VDR rs2228570 Polymorphism Is Related to Non-Progression to AIDS in Antiretroviral Therapy Naïve HIV-Infected Patients


 , , , and
, , , and
Abstract
:1. Introduction
Objective
2. Patients and Methods
2.1. Patients
2.2. DNA Genotyping
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
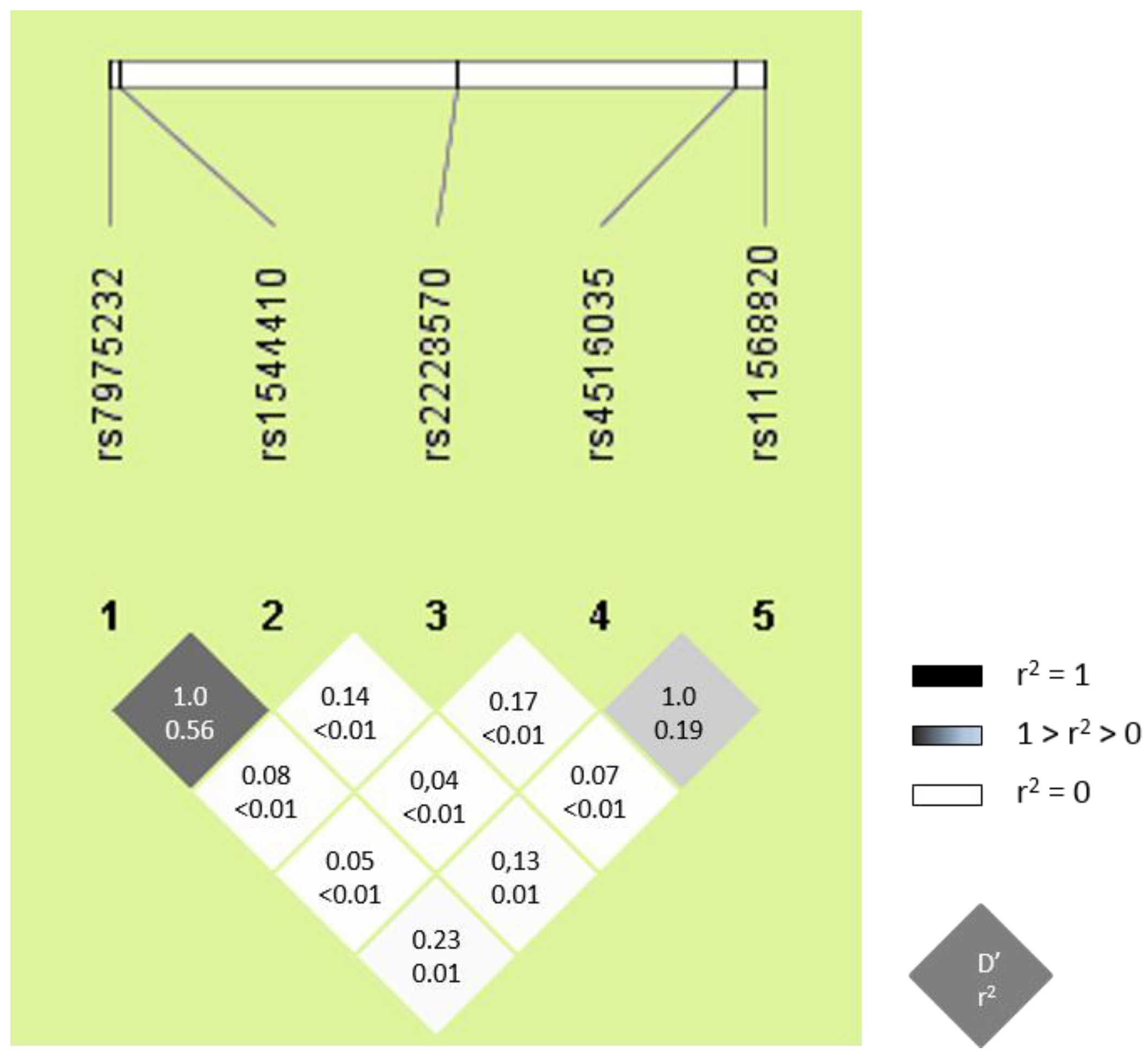
3.2. Characteristics of VDR SNPs
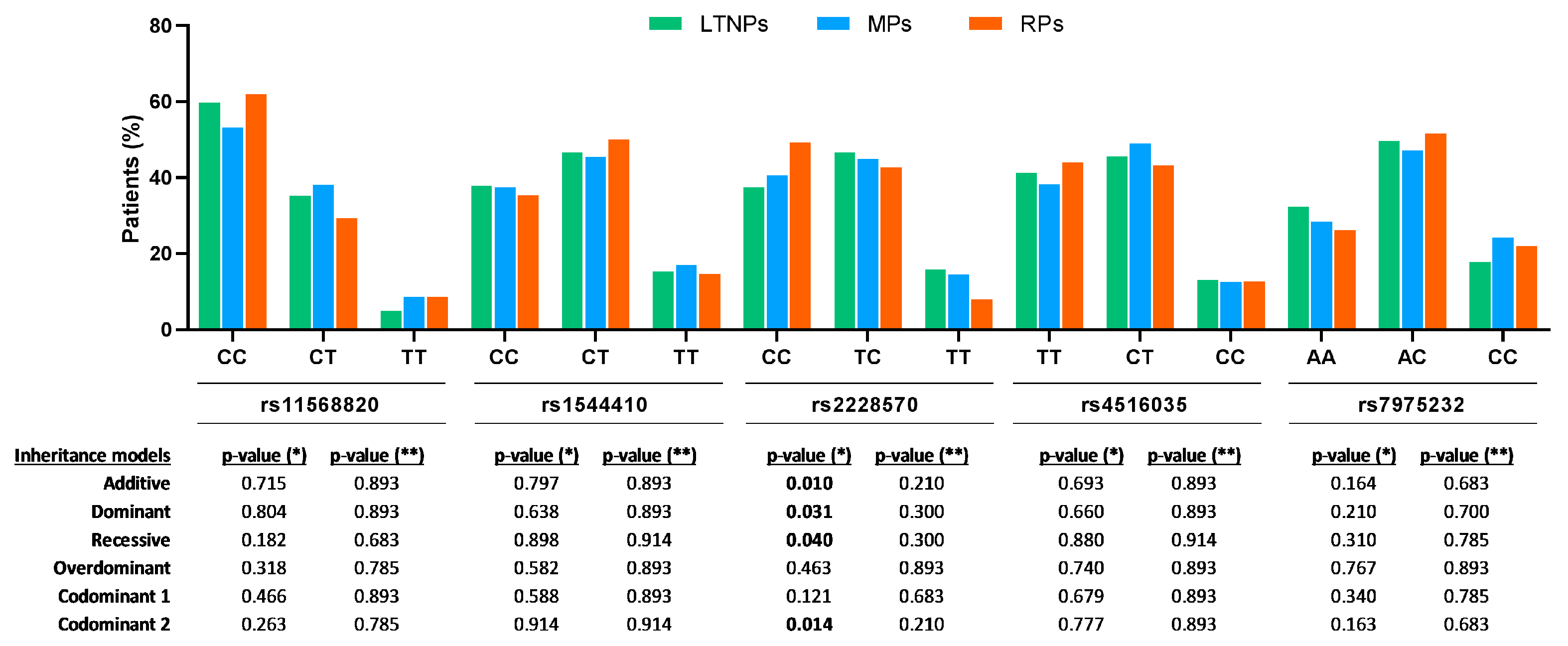
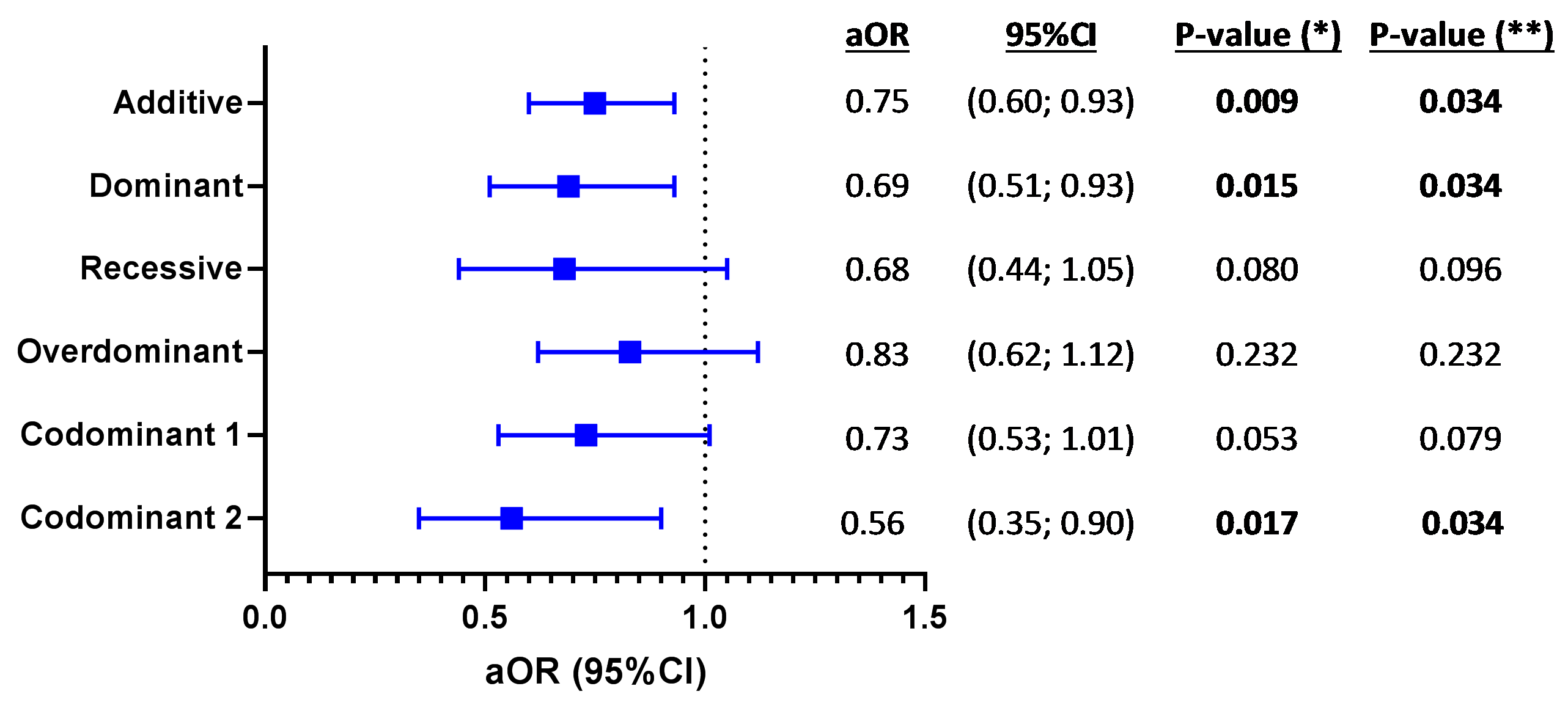
3.3. VDR SNPs and AIDS Progression
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B
- Centro Sanitario Sandoval—Madrid
- Hospital 12 de Octubre—Madrid
- Hospital Arnau de Vilanova—Lleida
- Hospital Asturias
- Hospital Bellvitge—Barcelona
- Hospital Castellón
- Hospital Clínic—Barcelona
- Hospital Donostia—San Sebastián
- Hospital Elche—Alicante
- Hospital Germans Trias i Pujol—Badalona
- Hospital Gregorio Marañón—Madrid
- Hospital Joan XXIII—Tarragona
- Hospital La Fe—Valencia
- Hospital La Paz/Carlos III—Madrid
- Hospital La Princesa—Madrid
- Hospital Navarra—Pamplona
- Hospital Parc Taulí- Sabadell
- Hospital Ramón y Cajal—Madrid
- Hospital San Cecilio—Granada
- Hospital San Pedro—Logroño
- Hospital Son Dureta—Mallorca
- Hospital Virgen del Rocío—Sevilla
References
- Munoz, A.; Sabin, C.A.; Phillips, A.N. The incubation period of AIDS. AIDS 1997, 11, S69–S76. [Google Scholar] [PubMed]
- Pantaleo, G.; Fauci, A.S. Immunopathogenesis of HIV infection. Ann. Rev. Microbiol. 1996, 50, 825–854. [Google Scholar] [CrossRef] [PubMed]
- Gurdasani, D.; Iles, L.; Dillon, D.G.; Young, E.H.; Olson, A.D.; Naranbhai, V.; Fidler, S.; Gkrania-Klotsas, E.; Post, F.A.; Kellam, P.; et al. A systematic review of definitions of extreme phenotypes of HIV control and progression. AIDS 2014, 28, 149–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estes, J.D.; LeGrand, R.; Petrovas, C. Visualizing the immune system: Providing key insights into HIV/SIV infections. Front. Immunol. 2018, 9, 423. [Google Scholar] [CrossRef] [PubMed]
- Biasin, M.; De Luca, M.; Gnudi, F.; Clerici, M. The genetic basis of resistance to HIV infection and disease progression. Expert Rev. Clin. Immunol. 2013, 9, 319–334. [Google Scholar] [CrossRef] [PubMed]
- Autier, P.; Boniol, M.; Pizot, C.; Mullie, P. Vitamin D status and ill health: A systematic review. Lancet Diabetes Endocrinol. 2014, 2, 76–89. [Google Scholar] [CrossRef]
- Jimenez-Sousa, M.A.; Martinez, I.; Medrano, L.M.; Fernandez-Rodriguez, A.; Resino, S. Vitamin D in human immunodeficiency virus infection: Influence on immunity and disease. Front. Immunol. 2018, 9, 458. [Google Scholar] [CrossRef] [PubMed]
- Lucas, R.M.; Gorman, S.; Geldenhuys, S.; Hart, P.H. Vitamin D and immunity. F1000Prime Rep. 2014, 6, 118. [Google Scholar] [CrossRef] [PubMed]
- Mansueto, P.; Seidita, A.; Vitale, G.; Gangemi, S.; Iaria, C.; Cascio, A. Vitamin D deficiency in HIV infection: Not only a bone disorder. BioMed Res. Int. 2015, 2015, 735615. [Google Scholar] [CrossRef] [PubMed]
- Gois, P.H.F.; Ferreira, D.; Olenski, S.; Seguro, A.C. Vitamin D and infectious diseases: Simple bystander or contributing factor? Nutrients 2017, 9, 651. [Google Scholar] [CrossRef] [PubMed]
- Hossein-nezhad, A.; Holick, M.F. Vitamin D for health: A global perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; van Meurs, J.B.; d’Alesio, A.; Jhamai, M.; Zhao, H.; Rivadeneira, F.; Hofman, A.; van Leeuwen, J.P.; Jehan, F.; Pols, H.A.; et al. Promoter and 3’-untranslated-region haplotypes in the vitamin D receptor gene predispose to osteoporotic fracture: The rotterdam study. Am. J. Hum. Genet. 2005, 77, 807–823. [Google Scholar] [CrossRef] [PubMed]
- Nejentsev, S.; Godfrey, L.; Snook, H.; Rance, H.; Nutland, S.; Walker, N.M.; Lam, A.C.; Guja, C.; Ionescu-Tirgoviste, C.; Undlien, D.E.; et al. Comparative high-resolution analysis of linkage disequilibrium and tag single nucleotide polymorphisms between populations in the vitamin D receptor gene. Hum. Mol. Genet. 2004, 13, 1633–1639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jolliffe, D.A.; Walton, R.T.; Griffiths, C.J.; Martineau, A.R. Single nucleotide polymorphisms in the vitamin D pathway associating with circulating concentrations of vitamin D metabolites and non-skeletal health outcomes: Review of genetic association studies. J. Steroid Biochem. Mol. Biol. 2016, 164, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Barber, Y.; Rubio, C.; Fernandez, E.; Rubio, M.; Fibla, J. Host genetic background at CCR5 chemokine receptor and vitamin D receptor loci and human immunodeficiency virus (HIV) type 1 disease progression among HIV-seropositive injection drug users. J. Infect. Dis. 2001, 184, 1279–1288. [Google Scholar] [CrossRef] [PubMed]
- Laplana, M.; Sanchez-de-la-Torre, M.; Puig, T.; Caruz, A.; Fibla, J. Vitamin-D pathway genes and HIV-1 disease progression in injection drug users. Gene 2014, 545, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Nieto, G.; Barber, Y.; Rubio, M.C.; Rubio, M.; Fibla, J. Association between AIDS disease progression rates and the Fok-I polymorphism of the VDR gene in a cohort of HIV-1 seropositive patients. J. Steroid Biochem. Mol. Biol. 2004, 89–90, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Torres, C.; Sanchez de la Torre, M.; Garcia-Moruja, C.; Carrero, A.J.; Trujillo Mdel, M.; Fibla, J.; Caruz, A. Immunophenotype of vitamin D receptor polymorphism associated to risk of HIV-1 infection and rate of disease progression. Curr. HIV Res. 2010, 8, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Merino, I.; de Las Cuevas, N.; Jimenez, J.L.; Gallego, J.; Gomez, C.; Prieto, C.; Serramia, M.J.; Lorente, R.; Munoz-Fernandez, M.A. The Spanish HIV BioBank: A model of cooperative HIV research. Retrovirology 2009, 6, 27. [Google Scholar] [CrossRef] [PubMed]
- Sobrino-Vegas, P.; Gutierrez, F.; Berenguer, J.; Labarga, P.; Garcia, F.; Alejos-Ferreras, B.; Munoz, M.A.; Moreno, S.; del Amo, J. The Cohort of the Spanish HIV Research Network (CoRIS) and its associated biobank; organizational issues, main findings and losses to follow-up. Enferm. Infec. Microbiol. Clin. 2011, 29, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Guzman-Fulgencio, M.; Jimenez, J.L.; Garcia-Alvarez, M.; Bellon, J.M.; Fernandez-Rodriguez, A.; Campos, Y.; Rodriguez, C.; Gonzalez-Garcia, J.; Riera, M.; Viciana, P.; et al. Mitochondrial haplogroups are associated with clinical pattern of AIDS progression in HIV-infected patients. J. Acquir. Immune Defic. Syndr. 2013, 63, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Guzman-Fulgencio, M.; Jimenez, J.L.; Jimenez-Sousa, M.A.; Bellon, J.M.; Garcia-Alvarez, M.; Soriano, V.; Gijon-Vidaurreta, P.; Bernal-Morell, E.; Viciana, P.; Munoz-Fernandez, M.A.; et al. ACSM4 polymorphisms are associated with rapid AIDS progression in HIV-infected patients. J. Acquir. Immune Defic. Syndr. 2014, 65, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Alagarasu, K.; Selvaraj, P.; Swaminathan, S.; Narendran, G.; Narayanan, P.R. 5′ regulatory and 3′ untranslated region polymorphisms of vitamin D receptor gene in south Indian HIV and HIV-TB patients. J. Clin. Immunol. 2009, 29, 196–204. [Google Scholar] [CrossRef] [PubMed]
- De la Torre, M.S.; Torres, C.; Nieto, G.; Vergara, S.; Carrero, A.J.; Macias, J.; Pineda, J.A.; Caruz, A.; Fibla, J. Vitamin D receptor gene haplotypes and susceptibility to HIV-1 infection in injection drug users. J. Infect. Dis. 2008, 197, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Jimenez, W.; Villegas-Ospina, S.; Gonzalez, S.; Zapata, W.; Saulle, I.; Garziano, M.; Biasin, M.; Clerici, M.; Rugeles, M.T. Precursor forms of vitamin D reduce HIV-1 infection in vitro. J. Acquir. Immune Defic. Syndr. 2016, 73, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Nunnari, G.; Fagone, P.; Lazzara, F.; Longo, A.; Cambria, D.; Di Stefano, G.; Palumbo, M.; Malaguarnera, L.; Di Rosa, M. Vitamin D3 inhibits TNFα-induced latent HIV reactivation in J-LAT cells. Mol. Cell. Biochem. 2016, 418, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Mendes, M.M.; Darling, A.L.; Hart, K.H.; Morse, S.; Murphy, R.J.; Lanham-New, S.A. Impact of high latitude, urban living and ethnicity on 25-hydroxyvitamin D status: A need for multidisciplinary action? J. Steroid Biochem. Mol. Biol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Gross, C.; Eccleshall, T.R.; Malloy, P.J.; Villa, M.L.; Marcus, R.; Feldman, D. The presence of a polymorphism at the translation initiation site of the vitamin D receptor gene is associated with low bone mineral density in postmenopausal Mexican-American women. J. Bone Min. Res. 1996, 11, 1850–1855. [Google Scholar] [CrossRef] [PubMed]
- Laplana, M.; Royo, J.L.; Fibla, J. Vitamin D Receptor polymorphisms and risk of enveloped virus infection: A meta-analysis. Gene 2018, 678, 384–394. [Google Scholar] [CrossRef] [PubMed]
- Ogunkolade, B.W.; Boucher, B.J.; Prahl, J.M.; Bustin, S.A.; Burrin, J.M.; Noonan, K.; North, B.V.; Mannan, N.; McDermott, M.F.; DeLuca, H.F.; et al. Vitamin D receptor (VDR) mRNA and VDR protein levels in relation to vitamin D status, insulin secretory capacity, and VDR genotype in Bangladeshi Asians. Diabetes 2002, 51, 2294–2300. [Google Scholar] [CrossRef] [PubMed]
- Kholghi Oskooei, V.; Geranpayeh, L.; Omrani, M.D.; Ghafouri-Fard, S. Assessment of functional variants and expression of long noncoding RNAs in vitamin D receptor signaling in breast cancer. Cancer Manag. Res. 2018, 10, 3451–3462. [Google Scholar] [CrossRef] [PubMed]
- Moran-Auth, Y.; Penna-Martinez, M.; Shoghi, F.; Ramos-Lopez, E.; Badenhoop, K. Vitamin D status and gene transcription in immune cells. J. Steroid Biochem. Mol. Biol. 2013, 136, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Vanessa, O.N.; Asani, F.F.; Jeffery, T.J.; Saccone, D.S.; Bornman, L. Vitamin D receptor gene expression and function in a south African population: Ethnicity, vitamin D and FokI. PLoS ONE 2013, 8, e67663. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Controls vs. All HIV Patients | HIV Groups of Patients | |||||
|---|---|---|---|---|---|---|---|
| Control | All HIV (*) | p-Value (a) | LTNPs | MPs | RPs | p-Value (b) | |
| No. | 113 | 667 | 183 | 334 | 150 | ||
| Male | 93 (82.3%) | 540 (81.4%) | 0.829 | 115 (64.2%) | 283 (84.7%) | 142 (94.7%) | <0.001 |
| Age (years) | 42.0 (37.0; 49.0) | 41.3 (35.0; 48.4) | 0.427 | 48.7 (46.0; 51.7) | 38.2 (33.2; 45.3) | 38.3 (33.0; 43.8) | <0.001 |
| Age of HIV diagnosis | – | 34.3 (29.0; 40.4) | – | 39.8 (34.3; 43.7) | 31.8 (27.0; 38.4) | 34.0 (29.6; 38.1) | <0.001 |
| Year of HIV diagnosis | – | 2006 (1999; 2008) | – | 1993 (1990; 1997) | 2006 (2004; 2008) | 2009 (2007; 2010) | <0.001 |
| HIV acquired | – | – | |||||
| IDU | – | 166 (25.0%) | – | 130 (72.6%) | 29 (8.7%) | 7 (4.7%) | <0.001 |
| Homosexual | – | 359 (54.1%) | – | 13 (7.3%) | 220 (65.9%) | 126 (84.0%) | |
| Heterosexual | – | 118 (17.8%) | – | 27 (15.1%) | 76 (22.8%) | 15 (10.0%) | |
| Others | – | 20 (3.0%) | – | 9 (5.0%) | 9 (2.7%) | 2 (1.3%) | |
| SNPs | HWE | Control | HWE | All HIV | p-Value | ||
|---|---|---|---|---|---|---|---|
| rs11568820 | n = 112 | n = 665 | |||||
| 0.616 | CC | 59.8% | 0.501 | CC | 57.0% | 0.800 | |
| CT | 33.9% | CT | 35.3% | ||||
| TT | 6.3% | TT | 7.7% | ||||
| rs1544410 | n = 112 | n = 666 | |||||
| 0.233 | CC | 36.6% | 0.835 | CC | 37.1% | 0.477 | |
| CT | 42.9% | CT | 46.8% | ||||
| TT | 20.5% | TT | 16.1% | ||||
| rs2228570 | n = 112 | n = 664 | |||||
| 0.474 | CC | 48.2% | 0.812 | CC | 41.7% | 0.435 | |
| CT | 40.2% | CT | 44.9% | ||||
| TT | 11.6% | TT | 13.4% | ||||
| rs4516035 | n = 113 | n = 666 | |||||
| 0.149 | TT | 40.7% | 0.895 | TT | 40.4% | 0.202 | |
| CT | 40.7% | CT | 46.8% | ||||
| CC | 18.6% | CC | 12.8% | ||||
| rs7975232 | n = 113 | n = 662 | |||||
| 0.294 | AA | 37.2% | 0.862 | AA | 29.0% | 0.217 | |
| AC | 43.4% | AC | 48.9% | ||||
| CC | 19.5% | CC | 22.1% | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez-Sousa, M.A.; Jiménez, J.L.; Fernández-Rodríguez, A.; Brochado-Kith, O.; Bellón, J.M.; Gutierrez, F.; Díez, C.; Bernal-Morell, E.; Viciana, P.; Muñoz-Fernández, M.A.; et al. VDR rs2228570 Polymorphism Is Related to Non-Progression to AIDS in Antiretroviral Therapy Naïve HIV-Infected Patients. J. Clin. Med. 2019, 8, 311. https://doi.org/10.3390/jcm8030311
Jiménez-Sousa MA, Jiménez JL, Fernández-Rodríguez A, Brochado-Kith O, Bellón JM, Gutierrez F, Díez C, Bernal-Morell E, Viciana P, Muñoz-Fernández MA, et al. VDR rs2228570 Polymorphism Is Related to Non-Progression to AIDS in Antiretroviral Therapy Naïve HIV-Infected Patients. Journal of Clinical Medicine. 2019; 8(3):311. https://doi.org/10.3390/jcm8030311
Chicago/Turabian StyleJiménez-Sousa, María A., José Luis Jiménez, Amanda Fernández-Rodríguez, Oscar Brochado-Kith, José María Bellón, Félix Gutierrez, Cristina Díez, Enrique Bernal-Morell, Pompeyo Viciana, María A. Muñoz-Fernández, and et al. 2019. "VDR rs2228570 Polymorphism Is Related to Non-Progression to AIDS in Antiretroviral Therapy Naïve HIV-Infected Patients" Journal of Clinical Medicine 8, no. 3: 311. https://doi.org/10.3390/jcm8030311