Predictive Factors and Oncologic Outcome of Downgrade to Pathologic Gleason Score 6–7 after Radical Prostatectomy in Patients with Biopsy Gleason Score 8–10

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Follow-Up
2.3. Statistical Analysis
2.4. Ethics Approval and Informed Consent
3. Results
3.1. Patient and Disease Characteristics
3.2. Preoperative Factors Related to Pathologic Gleason Score (GS) Downgrade (pGS ≤ 7)
3.3. Supplementary Analysis of 3-2 (646 Cases)
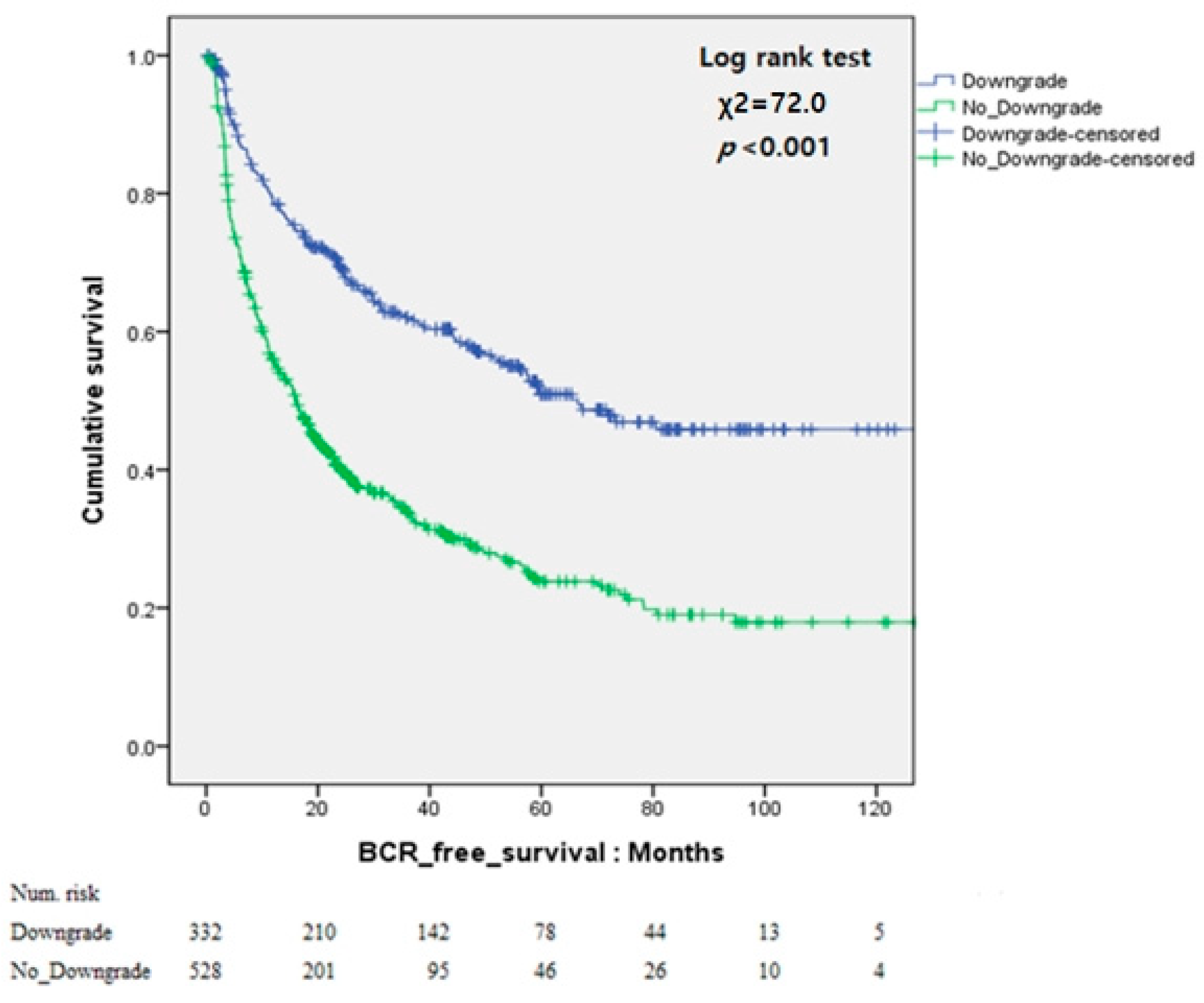
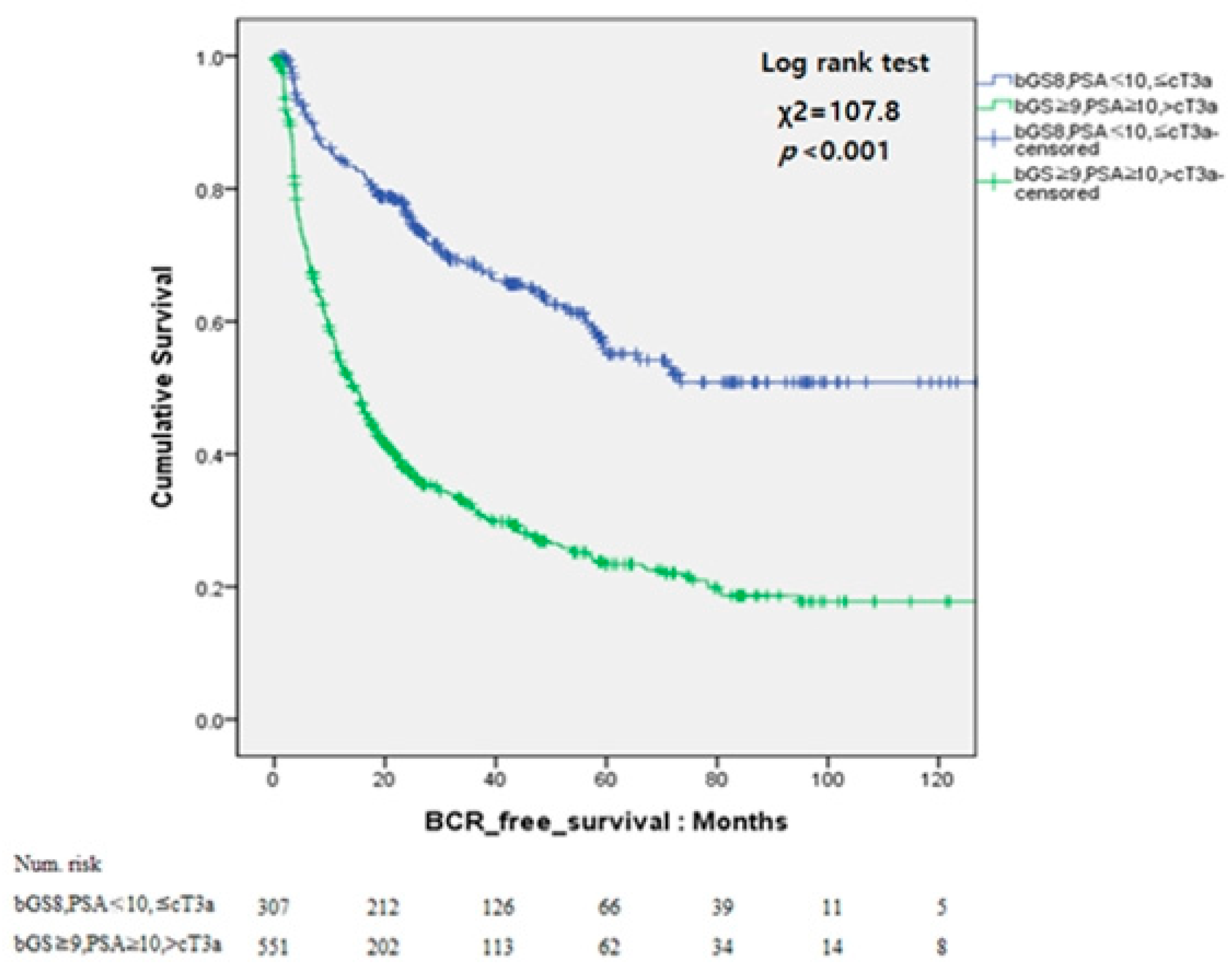
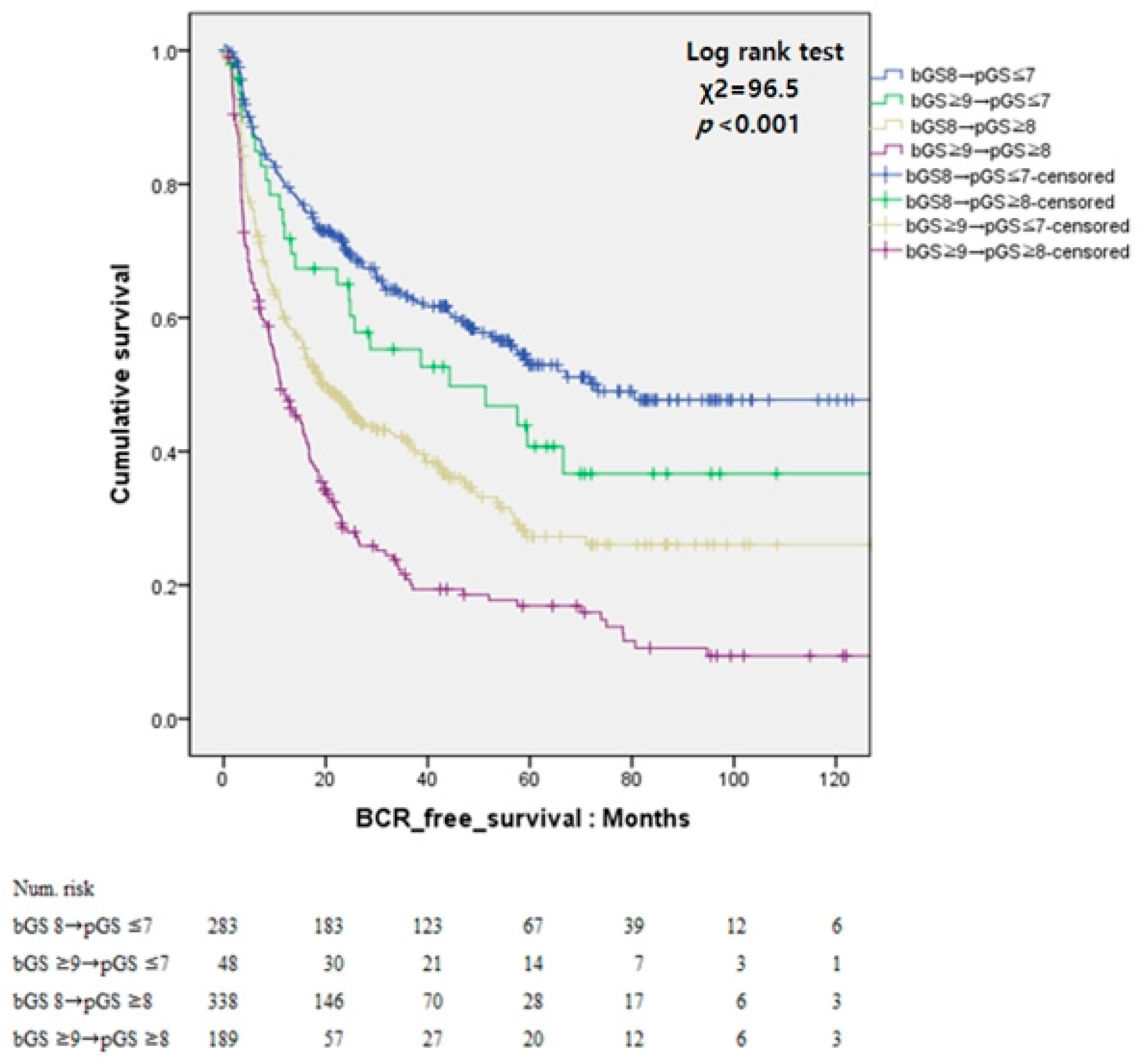
3.4. Oncologic Outcomes and Prognostic Factors
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Cooperberg, M.R.; Broering, J.M.; Kantoff, P.W.; Carroll, P.R. Contemporary trends in low risk prostate cancer: Risk assessment and treatment. J. Urol. 2007, 178, S14–S19. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Lubeck, D.P.; Meng, M.V.; Mehta, S.S.; Carroll, P.R. The changing face of low-risk prostate cancer: Trends in clinical presentation and primary management. J. Clin. Oncol. 2004, 22, 2141–2149. [Google Scholar] [CrossRef]
- Heidenreich, A.; Bastian, P.J.; Bellmunt, J.; Bolla, M.; Joniau, S.; van der Kwast, T.; Mason, M.; Matveev, V.; Wiegel, T.; Zattoni, F.; et al. EAU guidelines on prostate cancer. Part 1: Screening, diagnosis, and local treatment with curative intent—Update 2013. Eur. Urol. 2014, 65, 124–137. [Google Scholar] [CrossRef]
- Partin, A.W.; Kattan, M.W.; Subong, E.N.; Walsh, P.C.; Wojno, K.J.; Oesterling, J.E.; Scardino, P.T.; Pearson, J.D. Combination of prostate-specific antigen, clinical stage, and Gleason score to predict pathological stage of localized prostate cancer. A multi-institutional update. JAMA 1997, 277, 1445–1451. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.A.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998, 280, 969–974. [Google Scholar] [CrossRef]
- Gleason, D.F.; Mellinger, G.T. Prediction of prognosis for prostatic adenocarcinoma by combined histological grading and clinical staging. J. Urol. 1974, 111, 58–64. [Google Scholar] [CrossRef]
- Epstein, J.I.; Allsbrook, W.C., Jr.; Amin, M.B.; Egevad, L.L.; Committee, I.G. The 2005 international society of urological pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma. Am. J. Surg. Pathol. 2005, 29, 1228–1242. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A.; Grading, C. The 2014 international society of urological pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma: Definition of grading patterns and proposal for a new grading system. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Carroll, P.R.; Parsons, J.K.; Andriole, G.; Bahnson, R.R.; Castle, E.P.; Catalona, W.J.; Dahl, D.M.; Davis, J.W.; Epstein, J.I.; Etzioni, R.B.; et al. NCCN guidelines insights: Prostate cancer early detection, version 2.2016. J. Natl. Compr. Cancer Netw. 2016, 14, 509–519. [Google Scholar] [CrossRef]
- Muntener, M.; Epstein, J.I.; Hernandez, D.J.; Gonzalgo, M.L.; Mangold, L.; Humphreys, E.; Walsh, P.C.; Partin, A.W.; Nielsen, M.E. Prognostic significance of gleason score discrepancies between needle biopsy and radical prostatectomy. Eur. Urol. 2008, 53, 767–776. [Google Scholar] [CrossRef]
- Rajinikanth, A.; Manoharan, M.; Soloway, C.T.; Civantos, F.J.; Soloway, M.S. Trends in Gleason score: Concordance between biopsy and prostatectomy over 15 years. Urology 2008, 72, 177–182. [Google Scholar] [CrossRef]
- Djavan, B.; Kadesky, K.; Klopukh, B.; Marberger, M.; Roehrborn, C.G. Gleason scores from prostate biopsies obtained with 18-gauge biopsy needles poorly predict gleason scores of radical prostatectomy specimens. Eur. Urol. 1998, 33, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Donohue, J.F.; Bianco, F.J.; Kuroiwa, K.; Vickers, A.J.; Wheeler, T.M.; Scardino, P.T.; Reuter, V.A.; Eastham, J.A. Poorly differentiated prostate cancer treated with radical prostatectomy: Long-term outcome and incidence of pathological downgrading. J. Urol. 2006, 176, 991–995. [Google Scholar] [CrossRef]
- Gansler, T.; Fedewa, S.; Qi, R.; Lin, C.C.; Jemal, A.; Moul, J.W. Most gleason 8 biopsies are downgraded at prostatectomy—Does 4 + 4 = 7? J. Urol. 2018, 199, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Chung, D.Y.; Koh, D.H.; Goh, H.J.; Kim, M.S.; Lee, J.S.; Jang, W.S.; Choi, Y.D. Clinical significance and predictors of oncologic outcome after radical prostatectomy for invisible prostate cancer on multiparametric MRI. BMC Cancer 2018, 18, 1057. [Google Scholar] [CrossRef]
- Isbarn, H.; Ahyai, S.A.; Chun, F.K.; Budaus, L.; Schlomm, T.; Salomon, G.; Zacharias, M.; Erbersdobler, A.; Kollermann, J.; Sauter, G.; et al. Prevalence of a tertiary gleason grade and its impact on adverse histopathologic parameters in a contemporary radical prostatectomy series. Eur. Urol. 2009, 55, 394–401. [Google Scholar] [CrossRef]
- Cronin, A.M.; Godoy, G.; Vickers, A.J. Definition of biochemical recurrence after radical prostatectomy does not substantially impact prognostic factor estimates. J. Urol. 2010, 183, 984–989. [Google Scholar] [CrossRef]
- Billis, A.; Guimaraes, M.S.; Freitas, L.L.; Meirelles, L.; Magna, L.A.; Ferreira, U. The impact of the 2005 international society of urological pathology consensus conference on standard gleason grading of prostatic carcinoma in needle biopsies. J. Urol. 2008, 180, 548–552; discussion 552–553. [Google Scholar] [CrossRef]
- Tsivian, M.; Sun, L.; Mouraviev, V.; Madden, J.F.; Mayes, J.M.; Moul, J.W.; Polascik, T.J. Changes in gleason score grading and their effect in predicting outcome after radical prostatectomy. Urology 2009, 74, 1090–1093. [Google Scholar] [CrossRef] [PubMed]
- Uemura, H.; Hoshino, K.; Sasaki, T.; Miyoshi, Y.; Ishiguro, H.; Inayama, Y.; Kubota, Y. Usefulness of the 2005 international society of urologic pathology gleason grading system in prostate biopsy and radical prostatectomy specimens. BJU Int. 2009, 103, 1190–1194. [Google Scholar] [CrossRef] [PubMed]
- Ham, W.S.; Chalfin, H.J.; Feng, Z.; Trock, B.J.; Epstein, J.I.; Cheung, C.; Humphreys, E.; Partin, A.W.; Han, M. The impact of downgrading from biopsy gleason 7 to prostatectomy gleason 6 on biochemical recurrence and prostate cancer specific mortality. J. Urol. 2017, 197, 1060–1067. [Google Scholar] [CrossRef] [PubMed]
- Boesen, L.; Chabanova, E.; Logager, V.; Balslev, I.; Mikines, K.; Thomsen, H.S. Prostate cancer staging with extracapsular extension risk scoring using multiparametric MRI: A correlation with histopathology. Eur. Radiol. 2015, 25, 1776–1785. [Google Scholar] [CrossRef] [PubMed]
- Feng, T.S.; Sharif-Afshar, A.R.; Wu, J.; Li, Q.L.; Luthringer, D.; Saouaf, R.; Kim, H.L. Multiparametric mri improves accuracy of clinical nomograms for predicting extracapsular extension of prostate cancer. Urology 2015, 86, 332–337. [Google Scholar] [CrossRef]
- Barentsz, J.O.; Richenberg, J.; Clements, R.; Choyke, P.; Verma, S.; Villeirs, G.; Rouviere, O.; Logager, V.; Futterer, J.J. ESUR prostate MR guidelines 2012. Eur. Radiol. 2012, 22, 746–757. [Google Scholar] [CrossRef] [Green Version]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADs prostate imaging—Reporting and data system: 2015, version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef]
- Faiena, I.; Salmasi, A.; Mendhiratta, N.; Markovic, D.; Ahuja, P.; Hsu, W.; Elashoff, D.A.; Raman, S.S.; Reiter, R.E. PI-RADSV2 category on 3 tesla multiparametric prostate mri predicts oncologic outcomes in gleason 3+4 prostate cancer on biopsy. J. Urol. 2019, 201, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Krishna, S.; McInnes, M.; Lim, C.; Lim, R.; Hakim, S.W.; Flood, T.A.; Schieda, N. Comparison of prostate imaging reporting and data system versions 1 and 2 for the detection of peripheral zone Gleason score 3 + 4 = 7 cancers. AJR Am. J. Roentgenol. 2017, 209, W365–W373. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total | No_Downgrade | Downgrade | P value | |||
|---|---|---|---|---|---|---|---|
| N = 860 | N = 528 (61.4%) | N = 332 (38.6%) | |||||
| Median | IQR | Median | IQR | Median | IQR | ||
| Age, year | 67 | 62–71 | 67 | 62–71 | 66 | 62–70 | 0.578 |
| BMI, kg/m2 | 24.09 | 22.38–25.97 | 24.05 | 22.32–25.90 | 24.22 | 22.50–26.00 | 0.608 |
| PSA level, ng/mL | 10.59 | 6.58–19.39 | 12.03 | 7.09–22.72 | 8.60 | 5.99–14.74 | <0.001 |
| PSA group, ng/mL | N | % | N | % | N | % | <0.001 |
| <10 | 445 | 51.7 | 236 | 44.7 | 209 | 63.0 | |
| ≥10 | 415 | 48.3 | 292 | 55.3 | 123 | 37.0 | |
| PSA density, ng/mL2 | 0.33 | 0.20–0.62 | 0.38 | 0.22–0.75 | 0.28 | 0.18–0.50 | <0.001 |
| Prostate volume, mL | 32.0 | 26.0–40.5 | 32.6 | 26.0–40.9 | 31.1 | 25.8–40.0 | 0.367 |
| Clinical stage according to MRI | N | % | N | % | N | % | <0.001 |
| cT2 | 402 | 46.7 | 213 | 40.3 | 35 | 56.9 | |
| cT3a | 292 | 34.0 | 176 | 33.3 | 116 | 34.9 | |
| ≥cT3b | 166 | 19.3 | 139 | 26.3 | 27 | 8.1 | |
| Gleason score according to Biopsy | N | % | N | % | N | % | <0.001 |
| 8 | 623 | 72.4 | 339 | 64.2 | 284 | 85.5 | |
| ≥9 | 237 | 27.6 | 189 | 35.8 | 48 | 14.5 | |
| FU duration after RP, months | 51 | 26–78 | 44 | 25–71 | 59 | 32–83 | 0.317 |
| Pathologic Features after Radical Prostatectomy | |||||||
| Gleason Score according to Radical Prostatectomy | N | % | N | % | N | % | |
| 6 | 19 | 2.2 | - | 19 | 5.7 | ||
| 7 (3 + 4) | 130 | 15.1 | - | 130 | 39.2 | ||
| 7 (4 + 3) | 183 | 21.2 | - | 183 | 55.1 | ||
| 8 | 219 | 25.5 | 219 | 41.5 | - | ||
| ≥9 | 309 | 35.9 | 309 | 58.6 | - | ||
| Pathologic T Stage according to Radical Prostatectomy | N | % | N | % | N | % | <0.001 |
| T2 | 260 | 30.2 | 118 | 22.3 | 142 | 42.8 | |
| T3a | 348 | 40.5 | 208 | 39.4 | 140 | 42.2 | |
| ≥T3b | 252 | 29.3 | 202 | 38.3 | 50 | 15.1 | |
| ECE | 570 | 66.7 | 394 | 74.6 | 180 | 54.2 | <0.001 |
| SVI | 214 | 24.9 | 164 | 31.1 | 50 | 15.1 | <0.001 |
| PSM | 452 | 52.6 | 300 | 56.8 | 152 | 45.8 | 0.002 |
| LVI | 11 | 12.7 | 84 | 15.9 | 25 | 7.5 | <0.001 |
| PNI | 629 | 73.1 | 405 | 76.7 | 224 | 67.5 | 0.003 |
| HGPIN | 371 | 43.1 | 204 | 38.6 | 167 | 50.3 | 0.001 |
| BCR | 502 | 58.4 | 360 | 68.2 | 142 | 42.8 | <0.001 |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Age, year | 0.995 (0.975–1.015) | 0.592 | ||
| BMI, kg/m2 | 1.013 (0.964–1.064) | 0.607 | ||
| Prostate volume, mL | 0.996 (0.986–1.005) | 0.367 | ||
| PSA level, ng/mL | ||||
| <10 | 1 (Ref) | 1 (Ref) | ||
| ≥10 | 0.476 (0.359–0.630) | <0.001 | 0.606 (0.438–0.840) | 0.003 |
| PSA density | 0.679 (0.540–0.854) | 0.001 | 0.973 (0.799–1.185) | 0.783 |
| Gleason score | ||||
| 8 | 1 (Ref) | 1 (Ref) | ||
| ≥9 | 0.303 (0.213–0.432) | <0.001 | 0.342 (0.238–0.493) | <0.001 |
| Clinical stage according to MRI | ||||
| cT2 | 1 (Ref) | 1 (Ref) | ||
| cT3a | 0.743 (0.547–1.008) | 0.056 | 0.816 (0.592–1.123) | 0.211 |
| ≥cT3b | 0.219 (0.139–0.346) | <0.001 | 0.284 (0.176–0.458) | <0.001 |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age, year | 1.005 (0.992–1.018) | 0.469 | ||
| BMI, kg/m2 | 1.014 (0.982–1.046) | 0.399 | ||
| Prostate volume, ml | 1.003 (0.997–1.008) | 0.363 | ||
| PSA, ng/ml | 1.006 (1.005–1.008) | <0.001 | 1.005 (1.002–1.009) | 0.003 |
| <10 | 1 (Ref) | 1 (Ref) | ||
| ≥10 | 2.341 (1.956–2.803) | <0.001 | 1.539 (1.260–1.880) | <0.001 |
| PSA density, ng/mL2 | 1.186 (1.127–1.249) | <0.001 | 0.888 (0.780–1.011) | 0.073 |
| Biopsy Gleason score (bGS) | ||||
| 8 | 1 (Ref) | 1 (Ref) | ||
| ≥9 | 1.784 (1.485–2.143) | <0.001 | 1.233 (1.008–1.508) | 0.042 |
| Pathologic Gleason score (pGS) | ||||
| ≤7 (pGS_downgrade) | 1 (Ref) | 1 (Ref) | ||
| 8 | 1.735 (1.366–2.204) | <0.001 | 1.699 (1.328–2.175) | <0.001 |
| ≥9 | 2.810 (2.272–3.474) | <0.001 | 1.765 (1.396–2.231) | <0.001 |
| Pathologic T stage | ||||
| ≤T2 | 1 (Ref) | 1 (Ref) | ||
| ≥T3 | 5.044 (3.910–6.508) | <0.001 | 1.409 (0.788–2.520) | 0.247 |
| ECE | ||||
| No | 1 (Ref) | 1 (Ref) | ||
| Yes | 2.641 (2.122–3.286) | <0.001 | 1.016 (0.594–1.737) | 0.955 |
| SVI | ||||
| No | 1 (Ref) | 1 (Ref) | ||
| Yes | 3.139 (2.598–3.792) | <0.001 | 1.820 (1.473–2.249) | <0.001 |
| PSM | ||||
| No | 1 (Ref) | 1 (Ref) | ||
| Yes | 2.775 (2.298–3.351) | <0.001 | 1.819 (1.476–2.242) | <0.001 |
| LVI | ||||
| No | 1 (Ref) | 1 (Ref) | ||
| Yes | 2.069 (1.639–2.612) | <0.001 | 1.260 (0.987–1.608) | 0.063 |
| PNI | ||||
| No | 1 (Ref) | 1 (Ref) | ||
| Yes | 2.013 (1.612–2.512) | <0.001 | 1.244 (0.979–1.580) | 0.074 |
| HGPIN | ||||
| No | 1 (Ref) | |||
| Yes | 0.870 (0.728–1.040) | 0.126 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, D.Y.; Lee, J.S.; Goh, H.J.; Koh, D.H.; Kim, M.S.; Jang, W.S.; Choi, Y.D. Predictive Factors and Oncologic Outcome of Downgrade to Pathologic Gleason Score 6–7 after Radical Prostatectomy in Patients with Biopsy Gleason Score 8–10. J. Clin. Med. 2019, 8, 438. https://doi.org/10.3390/jcm8040438
Chung DY, Lee JS, Goh HJ, Koh DH, Kim MS, Jang WS, Choi YD. Predictive Factors and Oncologic Outcome of Downgrade to Pathologic Gleason Score 6–7 after Radical Prostatectomy in Patients with Biopsy Gleason Score 8–10. Journal of Clinical Medicine. 2019; 8(4):438. https://doi.org/10.3390/jcm8040438
Chicago/Turabian StyleChung, Doo Yong, Jong Soo Lee, Hyeok Jun Goh, Dong Hoon Koh, Min Seok Kim, Won Sik Jang, and Young Deuk Choi. 2019. "Predictive Factors and Oncologic Outcome of Downgrade to Pathologic Gleason Score 6–7 after Radical Prostatectomy in Patients with Biopsy Gleason Score 8–10" Journal of Clinical Medicine 8, no. 4: 438. https://doi.org/10.3390/jcm8040438