [CrossRef]
- Beddhu, S.; Baird, B.C.; Zitterkoph, J.; Neilson, J.; Greene, T. Physical Activity and Mortality in Chronic Kidney Disease (NHANES III). Clin. J. Am. Soc. Nephrol. 2009, 4, 1901–1906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stump, C.S. Physical Activity in the Prevention of Chronic Kidney Disease. Cardiorenal Med. 2011, 1, 164–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenvinkel, P.; Carrero, J.J.; Von Walden, F.; Ikizler, T.A.; Nader, G.A. Muscle wasting in end-stage renal disease promulgates premature death: Established, emerging and potential novel treatment strategies. Nephrol. Dial. Transplant. 2016, 31, 1070–1077. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.H.; Mitch, W.E. Mechanisms of muscle wasting in chronic kidney disease. Nat. Rev. Nephrol. 2014, 10, 504. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Nakagawa, H.; Murakami, Y.; Kitamura, A.; Kiyama, M.; Sakata, K.; Tsuji, I.; Miura, K.; Ueshima, H.; Okamura, T. Smoking increases the risk of all-cause and cardiovascular mortality in patients with chronic kidney disease. Kidney Int. 2015, 88, 1144–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorriz, J.L.; Martinez-Castelao, A. Proteinuria: Detection and role in native renal disease progression. Transplant. Rev. 2012, 26, 3–13. [Google Scholar] [CrossRef]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef]
- Souza, V.A.; Oliveira, D.; Mansur, H.N.; Fernandes, N.M.; Bastos, M.G. Sarcopenia in Chronic Kidney Disease. J. Bras. Nefrol. 2015, 37, 98–105. [Google Scholar] [CrossRef]
- Waters, D.D. LDL-cholesterol lowering and renal outcomes. Curr. Opin. Pediatr. 2015, 26, 195–199. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| n | Total | Death | ESRD | ||||
|---|---|---|---|---|---|---|---|
| No | Yes | p Value | No | Yes | p Value | ||
| 83,470 | 81,664 | 1,806 | 83,237 | 233 | |||
| Age, years, mean ± SD | 48.43 ± 13.34 | 48.09 ± 13.16 | 64.05 ± 12.02 | <0.001 | 48.41 ± 13.33 | 57.24 ± 12.97 | <0.001 |
| Male, n, (%) | 45,108(54.04) | 43,835(53.68) | 1,273(70.49) | <0.001 | 44,935(53.98) | 173(74.25) | <0.001 |
| Urban residence, n, (%) | 37,732(45.2) | 37,064(45.39) | 668(36.99) | <0.001 | 37,652(45.23) | 80(34.33) | <0.001 |
| Low Income, n, (%) | 12,956(15.52) | 12,562(15.38) | 394(21.82) | <0.001 | 12,893(15.49) | 63(27.04) | <0.001 |
| Diabetes Mellitus, n, (%) | 13,047(15.63) | 12,383(15.16) | 664(36.77) | <0.001 | 12,931(15.54) | 116(49.79) | <0.001 |
| Hypertension, n, (%) | 27,346(32.76) | 26,275(32.17) | 1,071(59.3) | <0.001 | 27,188(32.66) | 158(67.81) | <0.001 |
| Dyslipidemia, n, (%) | 21,377(25.61) | 20,801(25.47) | 576(31.89) | <0.001 | 21,275(25.56) | 102(43.78) | <0.001 |
| History of CVD, n, (%) | 1,326(1.59) | 1,198(1.47) | 128(7.09) | <0.001 | 1,312(1.58) | 14(6.01) | <0.001 |
| CCI, n, (%) | <0.001 | <0.001 | |||||
| 0 | 42,039(50.36) | 41,654(51.01) | 385(21.32) | 41,994(50.45) | 45(19.31) | ||
| 1 | 20,782(24.9) | 20,452(25.04) | 330(18.27) | 20,751(24.93) | 31(13.3) | ||
| 2 or more | 20,649(24.74) | 19,558(23.95) | 1,091(60.41) | 20,492(24.62) | 157(67.38) | ||
| Sufficient physical activity, n, (%) | 16,854(20.19) | 16,550(20.27) | 304(16.83) | <0.001 | 16,810(20.2) | 44(18.88) | 0.619 |
| Smoking, n, (%) | <0.001 | <0.001 | |||||
| No | 49,476(59.27) | 48,590(59.5) | 886(49.06) | 49,367(59.31) | 109(46.78) | ||
| Ex | 13,451(16.11) | 13,086(16.02) | 365(20.21) | 13,405(16.1) | 46(19.74) | ||
| Current | 20,543(24.61) | 19,988(24.48) | 555(30.73) | 20,465(24.59) | 78(33.48) | ||
| Alcohol consumption, n, (%) | <0.001 | 0.007 | |||||
| No | 41,602(49.84) | 40,533(49.63) | 1,069(59.19) | 41,466(49.82) | 136(58.37) | ||
| Mild | 34,622(41.48) | 34,102(41.76) | 520(28.79) | 34,549(41.51) | 73(31.33) | ||
| Heavy | 7,246(8.68) | 7,029(8.61) | 217(12.02) | 7,222(8.68) | 24(10.3) | ||
| eGFR, ml/min/1.73 m2, n, (%) | <0.001 | <0.001 | |||||
| 30–59 | 16,365(19.61) | 15,760(19.3) | 605(33.5) | 16,269(19.55) | 96(41.2) | ||
| 60–89 | 25,042(30) | 24,508(30.01) | 534(29.57) | 24,963(29.99) | 79(33.91) | ||
| 90- | 42,063(50.39) | 41,396(50.69) | 667(36.93) | 42,005(50.46) | 58(24.89) | ||
| Urine Dipstick, n, (%) | <0.001 | <0.001 | |||||
| Negative | 15,344(18.38) | 14,820(18.15) | 524(29.01) | 15,284(18.36) | 60(25.75) | ||
| Trace | 39,384(47.18) | 38,822(47.54) | 562(31.12) | 39,341(47.26) | 43(18.45) | ||
| 1+ or more | 28,742(34.43) | 28,022(34.31) | 720(39.87) | 28,612(34.37) | 130(55.79) | ||
| Fasting Glucose, n, (%) | <0.001 | <0.001 | |||||
| <90 | 27,850(33.37) | 27,508(33.68) | 342(18.94) | 27,798(33.4) | 52(22.32) | ||
| 90–130 | 46,947(56.24) | 45,909(56.22) | 1,038(57.48) | 46,837(56.27) | 110(47.21) | ||
| >130 | 8,673(10.39) | 8,247(10.1) | 426(23.59) | 8,602(10.33) | 71(30.47) | ||
| LDL, mg/dL, n, (%) | <0.001 | 0.059 | |||||
| <70 | 7,924(9.49) | 7,596(9.3) | 328(18.16) | 7,894(9.48) | 30(12.88) | ||
| 70–100 | 22,478(26.93) | 21,992(26.93) | 486(26.91) | 22,407(26.92) | 71(30.47) | ||
| >100 | 53068(63.58) | 52076(63.77) | 992(54.93) | 52,936(63.6) | 132(56.65) | ||
| BMI, n, (%) | <0.001 | 0.631 | |||||
| <20 | 10,247(12.28) | 9,960(12.2) | 287(15.89) | 10,223(12.28) | 24(10.3) | ||
| 20–25 | 43,758(52.42) | 42,774(52.38) | 984(54.49) | 43,635(52.42) | 123(52.79) | ||
| >25 | 29,465(35.3) | 28,930(35.43) | 535(29.62) | 27,379(35.3) | 86(36.91) | ||
| BP > 130/80 mmHg, n, (%) | 44,645(53.49) | 43,452(53.21) | 1,193(66.06) | <0.001 | 44,481(53.44) | 164(70.39) | <0.001 |
| N | ESRD | Follow-up Duration (Person × Year) | Crude HR (95%CI) | Adjusted HR (95%CI) a | Death | Follow-up Duration (Person × Year) | Crude HR (95%CI) | Adjusted HR (95%CI) a | |
|---|---|---|---|---|---|---|---|---|---|
| Smoking | |||||||||
| Non, Ex | 62,927 | 155 | 336,424.23 | 1(ref.) | 1(ref.) | 1,251 | 336,675.06 | 1(ref.) | 1(ref.) |
| Current | 20,543 | 78 | 108,623.67 | 1.41 (1.04,1.90) | 1.44 (1.06,1.95) | 555 | 108,733.86 | 1.7 (1.52,1.90) | 1.61 (1.44,1.80) |
| p-value | 0.03 | 0.02 | <0.001 | <0.001 | |||||
| Alcohol | |||||||||
| Non | 41,602 | 136 | 222,490.34 | 1(ref.) | 1(ref.) | 1,069 | 222,719.88 | 1(ref.) | 1(ref.) |
| <30 g/day or >30 g/day | 41,868 | 97 | 222,557.55 | 0.60 (0.45,0.80) | 0.59 (0.44,0.79) | 737 | 222,689.04 | 0.87 (0.79,0.97) | 0.83 (0.74,0.93) |
| p-value | <0.001 | <0.001 | 0.01 | <0.001 | |||||
| Physical Activity | |||||||||
| Insufficient | 66,616 | 189 | 354,888.68 | 1(ref.) | 1(ref.) | 1,502 | 355,182.57 | 1(ref.) | 1(ref.) |
| Sufficient | 16,854 | 44 | 90,159.22 | 0.79 (0.57,1.1) | 0.84 (0.60,1.17) | 304 | 90,226.35 | 0.69 (0.61,0.78) | 0.73 (0.64,0.83) |
| p-value | 0.16 | 0.30 | <0.001 | <0.001 | |||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.; Kwon, S.; Moon, J.J.; Han, K.; Paik, N.-J.; Kim, W.-S. The Effect of Health-Related Behaviors on Disease Progression and Mortality in Early Stages of Chronic Kidney Disease: A Korean Nationwide Population-Based Study. J. Clin. Med. 2019, 8, 1100. https://doi.org/10.3390/jcm8081100
Lee Y, Kwon S, Moon JJ, Han K, Paik N-J, Kim W-S. The Effect of Health-Related Behaviors on Disease Progression and Mortality in Early Stages of Chronic Kidney Disease: A Korean Nationwide Population-Based Study. Journal of Clinical Medicine. 2019; 8(8):1100. https://doi.org/10.3390/jcm8081100
Chicago/Turabian StyleLee, Yookyung, SuYeon Kwon, Jong Joo Moon, Kyungdo Han, Nam-Jong Paik, and Won-Seok Kim. 2019. "The Effect of Health-Related Behaviors on Disease Progression and Mortality in Early Stages of Chronic Kidney Disease: A Korean Nationwide Population-Based Study" Journal of Clinical Medicine 8, no. 8: 1100. https://doi.org/10.3390/jcm8081100