Thoracic Paravertebral Block with Adjuvant Dexmedetomidine in Video-Assisted Thoracoscopic Surgery: A Randomized, Double-Blind Study

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Thoracic Paravertebral Block
2.2. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Grogan, E.L.; Jones, D.R. VATS lobectomy is better than open thoracotomy: What is the evidence for short-term outcomes? Thorac. Surg. Clin. 2008, 18, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Hill, S.E.; Keller, R.A.; Stafford-Smith, M.; Grichnik, K.; White, W.D.; D’Amico, T.A.; Newman, M.F. Efficacy of single-dose, multilevel paravertebral nerve blockade for analgesia after thoracoscopic procedures. Anesthesiology 2006, 104, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Kotemane, N.C.; Gopinath, N.; Vaja, R. Analgesic techniques following thoracic surgery: A survey of United Kingdom practice. Eur. J. Anaesthesiol. 2010, 27, 897–899. [Google Scholar] [CrossRef] [PubMed]
- Kaya, F.N.; Turker, G.; Mogol, E.B.; Bayraktar, S. Thoracic paravertebral block for video-assisted thoracoscopic surgery: Single injection versus multiple injections. J. Cardiothorac. Vasc. Anesth. 2012, 26, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Kaya, F.N.; Turker, G.; Basagan-Mogol, E.; Goren, S.; Bayram, S.; Gebitekin, C. Preoperative multiple-injection thoracic paravertebral blocks reduce postoperative pain and analgesic requirements after video-assisted thoracic surgery. J. Cardiothorac. Vasc. Anesth. 2006, 20, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Thavaneswaran, P.; Rudkin, G.E.; Cooter, R.D.; Moyes, D.G.; Perera, C.L.; Maddern, G.J. Brief reports: Paravertebral block for anesthesia: A systematic review. Anesth. Analg. 2010, 110, 1740–1744. [Google Scholar] [CrossRef] [PubMed]
- Pintaric, T.S.; Potocnik, I.; Hadzic, A.; Stupnik, T.; Pintaric, M.; Novak Jankovic, V. Comparison of continuous thoracic epidural with paravertebral block on perioperative analgesia and hemodynamic stability in patients having open lung surgery. Reg. Anesth. Pain Med. 2011, 36, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Baidya, D.K.; Khanna, P.; Maitra, S. Analgesic efficacy and safety of thoracic paravertebral and epidural analgesia for thoracic surgery: A systematic review and meta-analysis. Interact. Cardiovasc. Thorac. Surg. 2014, 18, 626–635. [Google Scholar] [CrossRef] [PubMed]
- SC, O.R.; Donnell, B.O.; Cuffe, T.; Harmon, D.C.; Fraher, J.P.; Shorten, G. Thoracic paravertebral block using real-time ultrasound guidance. Anesth. Analg. 2010, 110, 248–251. [Google Scholar] [CrossRef]
- Williams, B.A.; Bottegal, M.T.; Kentor, M.L.; Irrgang, J.J.; Williams, J.P. Rebound pain scores as a function of femoral nerve block duration after anterior cruciate ligament reconstruction: Retrospective analysis of a prospective, randomized clinical trial. Reg. Anesth. Pain Med. 2007, 32, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Gerlach, A.T.; Dasta, J.F. Dexmedetomidine: An updated review. Ann. Pharmacother. 2007, 41, 245–252. [Google Scholar] [CrossRef]
- Abdallah, F.W.; Brull, R. Facilitatory effects of perineural dexmedetomidine on neuraxial and peripheral nerve block: A systematic review and meta-analysis. Br. J. Anaesth. 2013, 110, 915–925. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, F.W.; Dwyer, T.; Chan, V.W.; Niazi, A.U.; Ogilvie-Harris, D.J.; Oldfield, S.; Patel, R.; Oh, J.; Brull, R. IV and Perineural Dexmedetomidine Similarly Prolong the Duration of Analgesia after Interscalene Brachial Plexus Block: A Randomized, Three-arm, Triple-masked, Placebo-controlled Trial. Anesthesiology 2016, 124, 683–695. [Google Scholar] [CrossRef]
- Bae, H.B. Dexmedetomidine: An attractive adjunct to anesthesia. Korean J. Anesthesiol. 2017, 70, 375–376. [Google Scholar] [CrossRef]
- Vogt, A.; Stieger, D.S.; Theurillat, C.; Curatolo, M. Single-injection thoracic paravertebral block for postoperative pain treatment after thoracoscopic surgery. Br. J. Anaesth. 2005, 95, 816–821. [Google Scholar] [CrossRef]
- Xu, J.; Yang, X.; Hu, X.; Chen, X.; Zhang, J.; Wang, Y. Multilevel Thoracic Paravertebral Block Using Ropivacaine with/without Dexmedetomidine in Video-Assisted Thoracoscopic Surgery. J. Cardiothorac. Vasc. Anesth. 2018, 32, 318–324. [Google Scholar] [CrossRef]
- Shibata, Y.; Nishiwaki, K. Ultrasound-guided intercostal approach to thoracic paravertebral block. Anesth. Analg. 2009, 109, 996–997. [Google Scholar] [CrossRef]
- Mohamed, S.A.; Fares, K.M.; Mohamed, A.A.; Alieldin, N.H. Dexmedetomidine as an adjunctive analgesic with bupivacaine in paravertebral analgesia for breast cancer surgery. Pain Physician 2014, 17, E589–E598. [Google Scholar]
- Guo, T.Z.; Jiang, J.Y.; Buttermann, A.E.; Maze, M. Dexmedetomidine injection into the locus ceruleus produces antinociception. Anesthesiology 1996, 84, 873–881. [Google Scholar] [CrossRef]
- Fritsch, G.; Danninger, T.; Allerberger, K.; Tsodikov, A.; Felder, T.K.; Kapeller, M.; Gerner, P.; Brummett, C.M. Dexmedetomidine added to ropivacaine extends the duration of interscalene brachial plexus blocks for elective shoulder surgery when compared with ropivacaine alone: A single-center, prospective, triple-blind, randomized controlled trial. Reg. Anesth. Pain Med. 2014, 39, 37–47. [Google Scholar] [CrossRef]
- Andersen, J.H.; Grevstad, U.; Siegel, H.; Dahl, J.B.; Mathiesen, O.; Jaeger, P. Does Dexmedetomidine Have a Perineural Mechanism of Action When Used as an Adjuvant to Ropivacaine?: A Paired, Blinded, Randomized Trial in Healthy Volunteers. Anesthesiology 2017, 126, 66–73. [Google Scholar] [CrossRef]
- Marhofer, D.; Kettner, S.C.; Marhofer, P.; Pils, S.; Weber, M.; Zeitlinger, M. Dexmedetomidine as an adjuvant to ropivacaine prolongs peripheral nerve block: A volunteer study. Br. J. Anaesth. 2013, 110, 438–442. [Google Scholar] [CrossRef]
- Woodworth, G.E.; Ivie, R.M.J.; Nelson, S.M.; Walker, C.M.; Maniker, R.B. Perioperative Breast Analgesia: A Qualitative Review of Anatomy and Regional Techniques. Reg. Anesth. Pain Med. 2017, 42, 609–631. [Google Scholar] [CrossRef]
- Shimizu, H.; Kamiya, Y.; Nishimaki, H.; Denda, S.; Baba, H. Thoracic paravertebral block reduced the incidence of chronic postoperative pain for more than 1 year after breast cancer surgery. JA Clin. Rep. 2015, 1, 19. [Google Scholar] [CrossRef]
- Boughey, J.C.; Goravanchi, F.; Parris, R.N.; Kee, S.S.; Kowalski, A.M.; Frenzel, J.C.; Bedrosian, I.; Meric-Bernstam, F.; Hunt, K.K.; Ames, F.C.; et al. Prospective randomized trial of paravertebral block for patients undergoing breast cancer surgery. Am. J. Surg. 2009, 198, 720–725. [Google Scholar] [CrossRef] [Green Version]
- Mohta, M.; Kalra, B.; Sethi, A.K.; Kaur, N. Efficacy of dexmedetomidine as an adjuvant in paravertebral block in breast cancer surgery. J. Anesth. 2016, 30, 252–260. [Google Scholar] [CrossRef]
- Daly, D.J.; Myles, P.S. Update on the role of paravertebral blocks for thoracic surgery: Are they worth it? Curr. Opin. Anaesthesiol. 2009, 22, 38–43. [Google Scholar] [CrossRef]
- Kang, R.; Jeong, J.S.; Yoo, J.C.; Lee, J.H.; Choi, S.J.; Gwak, M.S.; Hahm, T.S.; Huh, J.; Ko, J.S. Effective Dose of Intravenous Dexmedetomidine to Prolong the Analgesic Duration of Interscalene Brachial Plexus Block: A Single-Center, Prospective, Double-Blind, Randomized Controlled Trial. Reg. Anesth. Pain Med. 2018. [Google Scholar] [CrossRef]
- Naja, Z.M.; El-Rajab, M.; Al-Tannir, M.A.; Ziade, F.M.; Tayara, K.; Younes, F.; Lonnqvist, P.A. Thoracic paravertebral block: Influence of the number of injections. Reg. Anesth. Pain Med. 2006, 31, 196–201. [Google Scholar] [CrossRef]
- Hurley, R.W.; Adams, M.C. Sex, gender, and pain: An overview of a complex field. Anesth. Analg. 2008, 107, 309–317. [Google Scholar] [CrossRef]
- Bartley, E.J.; Fillingim, R.B. Sex differences in pain: A brief review of clinical and experimental findings. Br. J. Anaesth. 2013, 111, 52–58. [Google Scholar] [CrossRef]
- Bobbio, A.; Dechartres, A.; Bouam, S.; Damotte, D.; Rabbat, A.; Regnard, J.F.; Roche, N.; Alifano, M. Epidemiology of spontaneous pneumothorax: Gender-related differences. Thorax 2015, 70, 653–658. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dexmedetomidine Group (n = 33) | Control Group (n = 33) | |
|---|---|---|
| Age (year) | 19.0 (17.0–22.0) | 19.0 (18.0–22.0) |
| Height (cm) | 173.3 (169.5–178.2) | 173.1 (166.6–178.2) |
| Weight (kg) | 58.2 ± 8.0 | 57.8 ± 8.1 |
| BMI (kg/m2) | 19.2 ± 2.2 | 19.3 ± 2.4 |
| Port number | ||
| 1 | 21 (63.6) | 13 (39.4) |
| 2 | 2 (6.1) | 4 (12.1) |
| 3 | 10 (30.3) | 16 (48.5) |
| Previous VATS history | 7 (21.2) | 11 (33.3) |
| Pleural adhesion | 3 (9.1) | 9 (27.3) |
| Dexmedetomidine Group (n = 33) | Control Group (n = 33) | p | |
|---|---|---|---|
| Extubation time (min) | 11.0 (9.0–13.0) | 10.0 (8.0–12.0) | 0.071 |
| PACU stay time (min) | 44.0 (39.0–53.0) | 42.0 (38.0–49.0) | 0.517 |
| Analgesic request in PACU | 4 (12.1%) | 14 (42.4%) | 0.013 |
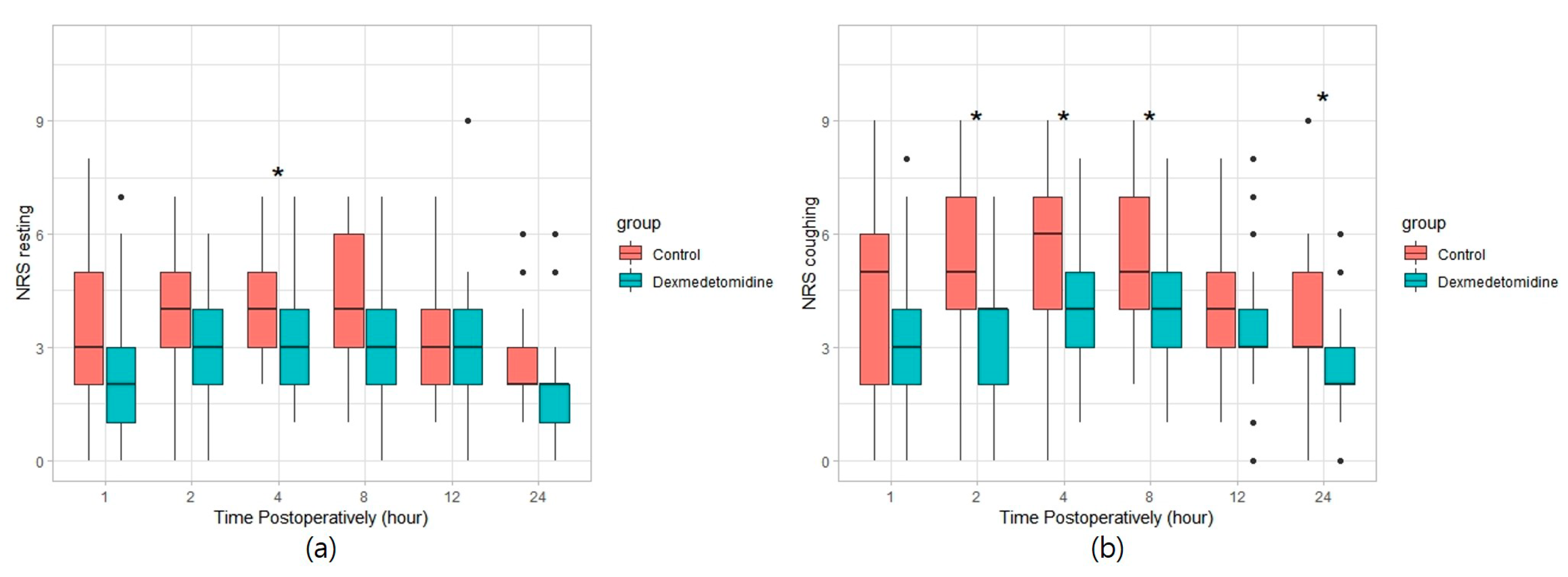
| Maximum NRS pain score | |||
| Resting | 4.0 (3.0–5.0) | 5.0 (4.0–6.0) | 0.032 |
| Coughing | 5.0 (4.0–6.0) | 7.0 (5.0–7.0) | 0.003 |
| Rescue analgesic (ketorolac) | 8 (24.2%) | 7 (21.2%) | 1.000 |
| Rescue analgesic (pethidine) | 1 (3.0%) | 3 (9.1%) | 0.606 |
| Discharge day after operation | 3.0 (3.0–5.0) | 3.0 (3.0–5.0) | 0.455 |
| Nausea | 4 (12.1%) | 3 (9.1%) | 1.000 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, B.; Lim, C.; Kang, H.; Eom, H.; Kim, Y.; Cho, H.J.; Han, W.; Lee, S.; Chung, W.; Kim, Y.-H. Thoracic Paravertebral Block with Adjuvant Dexmedetomidine in Video-Assisted Thoracoscopic Surgery: A Randomized, Double-Blind Study. J. Clin. Med. 2019, 8, 352. https://doi.org/10.3390/jcm8030352
Hong B, Lim C, Kang H, Eom H, Kim Y, Cho HJ, Han W, Lee S, Chung W, Kim Y-H. Thoracic Paravertebral Block with Adjuvant Dexmedetomidine in Video-Assisted Thoracoscopic Surgery: A Randomized, Double-Blind Study. Journal of Clinical Medicine. 2019; 8(3):352. https://doi.org/10.3390/jcm8030352
Chicago/Turabian StyleHong, Boohwi, ChaeSeong Lim, Hyemin Kang, Hongsik Eom, Yeojung Kim, Hyun Jin Cho, Woosik Han, Sunyeul Lee, Woosuk Chung, and Yoon-Hee Kim. 2019. "Thoracic Paravertebral Block with Adjuvant Dexmedetomidine in Video-Assisted Thoracoscopic Surgery: A Randomized, Double-Blind Study" Journal of Clinical Medicine 8, no. 3: 352. https://doi.org/10.3390/jcm8030352