Use of Hyperspectral/Multispectral Imaging in Gastroenterology. Shedding Some–Different–Light into the Dark

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
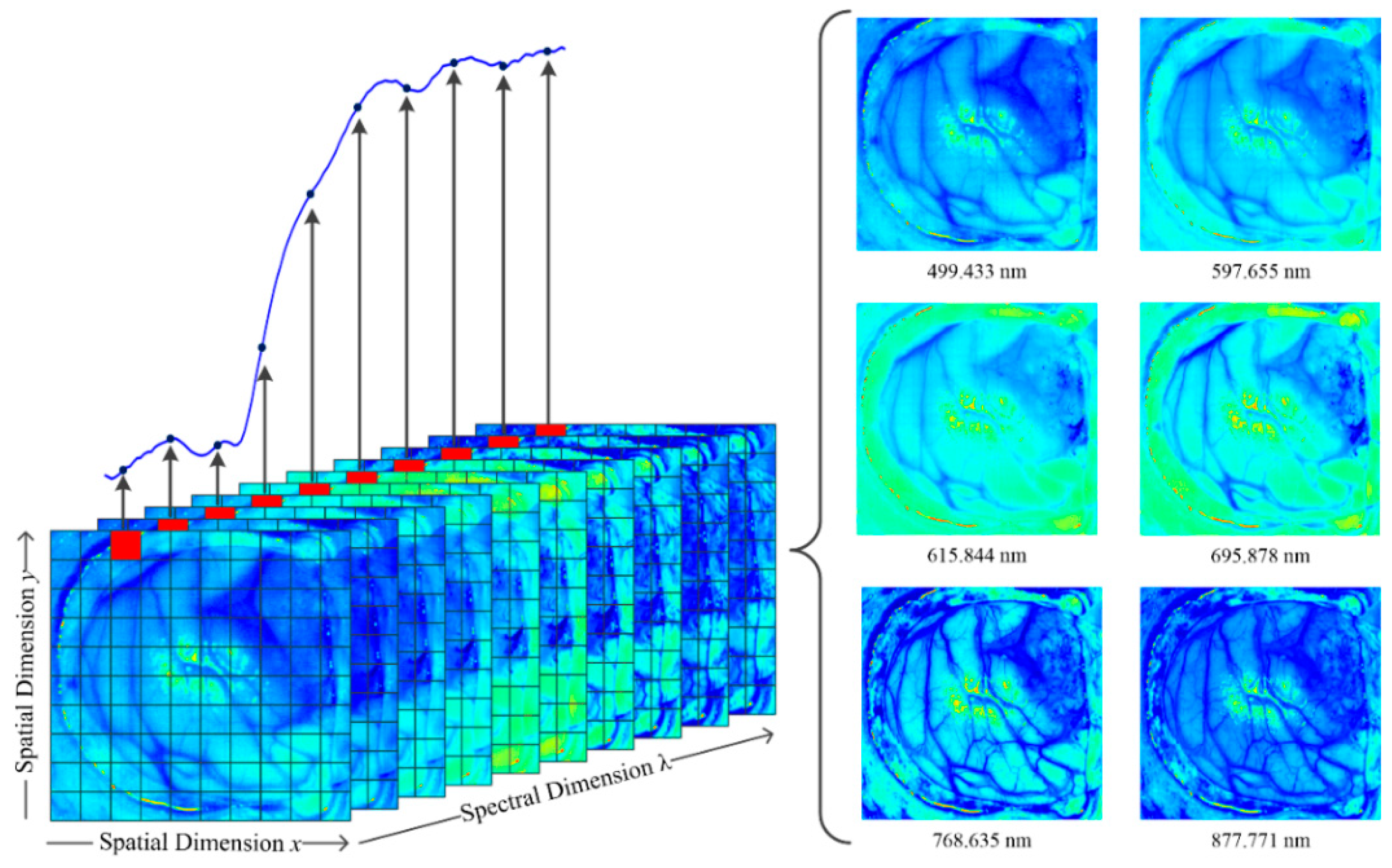
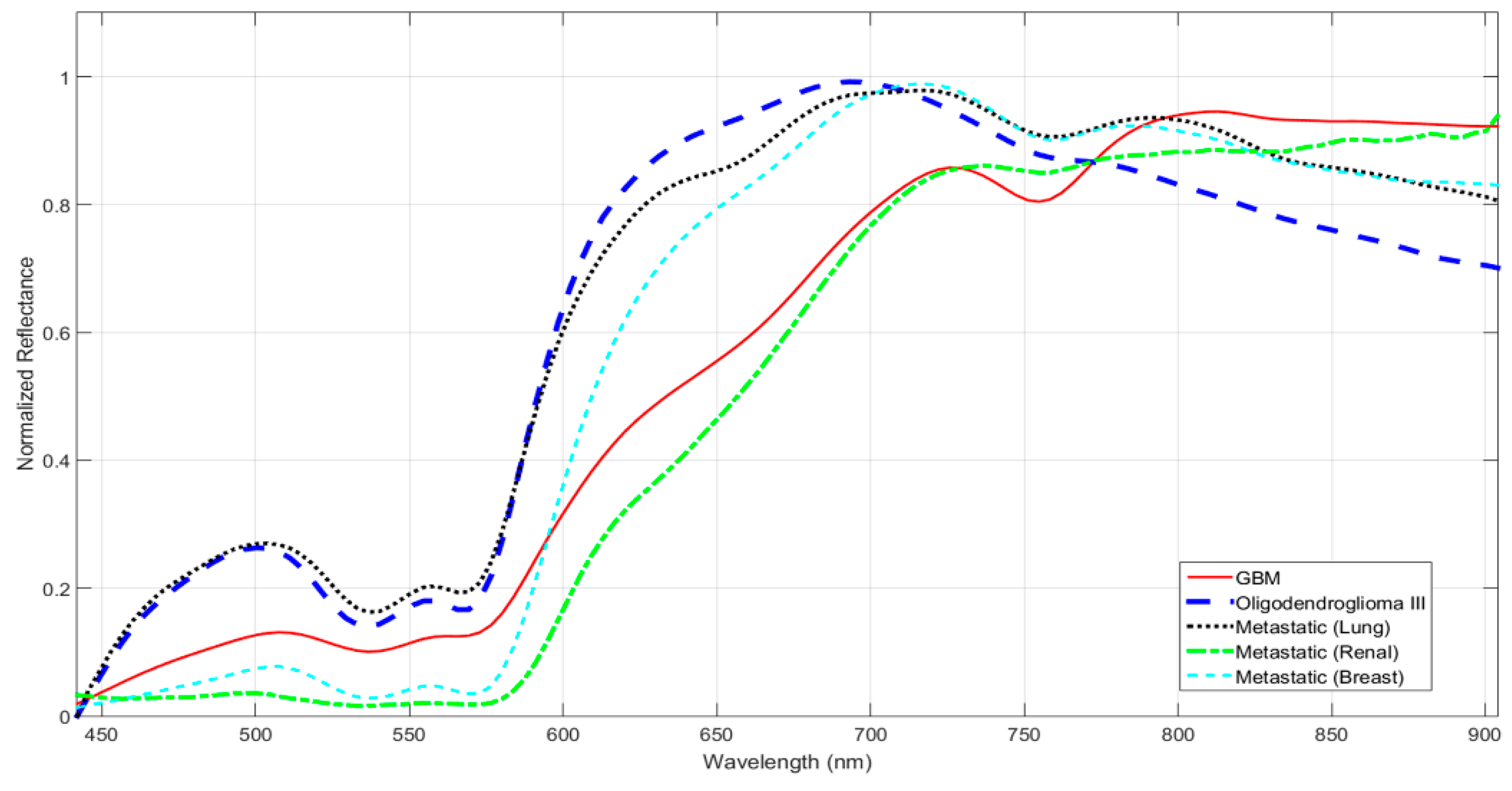
2. Medical Hyperspectral Imaging
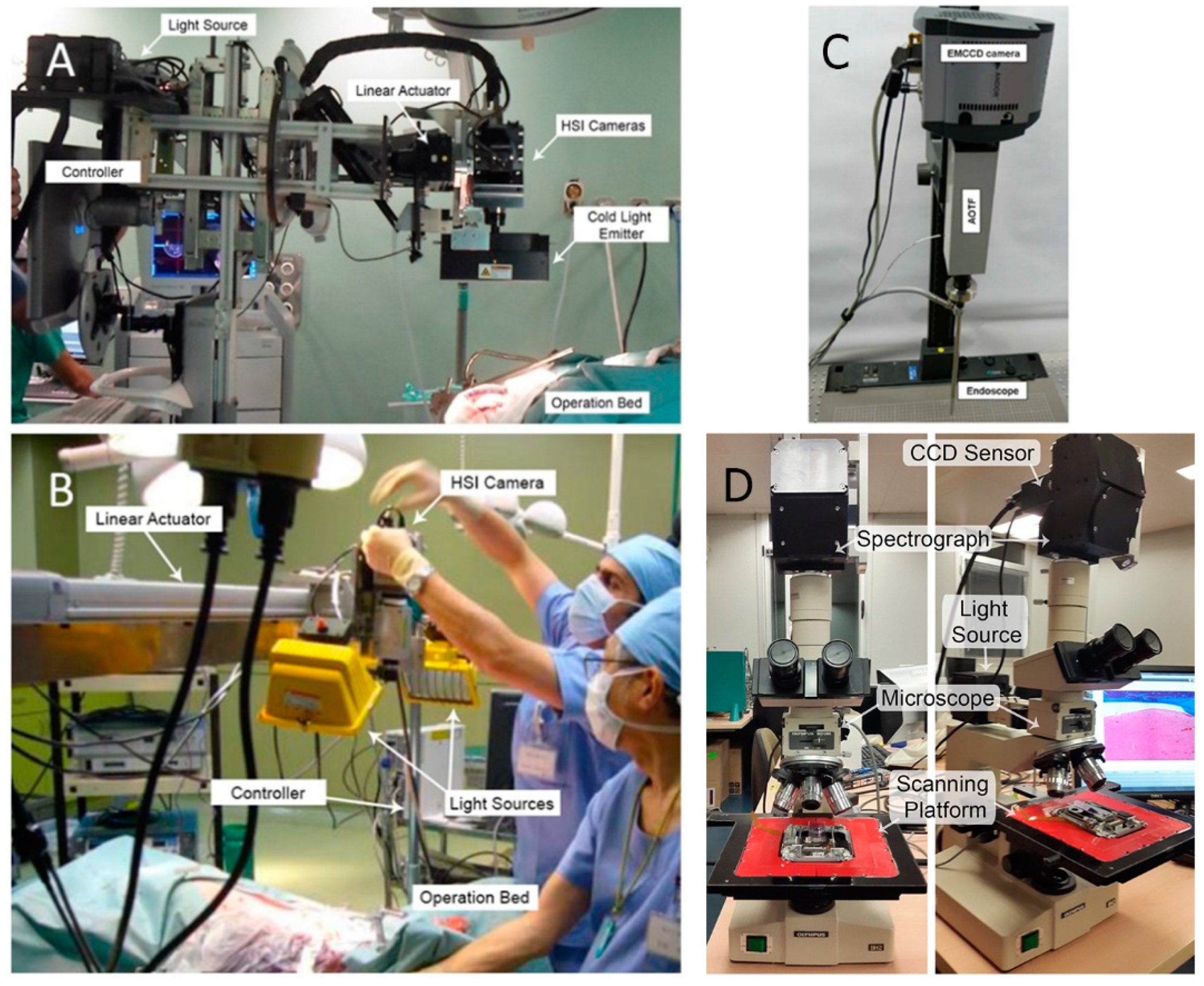
3. Hyperspectral Systems
4. Hyperspectral Image Analysis
5. Hyperspectral Imaging in GI Diagnosis
5.1. Surgical Assistance in Real-Time
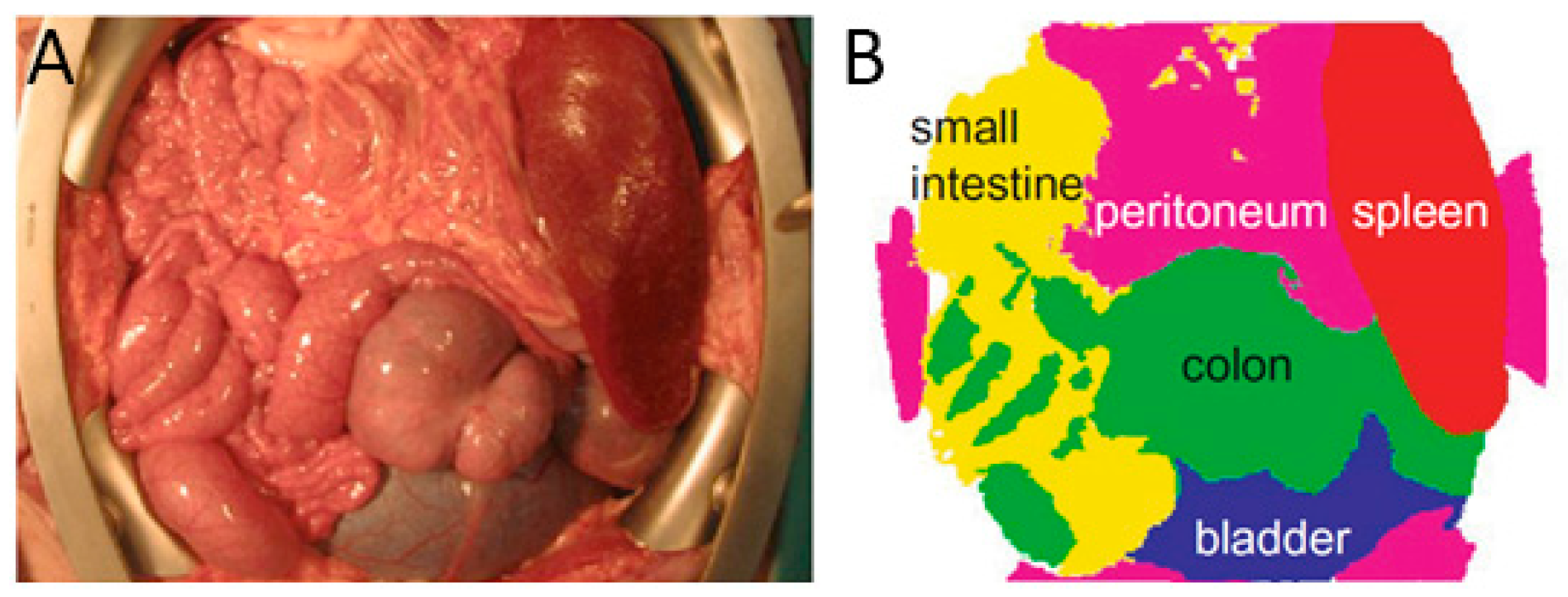
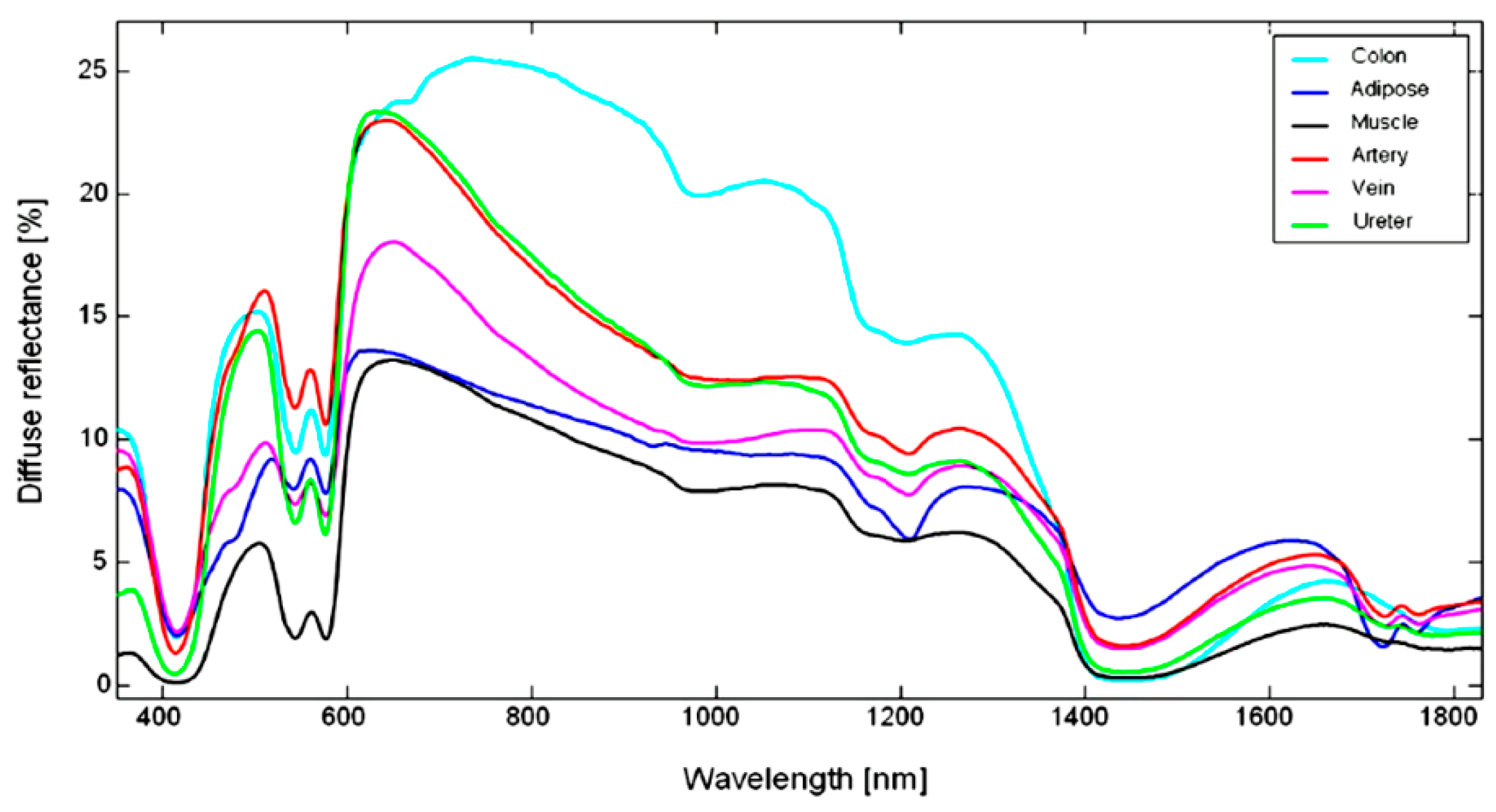
5.1.1. Abdominal Organs Differentiation
5.1.2. Colorectal Surgery
5.1.3. Bowel Anastomosis
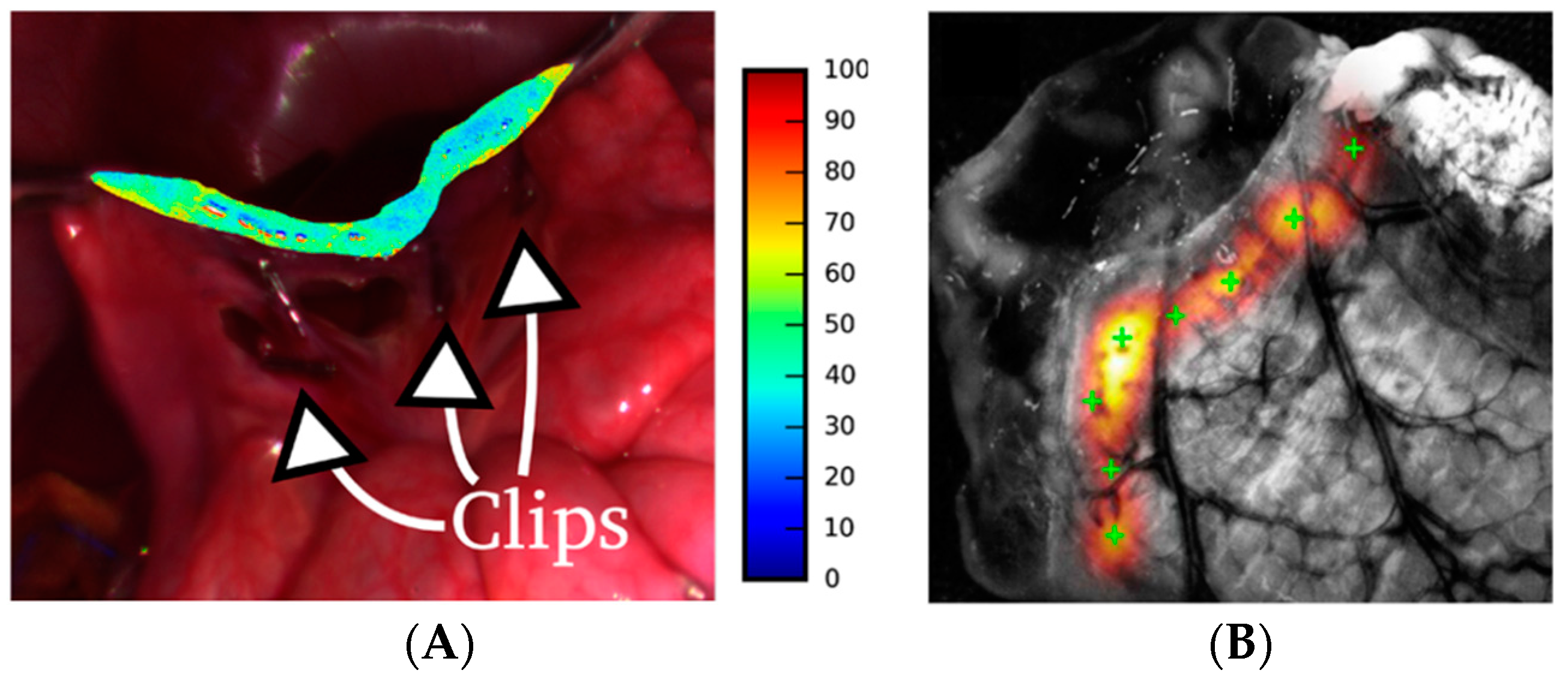
5.1.4. Biliary Anatomy Identification
5.1.5. Intestinal Ischemia Identification
5.1.6. Gastric Cancer Identification
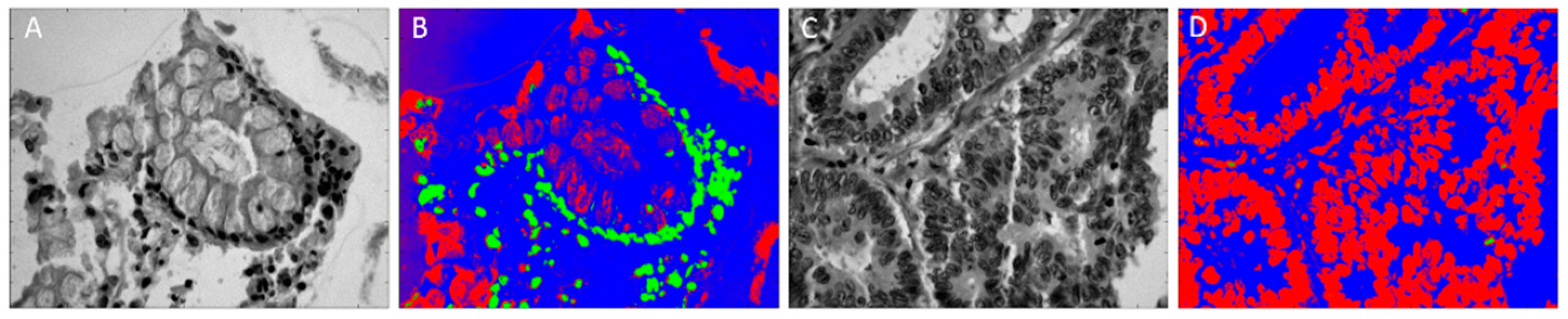
5.2. Pathological Assistance
5.3. HSI Application Summary
6. Discussion
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Grahn, H.F.; Geladi, P. (Eds.) Techniques and Applications of Hyperspectral Image Analysis; John Wiley & Sons, Ltd.: Chichester, UK, 2007; ISBN 9780470010884. [Google Scholar]
- Feng, Y.-Z.; Sun, D.-W. Application of Hyperspectral Imaging in Food Safety Inspection and Control: A Review. Crit. Rev. Food Sci. Nutr. 2012, 52, 1039–1058. [Google Scholar] [CrossRef] [PubMed]
- Lorente, D.; Aleixos, N.; Gómez-Sanchis, J.; Cubero, S.; García-Navarrete, O.L.; Blasco, J. Recent Advances and Applications of Hyperspectral Imaging for Fruit and Vegetable Quality Assessment. Food Bioprocess Technol. 2011, 5, 1121–1142. [Google Scholar] [CrossRef] [Green Version]
- Tatzer, P.; Wolf, M.; Panner, T. Industrial application for inline material sorting using hyperspectral imaging in the NIR range. Real-Time Imaging 2005, 11, 99–107. [Google Scholar] [CrossRef]
- Kubik, M. Chapter 5 Hyperspectral Imaging: A New Technique for the Non-Invasive Study of Artworks. Phys. Tech. Study Art, Archaeol. Cult. Herit. 2007, 2, 199–259. [Google Scholar] [CrossRef]
- Cucci, C.; Delaney, J.K.; Picollo, M. Reflectance Hyperspectral Imaging for Investigation of Works of Art: Old Master Paintings and Illuminated Manuscripts. Acc. Chem. Res. 2016, 49, 2070–2079. [Google Scholar] [CrossRef] [PubMed]
- Brossard, M.; Marion, R.; Carrére, V. Deconvolution of SWIR reflectance spectra for automatic mineral identification in hyperspectral imaging. Remote Sens. Lett. 2016, 7, 581–590. [Google Scholar] [CrossRef]
- Ben-Dor, E. Quantitative remote sensing of soil properties. In Advances in Agronomy; Elsevier BV: Amsterdam, The Netherlands, 2002; pp. 173–243. [Google Scholar]
- Behmann, J.; Steinrücken, J.; Plümer, L. Detection of early plant stress responses in hyperspectral images. ISPRS J. Photogramm. Remote Sens. 2014, 93, 98–111. [Google Scholar] [CrossRef]
- Fabelo, H.; Ortega, S.; Lazcano, R.; Madroñal, D.; MCallicó, G.; Juárez, E.; Salvador, R.; Bulters, D.; Bulstrode, H.; Szolna, A.; et al. An intraoperative visualization system using hyperspectral imaging to aid in brain tumor delineation. Sensors 2018, 18. [Google Scholar] [CrossRef]
- Handbook of Biomedical Optics; CRC Press: Boca Raton, FL, USA, 2016; ISBN 9781420090369.
- Jacques, S.L. Optical properties of biological tissues: A review. Phys. Med. Biol. 2013, 58, R37–R61. [Google Scholar] [CrossRef]
- Li, Q.; He, X.; Wang, Y.; Liu, H.; Xu, D.; Guo, F. Review of spectral imaging technology in biomedical engineering: Achievements and challenges. J. Biomed. Opt. 2013. [Google Scholar] [CrossRef]
- Lu, G.; Fei, B. Medical hyperspectral imaging: A review. J. Biomed. Opt. 2014, 19, 10901. [Google Scholar] [CrossRef] [PubMed]
- Calin, M.A.; Parasca, S.V.; Savastru, D.; Manea, D. Hyperspectral Imaging in the Medical Field: Present and Future. Appl. Spectrosc. Rev. 2013, 49, 435–447. [Google Scholar] [CrossRef]
- Milanic, M.; Bjorgan, A.; Larsson, M.; Strömberg, T.; Randeberg, L.L. Detection of hypercholesterolemia using hyperspectral imaging of human skin. In Clinical and Biomedical Spectroscopy and Imaging IV, Proceedings of SPIE—The International Society for Optical Engineering; Brown, J.Q., Deckert, V., Eds.; SPIE: Washington, DC, USA, 2015. [Google Scholar]
- Milanic, M.; Paluchowski, L.A.; Randeberg, L.L. Hyperspectral imaging for detection of arthritis: Feasibility and prospects. J. Biomed. Opt. 2015, 20, 96011. [Google Scholar] [CrossRef] [PubMed]
- Chin, J.A.; Wang, E.C.; Kibbe, M.R. Evaluation of hyperspectral technology for assessing the presence and severity of peripheral artery disease. J. Vasc. Surg. 2011, 54, 1679–1688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjorgan, A.; Denstedt, M.; Milanič, M.; Paluchowski, L.A.; Randeberg, L.L. Vessel contrast enhancement in hyperspectral images. In Optical Biopsy XIII: Toward Real-Time Spectroscopic Imaging and Diagnosis, Proceedings of SPIE—The International Society for Optical Engineering; Alfano, R.R., Demos, S.G., Eds.; SPIE: Washington, DC, USA, 2015. [Google Scholar]
- Akbari, H.; Kosugi, Y.; Kojima, K.; Tanaka, N. Blood vessel detection and artery-vein differentiation using hyperspectral imaging. In Proceedings of the 31st Annual International Conference of the IEEE Engineering in Medicine and Biology Society: Engineering the Future of Biomedicine, EMBC 2009, Minneapolis, MN, USA, 3–6 September 2009; pp. 1461–1464. [Google Scholar]
- Mordant, D.J.; Al-Abboud, I.; Muyo, G.; Gorman, A.; Sallam, A.; Ritchie, P.; Harvey, A.R.; McNaught, A.I. Spectral imaging of the retina. Eye 2011, 25, 309–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, M.; Chiba, T.; Nakamizo, A.; Kumashiro, R.; Murata, M.; Akahoshi, T.; Tomikawa, M.; Kikkawa, Y.; Yoshimoto, K.; Mizoguchi, M.; et al. Intraoperative visualization of cerebral oxygenation using hyperspectral image data: A two-dimensional mapping method. Int. J. Comput. Assist. Radiol. Surg. 2014, 9, 1059–1072. [Google Scholar] [CrossRef] [PubMed]
- Olweny, E.O.; Faddegon, S.; Best, S.L.; Jackson, N.; Wehner, E.F.; Tan, Y.K.; Zuzak, K.J.; Cadeddu, J.A. First Place: Renal Oxygenation During Robot-Assisted Laparoscopic Partial Nephrectomy: Characterization Using Laparoscopic Digital Light Processing Hyperspectral Imaging. J. Endourol. 2013, 27, 265–269. [Google Scholar] [CrossRef]
- Akbari, H.; Halig, L.V.; Schuster, D.M.; Osunkoya, A.; Master, V.; Nieh, P.T.; Chen, G.Z.; Fei, B. Hyperspectral imaging and quantitative analysis for prostate cancer detection. J. Biomed. Opt. 2012, 17, 0760051. [Google Scholar] [CrossRef] [Green Version]
- Lu, G.; Qin, X.; Wang, D.; Chen, Z.G.; Fei, B. Quantitative wavelength analysis and image classification for intraoperative cancer diagnosis with hyperspectral imaging. In Progress in Biomedical Optics and Imaging—Proceedings of SPIE; SPIE: Washington, DC, USA, 2015; Volume 9415. [Google Scholar]
- Lu, G.; Wang, D.; Qin, X.; Halig, L.; Muller, S.; Zhang, H.; Chen, A.; Pogue, B.W.; Chen, Z.G.; Fei, B. Framework for hyperspectral image processing and quantification for cancer detection during animal tumor surgery. J. Biomed. Opt. 2015, 20, 126012. [Google Scholar] [CrossRef] [Green Version]
- Panasyuk, S.V.; Yang, S.; Faller, D.V.; Ngo, D.; Lew, R.A.; Freeman, J.E.; Rogers, A.E. Medical hyperspectral imaging to facilitate residual tumor identification during surgery. Cancer Biol. Ther. 2007, 6, 439–446. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Wang, H.; Li, Q. Tongue tumor detection in medical hyperspectral images. Sensors 2012, 12, 162–174. [Google Scholar] [CrossRef] [PubMed]
- Duann, J.-R.; Jan, C.-I.; Ou-Yang, M.; Lin, C.-Y.; Mo, J.-F.; Lin, Y.-J.; Tsai, M.-H.; Chiou, J.-C. Separating spectral mixtures in hyperspectral image data using independent component analysis: Validation with oral cancer tissue sections. J. Biomed. Opt. 2013, 18, 126005. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.; Krueger, J.; Gareau, D. Hyperspectral imaging for melanoma screening. In Photonic Therapeutics and Diagnostics X, Proceedings of SPIE—The International Society for Optical Engineering; Choi, B., Kollias, N., Zeng, H., Eds.; SPIE: Washington, DC, USA, 2014. [Google Scholar]
- Nagaoka, T.; Kiyohara, Y.; Koga, H.; Nakamura, A.; Saida, T.; Sota, T. Modification of a melanoma discrimination index derived from hyperspectral data: A clinical trial conducted in 2 centers between March 2011 and December 2013. Ski. Res. Technol. 2015, 21, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Song, E.; Grant-Kels, J.M.; Swede, H.; D’Antonio, J.L.; Lachance, A.; Dadras, S.S.; Kristjansson, A.K.; Ferenczi, K.; Makkar, H.S.; Rothe, M.J. Paired comparison of the sensitivity and specificity of multispectral digital skin lesion analysis and reflectance confocal microscopy in the detection of melanoma in vivo: A cross-sectional study. J. Am. Acad. Dermatol. 2016, 75, 1187–1192.e2. [Google Scholar] [CrossRef] [PubMed]
- Fabelo, H.; Ortega, S.; Ravi, D.; Kiran, B.R.; Sosa, C.; Bulters, D.; Callicó, G.M.; Bulstrode, H.; Szolna, A.; Piñeiro, J.F.; et al. Spatio-spectral classification of hyperspectral images for brain cancer detection during surgical operations. PLoS One 2018, 13, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Xue, Y.; Xiao, G.; Zhang, J. Study on microscope hyperspectral medical imaging method for biomedical quantitative analysis. Sci. Bull. 2008, 53, 1431–1434. [Google Scholar] [CrossRef]
- Akbari, H.; Halig, L.V.; Zhang, H.; Wang, D.; Chen, Z.G.; Fei, B. Detection of Cancer Metastasis Using a Novel Macroscopic Hyperspectral Method. Proc. SPIE 2012, 8317, 831711. [Google Scholar] [CrossRef]
- Ortega, S.; Fabelo, H.; Camacho, R.; de la Luz Plaza, M.; Callicó, G.M.; Sarmiento, R. Detecting brain tumor in pathological slides using hyperspectral imaging. Biomed. Opt. Express 2018, 9, 818. [Google Scholar] [CrossRef]
- Akalin, A.; Mu, X.; Kon, M.A.; Ergin, A.; Remiszewski, S.H.; Thompson, C.M.; Raz, D.J.; Diem, M. Classification of malignant and benign tumors of the lung by infrared spectral histopathology (SHP). Lab. Investig. 2015, 95, 406–421. [Google Scholar] [CrossRef]
- Wu, D.; Sun, D.-W. Advanced applications of hyperspectral imaging technology for food quality and safety analysis and assessment: A review—Part I: Fundamentals. Innov. Food Sci. Emerg. Technol. 2013, 19, 1–14. [Google Scholar] [CrossRef]
- Holt, E.E.; Aikio, M.; Tutkimuskeskus, V.T. Hyperspectral Prism-grating-prism Imaging Spectrograph. In Hyperspectral Prism-grating-prism Imaging Spectrograph; VTT julkaisuja; Technical Research Centre of Finland: Espoo, Finland, 2001; ISBN 9789513858506. [Google Scholar]
- Fabelo, H.; Ortega, S.; Kabwama, S.; Callico, G.M.; Bulters, D.; Szolna, A.; Pineiro, J.F.; Sarmiento, R. HELICoiD project: A new use of hyperspectral imaging for brain cancer detection in real-time during neurosurgical operations. In Hyperspectral Imaging Sensors: Innovative Applications and Sensor Standards 2016, Proceedings of SPIE—The International Society for Optical Engineering; Bannon, D.P., Ed.; SPIE: Washington, DC, USA, 2016. [Google Scholar]
- Ortega, S.; Callico, G.M.; Plaza, M.L.; Camacho, R.; Fabelo, H.; Sarmiento, R. Hyperspectral database of pathological in-vitro human brain samples to detect carcinogenic tissues. In Proceedings of the International Symposium on Biomedical Imaging, Prague, Czech Republic, 13–16 April 2016. [Google Scholar]
- Gat, N. Imaging spectroscopy using tunable filters: A review. In Wavelet Applications VII, Proceedings of SPIE—The International Society for Optical Engineering; Szu, H.H., Vetterli, M., Campbell, W.J., Eds.; SPIE: Washington, DC, USA, 2000. [Google Scholar]
- Leitner, R.; De Biasio, M.; Arnold, T.; Dinh, C.V.; Loog, M.; Duin, R.P.W. Multi-spectral video endoscopy system for the detection of cancerous tissue. Pattern Recognit. Lett. 2013, 34, 85–93. [Google Scholar] [CrossRef]
- Hagen, N.; Kudenov, M.W. Review of snapshot spectral imaging technologies. Opt. Eng. 2013. [Google Scholar] [CrossRef]
- Chen, G.; Qian, S.-E. Denoising of Hyperspectral Imagery Using Principal Component Analysis and Wavelet Shrinkage. IEEE Trans. Geosci. Remote Sens. 2011, 49, 973–980. [Google Scholar] [CrossRef]
- Yuan, Q.; Zhang, L.; Shen, H. Hyperspectral Image Denoising Employing a Spectral-Spatial Adaptive Total Variation Model. IEEE Trans. Geosci. Remote Sens. 2012, 50, 3660–3677. [Google Scholar] [CrossRef]
- Kester, R.T.; Bedard, N.; Gao, L.; Tkaczyk, T.S. Real-time snapshot hyperspectral imaging endoscope. J. Biomed. Opt. 2011, 16, 56005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, Q.; Cheng, J.-H.; Sun, D.-W.; Zeng, X.-A. Advances in Feature Selection Methods for Hyperspectral Image Processing in Food Industry Applications: A Review. Crit. Rev. Food Sci. Nutr. 2015, 55, 1368–1382. [Google Scholar] [CrossRef] [PubMed]
- Khodr, J.; Younes, R. Dimensionality reduction on hyperspectral images: A comparative review based on artificial datas. In Proceedings of the 2011 4th International Congress on Image and Signal Processing, Shanghai, China, 15–17 October 2011; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA, 2011. [Google Scholar]
- Pattern Recognition; Elsevier: Amsterdam, The Netherlands, 2009; ISBN 9781597492720.
- Bioucas-Dias, J.M.; Plaza, A.; Dobigeon, N.; Parente, M.; Du, Q.; Gader, P.; Chanussot, J. Hyperspectral unmixing overview: Geometrical, statistical, and sparse regression-based approaches. IEEE J. Sel. Top. Appl. Earth Obs. Remote Sens. 2012, 5, 354–379. [Google Scholar] [CrossRef]
- Turvey, C.G.; Mclaurin, M.K. Applicability of the Normalized Difference Vegetation Index (NDVI) in Index-Based Crop Insurance Design. Weather. Clim. Soc. 2012, 4, 271–284. [Google Scholar] [CrossRef]
- Nagaoka, T.; Nakamura, A.; Okutani, H.; Kiyohara, Y.; Sota, T. A possible melanoma discrimination index based on hyperspectral data: A pilot study. Ski. Res. Technol. 2012, 18, 301–310. [Google Scholar] [CrossRef]
- Chang, C.-I. Hyperspectral data processing: Algorithm design and analysis; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Zuzak, K.J.; Naik, S.C.; Alexandrakis, G.; Hawkins, D.; Behbehani, K.; Livingston, E.H. Characterization of a Near-Infrared Laparoscopic Hyperspectral Imaging System for Minimally Invasive Surgery. Anal. Chem. 2007, 79, 4709–4715. [Google Scholar] [CrossRef]
- Ghamisi, P.; Plaza, J.; Chen, Y.; Li, J.; Plaza, A.J. Advanced Spectral Classifiers for Hyperspectral Images: A review. IEEE Geosci. Remote Sens. Mag. 2017, 5, 8–32. [Google Scholar] [CrossRef]
- Xu, R.; WunschII, D. Survey of Clustering Algorithms. IEEE Trans. Neural Networks 2005, 16, 645–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fauvel, M.; Tarabalka, Y.; Benediktsson, J.A.; Chanussot, J.; Tilton, J.C. Advances in spectral-spatial classification of hyperspectral images. Proc. IEEE 2013, 101, 652–675. [Google Scholar] [CrossRef]
- Claridge, E.; Hidović-Rowe, D.; Taniere, P.; Ismail, T. Quantifying mucosal blood volume fraction from multispectral images of the colon. In Medical Imaging 2007: Physiology, Function, and Structure from Medical Images; Manduca, A., Hu, X.P., Eds.; SPIE: Washington, DC, USA.
- Hidović-Rowe, D.; Claridge, E.; Ismail, T.; Taniere, P.; Graham, J. Analysis of multispectral images of the colon to reveal histological changes characteristic of cancer. Med. Image Underst. Anal. MIUA 2006, 1, 66–70. [Google Scholar]
- Akbari, H.; Kosugi, Y.; Kojima, K.; Tanaka, N. Wavelet-Based Compression and Segmentation of Hyperspectral Images in Surgery. In Lecture Notes in Computer Science; Springer Nature: Berlin, Germany; pp. 142–149.
- Schols, R.M.; Alic, L.; Beets, G.L.; Breukink, S.O.; Wieringa, F.P.; Stassen, L.P.S. Automated Spectroscopic Tissue Classification in Colorectal Surgery. Surg. Innov. 2015, 22, 557–567. [Google Scholar] [CrossRef]
- Schols, R.M.; Dunias, P.; Wieringa, F.P.; Stassen, L.P.S. Multispectral characterization of tissues encountered during laparoscopic colorectal surgery. Med. Eng. Phys. 2013, 35, 1044–1050. [Google Scholar] [CrossRef] [PubMed]
- Han, Z.; Zhang, A.; Wang, X.; Sun, Z.; Wang, M.D.; Xie, T. In vivo use of hyperspectral imaging to develop a noncontact endoscopic diagnosis support system for malignant colorectal tumors. J. Biomed. Opt. 2016, 21, 016001. [Google Scholar] [CrossRef] [PubMed]
- Wu, I.-C.; Syu, H.-Y.; Jen, C.-P.; Lu, M.-Y.; Chen, Y.-T.; Wu, M.-T.; Kuo, C.-T.; Tsai, Y.-Y.; Wang, H.-C. Early identification of esophageal squamous neoplasm by hyperspectral endoscopic imaging. Sci. Rep. 2018, 8, 13797. [Google Scholar] [CrossRef]
- Beaulieu, R.J.; Goldstein, S.D.; Singh, J.; Safar, B.; Banerjee, A.; Ahuja, N. Automated diagnosis of colon cancer using hyperspectral sensing. Int. J. Med. Robot. Comput. Assist. Surg. 2018, 14, e1897. [Google Scholar] [CrossRef]
- Clancy, N.T.; Arya, S.; Stoyanov, D.; Singh, M.; Hanna, G.B.; Elson, D.S. Intraoperative measurement of bowel oxygen saturation using a multispectral imaging laparoscope. Biomed. Opt. Express 2015, 6, 4179. [Google Scholar] [CrossRef]
- Wirkert, S.J.; Kenngott, H.; Mayer, B.; Mietkowski, P.; Wagner, M.; Sauer, P.; Clancy, N.T.; Elson, D.S.; Maier-Hein, L. Robust near real-time estimation of physiological parameters from megapixel multispectral images with inverse Monte Carlo and random forest regression. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 909–917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cha, J.; Shademan, A.; Le, H.N.D.; Decker, R.; Kim, P.C.W.; Kang, J.U.; Krieger, A. Multispectral tissue characterization for intestinal anastomosis optimization. J. Biomed. Opt. 2015, 20, 106001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clancy, N.T.; Arya, S.; Stoyanov, D.; Du, X.; Hanna, G.B.; Elson, D.S. Imaging the spectral reflectance properties of bipolar radiofrequency-fused bowel tissue. In Proceedings of the Clinical and Biomedical Spectroscopy and Imaging IV, Munich, Germany, 21–25 June 2015; Volume 9537. [Google Scholar]
- Zuzak, K.J.; Naik, S.C.; Alexandrakis, G.; Hawkins, D.; Behbehani, K.; Livingston, E. Intraoperative bile duct visualization using near-infrared hyperspectral video imaging. Am. J. Surg. 2008, 195, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Mitra, K.; Melvin, J.; Chang, S.; Park, K.; Yilmaz, A.; Melvin, S.; Xu, R.X. Indocyanine-green-loaded microballoons for biliary imaging in cholecystectomy. J. Biomed. Opt. 2012, 17, 116025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, B. Robotic Surgery—A Personal View of the Past, Present and Future. Int. J. Adv. Robot. Syst. 2015, 12, 54. [Google Scholar] [CrossRef]
- Akbari, H.; Kosugi, Y.; Kojima, K.; Tanaka, N. Detection and analysis of the intestinal ischemia using visible and invisible hyperspectral imaging. IEEE Trans. Biomed. Eng. 2010, 57, 2011–2017. [Google Scholar] [CrossRef]
- Akbari, H.; Uto, K.; Kosugi, Y.; Kojima, K.; Tanaka, N. Cancer detection using infrared hyperspectral imaging. Cancer Sci. 2011, 102, 852–857. [Google Scholar] [CrossRef] [Green Version]
- Gu, X.; Han, Z.; Yao, L.; Zhong, Y.; Shi, Q.; Fu, Y.; Liu, C.; Wang, X.; Xie, T. Image enhancement based onin vivohyperspectral gastroscopic images: A case study. J. Biomed. Opt. 2016, 21, 101412. [Google Scholar] [CrossRef] [PubMed]
- Ogihara, H.; Hamamoto, Y.; Fujita, Y.; Goto, A.; Nishikawa, J.; Sakaida, I. Development of a Gastric Cancer Diagnostic Support System with a Pattern Recognition Method Using a Hyperspectral Camera. J. Sens. 2016, 2016, 1–6. [Google Scholar] [CrossRef]
- Hohmann, M.; Kanawade, R.; Klämpfl, F.; Douplik, A.; Mudter, J.; Neurath, M.F.; Albrecht, H. In-vivo multispectral video endoscopy towards in-vivo hyperspectral video endoscopy. J. Biophotonics 2017, 10, 553–564. [Google Scholar] [CrossRef] [PubMed]
- Masood, K.; Rajpoot, N.; Rajpoot, K.; Qureshi, H. Hyperspectral Colon Tissue Classification using Morphological Analysis. In Proceedings of the International Conference on Emerging Technologies, Peshawar, Pakistan, 13–14 November 2006; pp. 735–741. [Google Scholar]
- Rajpoot, K.; Rajpoot, N. SVM Optimization for Hyperspectral Colon Tissue Cell Classification. In Medical Image Computing and Computer-Assisted Intervention (MICCAI) 2004; Springer Nature: Berlin, Germany, 2004; pp. 829–837. [Google Scholar] [Green Version]
- Masood, K.; Rajpoot, N. Texture based classification of hyperspectral colon biopsy samples using CLBP. In 2009 IEEE International Symposium on Biomedical Imaging: From Nano to Macro; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA, 2009. [Google Scholar]
- Zhu, S.; Su, K.; Liu, Y.; Yin, H.; Li, Z.; Huang, F.; Chen, Z.; Chen, W.; Zhang, G.; Chen, Y. Identification of cancerous gastric cells based on common features extracted from hyperspectral microscopic images. Biomed. Opt. Express 2015, 6, 1135–1145. [Google Scholar] [CrossRef] [PubMed]
- Leavesley, S.J.; Walters, M.; Lopez, C.; Baker, T.; Favreau, P.F.; Rich, T.C.; Rider, P.F.; Boudreaux, C.W. Hyperspectral imaging fluorescence excitation scanning for colon cancer detection. J. Biomed. Opt. 2016, 21, 104003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leavesley, S.J.; Deal, J.; Martin, W.A.; Lall, M.; Lopez, C.; Rich, T.C.; Boudreaux, C.W.; Rider, P.F.; Hill, S. Colorectal cancer detection by hyperspectral imaging using fluorescence excitation scanning. In Optical Biopsy XVI: Toward Real-Time Spectroscopic Imaging and Diagnosis; Alfano, R.R., Demos, S.G., Eds.; SPIE: Washington, DC, USA, 2018; Volume 10489, p. 19. [Google Scholar]
- Deal, J.; Harris, B.; Martin, W.; Lall, M.; Lopez, C.; Boudreaux, C.; Rich, T.; Leavesley, S.; Rider, P. Demystifying autofluorescence with excitation scanning hyperspectral imaging. In Imaging, Manipulation, and Analysis of Biomolecules, Cells, and Tissues XVI; Farkas, D.L., Nicolau, D.V., Leif, R.C., Eds.; SPIE: Washington, DC, USA, 2018; Volume 10497, p. 40. [Google Scholar]
- Kunhoth, S.; Al Maadeed, S. Building a multispectral image dataset for colorectal tumor biopsy. In Proceedings of the 2017 13th International Wireless Communications and Mobile Computing Conference (IWCMC), Valencia, Spain, 26–30 June 2017. [Google Scholar]
- Cassidy, R.J.; Berger, J.; Lee, K.; Maggioni, M.; Coifman, R.R. Analysis of hyperspectral colon tissue images using vocal synthesis models. In Proceedings of the Conference Record of the Thirty-Eighth Asilomar Conference on Signals, Systems and Computers, Pacific Grove, CA, USA, 7–10 November 2004; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA, 2004. [Google Scholar]
- Cassidy, R.J.; Berger, J.; Lee, K. Auditory Display of Hyperspectral Colon Tissue Images using Vocal Synthesis Models. In Proceedings of the ICAD 04óTenth Meeting of the International Conference on Auditory Display, Sydney, Australia, 6–9 July 2004. [Google Scholar]
- Kiyotoki, S.; Nishikawa, J.; Okamoto, T.; Hamabe, K.; Saito, M.; Goto, A.; Fujita, Y.; Hamamoto, Y.; Takeuchi, Y.; Satori, S.; et al. New method for detection of gastric cancer by hyperspectral imaging: A pilot study. J. Biomed. Opt. 2013, 18, 26010. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Zhang, D.; Wang, C.; Dai, B.; Zhao, M.; Li, B. Hyperspectral Imaging and SPA–LDA Quantitative Analysis for Detection of Colon Cancer Tissue. J. Appl. Spectrosc. 2018, 85, 307–312. [Google Scholar] [CrossRef]
- Kumashiro, R.; Konishi, K.; Chiba, T.; Akahoshi, T.; Nakamura, S.; Murata, M.; Tomikawa, M.; Matsumoto, T.; Maehara, Y.; Hashizume, M. Integrated Endoscopic System Based on Optical Imaging and Hyperspectral Data Analysis for Colorectal Cancer Detection. Anticancer Res. 2016, 36, 3925–3932. [Google Scholar]
- Lim, H.-T.; Murukeshan, V.M. A four-dimensional snapshot hyperspectral video-endoscope for bio-imaging applications. Sci. Rep. 2016, 6. [Google Scholar] [CrossRef]
- Bhutiani, N.; Samykutty, A.; McMasters, K.M.; Egilmez, N.K.; McNally, L.R. In vivo tracking of orally-administered particles within the gastrointestinal tract of murine models using multispectral optoacoustic tomography. Photoacoustics 2019, 13, 46–52. [Google Scholar] [CrossRef]
- Joshi, B.P.; Wang, T.D. Emerging trends in endoscopic imaging. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 72–73. [Google Scholar] [CrossRef]
- Qiu, Z.; Khondee, S.; Duan, X.; Li, H.; Mandella, M.J.; Joshi, B.P.; Zhou, Q.; Owens, S.R.; Kurabayashi, K.; Oldham, K.R.; et al. Vertical Cross-sectional Imaging of Colonic Dysplasia In Vivo With Multi-spectral Dual Axes Confocal Endomicroscopy. Gastroenterology 2014, 146, 615–617. [Google Scholar] [CrossRef] [Green Version]
- Joshi, B.P.; Miller, S.J.; Lee, C.M.; Seibel, E.J.; Wang, T.D. Multispectral Endoscopic Imaging of Colorectal Dysplasia In Vivo. Gastroenterology 2012, 143, 1435–1437. [Google Scholar] [CrossRef] [Green Version]
- Clancy, N.T.; Lin, J.; Arya, S.; Hanna, G.B.; Elson, D.S. Dual multispectral and 3D structured light laparoscope. In Proceedings of the Multimodal Biomedical Imaging X, San Francisco, CA, USA, 7–12 February 2015; Volume 9316, p. 93160C. [Google Scholar]
- Fornasaro, S.; Vicario, A.; De Leo, L.; Bonifacio, A.; Not, T.; Sergo, V. Potential use of MCR-ALS for the identification of coeliac-related biochemical changes in hyperspectral Raman maps from pediatric intestinal biopsies. Integr. Biol. 2018, 10, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Kröger-Lui, N.; Gretz, N.; Haase, K.; Kränzlin, B.; Neudecker, S.; Pucci, A.; Regenscheit, A.; Schönhals, A.; Petrich, W. Rapid identification of goblet cells in unstained colon thin sections by means of quantum cascade laser-based infrared microspectroscopy. Analyst 2015, 140, 2086–2092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, C.R.; Prtljaga, N.; Farries, M.; Ward, J.; Napier, B.; Lloyd, G.R.; Nallala, J.; Stone, N.; Bang, O. Mid-infrared multispectral tissue imaging using a chalcogenide fiber supercontinuum source. Opt. Lett. 2018, 43, 999. [Google Scholar] [CrossRef] [PubMed]
- Iakovidis, D.K.; Sarmiento, R.; Silva, J.S.; Histace, A.; Romain, O.; Koulaouzidis, A.; Dehollain, C.; Pinna, A.; Granado, B.; Dray, X. Towards Intelligent Capsules for Robust Wireless Endoscopic Imaging of the Gut. IEEE Int. Conf. Imaging Syst. Tech. 2014, 95–100. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Application/Disease | Spectral Range (nm) | HSI Technology | Experiment Type | Study Subjects | Data Analysis Methods (Category */Method ¥) | Reference(s) |
|---|---|---|---|---|---|---|
| Biliary tree visualization | 650–1050 | LCTF | In-vivo | Swine | D, E/PCA | [55] |
| Colon cancer detection | 400–700 | LCTF | Ex-vivo | Humans | F, E/LPM | [59,60] |
| Organs identification during surgery | 900–1700 | Push-broom | In-vivo | Swine | SA, P/DWT; C/SOM | [61] |
| Identifying tissues during surgery | 350–1830 | DRS | In-vivo | Humans | SA, F/SGAD; C/SVM | [62] |
| Tissue identification during colorectal surgery | 440–1830 | DRS | Ex-vivo | Humans | SA, C/TPCR | [63] |
| Malignant colorectal tumors and adenomatous polyps | 405–665 | Filter Wheel | In-vivo | Humans | R/RDFS; C/SVM | [64] |
| Colon cancer detection | 300–1800 | Spectroscopy | Ex-vivo | Humans | C/LDA; C/SVM | [66] |
| Oxygenation measurement (small bowel) | 400–720 | LCTF | In-vivo | Swine | Ex/Linear light model | [67] |
| Oxygenation measurement (small bowel) | 470–700 | Filter-based | In-vivo | Swine | Ex/Non-linear light model | [68] |
| Suture recommendation (intestinal anastomosis) | 470–770 | LED-based | Ex-vivo | Swine | Ex/2D-filtering, SAM and composite images from the multispectral image | [69] |
| Monitoring radiofrequency fusions in small bowel | 460–700 | LCTF | In-vivo | Swine | Ex/Linear light model | [70] |
| Biliary trees identification | 650–1100 | LCTF | In-vivo | Swine | D, E/PCA | [71] |
| Biliary anatomy visualization | 650–700 | LCTF | Ex-vivo | Swine | S/LMM, R/PCA | [72] |
| Intestinal ischemia identification | 400–1700 | Push-broom | In-vivo | Swine | I/Ischemia Index; C/SVM | [74] |
| Gastric cancer detection | 1000–2500 | Push-broom | Ex-vivo | Humans | I/Cancer Index; C/SVM | [75] |
| Gastric ulcers | 405–665 | Filter Wheel | In-vivo | Humans | R, E/DI | [76] |
| Gastric cancer | 400–800 | N/A | Ex-vivo | Humans | C/MDC | [77,89] |
| Gastric cancer | 400–650 | Tunable Light Source | In-vivo | Humans | C/SVM; C/RF; C/RobustBoost; C/AdaBoost | [78] |
| Colon cancer detection | 450–850 | Tunable Light Source | In-vitro | Humans | R/ICA; R/PCA; C/k-Means; C/LDA; C/SVM | [79,80] |
| Colon cancer detection | 440–700 | Tunable Light Source | In-vitro | Humans | F/CLBP; R/PCA; C/LDA; C/SVM | [81] |
| Gastric cancer cell identification | 420–720 | LCTF | In-vitro | Humans | R/Manual band selection; C/ANNs | [82] |
| Colonic adenocarcinoma identification | 390–700 | LCTF | Ex-vivo | Humans | SA | [83] |
| Colon cancer detection | 360–550 | LCTF | In-vitro | Humans | S/LMM; R/PCA | [84,85] |
| Colorectal cell differentiation | 400–1700 | LCTF | In-vitro | Humans | F/LBP, C/RF | [86] |
| Colon cancer detection | 400–1000 | Push-broom | Ex-vivo | Humans | DR/SPA; C/LDA | [90] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega, S.; Fabelo, H.; Iakovidis, D.K.; Koulaouzidis, A.; Callico, G.M. Use of Hyperspectral/Multispectral Imaging in Gastroenterology. Shedding Some–Different–Light into the Dark. J. Clin. Med. 2019, 8, 36. https://doi.org/10.3390/jcm8010036
Ortega S, Fabelo H, Iakovidis DK, Koulaouzidis A, Callico GM. Use of Hyperspectral/Multispectral Imaging in Gastroenterology. Shedding Some–Different–Light into the Dark. Journal of Clinical Medicine. 2019; 8(1):36. https://doi.org/10.3390/jcm8010036
Chicago/Turabian StyleOrtega, Samuel, Himar Fabelo, Dimitris K. Iakovidis, Anastasios Koulaouzidis, and Gustavo M. Callico. 2019. "Use of Hyperspectral/Multispectral Imaging in Gastroenterology. Shedding Some–Different–Light into the Dark" Journal of Clinical Medicine 8, no. 1: 36. https://doi.org/10.3390/jcm8010036