A Novel Osteotomy Preparation Technique to Preserve Implant Site Viability and Enhance Osteogenesis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals and Experimental Plan
2.2. Ovariectomy and Tooth Extraction
2.3. Osteotomy Site Preparation
2.4. Tissue Collection and Processing
2.5. Histology
2.6. Quantification of Programmed Cell Death
2.7. Tartrate-Resistant Acid Phosphatase (TRAP) Activity
2.8. Immunostaining
2.9. Histomorphometric Analyses
2.10. Micro-Computed Tomography (µCT)
2.11. Calculation of Osteotomy Surface Roughness
2.12. Heat Transfer During Drilling
2.13. Statistical Analyses
3. Results
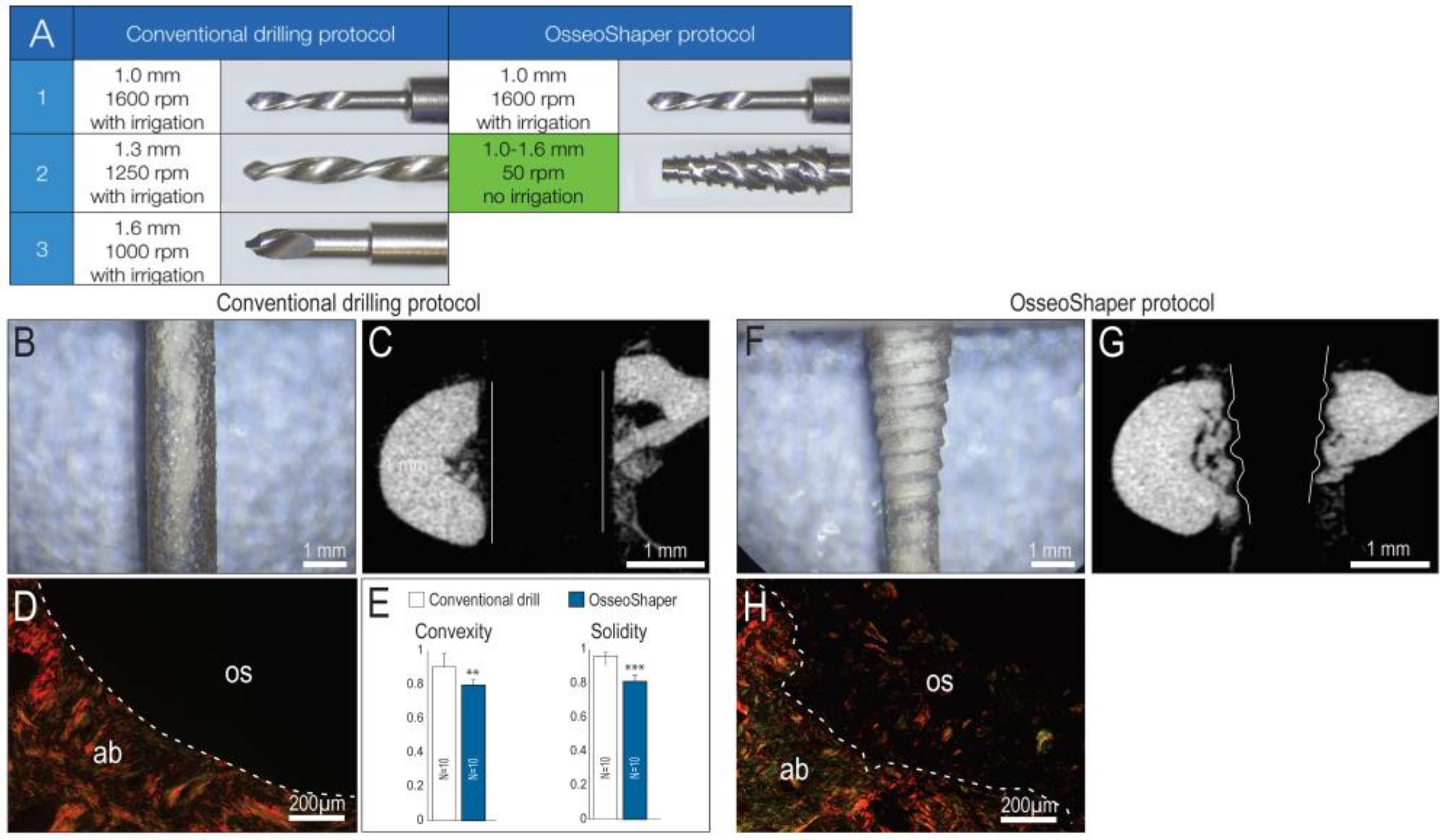
3.1. A New Surgical Drilling Tool That Cuts Efficiently at Very Low Speeds
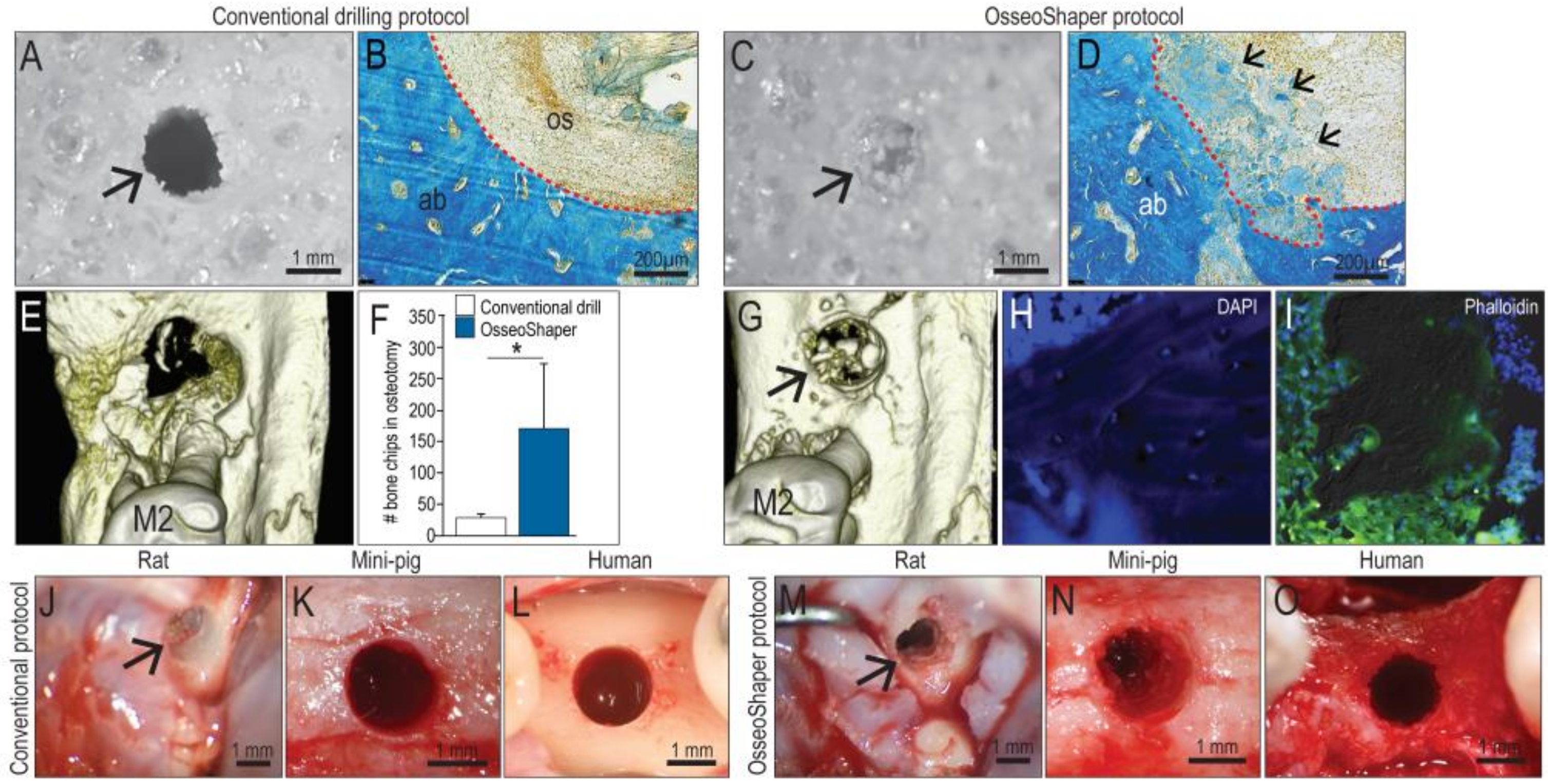
3.2. The OsseoShaper Allows the Retention of Viable, Autologous Bone Chips in the Osteotomy
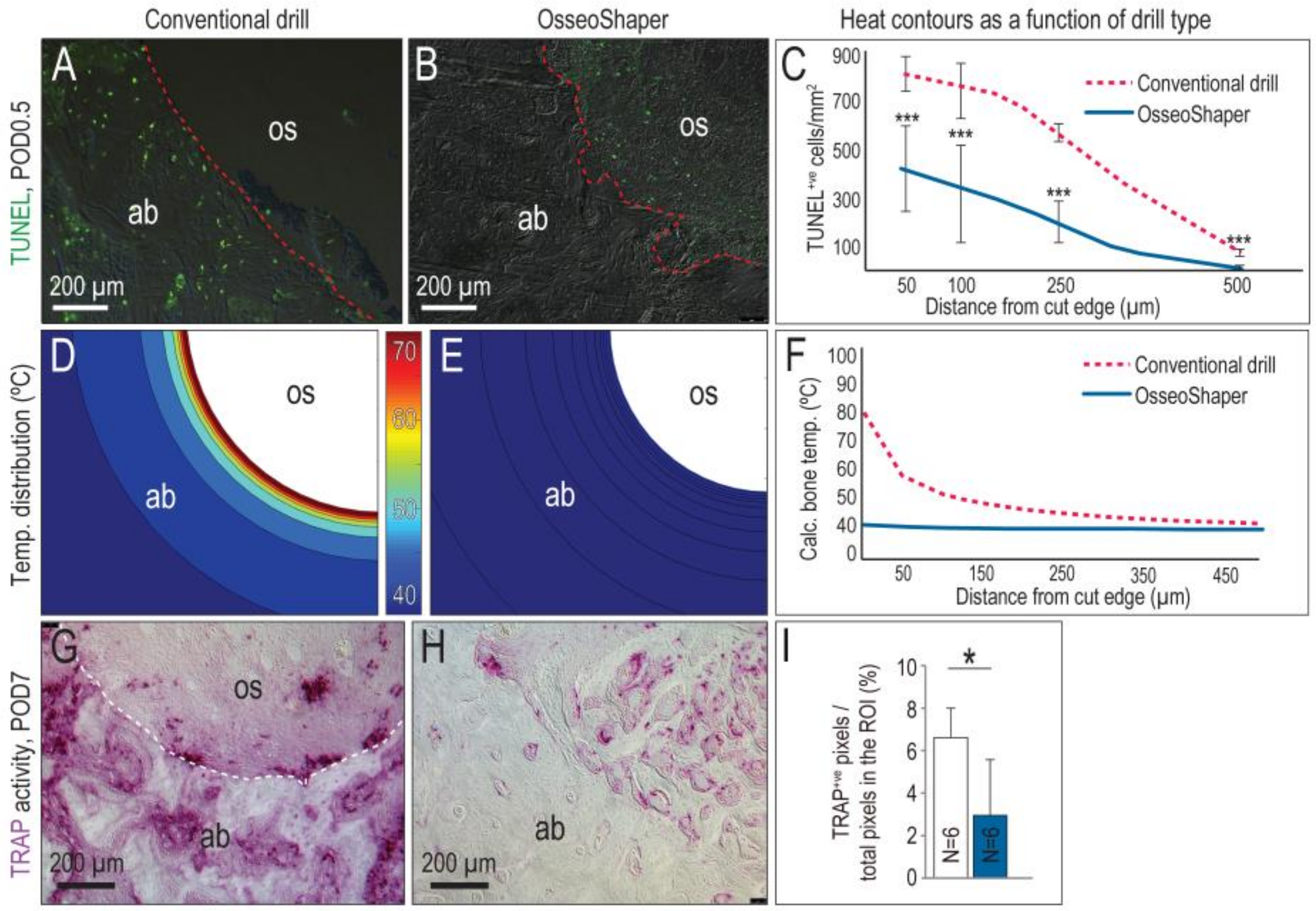
3.3. The Mini OsseoShaper Preserves Peri-Implant Bone by Limiting Heat Transfer and Minimizing Thermal Apoptosis
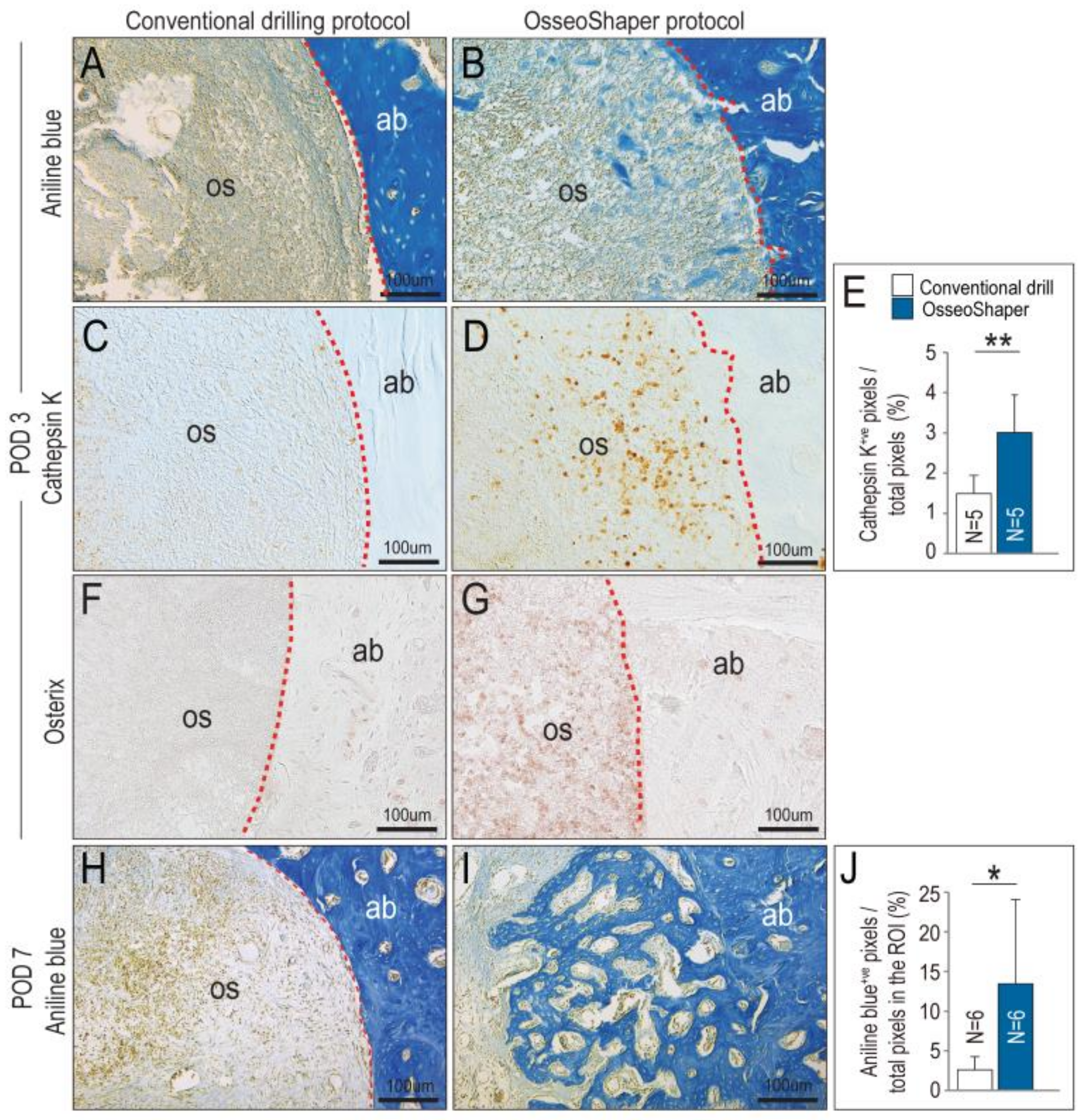
3.4. In Mini OsseoShaper Osteotomies, New Bone Formation Is Accelerated
4. Discussion
4.1. A Unique Design That Enables Retention of Bone Chips and Osseous Coagulum in an Osteotomy Site
4.2. A Streamlined Protocol for Osteotomy Site Preparation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jackson, C.J.; Ghosh, S.K.; Johnson, W. On the evolution of drill-bit shapes. J. Mech. Work Technol. 1989, 18, 231–267. [Google Scholar] [CrossRef]
- Pandey, R.K.; Panda, S.S. Drilling of bone: A comprehensive review. J. Clin. Orthop. Trauma 2013, 4, 15–30. [Google Scholar] [CrossRef] [PubMed]
- Abouzgia, M.B.; James, D.F. Measurements of shaft speed while drilling through bone. J. Oral. Maxillofac. Surg. 1995, 53, 1308–1315, Discussion in 1995, 53, 1315–1316. [Google Scholar] [CrossRef]
- Yan, P.; Rong, Y.M.; Wang, G. The effect of cutting fluids applied in metal cutting process. Proc. Inst. Mech. Eng. B 2016, 230, 19–37. [Google Scholar] [CrossRef]
- Aghvami, M.; Brunski, J.B.; Serdar Tulu, U.; Chen, C.H.; Helms, J.A. A Thermal and Biological Analysis of Bone Drilling. J. Biomech. Eng. 2018, 140. [Google Scholar] [CrossRef]
- Cha, J.Y.; Pereira, M.D.; Smith, A.A.; Houschyar, K.S.; Yin, X.; Mouraret, S.; Brunski, J.B.; Helms, J.A. Multiscale analyses of the bone-implant interface. J. Dent. Res. 2015, 94, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Aghvami, M.; Brunski, J.; Helms, J. Biophysical regulation of osteotomy healing: An animal study. Clin. Implant Dent. Relat. Res. 2017, 19, 590–599. [Google Scholar] [CrossRef] [PubMed]
- Pei, X.; Wang, L.; Chen, C.; Yuan, X.; Wan, Q.; Helms, J.A. Contribution of the PDL to osteotomy repair and implant osseointegration. J. Dent. Res. 2017, 96, 909–916. [Google Scholar] [CrossRef]
- Li, J.; Yin, X.; Huang, L.; Mouraret, S.; Brunski, J.B.; Cordova, L.; Salmon, B.; Helms, J.A. Relationships among bone quality, implant osseointegration, and Wnt signaling. J. Dent. Res. 2017, 96, 822–831. [Google Scholar] [CrossRef]
- Chen, C.H.; Pei, X.; Tulu, U.S.; Aghvami, M.; Chen, C.T.; Gaudilliere, D.; Arioka, M.; Maghazeh Moghim, M.; Bahat, O.; Kolinski, M.; et al. A comparative assessment of implant site viability in humans and rats. J. Dent. Res. 2018, 97, 451–459. [Google Scholar] [CrossRef]
- Chen, C.H.; Wang, L.; Serdar Tulu, U.; Arioka, M.; Moghim, M.M.; Salmon, B.; Chen, C.T.; Hoffmann, W.; Gilgenbach, J.; Brunski, J.B.; et al. An osteopenic/osteoporotic phenotype delays alveolar bone repair. Bone 2018, 112, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Arioka, M.; Zhang, X.; Li, Z.; Tulu, U.S.; Liu, Y.; Wang, L.; Yuan, X.; Helms, J.A. Osteoporotic changes in the periodontium impair alveolar bone healing. J. Dent. Res. 2019. [Google Scholar] [CrossRef]
- Mangano, F.; Mortellaro, C.; Mangano, N.; Mangano, C. Is low serum vitamin d associated with early dental implant failure? A retrospective evaluation on 1625 implants placed in 822 patients. Mediators Inflamm. 2016. [Google Scholar] [CrossRef] [PubMed]
- Kalu, D.N. The ovariectomized rat model of postmenopausal bone loss. Bone Miner. 1991, 15, 175–191. [Google Scholar] [CrossRef]
- Cummings, S.R.; Melton, L.J. Epidemiology and outcomes of osteoporotic fractures. Lancet 2002, 359, 1761–1767. [Google Scholar] [CrossRef]
- Chen, S.T.; Beagle, J.; Jensen, S.S.; Chiapasco, M.; Darby, I. Consensus statements and recommended clinical procedures regarding surgical techniques. Int. J. Oral Maxillofac. Implants 2009, 24, 272–278. [Google Scholar]
- Yin, X.; Li, J.; Chen, T.; Mouraret, S.; Dhamdhere, G.; Brunski, J.B.; Zou, S.; Helms, J.A. Rescuing failed oral implants via Wnt activation. J. Clin. Periodontol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Minear, S.; Leucht, P.; Jiang, J.; Liu, B.; Zeng, A.; Fuerer, C.; Nusse, R.; Helms, J.A. Wnt proteins promote bone regeneration. Sci. Transl. Med. 2010, 2. [Google Scholar] [CrossRef]
- Bouxsein, M.L.; Boyd, S.K.; Christiansen, B.A.; Guldberg, R.E.; Jepsen, K.J.; Muller, R. Guidelines for assessment of bone microstructure in rodents using micro-computed tomography. J. Bone Miner. Res. 2010, 25, 1468–1486. [Google Scholar] [CrossRef]
- Wagner, T.; Lipinski, H.G. IJBlob: An ImageJ library for connected component analysis and shape analysis. J. Open Res. Softw. 2013, 1, 6–8. [Google Scholar]
- Wang, L.; Wu, Y.; Perez, K.C.; Hyman, S.; Brunski, J.B.; Tulu, U.; Bao, C.; Salmon, B.; Helms, J.A. Effects of Condensation on Peri-implant Bone Density and Remodeling. J. Dent. Res. 2017, 96, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Isler, S.C.; Cansiz, E.; Tanyel, C.; Soluk, M.; Selvi, F.; Cebi, Z. The effect of irrigation temperature on bone healing. Int. J. Med. Sci. 2011, 8, 704–708. [Google Scholar] [CrossRef] [PubMed]
- Almeida, K.P.; Delgado-Ruiz, R.; Carneiro, L.G.; Leiva, A.B.; Calvo-Guirado, J.L.; Gomez-Moreno, G.; Malmstrom, H.; Romanos, G.E. Influence of Drilling Speed on Stability of Tapered Dental Implants: An Ex Vivo Experimental Study. Int. J. Oral Maxillofac. Implants 2016, 31, 795–798. [Google Scholar] [CrossRef] [PubMed]
- Dolan, E.B.; Haugh, M.G.; Tallon, D.; Casey, C.; McNamara, L.M. Heat-shock-induced cellular responses to temperature elevations occurring during orthopaedic cutting. J. R. Soc. Interface 2012, 9, 3503–3513. [Google Scholar] [CrossRef] [PubMed]
- Robinson, R.E. The osseous coagulum for bone induction technique. A review. J. Calif. Dent. Assoc. 1970, 46, 18–27. [Google Scholar] [PubMed]
- Robinson, E. Osseous coagulum for bone induction. J. Periodontol. 1969, 40, 503–510. [Google Scholar] [CrossRef]
- Preston, C.F.; Fulkerson, E.W.; Meislin, R.; Di Cesare, P.E. Osteotomy about the knee: Applications, techniques, and results. J. Knee Surg. 2005, 18, 258–272. [Google Scholar] [CrossRef]
- Yeniyol, S.; Jimbo, R.; Marin, C.; Tovar, N.; Janal, M.N.; Coelho, P.G. The effect of drilling speed on early bone healing to oral implants. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 550–555. [Google Scholar] [CrossRef]
- Giro, G.; Marin, C.; Granato, R.; Bonfante, E.A.; Suzuki, M.; Janal, M.N.; Coelho, P.G. Effect of drilling technique on the early integration of plateau root form endosteal implants: an experimental study in dogs. J. Oral Maxillofac. Surg. 2011, 69, 2158–2163. [Google Scholar] [CrossRef]
- Miron, R.J.; Gruber, R.; Hedbom, E.; Saulacic, N.; Zhang, Y.; Sculean, A.; Bosshardt, D.D.; Buser, D. Impact of bone harvesting techniques on cell viability and the release of growth factors of autografts. Clin. Implant Dent. Relat. Res. 2013, 15, 481–489. [Google Scholar] [CrossRef]
- Maus, U.; Andereya, S.; Gravius, S.; Siebert, C.H.; Schippmann, T.; Ohnsorge, J.A.; Niedhart, C. How to store autologous bone graft perioperatively: an in vitro study. Arch. Orthop. Trauma Surg. 2008, 128, 1007–1011. [Google Scholar] [CrossRef] [PubMed]
- Laursen, M.; Christensen, F.B.; Bunger, C.; Lind, M. Optimal handling of fresh cancellous bone graft: different peroperative storing techniques evaluated by in vitro osteoblast-like cell metabolism. Acta Orthop. Scand. 2003, 74, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Davidson, S.R.; James, D.F. Drilling in bone: Modeling heat generation and temperature distribution. J. Biomech. Eng. 2003, 125, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, A.R.; Albrektsson, T. Temperature threshold levels for heat-induced bone tissue injury: A vital-microscopic study in the rabbit. J. Prosthet. Dent. 1983, 50, 101–107. [Google Scholar] [CrossRef]
- Lundskog, J. Heat and bone tissue. An experimental investigation of the thermal properties of bone and threshold levels for thermal injury. Scand. J. Plast. Reconstr. Surg. 1972, 9, 1–80. [Google Scholar] [PubMed]
- Eriksson, A.; Albrektsson, T.; Grane, B.; McQueen, D. Thermal injury to bone. A vital-microscopic description of heat effects. Int. J. Oral Surg. 1982, 11, 115–121. [Google Scholar] [CrossRef]
- Matthews, L.S.; Hirsch, C. Temperatures measured in human cortical bone when drilling. J. Bone Joint. Surg. Am. 1972, 54, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Tawy, G.F.; Rowe, P.J.; Riches, P.E. Thermal damage done to bone by burring and sawing with and without irrigation in knee arthroplasty. J. Arthroplasty 2016, 31, 1102–1108. [Google Scholar] [CrossRef]
- Gazdag, A.R.; Lane, J.M.; Glaser, D.; Forster, R.A. Alternatives to autogenous bone graft: Efficacy and indications. J. Am. Acad Orthop. Surg. 1995, 3, 1–8. [Google Scholar] [CrossRef]
- Khan, S.N.; Cammisa, F.P., Jr.; Sandhu, H.S.; Diwan, A.D.; Girardi, F.P.; Lane, J.M. The biology of bone grafting. J. Am. Acad Orthop. Surg. 2005, 13, 77–86. [Google Scholar] [CrossRef]
- Burchardt, H. Biology of bone transplantation. Orthop. Clin. North Am. 1987, 18, 187–196. [Google Scholar] [PubMed]
- Chen, T.; Li, J.; Cordova, L.A.; Liu, B.; Mouraret, S.; Sun, Q.; Salmon, B.; Helms, J. A WNT protein therapeutic improves the bone-forming capacity of autografts from aged animals. Sci. Rep. 2018, 8, 119. [Google Scholar] [CrossRef] [PubMed]
- Bertollo, N.; Walsh, W.R. Drilling of bone: Practicality, limitations and complications associated with surgical drill-bits. Biomech. Appl. 2011. [Google Scholar] [CrossRef]
- Lustmann, J.; Ulmansky, M.; Fuxbrunner, A.; Lewis, A. Photoacoustic injury and bone healing following 193nm excimer laser ablation. Lasers Surg. Med. 1992, 12, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Venugopalan, V. Mechanisms of pulsed laser ablation of biological tissues. Chem. Rev. 2003, 103, 577–644. [Google Scholar] [CrossRef] [PubMed]
- Leucht, P.; Lam, K.; Kim, J.B.; Mackanos, M.A.; Simanovskii, D.M.; Longaker, M.T.; Contag, C.H.; Schwettman, H.A.; Helms, J.A. Accelerated bone repair after plasma laser corticotomies. Ann. Surg. 2007, 246, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Romanos, G.E.; Gupta, B.; Yunker, M.; Romanos, E.B.; Malmstrom, H. Lasers use in dental implantology. Implant Dent. 2013, 22, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Rivault, A.F.; Toto, P.D.; Levy, S.; Gargiulo, A.W. Autogenous bone grafts: osseous coagulum and osseous retrograde procedures in primates. J. Periodontol. 1971, 42, 787–796. [Google Scholar] [CrossRef]
- Bell, S.; Ajami, E.; Davies, J.E. An improved mechanical testing method to assess bone-implant anchorage. J. Vis. Exp. 2014. [Google Scholar] [CrossRef]
- Young, M.P.; Worthington, H.V.; Lloyd, R.E.; Drucker, D.B.; Sloan, P.; Carter, D.H. Bone collected during dental implant surgery: A clinical and histological study. Clin. Oral Implants Res. 2002, 13, 298–303. [Google Scholar] [CrossRef]
- Schneider, D.; Marquardt, P.; Zwahlen, M.; Jung, R.E. A systematic review on the accuracy and the clinical outcome of computer-guided template-based implant dentistry. Clin. Oral Implants Res. 2009, 20 (Suppl. 4), 73–86. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, J.; Zuabi, O.; Machtei, E.E. Accuracy of a computerized tomography-guided template-assisted implant placement system: an in vitro study. Clin. Oral Implants Res. 2009, 20, 1156–1162. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Company | External Diameter | Product Identifier |
|---|---|---|
| OsteoMed | 1.0 mm | 220-0065 |
| OsteoMed | 1.3 mm | 220-0064 |
| OsteoMed | 1.6 mm | 220-0116 |
| Downscaled prototype of the OsseoShaper | 1.0 mm (apex) 1.6 mm (crest) | Non-commercial prototype |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-H.; Coyac, B.R.; Arioka, M.; Leahy, B.; Tulu, U.S.; Aghvami, M.; Holst, S.; Hoffmann, W.; Quarry, A.; Bahat, O.; et al. A Novel Osteotomy Preparation Technique to Preserve Implant Site Viability and Enhance Osteogenesis. J. Clin. Med. 2019, 8, 170. https://doi.org/10.3390/jcm8020170
Chen C-H, Coyac BR, Arioka M, Leahy B, Tulu US, Aghvami M, Holst S, Hoffmann W, Quarry A, Bahat O, et al. A Novel Osteotomy Preparation Technique to Preserve Implant Site Viability and Enhance Osteogenesis. Journal of Clinical Medicine. 2019; 8(2):170. https://doi.org/10.3390/jcm8020170
Chicago/Turabian StyleChen, Chih-Hao, Benjamin R. Coyac, Masaki Arioka, Brian Leahy, U. Serdar Tulu, Maziar Aghvami, Stefan Holst, Waldemar Hoffmann, Antony Quarry, Oded Bahat, and et al. 2019. "A Novel Osteotomy Preparation Technique to Preserve Implant Site Viability and Enhance Osteogenesis" Journal of Clinical Medicine 8, no. 2: 170. https://doi.org/10.3390/jcm8020170